People with learning disabilities 2026 update
People with learning disabilities
- Glossary
- Executive Summary
- Introduction
- Local picture
- Health inequalities
- Physical health outcomes
- Respiratory conditions including COVID-19 and vaccination uptake
- Cardiovascular disease
- Hypertension
- Weight management
- Type 2 Diabetes
- Cancer and cancer screening
- Physical activity
- Gender based inequalities within the learning disabilities population
- Primary care
- Variations in physical health between Surrey Heartlands Four ‘Places’
- Dental outcome
- Postural care
- Dementia and learning disabilities
- People with learning disabilities and ageing
- Sensory Impairment
- Podiatry
- Sex, sexual health, sexual awareness and sexual expression
- Pregnancy care and outcomes
- Access to health services
- Access to primary care
- Access to acute healthcare
- Hospital learning disability team
- Specialist Health Care support
- Mental health and outcomes, including inpatient admissions
- STOMP and STAMP (STopping Over Medication of people with a learning disability, autism or both with Psychotropic medicines)
- Inpatient use
- Wider determinants
- Poverty and Health
- Accommodation
- Employment
- Hate and mate crime
- Domestic Abuse
- Crime, concerning behaviour
- Community voice
- Evidence base, what works
- Summary of Recommendations
- Appendices
- Chapter Contacts
- References
Glossary
ADHD Attention Deficit Hyperactivity Disorder
AHC Annual Health Check
ASD / ASC Autistic Spectrum Disorder / Autistic Spectrum Condition
BMI Body Mass Index
CASSR Councils with Adult Social Services Responsibilities
CETR Care, Education and Treatment Review
CIPFA Chartered Institute of Public Finance and Accountancy
CQC Care Quality Commission
CTR Care and Treatment Review
CTPLD Community Team for People with Learning Disabilities
CVD Cardiovascular Disease
DNACPR Do not Attempt Resuscitation
EHCP Education, Health and Care Plan
GORD Gastric oesophageal reflux disease
ICP Integrated Care Partnership
ICS Integrated Care System
IHD Ischaemic Heart Disease
JSNA Joint Strategic Needs Assessment
LeDeR Learning from Lives and Deaths of People with a Learning Disability
NHS National Health Service
NICE National Institute for Health and Care Excellence
PANSI Projecting Adult Needs and Service Information
PCC Primary Client Category
PLD People with Learning Disabilities
POPPI Projecting Older People Population Information
PSR Primary Support Reason
SCC Surrey County Council
SCIE Social Care Institute for Excellence
STOMP Stopping over medication of people with a learning disability, autism or both
STAMP Supporting Treatment and Appropriate Medication in Paediatrics
TIA Transient Ischaemic Attack
Executive Summary
The national policy direction for people with a learning disability (including those with autism) remains one of a human rights-based approach and one where adults, children, and young people with a learning disability, and autistic adults, children and young people should be equal citizens in their communities as referenced in the ‘Building the Right Support Action plan 2022’ (BTRS plan)
This Joint Strategic Needs Assessment (JSNA) outlines what we know about the lives of people with learning disabilities of all ages in Surrey, their health outcomes and access including the experience of Covid, social care needs and provision, their living circumstances, education and employment and how much of a voice they have in their lives, services they use and their communities.
It also outlines where we need to know more about the impact of the cost-of-living crisis, access to community health, police services and support in prison for people with learning disabilities. In doing so, it challenges Surrey to ensure that the vision of ‘no one is left behind’ becomes a reality for this highly diverse group within our communities.
The JSNA makes fifty recommendations, testament to the need to better understand the experiences in Surrey of people with learning disabilities. These are threaded throughout the JSNA and are brought together in one section towards the end of the JSNA. They come under the following themes:
- Legislative / Policy Framework
- Primary care, all-age learning disability registers
- Learning disability population projections
- Number of adults with a learning disability open to Social Care
- Safeguarding
- Prevalence of behaviour risk factors
- Physical health outcomes
- Gender based inequalities within the learning disabilities population
- Primary Care
- Variations in physical health between Surrey Heartlands Four ‘Places’
- Dental outcome
- Postural care
- Dementia and learning disabilities
- People with learning disabilities and ageing
- Sensory Impairment
- Podiatry
- Sex, sexual health, sexual awareness and sexual expression
- Pregnancy care and outcomes
- Access to health services
- Mental health and outcomes, including inpatient admissions
- Integrated Intensive Support Service
- LAEP meeting and Care (education) and treatment reviews
- Future considerations for proposed Mental Health Act changes
- Poverty and Health
- Employment
- Domestic Abuse
- Crime, concerning behaviour
- Adult Social Care Survey England – 2023/24
Introduction
This JSNA outlines what we know about the lives of people with learning disabilities of all ages in Surrey, their health outcomes and access including the experience of Covid, social care needs and provision, their living circumstances, education and employment and how much of a voice they have in their lives, services they use and their communities.
It also outlines areas where we need to know more, for example about the impact of the cost-of-living crisis, access to community health, police services and support in prison for people with learning disabilities. In doing so, it challenges Surrey to ensure that the vision of ‘no one is left behind’ becomes a reality for this highly diverse group within our communities.
The JSNA aims to cover all ages as far as possible, with reference to further detail for children and young people contained within the Children and Young People with Additional Needs and Disabilities Joint Strategic Needs Assessment.
It seeks to look at support in the round and identify how people’s experiences can be better understood, the hard and soft intelligence, quantitative and qualitative data.
The county of Surrey falls into the boundaries of two integrated care systems – Surrey Heartlands (the predominant part) and Frimley. This JSNA attempts to cover both Surrey Heartlands and Frimley and specify where this has not been possible due to a lack of pertinent data.
Surrey context
The Community Vision for Surrey states that by 2030, Surrey will
‘…be a uniquely special place where everyone has a great start to life, people live healthy and fulfilling lives, are enabled to achieve their full potential and contribute to their community and no one is left behind.’
The ambitions for people that the Strategy set out are as follows:
- Children and young people are safe and feel safe and confident.
- Everyone benefits from education, skills and employment opportunities that help them succeed in life.
- Everyone lives healthy, active and fulfilling lives, and makes good choices about their well-being.
- Everyone gets the health and social care support and information they need at the right time and place.
- Communities are welcoming and supportive, especially of those most in need, and people feel able to contribute to community life.
The Strategy also set out ambitions for the place:
‘…our county’s economy to be strong, vibrant and successful and Surrey to be a great place to live, work and learn. A place that capitalises on its location and natural assets, and where communities feel, and people can support each other.’
In 2022 the refreshed Health and Well-Being Strategy set out Surrey’s priorities and captures the revised outcomes. It identifies specific groups of people who experience health inequalities that have been exacerbated during the COVID-19 pandemic and outlines how we need to collaborate so we can better meet their needs.
The Integrated Care System will focus on delivering these outcomes within our priority populations – communities of identity and geography which are often overlooked and currently most at risk of experiencing poor health outcomes, as identified by the COVID Community Impact Assessment and Rapid Needs Assessments.
This includes people who experience the poorest health outcomes:
- Children with additional needs and disabilities
- Adults with learning disabilities and/or autism
Surrey will remain focused on three interconnected priorities – supporting people to lead physically healthy lives / to have good mental health and emotional wellbeing and creating the contexts in which individuals and communities can reach their potential, with a clearer intent on addressing the wider determinants of health. These priorities adopt both primary prevention (stopping ill health in the first instance) and secondary/tertiary prevention (making sure things don’t get any worse) approach, and focus on providing the right physical, psychological, social and economic contexts for communities that experience the poorest health outcomes to begin to thrive.
The Health and Well Being Board strategic focus will continue to evolve, reflecting the latest data, evidence, and insights, including that presented in the different chapters of the Joint Strategic Needs Assessment (JSNA) as they are updated in accordance with the rolling programme.
Scope
What is a learning disability?
‘Learning disability’ is an umbrella term used to describe people who have “a significantly reduced ability to understand new or complex information and to learn new skills (impaired intelligence); a reduced ability to cope independently (impaired social functioning) and; a disability that started before adulthood, with a lasting effect on development”.
The term ‘intellectual disability’ is also used both within research and within the International Classification of Disease coding system where the description also includes impairment of cognitive, motor and social abilities. The coding system defines learning disability by severity using IQ as a guide; a person with an IQ less than 70 is considered to have a learning disability. Alongside an IQ of less than 70, the other two core criteria indicating a learning disability are significant impairment of social or adaptive functioning and onset in childhood. These are used as both diagnostic criteria and as a diagnosis code within the NHS.
For the purposes of this JSNA ‘learning disability’ is used as a definition except where children’s Special Educational Needs coded data is referenced as this utilises the terms ‘moderate learning difficulty’, ‘severe learning difficulty’ and ‘profound multiple learning difficulty’, which relate to general impairments in learning of different severity. These can be interchangeable with the term ‘learning disability’ and the groups of mild, moderate, severe and profound learning disabilities.
People with learning disabilities are not one homogenous group. They can have associated conditions, some of the most common of which are Down Syndrome, Autism, Williams Syndrome, Fragile X Syndrome and Cerebral Palsy. See Appendix 1 for further detail. [1][2][3][4]
What a learning disability is not
Mencap states that ‘a learning disability is different from a learning difficulty as a learning difficulty does not affect general intellect’. Learning difficulties can include dyslexia, dyspraxia, and dyscalculia. These learning difficulties can co-occur alongside a learning disability. A Learning Difficulty is a type of Special Education Need (SEN) which affects areas of learning, such as reading, writing, spelling and mathematics.
What causes learning disability [5]
We do not always know why a person has a learning disability [6]. Sometimes it is because a person’s brain development is affected, either before they are born, during their birth or in early childhood. Possible causes include:
- the mother becoming ill in pregnancy
- problems during the birth that stop enough oxygen getting to the brain
- the unborn baby having some genes passed on from its parents that make having a learning disability more likely
- illness, such as meningitis, or injury in early childhood
There are specific health conditions where a learning disability is more likely such as Down’s syndrome, where everyone is likely to have some level of learning disability, many autistic people, and people with cerebral palsy.
Mild Learning Disability is usually caused by a combination of restricted learning and social opportunities plus a high rate of low to average intellectual ability and learning disability in close relatives.
Moderate-to-profound Learning Disability usually has a specific biological cause.
Key policy drivers for changes or improvements related to learning disabilities
There are several key policy and guidance drivers for change and improvement relevant to people with learning disabilities.
The ‘Building the Right Support Action plan 2022’ published July 2022, is an action plan to strengthen community support for people with a learning disability and autistic people and to reduce reliance on mental health inpatient care.
The driver for the action plan is ‘adults, children, and young people with a learning disability, and autistic adults, children and young people should be equal citizens in their communities’.
The action plan brings together, in one place, commitments across systems to reduce reliance on inpatient care in mental health hospitals for children, young people and adults with a learning disability and for autistic children, young people and adults by building the right support in the community.
The key areas of focus set out in this action plan are:
- ensuring that people with a learning disability and autistic people of all ages experience high-quality, timely support that respects individual needs and wishes, and upholds human rights
- understanding that every citizen has the right to live an ordinary, self-directed life in their community
- keeping each person at the centre of our ambitions and ensuring that we consider a person’s whole life journey
- collaborating across systems to put in place the support that prevents crisis and avoids admission
- ensuring that, when someone would benefit from admission to a mental health hospital, they receive therapeutic, high-quality care and remain in hospital for the shortest time possible
- making sure that the people with a learning disability and autistic people who are in mental health hospitals right now are safe, and that they are receiving the care and treatment that is right for them
- working together to ensure that any barriers to an individual leaving a mental health hospital, when they are ready to do so, are removed
The action plan is arranged into 6 chapters:
- Keeping people safe and ensuring high-quality health and social care
- Making it easier to leave hospital
- Living an ordinary life in the community
- A good start to life
- Working with changes to the system
- National and local accountability to deliver
The immediate and future impacts of this action plan are included within this chapter.
The Down Syndrome Act 2022 became law in April 2022 with an aim of improving access to services and to improve the quality of life for people with Down’s syndrome. It aims to ensure that health, social care, education and other local authority services such as housing take account of the specific needs of people with Down’s syndrome when commissioning or providing services.
The Act requires the Secretary of State to publish guidance for relevant authorities (for example, NHS hospitals or local councils) on the steps it would be appropriate for those authorities to take to meet the needs of people with Down’s syndrome when carrying out some of their most important functions. Once the guidance is published these authorities are legally required to take the guidance into account when providing certain core services.
A call for evidence is currently underway to inform the guidance.
Recommendation: Following the publication of the evidence we will review whether the detail of Down Syndrome Act is already in place and consider the impact of the Act and subsequent guidance both on this community and the wider community of people with learning disabilities.
The NHS Long Term Plan (2019), Chapter Three, sets the NHS’s priorities for care quality and outcomes improvement for the decade from 2019 which includes people with learning disabilities.
The priorities are:
Action taken to tackle the causes of morbidity and preventable deaths in people with a learning disability and for autistic people by:
- Increasing uptake of the existing annual health check (AHC) in primary care for people aged over 14 years with a learning disability to at least 75% of those eligible.
- Expand the Stopping over medication of people with a learning disability autism or both and Supporting Treatment and Appropriate Medication in Paediatrics (STOMP-STAMP) programmes to stop the overmedication of people with a learning disability.
- Continue to fund the Learning Disabilities Mortality Review Programme (LeDeR), the first national programme aiming to make improvements to the lives of people with learning disabilities.
The whole NHS will improve its understanding of the needs of people with learning disabilities and autism, and work together to improve their health and wellbeing
- NHS staff will receive information and training on supporting people with a learning disability and/ or autism (this has since developed into the Oliver McGowan Mandatory Training)
- Sustainability and Transformation Partnerships (STPs) and integrated care systems (ICSs) will be expected to make sure all local healthcare providers are making reasonable adjustments to support people with a learning disability or autism.
- National learning disability improvement standards will be implemented and will apply to all services funded by the NHS.
- By 2023/24, a ‘digital flag’ in the patient record will ensure staff know a patient has a learning disability or autism
- Work with the Department for Education and local authorities to improve their awareness of, and support for, children and young people with learning disabilities, autism or both
- Work with partners to bring hearing, sight and dental checks to children and young people with a learning disability, autism or both in special residential schools
Children and young people with suspected autism wait too long before being provided with a diagnostic assessment
- Autism diagnosis will be included alongside work with children and young people’s mental health services to test and implement the most effective ways to reduce waiting times for specialist services to attempt to achieve timely diagnostic assessments in line with best practice guidelines.
- Together with local authority children’s social care and education services as well as expert charities, we will jointly develop packages to support children with autism or other neurodevelopmental disorders including attention deficit hyperactivity disorder (ADHD) and their families, throughout the diagnostic process.
- By 2023/24 children and young people with a learning disability, autism or both with the most complex needs will have a designated keyworker, implementing the recommendation made by Dame Christine Lenehan.
Children, young people and adults with a learning disability, autism or both, with the most complex needs, have the same rights to live fulfilling lives
- By March 2023/24, inpatient provision will have reduced to less than half of 2015 levels (on a like for like basis and taking into account population growth).
- For everyone million adults, there will be no more than 30 people with a learning disability and/or autism cared for in an inpatient unit.
- For children and young people, no more than 12 to 15 children with a learning disability, autism, or both per million, will be cared for in an inpatient facility.
- To move more care to the community, we will support local systems to take greater control over how budgets are managed. Drawing on learning from the New Care Models in tertiary mental health services, local providers will be able to take control of budgets to reduce avoidable admissions, enable shorter lengths of stay and end out of area placements.
- Where possible, people with a learning disability, autism or both will be enabled to have a personal health budget (PHBs).
Increased investment in intensive, crisis and forensic community support will also enable more people to receive personalised care in the community, closer to home, and reduce preventable admissions to inpatient services
Every local health system will be expected to use some of this growing community health services investment to have a seven-day specialist multidisciplinary service and crisis care. We will continue to work with partners to develop specialist community teams for children and young people, such as the Ealing Model, which has evidenced that an intensive support approach prevents children being admitted into institutional care.
Focus on improving the quality of inpatient care across the NHS and independent sector. By 2023/24, all care commissioned by the NHS will need to meet the Learning Disability Improvement Standards
- Work with the CQC to implement recommendations on restricting the use of seclusion, long-term segregation and restraint for all patients in inpatient settings, particularly for children and young people.
- Closely monitor and bring down the length of time people stay in inpatient care settings and support earlier transfers of care from inpatient settings.
- All areas of the country will implement and be monitored against a ‘12-point discharge plan’ to ensure discharges are timely and effective.
- Review and look to strengthen the existing Care, Education and Treatment Review (CETR) and Care and Treatment Review (CTR) policies, in partnership with people with a learning disability, autism or both, families and clinicians to assess their effectiveness in preventing and supporting discharge planning. This update was released in January 2023.
The Surrey Heartlands geography has a three-year delivery plan 2021/22 to2023/24 which describes their commitments against the long-term plan and is aligned with the Frimley plan to ensure Surrey wide coverage. The county of Surrey falls into the boundaries of two systems – Surrey Heartlands (the larger part) and Frimley. The Surrey Heartlands delivery plan includes specific projects and actions that were committed to against the long-term plan including AHC delivery and reducing reliance on inpatient beds. Much of the plan is referenced within this JSNA.
Recommendation: Use the outputs from all of the reports of The learning disability improvement standards for NHS trusts in strategic discussions to share good practice and reduce unwarranted variation across Surrey.
Recommendation: Joint work across health and social care system leaders, including leaders at ‘place’, to ensure that the full benefits of the Fuller Stocktake are fully realised for people with a learning disability.
Local picture
Population distribution
Primary care, all-age learning disability registers
Learning disability registers are lists of children, young people and adults who have a learning disability. The register is used by doctors to ensure that people with a learning disability can get the right help and support. Young people and adults over 14 years can have a free AHC (see the access section for uptake of health checks).
To get on the register the GP must enter an appropriate recognised learning disability code onto the patient’s records (usually simply “Learning Disability” but there are variations that will also get picked up). If the patient has the correct code in their notes they are automatically on the Learning Disability register – the patient record system creates the register directly from the codes.
There is some concern raised between system leaders within children’s services that the use of a diagnostic process does not identify everyone with a learning disability and that there is a resulting impact upon people’s access to services including a lack of clarity about the terminology used in children’s services, specifically ‘global developmental delay’.
Recommendation: Surrey all-age system leaders need to consider what diagnostic processes are in place and, depending upon the findings, consider if access to services in the future will not be diagnostic dependent.
Recommendation: Surrey all-age system leaders need to consider how best to provide clarity regarding terminology and ensure that necessary differences does lead to poor access or the robustness of intelligence.
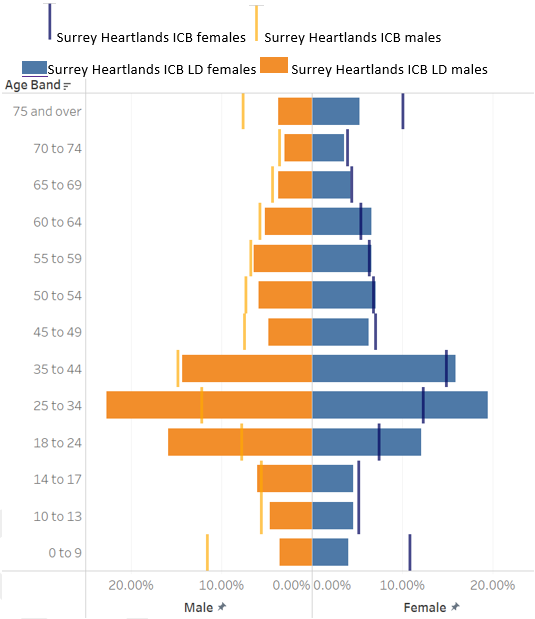
Tables 1 and 2 show the number of children, young people and adults on the learning disability register in Surrey Heartlands and Frimley ICBs respectively. The proportion of males on the disability register is higher than females for both ICBs at 58.4% for Surrey Heartlands and 58.1% for Frimley (higher numbers for males are typical nationally both currently and in recent history).
Reference Learning disability statistics | Foundation for People with Learning Disabilities
Table 1: Surrey Heartlands ICB population with a learning disability on the Learning Disability Register, 2023/24
| Surrey Heartlands ICB | Number Aged <18 | Number Aged 18-24 | Number Aged 25-64 | Number Aged 65-74 | Number Aged 75+ | Number All Ages |
% Aged <18 | % Aged 18-24 | % Aged 25-64 | % Aged 65-74 | % Aged 75+ |
| Persons | 730 | 685 | 2,885 | 325 | 180 | 4,805 | 15.2% | 14.3% | 60.0% | 6.8% | 3.7% |
| Male | 435 | 455 | 1,650 | 175 | 90 | 2,805 | 15.5% | 16.2% | 58.8% | 6.2% | 3.2% |
| Female | 295 | 230 | 1,235 | 150 | 90 | 2,000 | 14.8% | 11.5% | 61.8% | 7.5% | 4.5% |
Table 2: Frimley ICB population with a learning disability on the Learning Disability Register, 2023/24
| Surrey Heartlands ICB | Number aged <18 | Number aged 18-24 | Number aged 25-64 | Number aged 65-74 | Number aged 75+ | Number all ages | % Aged <18 | % Aged 18-24 | % Aged 25-64 | % Aged 65-74 | % Aged 75+ |
| Persons | 705 | 520 | 1,870 | 205 | 85 | 3,385 | 20.8% | 15.4% | 55.2% | 6.1% | 2.5% |
| Male | 440 | 325 | 1,060 | 100 | 40 | 1,965 | 22.4% | 16.5% | 53.9% | 5.1% | 2.0% |
| Female | 265 | 195 | 810 | 105 | 45 | 1,420 | 18.7% | 13.7% | 57.0% | 7.4% | 3.2% |
Figure 1: Frimley ICB population pyramid 2023/24
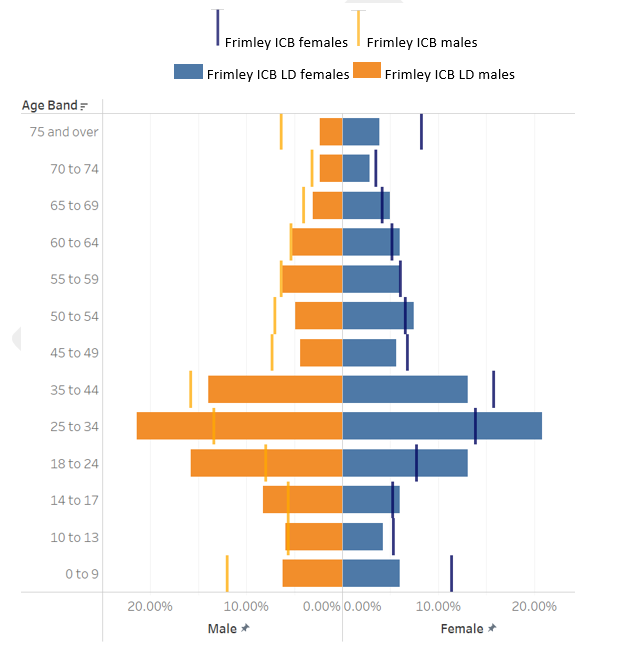
Figure 2 : Surrey Heartlands ICB population pyramid 2023/24
Public Health England ‘Learning Disabilities Observatory People with learning disabilities in England 2015: Main report’ indicated only 23% of adults with learning disabilities in England are identified as such on GP registers and considered this the most comprehensive identification source within health or social services in England. It is estimated that in 2030 approximately 22,500 adults in Surrey will have a learning disability, with only a proportion of this group known to health and social services. Applying the 23% to the overall prevalence rate, we should have 5060 people on the GP register (which is broadly the case) [7].
However, the remaining 77% are often referred to as the ‘hidden majority’ of adults with learning disabilities who typically remain invisible in data collections and in this case, not on a register which would entitle them to an annual health check [8].
Recommendation: To increase the number of people of all ages with a learning disability on the GP Register, paying particular attention to those from minority groups. There is no available breakdown by ethnic group. This is a symptom of a broader lack of routine ethnic monitoring in General Practice that needs to be addressed.
Learning disability population projections
Predictions are based on national prevalence estimates, using an adjusted model to predict population, which takes into account local ethnicity and mortality rates. They should be viewed in the context of advances in medical science which lead a greater number of people having a longer life expectancy from birth.
The estimated number of adults in Surrey aged 18+ with a learning disability is expected to increase by around 10% over time from 23,019 in 2025 to 25,390 in 2045 (Table 3).
Table 3: People in Surrey aged 18+ predicted to have a learning disability by age group, projected to 2045*
| Age group | 2025 | 2030 | 2035 | 2040 | 2045 |
| 18 to 24 | 2,509 | 2,633 | 2,620 | 2,480 | 2,334 |
| 25 to 34 | 3,523 | 3,543 | 3,658 | 3,780 | 3,730 |
| 35 to 44 | 4,245 | 4,346 | 4,415 | 4,487 | 4,624 |
| 45 to 54 | 4,077 | 4,111 | 4,263 | 4,379 | 4,457 |
| 55 to 64 | 3,649 | 3,619 | 3,571 | 3,627 | 3,769 |
| 65 to 74 | 2,456 | 2,746 | 2,948 | 2,941 | 2,912 |
| 75 to 84 | 1,811 | 1,872 | 1,885 | 2,140 | 2,308 |
| 85 and over | 749 | 868 | 1,085 | 1,154 | 1,256 |
| Total | 23,019 | 23,738 | 24,445 | 24,989 | 25,390 |
Source: POPPI and PANSI September 2025 (Data uses POPPI and PANSI national prevalence model applied to the ONS population projections)
The projected increase is lower than nationally, which is estimated as around 7.1% and regionally, which is around 6.9%, over time from 139,808 in 2025 to 149,440 in 2045 (Table 4).
Table 4: People aged 18+ predicted to have a learning disability in England, South East region, Surrey, and local authorities, projected to 2045*
| Local Authority | 2025 | 2030 | 2035 | 2040 | 2045 |
| England | 874,790 | 891,010 | 907,384 | 923,664 | 937,083 |
| South East | 139,808 | 142,388 | 144,928 | 147,440 | 149,440 |
| Surrey | 23,019 | 23,738 | 24,445 | 24,989 | 25,390 |
| Elmbridge | 2,012 | 2,044 | 2,075 | 2,094 | 2,107 |
| Epsom & Ewell | 1,187 | 1,210 | 1,237 | 1,250 | 1,251 |
| Guildford | 2,376 | 2,397 | 2,418 | 2,418 | 2,419 |
| Mole Valley | 1,194 | 1,197 | 1,198 | 1,210 | 1,223 |
| Reigate & Banstead | 2,290 | 2,362 | 2,427 | 2,488 | 2,521 |
| Runnymede | 1,443 | 1,469 | 1,491 | 1,503 | 1,505 |
| Spelthorne | 1,567 | 1,590 | 1,620 | 1,645 | 1,650 |
| Surrey Heath | 1,325 | 1,337 | 1,353 | 1,374 | 1,386 |
| Tandridge | 1,241 | 1,256 | 1,279 | 1,312 | 1,332 |
| Waverley | 1,797 | 1,832 | 1,866 | 1,889 | 1,925 |
| Woking | 1,565 | 1,566 | 1,576 | 1,587 | 1,590 |
Source: POPPI and PANSI September 2025 (Data uses POPPI and PANSI national prevalence model applied to the ONS population projections)
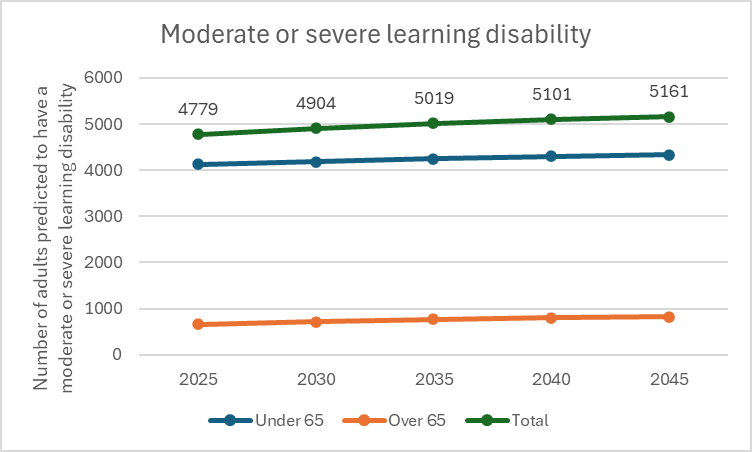
Among the estimated number of adults in Surrey aged 18+ with a learning disability, the number with a moderate or severe learning disability, estimated as 4779 in 2025, is projected to increase to 5,161 by 2045 (Figure 3).
Figure 3 : Estimated number of adults to have a moderate to severe learning disability in Surrey, projected to 2045
Down’s Syndrome
Down’s syndrome and the learning disability register
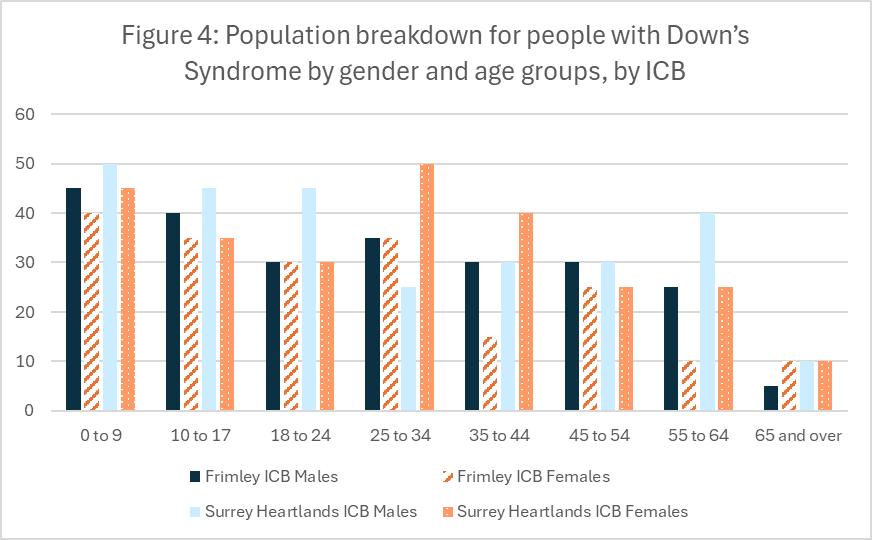
There are 975 children, young people and adults registered on a GP disability register with a diagnosis of Downs syndrome. Approximately 34.3% are children and young people aged under 18 years, 62.1% are adults of working age (18 to 64 years) and 3.5% are 65 years and over. There are slightly more males (52.8%) than females (47.2%). (Figure 4).
Figure 4: Population breakdown for people with Down’s Syndrome by gender and age groups, by ICB
Down’s syndrome projections
Using an adjusted model to predict population which takes into account local ethnicity and mortality rates, it is estimated that in 2025 approximately 514 adults (aged 18+) in Surrey will have Down’s Syndrome.
Table 5: Estimated number of adults with Down’s Syndrome by age group living in Surrey, projected to 2045
| Age Group | 2025 | 2030 | 2035 | 2040 | 2045 |
| 18 to 24 | 85 | 89 | 89 | 84 | 79 |
| 25 to 34 | 102 | 103 | 106 | 110 | 108 |
| 35 to 44 | 104 | 106 | 108 | 110 | 113 |
| 45 to 54 | 136 | 137 | 142 | 146 | 148 |
| 55 to 64 | 69 | 68 | 68 | 69 | 72 |
| 65 and over | 18 | 20 | 21 | 21 | 21 |
| Total | 514 | 523 | 534 | 540 | 541 |
Source: POPPI and PANSI September 2025 (Data uses POPPI and PANSI national prevalence model applied to the ONS population projections)
This number is expected to increase by 5.3% to 541 in 2045 (the estimates for the all individual local authorities in Surrey 2025 are predicted to increase or remain the same by 2040). This increase is in line with national trends where a 7.5% increase is estimated.
Table 6: Estimated number of adults with Down’s Syndrome, in England, South East region, Surrey and local authorities, projected to 2045*
| Local Authority | 2025 | 2030 | 2035 | 2040 | 2045 |
| England | 25,045 | 25,634 | 26,319 | 26,761 | 26,915 |
| South East | 3,992 | 4,088 | 4,132 | 4,262 | 4,285 |
| Surrey | 514 | 523 | 534 | 540 | 541 |
| Elmbridge | 57 | 57 | 59 | 59 | 59 |
| Epsom & Ewell | 34 | 34 | 36 | 35 | 36 |
| Guildford | 70 | 70 | 72 | 70 | 71 |
| Mole Valley | 35 | 34 | 35 | 35 | 35 |
| Reigate & Banstead | 65 | 66 | 70 | 72 | 72 |
| Runnymede | 42 | 43 | 44 | 43 | 42 |
| Spelthorne | 45 | 47 | 47 | 48 | 46 |
| Surrey Heath | 37 | 38 | 39 | 39 | 39 |
| Tandridge | 34 | 37 | 37 | 38 | 37 |
| Waverley | 51 | 53 | 54 | 54 | 56 |
| Woking | 44 | 45 | 46 | 46 | 45 |
Source: POPPI and PANSI September 2025 (Data uses POPPI and PANSI national prevalence model applied to the ONS population projections)
Figure 5: Number of people aged 18+ predicted to have Down’s syndrome by age group, living in Surrey, 2025
Source: POPPI and PANSI September 2025 (Data uses POPPI and PANSI national prevalence model applied to the ONS population projections)
Autism
The Autistica website suggests that around 40% of autistic people have a learning disability, compared with just 1% of people without autism. Around 1 in 10 people with a learning disability are autistic so the two significantly co-occur [9].
Surrey has an All-Age Autism Strategy. A separate chapter of the overall JSNA looking at neurodivergent people including autistic people is being produced.
The Surrey All Age Autism Strategy indicates that it is common for autistic people to have other neurodevelopmental conditions, including learning disabilities (affecting between 15% and 30% of autistic people). Delays in language development are common in autism, and up to 30% of autistic people are non-speaking (completely, temporarily, or in certain contexts).
Using an adjusted model to predict population which takes into account local ethnicity and mortality rates, it is estimated that in 2025 approximately 9,558 adults (aged 18+) in Surrey are Autistic. The estimated number of Autistic people in Surrey aged 18+ is expected to increase by 12% from 2025 to 2045 (10,709).
Table 7: Estimated number of autistic people by age group living in Surrey, projected to 2045
| Age Group | 2025 | 2030 | 2035 | 2040 | 2045 |
| 18 to 24 | 954 | 1,003 | 997 | 945 | 890 |
| 25 to 34 | 1,405 | 1,448 | 1,510 | 1,560 | 1,540 |
| 35 to 44 | 1,658 | 1,703 | 1,760 | 1,823 | 1,895 |
| 45 to 54 | 1,709 | 1,703 | 1,757 | 1,816 | 1,880 |
| 55 to 64 | 1,590 | 1,578 | 1,555 | 1,562 | 1,615 |
| 65 to 74 | 1,101 | 1,232 | 1,312 | 1,308 | 1,294 |
| 75 and over | 1,142 | 1,227 | 1,330 | 1,473 | 1,595 |
Source: POPPI and PANSI September 2025 (Data uses POPPI and PANSI national prevalence model applied to the ONS population projections)
Table 8: Estimated number of autistic adults in England, South East region, Surrey and local authorities, projected to 2045
| Local authority | 2025 | 2030 | 2035 | 2040 | 2045 |
| England | 459,357 | 477,941 | 495,508 | 509,433 | 520,234 |
| South East | 74,917 | 78,054 | 81,006 | 83,422 | 85,373 |
| Surrey | 9,558 | 9,894 | 10,220 | 10,488 | 10,709 |
| Elmbridge | 1,053 | 1,093 | 1,134 | 1,164 | 1,191 |
| Epsom & Ewell | 618 | 634 | 653 | 666 | 682 |
| Guildford | 1,211 | 1,253 | 1,278 | 1,296 | 1,313 |
| Mole Valley | 695 | 718 | 742 | 760 | 774 |
| Reigate & Banstead | 1,202 | 1,263 | 1,320 | 1,362 | 1,395 |
| Runnymede | 725 | 748 | 770 | 788 | 798 |
| Spelthorne | 817 | 843 | 874 | 897 | 918 |
| Surrey Heath | 728 | 751 | 779 | 798 | 817 |
| Tandridge | 679 | 707 | 730 | 754 | 771 |
| Waverley | 1,006 | 1,047 | 1,090 | 1,123 | 1,150 |
| Woking | 820 | 837 | 856 | 875 | 886 |
Source: POPPI and PANSI September 2025 (Data uses POPPI and PANSI national prevalence model applied to the ONS population projections)
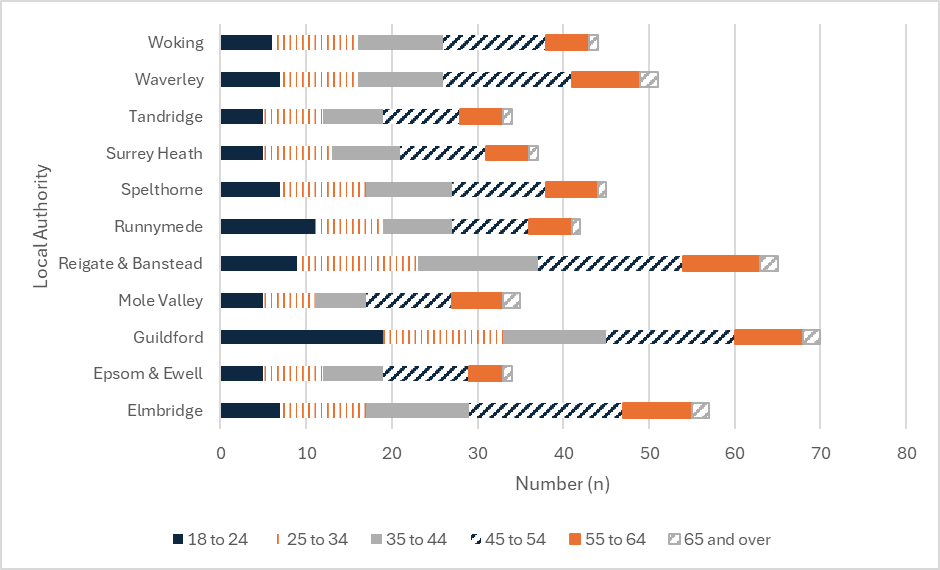
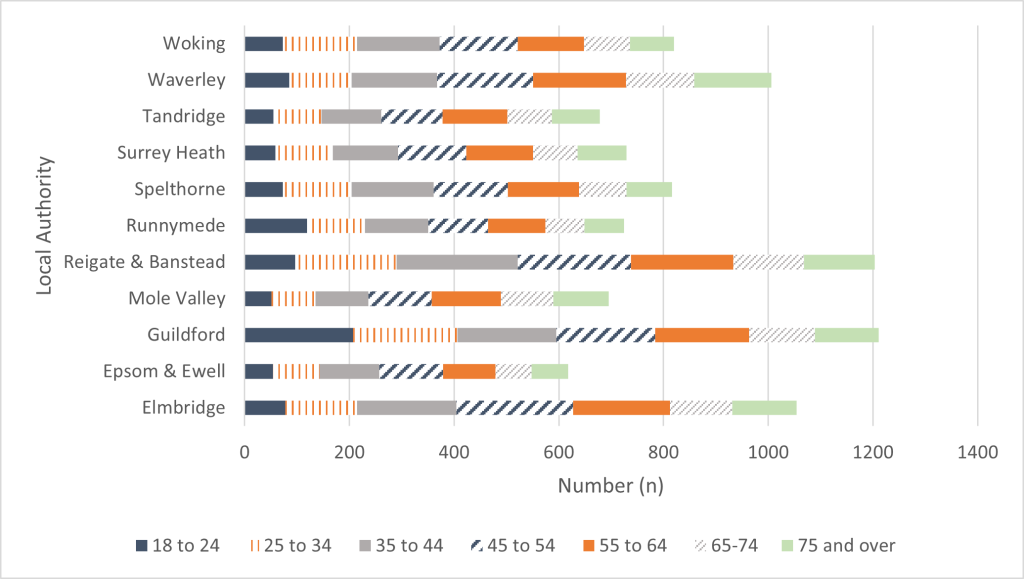
Table 9: Estimated number of autistic people in Surrey aged 18+ by age group and local authority, 2025
| Local Authority | 18 to 24 | 25 to 34 | 35 to 44 | 45 to 54 | 55 to 64 | 65 to 74 | 75 and over | Total |
| England | 51,805 | 79,811 | 78,196 | 71,209 | 73,746 | 54,359 | 50,232 | 459,357 |
| South East | 7,720 | 11,638 | 12,801 | 12,253 | 12,387 | 9,108 | 9,009 | 74,917 |
| Surrey | 954 | 1,405 | 1,658 | 1,709 | 1,590 | 1,101 | 1,142 | 9,558 |
| Elmbridge | 78 | 137 | 189 | 223 | 185 | 119 | 123 | 1,053 |
| Epsom & Ewell | 54 | 89 | 114 | 122 | 100 | 69 | 70 | 618 |
| Guildford | 207 | 199 | 189 | 189 | 180 | 125 | 122 | 1,211 |
| Mole Valley | 51 | 84 | 101 | 121 | 132 | 101 | 105 | 695 |
| Reigate & Banstead | 97 | 193 | 232 | 216 | 195 | 135 | 135 | 1,202 |
| Runnymede | 119 | 111 | 121 | 114 | 109 | 75 | 76 | 725 |
| Spelthorne | 73 | 131 | 157 | 142 | 136 | 90 | 87 | 817 |
| Surrey Heath | 59 | 109 | 125 | 130 | 128 | 85 | 93 | 728 |
| Tandridge | 55 | 92 | 114 | 117 | 124 | 85 | 91 | 679 |
| Waverley | 85 | 119 | 164 | 183 | 177 | 131 | 147 | 1,006 |
| Woking | 73 | 142 | 157 | 150 | 126 | 88 | 84 | 820 |
Source: POPPI and PANSI September 2025 (Data uses POPPI and PANSI national prevalence model applied to the ONS population projections)
Figure 6: Estimated number of autistic people aged 18+ by age group, living in Surrey, 2025
Epilepsy
The prevalence rate of epilepsy amongst people with learning disabilities is estimated to be 22%, compared to prevalence rates for the general population of 0.4% to 1%. There was no available data about the numbers of people with learning disability and those without learning disability across Surrey who have epilepsy.
However, there is data about the numbers of people with and without a learning disability who are currently on drug treatment for their epilepsy. Seizures are commonly multiple and resistant to drug treatment. Uncontrolled epilepsy can have serious negative consequences on both quality of life and the life span, although guidelines on the successful management of epilepsy in people with learning disabilities are available [10].
Table 10: Percentage of patients with an active diagnosis of epilepsy currently on drug treatment for epilepsy, as at 31 March, by year
| Year | Surrey Heartlands ICB with learning disability | Surrey Heartlands ICB without learning disability | Frimley ICB with learning disability | Frimley ICB without learning disability |
| 2019/20 | 17.90% | 0.50% | 16.60% | 0.50% |
| 2020/21 | 18.00% | 0.50% | 17.40% | 0.50% |
| 2021/22 | 18.42% | 0.51% | 17.40% | 0.52% |
| 2022/23 | 18.63% | 0.51% | 17.77% | 0.53% |
| 2023/24 | 18.22% | 0.49% | 17.22% | 0.52% |
Source: Health and Care of People with Learning Disabilities, Experimental Statistics 2023 to 2024- NHS England Digital
In Surrey Heartlands ICB, there has been little change in the percentage of the general population who have a learning disability and epilepsy and who are on drug treatment for epilepsy between 2019 and 2024. Frimley ICB shows a slight percentage increase from 2019 to 2024 but at 17.22% remains lower than Surrey Heartlands at 18.22%. The data shows that a much greater percentage of epileptic people with LD need drugs to control the epilepsy than those without LD.
Learning Disability and challenging behaviours
Challenging behaviours can be defined as:
‘Culturally abnormal behaviour(s) of such an intensity, frequency or duration that the physical safety of the person or others is likely to be placed in serious jeopardy, or behaviour which is likely to seriously limit use of, or result in the person being denied access to, ordinary community facilities.’ [11]
‘Behaviour can be described as challenging when it is of such an intensity, frequency, or duration as to threaten the quality of life and/or the physical safety of the individual or others and it is likely to lead to responses that are restrictive, aversive or result in exclusion.’ [12]
They may also be referred to as distressed behaviour or ‘behaviours of concern’.
Using an adjusted model to predict population which considers population projections, local ethnicity and mortality rates, it is estimated that in 2025 approximately 333 adults (18 to 64 years) in Surrey will present challenging behaviour and that this number of is expected to increase steadily to 2045. The projections from PANSI use a prevalence rate of 0.045% of the population aged 5 and over for people with a learning disability displaying challenging behaviour [3]. However, NICE guideline 2015 cite a higher prevalence quoting:
‘It is relatively common for people with a learning disability to develop behaviour that challenges, and more common for people with more severe disability. Prevalence rates are around 5 to 15% in educational, health or social care services for people with a learning disability. Rates are higher in teenagers and people in their early 20s, and in particular settings (for example, 30 to 40% in hospital settings). People with a learning disability who also have communication difficulties, autism, sensory impairments, sensory processing difficulties and physical or mental health problems (including dementia) may be more likely to develop behaviour that challenges.’ [13]
As such the projections in Tables 11 and 12 may be an underestimation and local intelligence indicates a rate more aligned with NICE guidance.
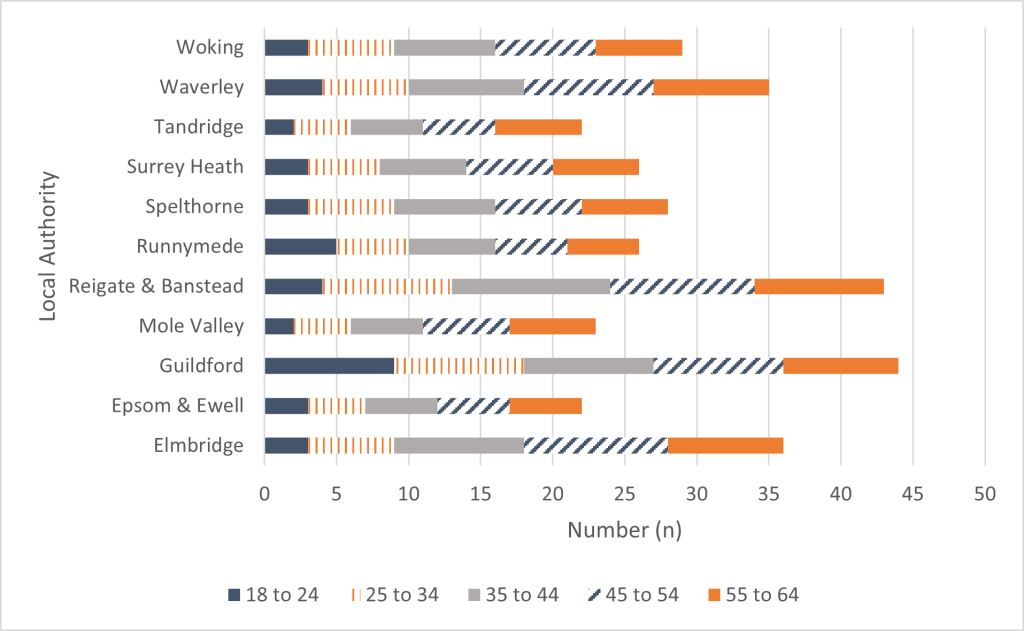
Table 11: Estimated number of people in Surrey aged 18 to 64 with challenging behaviour by age group living, projected to 2045
| Age Group | 2025 | 2030 | 2035 | 2040 | 2045 |
| 18 to 24 | 42 | 44 | 44 | 41 | 39 |
| 25 to 34 | 64 | 64 | 66 | 68 | 67 |
| 35 to 44 | 77 | 79 | 81 | 82 | 84 |
| 45 to 54 | 78 | 79 | 82 | 84 | 85 |
| 55 to 64 | 72 | 72 | 71 | 72 | 75 |
| Total | 333 | 338 | 343 | 347 | 351 |
Source: POPPI and PANSI September 2025 (Data uses POPPI and PANSI national prevalence model applied to the ONS population projections)
Table 12: Estimated number of people with challenging behaviour in England, South East region, Surrey and local authorities, projected to 2040
| Area | 2025 | 2030 | 2035 | 2040 | 2045 |
| England | 16,133 | 16,421 | 16,717 | 17,035 | 17,318 |
| South East | 2,586 | 2,632 | 2,678 | 2,728 | 2,770 |
| Surrey | 333 | 338 | 343 | 347 | 351 |
| Elmbridge | 37 | 38 | 39 | 39 | 39 |
| Epsom & Ewell | 22 | 22 | 23 | 23 | 23 |
| Guildford | 43 | 44 | 44 | 44 | 44 |
| Mole Valley | 22 | 22 | 22 | 23 | 23 |
| Reigate & Banstead | 42 | 44 | 45 | 46 | 47 |
| Runnymede | 26 | 27 | 27 | 28 | 28 |
| Spelthorne | 29 | 29 | 30 | 30 | 31 |
| Surrey Heath | 25 | 25 | 25 | 26 | 26 |
| Tandridge | 23 | 23 | 24 | 24 | 25 |
| Waverley | 33 | 34 | 35 | 35 | 36 |
| Woking | 29 | 29 | 29 | 29 | 29 |
Source: POPPI and PANSI September 2025 (Data uses POPPI and PANSI national prevalence model applied to the ONS population projections)
Figure 7: Estimated number of people aged 18 to 64 with challenging behaviour by age group, living in Surrey, 2025
Recommendation: Given that the predicted rate is likely to be lower than the actual rate, the numbers of people presenting with challenging / distressed behaviours and behaviours of concern will need to be kept under review including via the dynamic support register.
Those who exhibit challenging behaviour are at risk of inpatient admissions. Please see the section on this later in the chapter.
Underrepresented communities and intersectionality
Gypsy, Roma and Traveller (GRT) Community
As noted above, the collection of ethnic origin data across the system is poor. The 2021-2024 Surrey Heartlands Strategy includes reference to how Surrey Heartlands will reduce health inequalities faced by people from Black, Asian and Minority Ethnic backgrounds who have a learning disability, as highlighted in LeDeR reviews.
While the ‘GRT community’ label includes groups from a range of distinct ethnicities, they are often reported together as they are believed to face similar challenges. There is data collated against the Autism Strategy which includes ‘White: Gypsy or Irish Traveller’ as a category, however this does not reflect the multiple categories newly referenced in the 2021 England and Wales census, which included more distinct group categories for the first time, including Roma. The collection of data will need to be developed for people with a learning disability and should appropriately reflect the distinctions within the GRT community. Until this time, it is important to note the census caveats of a likely substantial undercount against research statistics (drawn from bi-annual Traveller caravan count and school roll figures) [14] [15].
The Friends, Families and Travellers organisation completed research together with Amaze, an organisation which gives information, advice and support to families with disabled children and young people. Data was collected through a focus group and an online survey to discover more about awareness of learning disabilities in Gypsy and Traveller communities and to find out how community members would like to receive information on learning disabilities. Using focus groups and online surveys they found that face to face support was preferable [16].
Recommendation: Data on all underrepresented groups within Surrey will need to be gathered including the GRT community using the more distinct categories for these communities that are under development. This data can then be used to consider raising awareness and offering support to members of under-represented communities with a learning disability.
Sexual Orientation
The Mencap website states that it is important to recognise that people with a learning disability can be lesbian, gay, bisexual and transgender.
People with learning disabilities experience many barriers that prevent them from expressing their sexuality and developing loving and sexual relationships, particularly if they identify as lesbian, gay, bisexual and trans (LGBT) [17][18].
The 2021 census in England and Wales is the first census that has asked people about their sexual orientation. Around 3.6 million people (7.5%) did not answer the census question. Respondents were able to select from options including heterosexual, gay, lesbian and bisexual. 2.9 million (6.0%) chose not to disclose their gender identity. 1.5% responded that their sexual orientation was gay or lesbian, 1.3% bisexual and 0.3% ‘all other sexual orientations’.
For people with a learning disability, applying the percentages above to the prevalence rate of people with learning disabilities of 23,019 in 2025 this may indicate there are potentially:
- 345 who are gay or lesbian
- 299 who are bisexual
However, given the presence of significant gaps in response (7.5% no answer, 6% not answering), these estimations should be treated with caution and further data sought as per the wider recommendation about underrepresented groups.
For people with a learning disability who are also autistic, it is worth noting that recent studies are finding that autistic individuals are less likely to identify as heterosexual and more likely to identify with a diverse range of sexual orientations than non-autistic individuals [19].
Gender Identity
The 2021 census in England and Wales is the first census that has asked people about their gender identity. Respondents were also asked whether their gender identity matched their sex registered at birth. Those who selected “no” were asked to fill in a text box describing their gender identity.
93.5% of respondents said they identified the same as their sex at birth, 0.5% said they didn’t and 6% didn’t answer.
For people with a learning disability, applying the 0.5% above to the prevalence rate of people with learning disabilities of 23,019 in 2025 this may indicate there are 115 people with a learning disability within Surrey that do not identify with the same sex at birth.
Recent research indicates that lesbian, gay, bisexual, transgender, queer (LGBTQ) and gender diverse adults with intellectual disability experience exclusion within disability services [20]
Recommendation: Data to be gathered within Surrey and consideration given to understanding the numbers and experiences of people with a learning disability identifying as LGBGTQ+ in order to ensure barriers to expression are tackled and equity of access to services and support.
Life expectancy
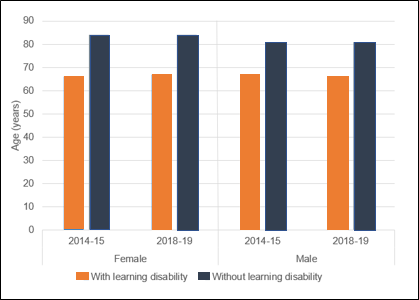
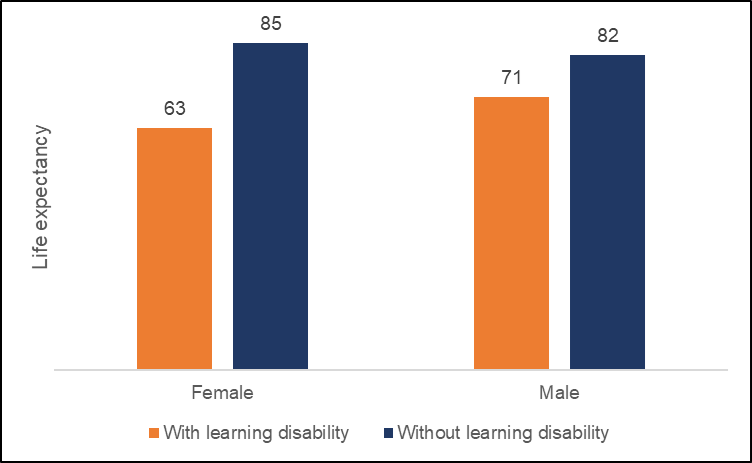
National data for life expectancy shows that in 2018/19, males with a learning disability had a life expectancy at birth of 66 years. This is 14 years lower than for males in the general population. Similarly, females with a learning disability have a life expectancy of 67 years, which is 17 years lower than for females in the general population. There has been no statistically significant change in life expectancy for people with a learning disability between 2014/15 and 2018/19 [21].
Figure 8: Life expectancy for males and females with and without a learning disability, for 2014/15 to 2018/19 – England
The Surrey Heartlands’ LeDeR Annual Report 2021, showed a greater disparity for females, women with learning disabilities dying 22 years sooner than the general population. For males the disparity is reduced compared with the national picture, men with learning disabilities dying 11 years sooner than the general population (Figure 9).
The LeDeR programme (Learning from Lives and Deaths) is the national review programme which reviews the deaths of people with learning disabilities and autism across England. It started in 2018 and aims to support local areas to review the deaths of people with learning disabilities (aged four years and above) and autistic people (aged 18 years old and over), identify learning from those deaths, and ensure services are developed in order to address any learning from the review.
Figure 9: Life expectancy in Surrey, 2020/21
The Surrey Heartlands LeDeR Annual Report includes the deaths of children with learning disabilities.
In 2021/22
- There was a total of 3 deaths
- The range of age at death was 12 to 14
- The mean average age of death was 13
- The median average age was 13
In 2022/23:
- There was a total of 7 deaths
- The range of age at death was 4 to 17
- The mean average age of death was 11
- The median average age was 1
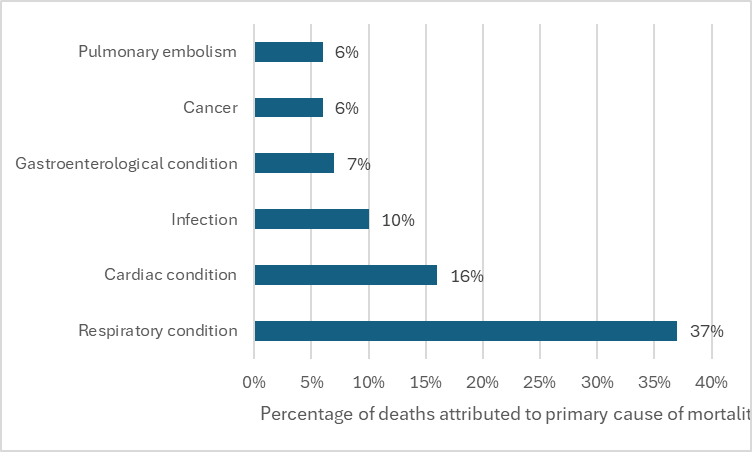
LeDeR has found that as well as dying earlier than people who don’t have learning disabilities, people with learning disabilities are three times more likely to die from an avoidable cause (University of Bristol, 2019) [22]. The 2020 national LeDeR Annual Report identifies that the four most common causes of mortality amongst people with learning disabilities are:
- Respiratory disorders
- Circulatory disorders
- Chromosomal disorders
- Neoplasms
Similarly in Surrey, people with learning disabilities die most commonly from respiratory, circulatory conditions, and infections, in order of magnitude – when grouped according to these categories, the mortality profile in Surrey (Figure 10) broadly corresponds to this national picture.
Figure 10: Causes of mortality amongst people with learning disability in Surrey (2022/23)
The national LeDeR policy outlined local delivery expectations required from each Integrated Care System (ICS). One of these is to have a three-year LeDeR strategy demonstrating how Surrey Heartlands will act strategically to tackle the areas of health inequality experienced by people with a learning disability and autistic people. The areas of the 2021-2024 Surrey Heartlands Strategy have been identified through the thematic learning from LeDeR reviews and include reference to how Surrey Heartlands will reduce health inequalities faced by people from Black, Asian and Minority Ethnic backgrounds who have a learning disability. The Frimley LeDeR strategy is in draft and as such is not included.
Social care
Number of children with a learning disability open to social care
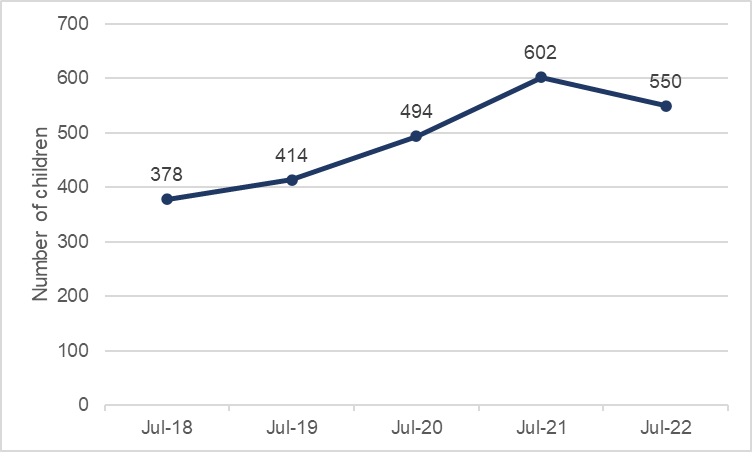
As of 24 October 2022, there were 1,376 children (under 18 years) who have an Education, Health and Care Plan (EHCP) and social care involvement. Of these, 503 (or 36.5%) have a recorded learning disability.
The number of children who are open to social care and have a recorded learning disability as at 30 July each year from 2018 is shown in Figure 11. There has been an overall increase of 45% during this period, although the number in 2022 was a decrease from 2021. Most referrals related to Learning Disability, which covers a wide spectrum of need, are generated by schools based on their assessment of pupil’s emerging needs. There has been a corresponding increase in the number of requests for EHCP’s as a way of addressing this need. The drop in referrals in 2022 may be as a result of the 2021/2022 Academic year being affected by the period of Covid lockdown and a consequent decrease in early identification and referral but further audit activity would be required for conclusive reasons.
It is of note that disability types are rarely recorded on children’s education records, so the data is drawn from the disability type recorded on social care records, though this recording is still variable.
Figure 11: The number of children with a learning disability open to social care 2018 to 2022
Surrey’s Children and Young People with Additional Needs and Disabilities Joint Strategic Needs Assessment 2022 contains significant data and insight into transitioning from being a child into an adult including the in detail in the ‘preparing for adulthood’ section (slides 115-120) and also throughout the document (Children and young people with Additional Needs | Surrey-i (surreyi.gov.uk)).
Number of adults with a learning disability open to social care
The number of people open to Adult Social Care (ASC) in Surrey with a Primary Support Reason (PSR) or Primary Client Category (PCC) of Learning Disability is 4,442. The Primary Support Reason is a national indicator that shows what social care an individual is provided with, while Primary Client Category is the main reason a person is known to Adult Social Care.
The data is broken down into geography (district and boroughs), those living at home with family carers, age, gender and ethnicity.
The largest proportion of people who have learning disability and/or autism (LDA) open to ASC live in Reigate and Banstead (14.9%) or are based out of county (OOC) (12.7%), where address is known. The high portion of people with a learning disability in Reigate and Banstead can be attributed to the closure of the long stay hospitals in the 1990s including Manor Park, St Ebbas and Westfield Park which resulted in a number of residential and community homes being established in the area.
Table 13: The number of people aged 18 or over open to Adult Social Care in Surrey with a PSR or PCC of Learning Disability by District & Boroughs (excluding unknown addresses)
| D&B or OOC | Count | % ASC LDA customers |
| Elmbridge | 301 | 6.8% |
| Epsom & Ewell | 259 | 5.8% |
| Guildford | 422 | 9.5% |
| Mole Valley | 303 | 6.8% |
| Reigate & Banstead | 661 | 14.9% |
| Runnymede | 253 | 5.7% |
| Spelthorne | 279 | 6.3% |
| Surrey Heath | 281 | 6.3% |
| Tandridge | 303 | 6.8% |
| Waverley | 479 | 10.8% |
| Woking | 336 | 7.6% |
| Outside Surrey | 565 | 12.7% |
| Total | 4,442 | 100% |
PSR = primary care support, PCC = primary care category
Numbers or totals may have been slightly altered to avoid disclosure on this or other tables
The number of people living at home with family carers
Adult Social Care are currently refreshing the Short Breaks offer. Data has been selected using the following criteria:
- Individuals open to ASC with a Primary Support Reason or Primary Client Category of LD, which includes people on the Autism Spectrum, regardless of whether they have a learning disability
- Accommodation Status set to ‘Settled mainstream housing with family/friends’ or ‘Living with Parents’ (excludes people with a current costed service of Residential, Nursing or Supported Living)
- Carers identified by those recorded as Main Carer
- Living in Surrey
It shows that there are 1,345 individuals over 18 years who are living at home with family carers. Of these, 268 are in East Surrey, 296 in Mid Surrey, 304 in South West Surrey and 477 in North West (October 2021).
Ethnicity
Table 14: The number of people open to Adult Social Care in Surrey with a PSR or PCC of Learning Disability by District & Boroughs (excluding unknown addresses) and by ethnicity (excluding undeclared or not known)
| D&B | Asian/ Asian British | Black/ African/ Caribbean/ Black British | Mixed/ multiple ethnic groups | Other ethnic group | White |
| Elmbridge | 20 | 5 | 10 | 10 | 260 |
| Epsom & Ewell | 20 | 10 | 10 | 5 | 220 |
| Guildford | 15 | 5 | 15 | 10 | 375 |
| Mole Valley | 5 | 5 | 15 | 5 | 285 |
| Reigate & Banstead | 25 | 15 | 30 | 10 | 580 |
| Runnymede | 5 | 5 | 15 | 5 | 235 |
| Spelthorne | 20 | 5 | 10 | 10 | 235 |
| Surrey Heath | 15 | 5 | 10 | 5 | 245 |
| Tandridge | 10 | 10 | 10 | 5 | 270 |
| Waverley | 15 | 5 | 20 | 5 | 435 |
| Woking | 55 | 5 | 15 | 5 | 265 |
| Outside Surrey | 10 | 15 | 15 | 10 | 525 |
PSR = primary care support, PCC = primary care category
Numbers all rounded up to nearest 5 above to ensure anonymity while ensuring all groups present in the data are represented
Table 15: The percentage of people open to Adult Social Care (ASC) in Surrey with a PSR or PCC of Learning Disability by District & Boroughs, excluding unknown addresses, by Ethnicity, excluding undeclared or not known compared with the general population (Pop) ethnicity
| D&B or OOC | Asian / Asian British (ASC) | Black / African / Caribbean / Black British (ASC) | Mixed / multiple ethnic groups (ASC) | Other ethnic group (ASC) | White (ASC) | Asian / Asian British (Pop) | Black / African / Caribbean / Black British (Pop) | Mixed / multiple ethnic groups (Pop) |
Other ethnic group (Pop) | White (Pop) |
| Elmbridge | 6.6% | 1.6% | 3.3% | 3.3% | 85.2% | 6.5% | 1.2% | 4.1% | 2.0% | 86.1% |
| Epsom & Ewell | 7.5% | 3.8% | 3.8% | 1.9% | 83.0% | 11.4% | 1.9% | 4.4% | 2.8% | 79.5% |
| Guildford | 3.6% | 1.2% | 3.6% | 2.4% | 89.3% | 6.7% | 1.5% | 3.1% | 1.9% | 86.9% |
| Mole Valley | 1.6% | 1.6% | 4.8% | 1.6% | 90.5% | 3.0% | 0.8% | 2.5% | 0.9% | 92.7% |
| Reigate & Banstead | 3.8% | 2.3% | 4.5% | 1.5% | 87.9% | 7.5% | 2.9% | 3.7% | 1.4% | 84.4% |
| Runnymede | 1.9% | 1.9% | 5.7% | 1.9% | 88.7% | 9.2% | 1,8% | 3.5% | 1.9% | 83.5% |
| Spelthorne | 7.1% | 1.8% | 3.6% | 3.6% | 83.9% | 12.8% | 2.5% | 3.7% | 2.4% | 78.7% |
| Surrey Heath | 5.4% | 1.8% | 3.6% | 1.8% | 87.5% | 8.9% | 1.6% | 2.7% | 1.8% | 85.0% |
| Tandridge | 3.3% | 3.3% | 3.3% | 1.6% | 88.5% | 3.7% | 2.2% | 3.8% | 0.9% | 89.4% |
| Waverley | 3.1% | 1.0% | 4.2% | 1.0% | 90.6% | 2.8% | 0.7% | 2.2% | 0.6% | 93.7% |
| Woking | 15.9% | 1.4% | 4.3% | 1.4% | 76.8% | 14.2% | 1.8% | 3.5% | 2.1% | 78.4% |
| OOC | 1.7% | 2.6% | 2.6% | 1.7% | 91.3% | – | – | – | – | – |
Source: SCC Adult Social Care, Nov 25 and Census 2021 data.
Numbers all rounded up to nearest 5 above to ensure anonymity while ensuring all groups present in the data are represented
The Race Equality Foundation indicated that available data does not give a definitive answer as to how many people with learning disabilities are from BAME communities which may cause difficulty in ascertaining the exact numbers of People of Colour who are reported in the statistics. [23]
According to Lancaster University’s Centre for Disability Research, between 2011 and 2020, 25% of new entrants to adult social care with learning disabilities were from minority ethnic communities. Higher rates of identification of more severe forms of intellectual disability are recorded among children of Pakistani and Bangladeshi heritage. [24] [25] Below shows the percentages of individuals with an ethnicity of Asian/Asian British Pakistani or Asian/Asian British Bangladeshi open to Adult Social Care and shows percentage increases except for 2021.
Table 16: Individuals with an ethnicity of Asian/Asian British Pakistani or Asian/Asian British Bangladeshi open to ASC as a % of all individuals open to ASC with an Ethnicity of Arab, Asian/Asian British, Black/Black British and Chinese (PSR or PCC of Learning Disability and excluding unknown addresses)
| Year | Percentage |
| 2019 | 25% |
| 2020 | 28.3% |
| 2021 | 27.4% |
| 2022 | 29.1% |
| 2023 | 27.7% |
| 2024 | 29% |
| 2025 | 27.8% |
Source: SCC Adult Social Care, November 25 data as at 1st September each year
In Surrey between 2019 and 2025 the number of entrants of those with an ethnicity of Asian/Asian British Pakistani or Asian/Asian British Bangladeshi increased by74.0%, with the predominant increases occurring between 2019 and 2020 and 2023 and 2024.
Recommendation: Seek to understand this increase, including if the higher rates of identification of more severe forms of intellectual disability are recorded among children of Pakistani and Bangladeshi heritage.
Recommendation: Ensure commissioning strategies and services are able to meet cultural needs, working with the VCSE (including Surrey Minority Ethic Forum).
Age
Table 17: The number of people open to Adult Social Care in Surrey with a PSR PCC of learning disability by district and boroughs, excluding unknown addresses, by age group
| D&B or OOC | 18 to 29 | 30 to 39 | 40 to 49 | 50 to 59 | 60 to 69 | 70 and over |
| Elmbridge | 133 | 49 | 27 | 42 | 31 | 19 |
| Epsom & Ewell | 96 | 39 | 27 | 26 | 37 | 34 |
| Guildford | 185 | 91 | 45 | 50 | 35 | 16 |
| Mole Valley | 112 | 65 | 33 | 37 | 33 | 23 |
| Reigate & Banstead | 222 | 160 | 82 | 82 | 63 | 52 |
| Runnymede | 85 | 45 | 28 | 36 | 32 | 27 |
| Spelthorne | 117 | 50 | 46 | 33 | 27 | 6 |
| Surrey Heath | 105 | 72 | 34 | 22 | 30 | 18 |
| Tandridge | 120 | 60 | 32 | 45 | 30 | 16 |
| Waverley | 165 | 103 | 57 | 58 | 62 | 34 |
| Woking | 147 | 73 | 46 | 29 | 25 | 16 |
| Outside Surrey | 96 | 131 | 86 | 95 | 102 | 55 |
| Total | 1,582 | 937 | 543 | 555 | 507 | 316 |
| % | 35.6% | 21.1% | 12.2% | 12.5% | 11.4% | 7.1% |
PSR = primary care support, PCC = primary care category
Numbers or totals may have been slightly altered to avoid disclosure on this or other tables
Gender (The issues discussed in the section on Page 25 relating to ‘gender identity’ relate.)
Consistent with the disability registers discussed above, social care data shows that there are more males than females with a learning disability. This is true in each of eleven district and borough Local Authority areas.
Table 18: The number of people open to Adult Social Care in Surrey with a PSR or PCC of Learning Disability by District & Boroughs, excluding unknown addresses, by gender
| D&B or OOC | Female | Male | Other or unknown |
| Elmbridge | 111 | 188 | * |
| Epsom & Ewell | 94 | 164 | * |
| Guildford | 174 | 245 | * |
| Mole Valley | 134 | 167 | * |
| Reigate & Banstead | 243 | 417 | * |
| Runnymede | 96 | 157 | * |
| Spelthorne | 107 | 172 | * |
| Surrey Heath | 116 | 163 | * |
| Tandridge | 116 | 186 | * |
| Waverley | 207 | 272 | * |
| Woking | 125 | 208 | * |
| Outside Surrey | 227 | 338 | * |
| Grand Total | 1,750 | 2,677 | 15 |
| Total percentage | 39.5% | 60.5% | 0.3% |
PSR = primary care support, PCC = primary care category
*Gender other or unknown unable to be broken down further due to small numbers recorded in each District and Borough
Numbers or totals may have been slightly altered to avoid disclosure on this or other tables
Figure 12: The number of people open to Adult Social Care in Surrey with a PSR or PCC of Learning Disability by age group and gender, excluding unknown addresses
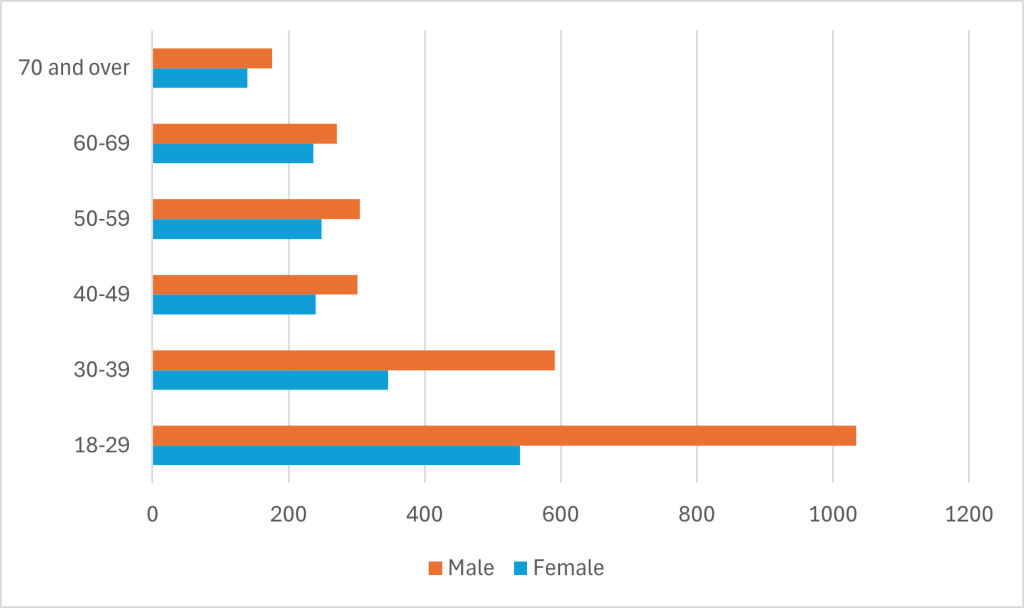
Source: SCC Adult Social Care, November 25
Note: Data on those whose gender is “Other or Unknown” is available for the 18-29 age group (9 people) and for the 30-39 age group (6 people)
Safeguarding
Referrals to adult safeguarding have increased over time for people aged 18 and over with learning disabilities. The rate of individuals referred has gone from 36.8 per 1,000 people on the GP learning disability register in 2015/16 to 80.1 per 1,000 in 2018/19.
Figure 13: Individuals with learning disabilities involved in Section 42 safeguarding enquiries, trends over time 2015/16 to 2018/19
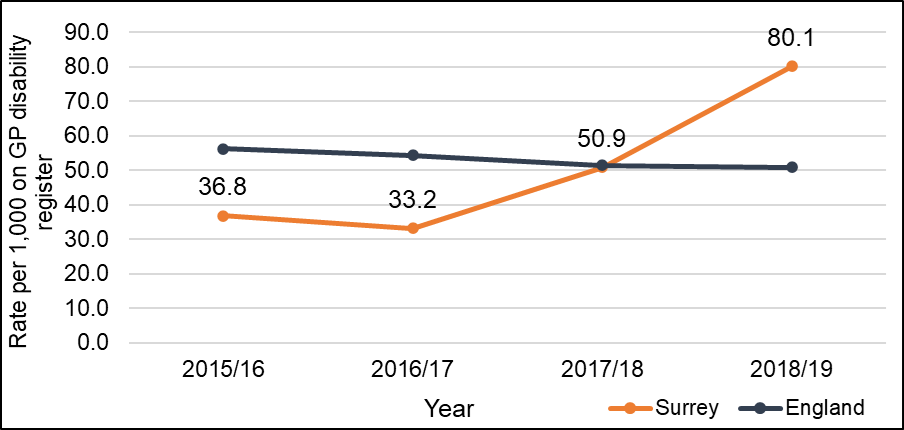
This increase reflects a change in policy regarding safeguarding reporting. All parties are now encouraged to report all concerns in order that they can be properly assessed, and no issue missed. Further analysis is underway to understand how the safeguarding data is used, including benchmarking and how the learning informs preventative initiatives.
Recommendation: Safeguarding data needs routinely to be benchmarked, themes from enquiries highlighted and preventative action undertaken.
Education
The number of those receiving special educational needs (SEN) support in state-funded nursery, primary, secondary and specialist schools, non- maintained specialist schools, pupil referral unit and independent schools in Surrey was 29,971 (14.7%) in 2024/25 [26]. In January 2025 16,069 had an Education, Health and Care Plan (EHCP). [25]
Primary need
The prevalence of learning difficulties in schools will give an insight into the prevalence and the future need in the population.
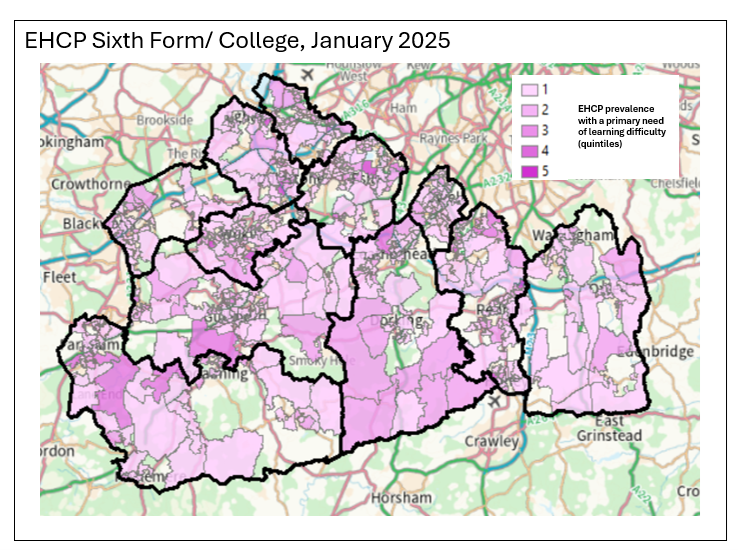
Map 1: The primary need for all pupils, all ages with a learning difficulty, 2025
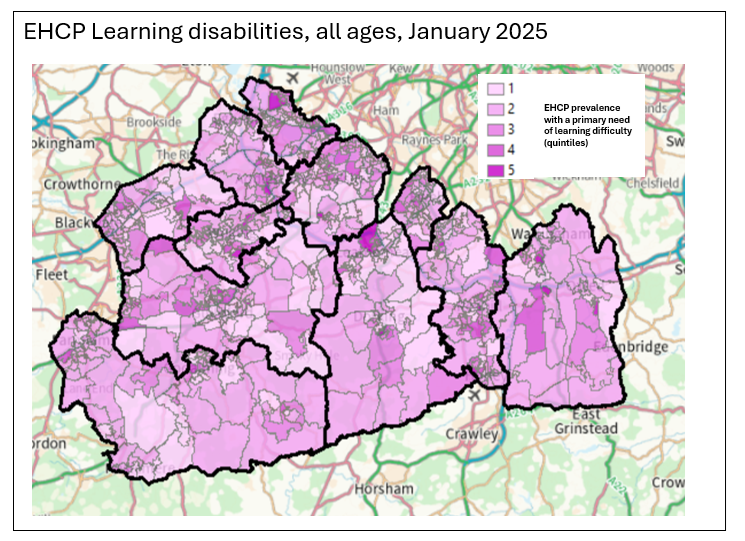
Table 19 shows the primary need for SEN support is moderate learning difficulty (13.9%), followed by specific learning difficulty (4.3%).
Table 19: Primary need of pupils identified with special educational need in Surrey maintained and academies schools, learning difficulty specific, 2021
| Primary Care Need | Total Early Years (Nursery School) | Total Primary School | Total Secondary School | Total Sixth Form/College | Total percentage of all needs |
| Moderate learning difficulty | 20 | 613 | 1,009 | 616 | 13.9% |
| Profound and multiple learning difficulty | 8 | 31 | 39 | 41 | 0.7% |
| Severe learning difficulty | 9 | 231 | 165 | 192 | 3.7% |
| Specific learning difficulty | 6 | 129 | 349 | 205 | 4.3% |
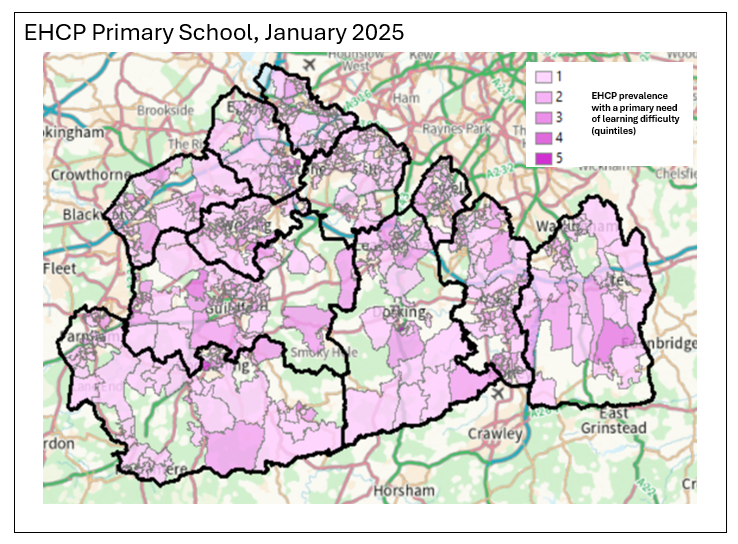
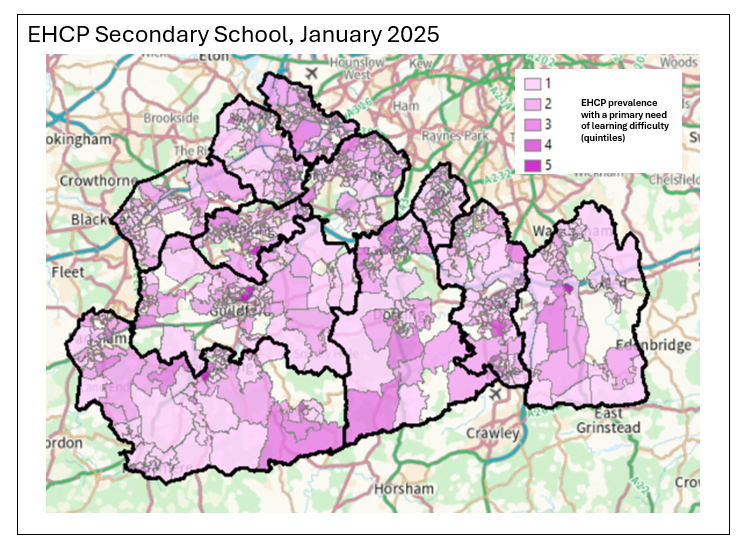
Maps 2 to 4 shows the pupil data grouped into deciles (1-10) to identify the largest population counts of primary, secondary and college/sixth form school pupils with an EHCP.
Map 2: The number of primary school children with a primary need of learning difficulty by LSOA, 2025
Map 3: The number of secondary school children with a primary need of learning difficulty by LSOA, 2025
Map 4: The number of sixth form or college school children with a primary need of learning difficulty by LSOA, 2025
Prevalence of behaviour risk factors
The Health and well Being Strategy for Surrey includes in Priority 1 the following ambition:
‘Supporting people to lead healthy lives by preventing physical ill health and promoting physical well-being’
The outcomes include ‘supporting prevention and reduce substance misuse, including alcohol misuse, alcohol related harm and smoking’. Out of three behavioural markers (drug use, heavy drinking and smoking), only smoking produced significant data [6].
Smoking rate
Surrey Heartlands commissioned an analysis and report (from the PSC) during 2022 to understand the health inequalities experienced by people with learning disabilities (funded by Public Health in Surrey County Council). The report offered insight into the smoking behaviour of people with a learning disability on the GP register and the primary care offer in terms of lifestyle interventions using data extracted by EMIS from primary care settings across Surrey.
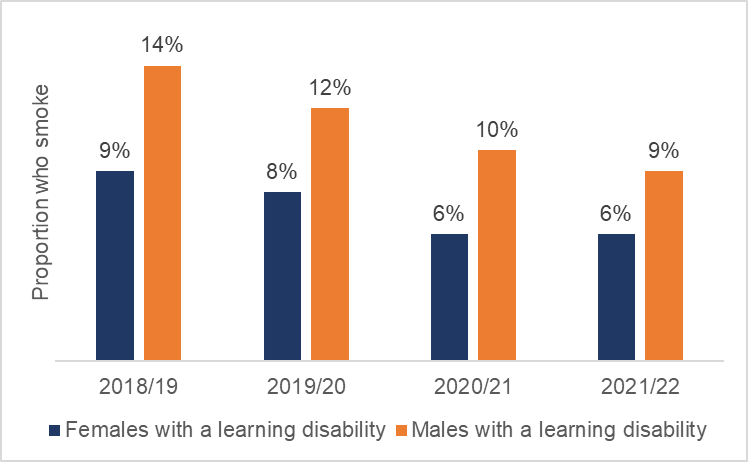
Data from 2021/22 showed that men with a learning disability were 48% more likely than women with a learning disability to be smokers, and this increased likelihood is observed at a similar level in each of the three previous years also. The overall proportion of people with a learning disability on the GP register who smoked was 8% in 2021/22 the same as the previous year [27].
Figure 14: Proportion of males and females with a learning disability who smoke in Surrey, 2018/19 to 2021/22
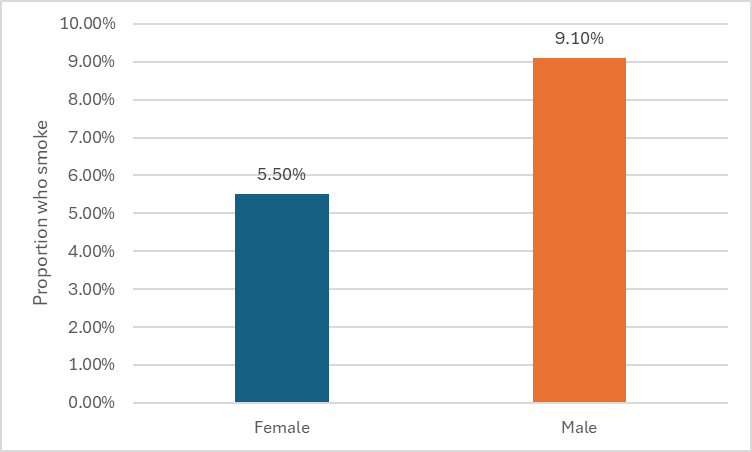
In Surrey, the prevalence of smoking in all adults aged 18 and over was 10.3% in 2020 [28], this is higher than the 8% for those with a learning disability for a similar time period (2020/21). When split by gender, the trend seen in those with learning disabilities is also seen in all adults, with males more likely to be smokers than females.
Figure 15: Prevalence of adults aged 18 and over who smoke in Surrey by gender, 2023
Recommendation: Ensure smoking cessation support is reasonably adjusted to meet the needs of people with a learning disability and that targeted support is offered in North West place.
Advocacy support
Under the Care Act 2014, local authorities must involve people in decisions made about them and their care and support. No matter how complex a person’s needs, local authorities are required to help people express their wishes and feelings, support them in assessing their options, and assist them in making their own decisions. The advocacy duty applies from the point of first contact with the local authority and at any subsequent stage of the assessment, planning, care review, safeguarding enquiry or safeguarding adult review. Advocacy is a statutory service, that supports vulnerable people to:
- access information and services
- be involved in decisions about their lives
- explore choices and options
- defend and promote their rights and responsibilities
- speak out about issues that matter to them
Surrey County Council deliver advocacy services via two separate contracts to meet a variety of statutory legislative requirements.
Adult Non-Instructed Advocacy
This is advocacy for adults unable to instruct an advocate as they (temporarily or permanently) lack mental capacity, subject to the Mental Capacity Act, and Deprivation of Liberty Safeguards (DoLS). This also applies to subjects of the Care Act 2014 who lack capacity to instruct an advocate but might not meet MCA/DoLS criteria.
This contract is a cost and volume contract spot commissioned and funded directly by the Deprivation of Liberty Safeguards (DoLS) team on a spot commissioned case by case basis rather than block commissioned as the Adults instructed advocacy contract
This contract was awarded to Matrix Ltd commencing 1st July 2022 until the end of June 2025. The contract has since been extended for a further 24 months, ending in June 2027.
Adult Instructed Advocacy
This relates to statutory advocacy for people able to instruct an advocate. The people concerned might be:
- Detained under the Mental Health in line with statutory legislation and will include those detained under Part 2 of the Mental Health Act such as those under section, guardianship, community treatment order (CTO) or Part 3 of the Mental Health Act such as those under section 37/41, 47 and 48.
- Residents of other boroughs detained in Surrey facilities under the mental health acts
- People in Prison or approved premises (in line with statutory legislation and best practice guidance and includes Care Act advocacy)
- Be entitled to advocacy under the Advocacy Care Act 2014 – for example people who have substantial difficulty understanding: (in line with statutory legislation and best practice guidance regarding Care Act advocacy, safeguarding support and young carer’s assessment and applies equally to carers in accordance with the parity they are given in the Care Act).
Care Act advocacy for young people (in line with statutory legislation and best practice) moving from Children’s to adult’s services.
Non-Statutory “Discretionary” Advocacy
The instructed advocacy contract also encompasses non-statutory/discretionary advocacy to people at risk and who require preventative support around a range of preventative issues in line with best practice such as people:
- accessing mental health/health services
- receiving substance misuse support
- living with a long-term condition or diagnosis, such as HIV
- with care and support needs who have difficulty understanding or retaining information and are at high risk of an escalation in care needs if preventative measures are not taken
This contract was newly awarded to Pohwer Ltd, commencing July 2022 – June 2025 and has since been extended by a further 24 months, until June 2027. It is a block commissioned contract funded in partnership between:
- SCC, to meet statutory duties under the Care Act for clients with capacity to instruct an advocate
- Public Health Surrey, to provide support to people with substance misuse needs
- NWS CCG representing all CCGs in Surrey, to support engagement of people needing advocacy in health and public health settings
Out of Scope
Specifications do not encapsulate:
- Independent Health Complaints Advocacy: this is commissioned by Healthwatch Surrey and delivered by Surrey independent Living council (SILC). The contract expires in 2025/27.
- “Appropriate adults” as defined by Police and Criminal Evidence Act, 1984
- Advocacy services to meet long term ongoing support needs such as mediation or counselling or representation at tribunals.
- Advice and information is out of scope unless it falls within the General Care Act Duty.
- Self-Advocacy
Children’s Advocacy
The Children’s Advocacy service supports SCC to fulfil certain statutory duties detailed within the following legislation:
- Children Act 1989
- Children Leaving Care Act 2000
- Adoption and Children Act 2002
- Children and Families Act 2014
- Care Planning, Placement and Review Regulations 2010
The service follows and adheres to the broad legal frameworks of the United Nations Convention on the rights of the child and the European Court of Human Rights which promotes the rights of children and young people. The child’s right to be in heard in matters affecting them is enshrined in Article 12 of the Convention of the Rights of the Child, which also stipulates that the child shall be provided with opportunities to be heard in any judicial and administrative proceedings affecting the child, either directly, or through a representative or appropriate body. The Service Provider, in partnership with SCC, is responsible for raising awareness regarding the promotion of children’s rights.
SCC commissioned Antser Holdings Ltd (Reconstruct) to deliver Advocacy Services for up to 415 Children and Young People (see below), July 2022 – July 2027, utilising all available extensions. The service is monitored to ensure the delivery of high-quality, independent advocacy that enables improved outcomes for:
- Looked after children
- Children subject to child protection planning
- Care leavers up to the age of 25
- Children and young people with special educational needs and/or disabilities (SEND), who have an Education Health and Care Plan (EHCP) and do not have appropriate representation
The service is monitored to ensure the delivery of high-quality, independent advocacy that enables improved outcomes for:
- Looked after children
- Children subject to child protection planning
- Care leavers up to the age of 25
- Children and young people with special educational needs and/or disabilities (SEND), who have an Education Health and Care Plan (EHCP) and do not have appropriate representation
The purpose of the service is to ensure that eligible children and young people:
- Have a voice throughout their journey within the care system and feel listened too, safe and cared for – both being able to share their views, wishes and feelings about decisions that are made about their care and education by the Local Authority and knowing that these are actively considered;
- Know that advocacy services are available to them, have easy access to the right support, in the right place, at the right time and that this is independent from the Local Authority;
- Understand how their engagement with advocacy can impact positively on the quality of service(s) provided, including how their feedback is used to improve the wider care system for others;
- Feel empowered by advocacy services, ensuring their views and ideas are the focus of any action taken that relates directly to them – with professionals being influenced by their experiences, wishes and feelings; and
- Know that their feedback (and that of their families) is used to inform practice and service development
Health inequalities
People with learning disabilities encounter significant health inequalities. These are systematic and unfair differences in their health outcomes and access to healthcare services when compared to people without learning disabilities.
The health inequalities section first looks at outcomes from primary health care data analysis, some more specific areas of health relating to either specialist related needs such as postural care or specialist access requirements including dementia and pregnancy and finally there is a separate section on access.
The LeDeR programme has found that, as well as dying earlier than people who don’t have learning disabilities, people with learning disabilities are three times more likely to die from an avoidable cause. Combating inequalities for people with learning disabilities is key to creating a more equal and just society.
The NHS Long Term Plan is explicit in its ambition to reduce health inequalities so that people with a learning disability can lead ’longer, happier and healthier lives’ [29]. Similarly, the recently published NHS Mandate for 2022/23 contains a specific objective about tackling disparities in health outcomes and access [30]. The higher risk of premature death among people with learning disability in England is well known and documented. [31]
In 2021/22 a report was commissioned covering the Surrey Heartlands geography in to support the Integrated Care System’s efforts in reducing the inequalities faced by people with learning disabilities, particularly the mortality gap, and to inform strategic prioritisation of these efforts. This was in addition to the annual LeDeR report. This section presents more detailed data relating to these inequalities including place based as well as others (with additional data added to cover the Frimley system where this is available).
In its 2021/22 plan, Surrey Heartlands ICS committed to a clear focus on those with learning disability and to drive efforts in significantly improving their life expectancy leading up to 2030.
The analysis presented in this report addresses three questions:
- What are the most common causes of death for people with learning disability and what are the associated risk factors?
- What are the most marked inequalities that emerge when comparing the populations of people with learning disability and those without learning disability in Surrey?
- What are the most significant inequalities that emerge when comparing data from within the population of people with learning disability in Surrey, segmented by age, gender, location and time?
Key findings are as follows:
- People with learning disability in Surrey Heartlands face considerable health inequalities – most notably for Type 2 diabetic blood glucose, obesity, and hypertension. We do not know if there is a higher incidence, greater propensity or poorer care.
- For inequalities related to age of mortality, diabetes, BMI, and hypertension, the gap is greater for women with learning disability – when compared to women without learning disability – than men with learning disability
- People with learning disability in Surrey Heartlands are significantly less likely than people without learning disability to receive cancer screenings
Other important findings are as follows:
- Over the last 4 years, the proportion of people in Surrey Heartlands with learning disability with BMI≥25 has not decreased at the same rate as the proportion of those receiving BMI-related interventions has increased
- Screening rates for cervical and breast cancer have not improved for people in Surrey Heartlands with learning disability over the last 4 years
- Although there was a marked increase in the proportion of people in Surrey with learning disability receiving AHCs between 2019/20 and 2021/22, this did not translate into a markedly higher proportion of the population receiving interventions for which they would be eligible
Comparisons by gender
- Women with learning disability in Surrey Heartlands are significantly more likely than men to have a BMI≥25
- Men with learning disability in Surrey Heartlands are significantly more likely than women to be smokers
Comparisons by age
- Receipt of health interventions available to all people with learning disability in Surrey Heartlands is significantly lower in the 14-19 and 20-29 age groups than older age groups
- The proportion of people with learning disability in Surrey Heartlands with a BMI≥25 increases significantly between the 14-19 and 20-29 age groups
Comparisons by ‘Place’ (as defined by the Surrey Heartlands Integrated Care Board)
- BMI ≥25 was the health outcome with the highest degree of variation observed across the four ‘places’ in Surrey Heartlands, with Northwest Surrey the lowest performing ‘place’ on several health outcome measures – most notably diabetes, BMI≥25 and smoking
- There are significant discrepancies between the four ‘places’ for uptake of breast and cervical cancer screenings by people with learning disability in Surrey Heartlands
Active diagnoses recorded for people with learning disabilities
Table 20: Percentage of adult patients (aged 18+) recorded on their general practice’s QOF learning disabilities register who have an active diagnosis of condition type
| Condition Type (Adults aged 18+) |
Frimley ICB: Prevalence for general patient population | Frimley ICB: Prevalence for patients with a recorded Learning Disability | Surrey Heartlands ICB: Prevalence for general patient population | Surrey Heartlands ICB: Prevalence for patients with a recorded Learning Disability |
| Asthma | 6.04% | 10.28% | 6.09% | 8.85% |
| Cancer | 4.16% | 2.94% | 5.08% | 2.55% |
| Dysphagia | Not Available | 12.48% | Not Available | 11.03% |
| GORD* | Not Available | 11.56% | Not Available | 12.12% |
| Severe Mental Illness | 0.96% | 9.91% | 0.94% | 9.09% |
| Dementia | 0.93% | 2.20% | 1.10% | 1.04% |
| Depression | 16.53% | 20.18% | 16.29% | 17.58% |
| Diabetes Type 1 | 0.47% | 2.02% | 0.46% | 1.09% |
| Diabetes Type 2 | 6.79% | 9.91% | 5.33% | 7.76% |
| Hypertension | 16.94% | 13.94% | 16.32% | 12.85% |
| BMI 30+ | 11.88% | 32.29% | 9.79% | 28.00% |
| BMI 18.4 (underweight) | 0.98% | 5.14% | 1.02% | 4.97% |
Source: Health and Care of People with Learning Disabilities, Experimental Statistics 2023 to 2024 – NHS England Digital
Table 21: Percentage of patients <18 years recorded on their general practice’s QOF learning disabilities register who have an active diagnosis of condition type
| Condition Type (children and young people < 18) | Frimley ICB: Prevalence for general patient population | Frimley ICB: Prevalence for patients with a recorded Learning Disability | Surrey Heartlands ICB: Prevalence for general patient population | Surrey Heartlands ICB: Prevalence for patients with a recorded Learning Disability |
| Asthma | 3.00% | 8.00% | 2.93% | 5.30% |
| Cancer | 0.12% | 2.40% | 0.13% | 3.03% |
| Dysphagia | No data | 4.00% | No data | 6.82% |
| GORD | No data | 13.60% | No data | 21.21% |
| Severe Mental Illness | 0.01% | 0.00% | 0.01% | 0.76% |
| Dementia | 0.00% | 0.00% | 0.00% | 0.00% |
| Depression | 0.48% | 1.60% | 0.49% | 1.52% |
| Diabetes Type 1 | 0.23% | 2.40% | 0.20% | 2.27% |
| Diabetes Type 2 | 0.01% | 0.80% | 0.01% | 0.00% |
| Hypertension | 0.04% | 0.80% | 0.02% | 2.27% |
| BMI 30+ | 0.74% | 7.20% | 0.51% | 6.06% |
| BMI 18.4 (underweight) | 4.58% | 16.80% | 4.09% | 14.39% |
Physical health outcomes
Respiratory conditions including COVID-19 and vaccination uptake
The national LeDeR report [32] indicates respiratory disease is possibly the leading cause of death for people with learning disabilities (46% to 52%), with rates much higher than for the general population (15% to 17%). People with asthma and learning disabilities were found to be twice more likely to be smokers than patients with learning disabilities who do not have asthma. More than half of women with learning disabilities and asthma are also obese.
The Surrey Heartlands ICB LeDeR report 2021/2022 found that Aspiration pneumonia was the most common cause of death in people with learning disabilities in Surrey Heartlands. It accounted for 40% of the deaths they reviewed. The second most common cause of death was pneumonia which made up 10% of the deaths reviewed.
Recommendation: Sustain the deep dive into respiratory deaths in order to better understand how these can be reduced, as recommended by the LeDeR review.
COVID-19
The COVID-19 pandemic highlighted the inequalities for people with learning disabilities, for example they are more likely to contract COVID-19, have a more severe case and were considered four times more likely to die from COVID-19 than the general population in 2020 according to Public Health England [33] [34]. Research [35] [36] [37] indicates that people with learning disabilities with COVID-19 were five times more likely to be admitted to hospital and eight times more likely to die. Mortality rates in this group were up to three times higher than that of the general population.
The Surrey Heartlands ICB LeDeR report 2020/2021 reported that the most common cause of death was COVID-19 followed by pneumonia. 51 adults with learning disabilities died from confirmed or suspected COVID-19 in 2020-2021, ages ranging from 30-96 with a mean age of 67 and median was 69. There were 19 women and 34 men, meaning male deaths accounted for 63% of all COVID-19 deaths reported to LeDeR in 2020/ 2021. Two of the deaths reported related to someone from a Black, Asian or Minority Ethnic community. In this instance, the individuals were from a Black British community.
Worrying attitudes and prejudices about the value of the lives of people with learning disabilities have surfaced during the pandemic [38]. For example:
- Reports of blanket use of DNACPR (Do Not Attempt Cardiopulmonary Resuscitation) orders that were not based on an individual’s best interests.
- Access to covid-19 vaccination programme prioritised people according to vulnerability but excluded learning disability within the criteria.
During the first wave of the Covid-19 pandemic, concerns were raised about the potential for “blanket” decisions being made around resuscitation, particularly for more vulnerable populations. As a result, this was reviewed as part of the LeDeR process. We found that ‘DNACPR orders’ were completed correctly and followed in 77% of the reviews. This reflects the work carried out in response to the 2019 LeDeR annual report findings and local recognition of the need to address this potential issue particularly during the pandemic and to continue to do so going forward.
Recommendation: Ensure that the ‘lessons learnt’ review of experience in the pandemic incorporates the views of the provider sector e.g. access to PPE.
Uptake of COVID-19 vaccination
Data from the commissioning support unit for Surrey Heartlands ICB shows that 86.5% of the 5,144 people on the GP register with a learning disability flag received a complete primary course of the COVID-19 vaccination (two doses and a booster), performing first in the South East region. Frimley ICB saw 84.0% of 3,064 people receiving a complete primary course (correct as of 02 November 2022).
As of 02 November 2022, of those eligible for a winter booster (GP registered population with a learning disability flag who have completed the primary course) Surrey Heartlands ICB was first in the region at 54.8%, Frimley ICB was second at 50.2%, with rollout incomplete. Both are higher than the proportion at National level (80.8% primary course, 42.9% Autumn booster).
Data may vary between local systems and region/ registers.
Recommendation: Ascertain if mass vaccination centres can use the learning disability flag and routinely offer reasonable adjustments.
Uptake of Flu vaccination
Influenza vaccination uptake for those with a learning disability indicator recorded in their GP records has been increasing over time in Surrey Heartlands CCG (63.4%) decreasing in Frimley CCG (59.6%) in 2023/24*.
Table 22: Percentage of patients with a learning disability indicator who had an immunisation against seasonal influenza 01 August to 31 March by year
| Year | NHS Surrey Heartlands ICB % * | NHS Frimley ICB % * |
| 2019/20 | 45 | 47.6 |
| 2020/21 | 62 | 60.4 |
| 2021/22 | 66.8 | 65.9 |
| 2022/23 | 63.1 | 60.6 |
| 2023/24 | 63.4 | 59.6 |
Source: Health and Care of People with Learning Disabilities, Experimental Statistics 2023 to 2024 – NHS England Digital
Cardiovascular disease [39]
Cardiovascular disease (CVD) is a general term for conditions affecting the heart or blood vessels and is one of the main causes of death and disability in the UK. Deaths by CVD can be preventable by leading a healthy lifestyle: high blood pressure (hypertension) is one of the most important risk factors for CVD along with smoking, diabetes and obesity [40].
Epidemiological research on age-related rates of CVD in people with learning disabilities is scarce and inconclusive [41]. The prevalence of CVD in adults with learning disabilities may be greater and apparent earlier in life than that found in the general population [42]. However, there may be variation depending on type of CVD. Primary care records of nearly 15,000 adults with learning disabilities in England indicate that the prevalence of ischaemic heart disease (IHD) is lower than in the general population (prevalence ratio 0.65 (95% CI 0.57, 0.74) but rates of heart failure are higher (prevalence ratio 2.26 (95% CI 1.84, 2.78) as are rates of stroke and transient ischaemic attack (TIA) (prevalence ratio 1.74 (95% CI 1.52 to 1.98)[43]
A systematic review on causes of death of people with Down’s syndrome found that congenital heart anomalies were reported as the leading primary or underlying cause of mortality in the majority of the studies. Congenital heart anomalies were substantially more common as a cause of death in Down’s syndrome than the general population [44].
Based on data regarding roughly 5% of the population of England, diseases of the circulatory system were responsible for the largest number of deaths of people with learning disabilities. Myocardial infarction (heart attack) and chronic ischemic heart disease caused the most deaths. After adjusting for age and gender, death rates for these conditions in people with learning disabilities were double those in the general population [45]
Hypertension
Primary care data from 2023/24 showed that people with learning disabilities in Surrey are slightly more likely to be hypertensive than people without learning disabilities, with a standardised prevalence ratio (SPR) of 1.1. Greater inequalities emerge for specific age groups.
Table 23 shows that inequality is particularly pronounced in the 35 to 44 and 45 to 54 cohorts. People with learning disability aged 35 to 44 are 2.3 times more likely that people without learning disabilities to have hypertension (9% compared to 4%); for the 45 to 54 cohort, the number is 1.5 times more likely (19% compared to 13%).
Hypertension inequalities by age group
For hypertension the degree of inequality experienced by younger cohorts with learning disability is greater than that for older cohorts. For cohorts older than 65 years, people without learning disabilities are more likely to be hypertensive than people with learning disabilities (Table 23). It is important to note here that, according to the 2020 LeDeR national report, circulatory diseases are the second most common cause of mortality amongst people with learning disabilities. Suggesting that people with learning disabilities are more likely to die at an earlier age from hypertension than the general population, which will contribute to the difference shown in the prevalence of hypertension in people aged 65 and over.
Table 23: Prevalence of hypertension within the populations of Frimley and Surrey Heartlands ICB, 2023/2024
| Age groups | Frimley ICB with a Learning Disability | Frimley ICB without a Learning Disability |
Surrey Heartlands with a Learning Disability |
Surrey Heartlands without a Learning Disability |
| 18 to 24 | 1.92% | 0.18% | 1.46% | 0.15% |
| 25 to 34 | 2.82% | 0.83% | 1.96% | 0.75% |
| 35 to 44 | 9.09% | 3.91% | 7.64% | 3.09% |
| 45 to 54 | 18.84% | 12.78% | 15.93% | 10.05% |
| 55 to 64 | 30.67% | 25.98% | 25.86% | 22.41% |
| 65 to 74 | 36.59% | 43.02% | 38.46% | 38.08% |
| 75 and over | 64.71% | 60.11% | 44.44% | 55.66% |
Figure 16: Prevalence of hypertension in Frimley and Surrey Heartlands Integrated Care System, by age group, for people with and without learning disabilities, 2023/24
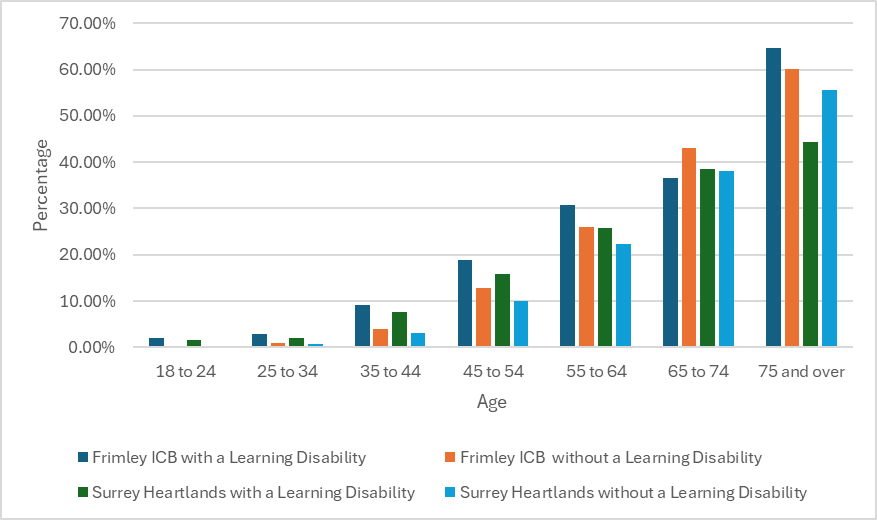
Weight management
The national prevalence for obesity (defined as BMI≥30) was 37% for people with learning disabilities, compared to 30% for the general population [46]. People with learning disabilities are therefore 23% more likely to be obese than people without learning disabilities, according to this data. Although we do not have Surrey-specific comparisons of obesity amongst people with learning disability and people without learning disability, we can expect a similar pattern of greater inequality at younger ages to that presented in the national data to emerge. This highlights the importance of tailored initiatives to focus on younger age groups.
The commissioned report found that over the last 4 years, the proportion of people in Surrey with learning disability with BMI≥25 (overweight) has not decreased at the same rate as the proportion of those receiving BMI-related interventions has increased. Between 2018/19 and 2021/22, the proportion of people with learning disability with a BMI≥25 decreased by 5 percentage points (63% to 58%). This improvement should be celebrated. However, this reduction is also set against more marked increases in the levels of BMI-related interventions being received:
- the proportion of eligible people with learning disability receiving a weight intervention for BMI≥25 increased from 28% to 40% between 2018/19 and 2021/22
- the proportion of people with learning disability receiving assessments of nutritional status, diet and level of physical activity increased from 24% to 32% between 2018/19 and 2021/22.
This divergence suggests that these interventions are not working as effectively as they could be.
Two groups emerged as experiencing greater inequalities regarding obesity – young people and women. ‘Young people’ is covered below.
The proportion of people with a learning disability in Surrey Heartlands with a BMI ≥25 increases significantly between the 14 to 19 and 20 to 29 age groups
Despite lower uptake of annual health checks the proportion of people with learning disability in Surrey Heartlands with a BMI≥25 increases significantly between the 14 to 19 and 20 to 29 age groups.
Although the proportion of people with a learning disability with a BMI ≥25 is larger for older age groups, data from 2021/22 shows that the biggest single increase between age groups is 19 percentage points between the 14 to 19 cohort (32%) and the 20 to 29 cohort (51%) – with a similar pattern observed in the preceding 3 years of data as well.
Figure 17: Proportion of people with a learning disability in Surrey Heartlands with BMI ≥25, by age group
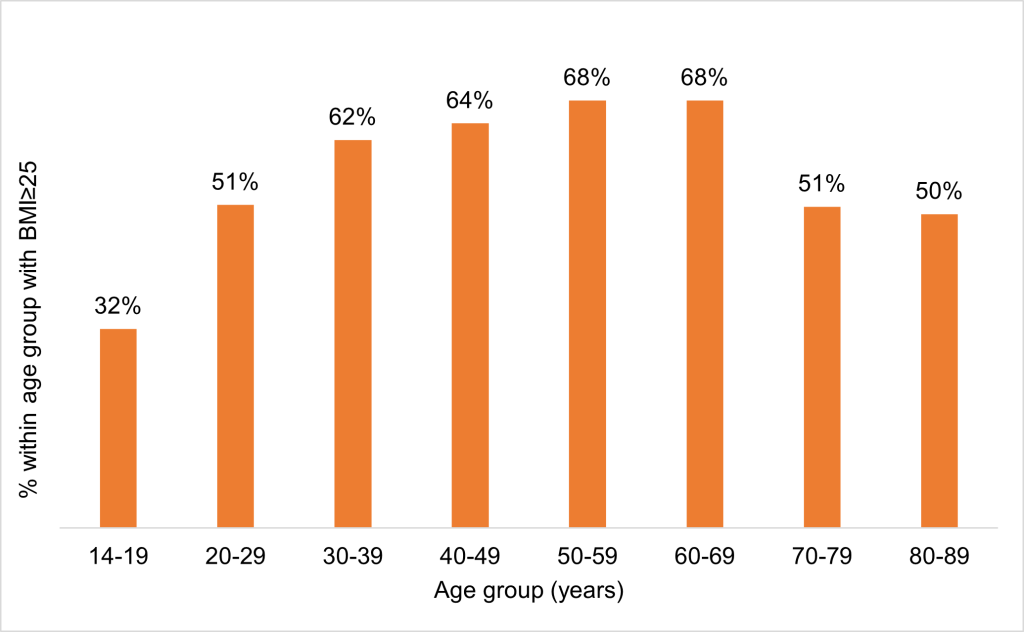
This increase comes despite a greater proportion of the population receiving an assessment of nutritional status, diet and level of activity in the 20 to 29 age group (28%) compared to the 14 to 19 age group (22%).
It is well known that the difficulty of transitioning from adolescence to young adulthood is often compounded for people with learning disabilities. This occurs for a range of reasons including an extended duration of transition, the ‘routinisation’ of parental autonomy and reduced opportunity to have experiences that aid successful transitions [47]. However, the specific effect of transition on health outcomes remains under-researched and systematic reviews have called for future work in this area [48].
Further information is available in the Surrey’s Children and Young People with Additional Needs and Disabilities Joint Strategic Needs Assessment 2022 which contains significant data and insight into transitions including the in detail in the ‘preparing for adulthood’ section (slides 115-120) and also throughout the document (Children and Young People with Additional Needs and Disabilities | Surrey-i (surreyi.gov.uk)).
Data for Frimley is also provided; the data for Frimley residents who live within Surrey but outside of the Surrey Heartlands footprint was not included in the commissioned health inequalities report commissioned.
The data for both Surrey Heartlands (Figure 19) and Frimley (Figure 18) details a comparator between those with and without learning disabilities differs in that it references obesity levels by BMI >= 30.0 whereas the Surrey Heartlands commissioned report analysis references BMI≥25 above.
For both Frimley and Surrey Heartlands, although the percentage of people with a BMI >= 30.0 is higher for people with a learning disability, the trajectory broadly follows the general population except in the 55 to 64 age range.
We also see the steep rise of young people becoming young adults entering this BMI category.
Figure 18: Percentage of patients in Frimley ICB whose most recent BMI assessment classification (or downs syndrome BMI centile classification) in the last 15 months up to and including 31 March, is obese (BMI >= 30.0), by age band
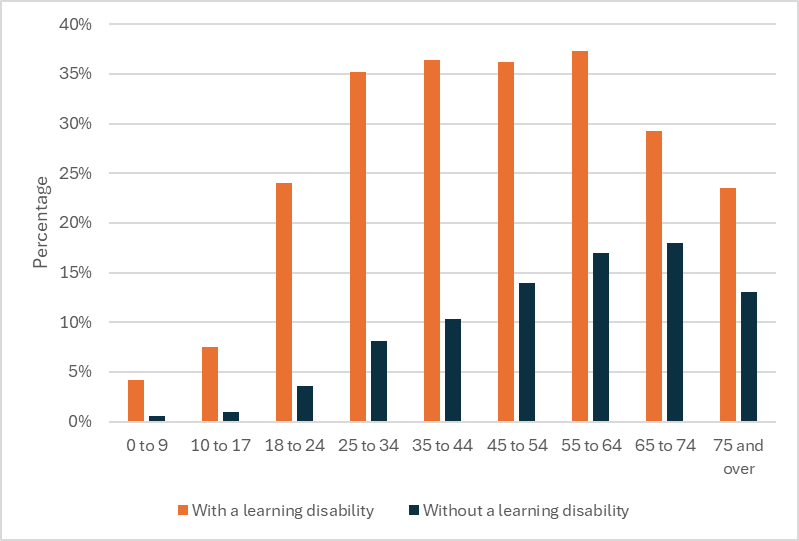
Figure 19: Percentage of patients in Surrey Heartlands ICB whose most recent BMI assessment classification (or downs syndrome BMI centile classification) in the last 15 months up to and including 31 March, is obese (BMI >= 30.0), by age band
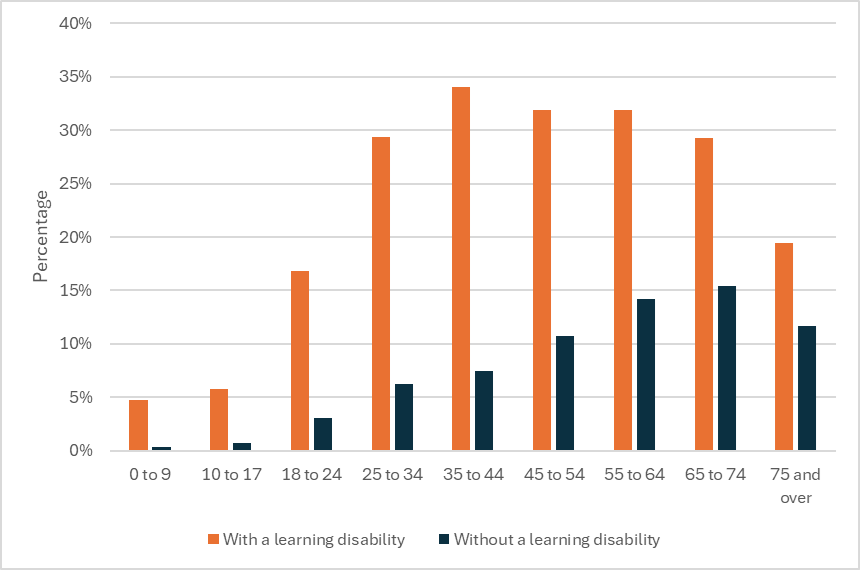
Figure 20: Percentage of patients in Frimley ICB whose most recent BMI assessment classification (or downs syndrome BMI centile classification) in the last 15 months up to and including 31 March, is overweight (BMI >= 25.0 to 29.9), by age band
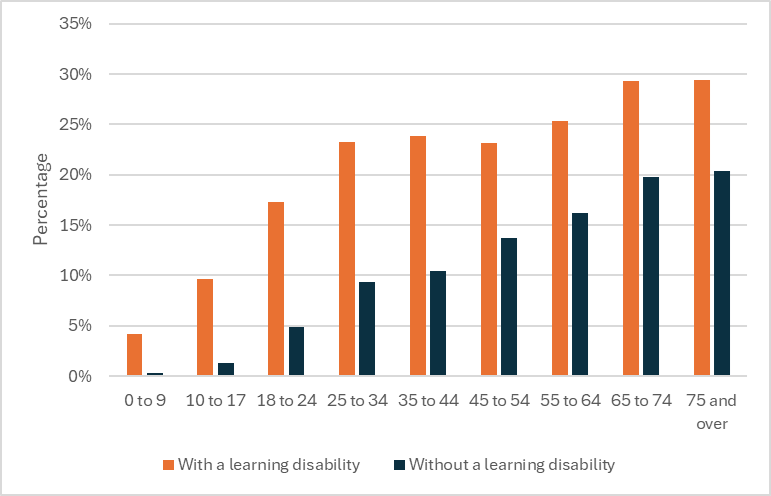
Figure 21: Percentage of patients in Surrey Heartlands ICS whose most recent BMI assessment classification (or downs syndrome BMI centile classification) in the last 15 months up to and including 31 March, is overweight (BMI >= 25.0 to 29.9), by age band
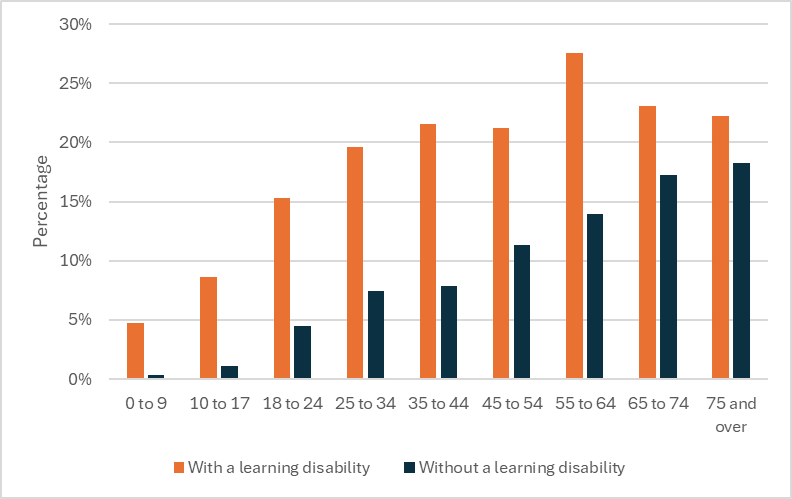
Recommendation: Work with public health and system clinical leads to ensure that:
- weight management support is reasonably adjusted to meet the needs of younger people with a learning disability
- targeted support is offered to try to reduce the proportion of young people becoming obese.
Type 2 Diabetes [49]
According to the national General Practice Extraction Survey (GPES) data in 2017/18, an average 6.8% of people with learning disabilities have type 2 diabetes compared with 4.8% of the general population. A study that examined the rates of undiagnosed diabetes put the overall prevalence rate for people with learning disabilities at 8.5%, slightly higher than the overall GPES prevalence.[50]
Primary care data from 2020/21 showed that people with learning disabilities in Surrey were 2.1 times more likely to have type 2 diabetes than people without learning disabilities [51] according to the Standardised Prevalence Ratio.
The degree of inequality concerning the prevalence of diabetes appears to be worsening over time. In 2016/17, people with learning disabilities were 1.8 times more likely to be diabetic than those without a learning disability.
Type 2 Diabetes inequalities by age
Even greater inequalities emerge when examining specific age groups. People aged between 35 and 44 years with learning disabilities are more than 5 times as likely to be diabetic than people without learning disabilities in the same age cohort (6% compared to 1%); people aged between 45 and 54 years with learning disabilities are 3.4 times more likely to be diabetic (11% compared to 3%).
The fact that the gap between people with and without learning disabilities is largest for younger cohorts highlights the importance of early intervention.
Figure 22: Prevalence of type 2 diabetes in Surrey Heartlands and Frimley by age group for people with learning disabilities and people without learning disabilities (2023/24)
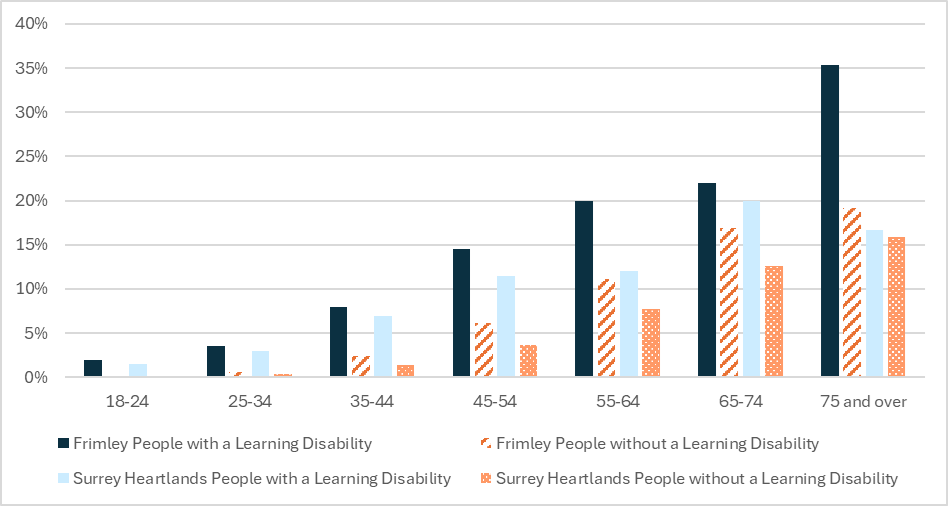
Type 2 Diabetes inequalities by gender
For men with learning disabilities in Surrey Heartlands, prevalence was at 6%, compared to 5% of men without learning disabilities. For men with learning disabilities in Frimley, prevalence was 7%, compared to 6% of men without learning disabilities.
There is a significant inequality for women, in 2023/24, the prevalence of Type 2 diabetes amongst women with learning disabilities in Surrey Heartlands was 7%, compared to 4% of women without learning disabilities. For women with learning disabilities in Frimley, prevalence was 10%, compared to 5% of women without learning disabilities.
Figure 23: Prevalence of diabetes for women and men, with and without learning disabilities, in Frimley and Surrey Heartlands (2023/24)
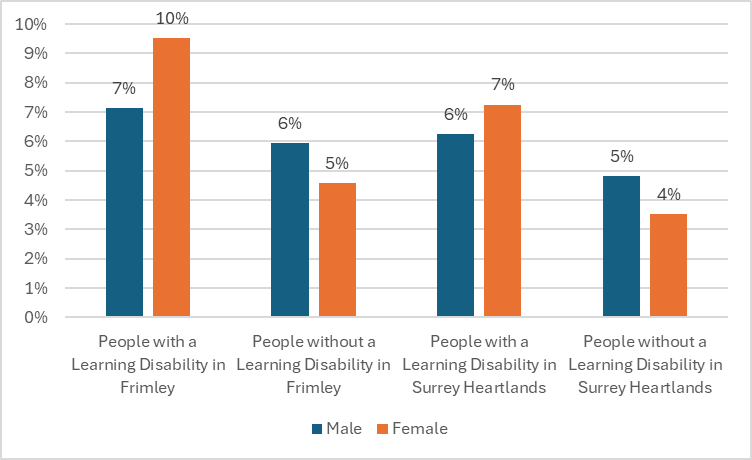
Cancer and cancer screening
Fewer people with learning disabilities in Surrey died from cancer than expected in 2021/22, given the degree of inequality in cancer screening rates between people with and without learning disabilities.
Uptake of cancer screening in Surrey
National data has shown that people with learning disabilities are markedly less likely to receive cancer screenings than people without learning disabilities [52] and this is reflected in local data. The aforementioned commissioned report found that people with learning disabilities in Surrey Heartlands are significantly less likely than people without learning disabilities to receive cancer screenings and that screening rates for cervical and breast cancer had not improved for people in Surrey Heartlands with learning disabilities over the last 4 years.
In the context of this, it is surprising that the percentage of deaths from cancer appears to be relatively low amongst the population of people with learning disability, at 9% for all cancers (not just those screened). Surrey’s profile aligns closely to the national picture, where cancer is only the fourth most common cause of death, at 11% of total deaths. This finding should not reduce the momentum behind existing initiatives in Surrey – spearheaded by the LeDeR Screening Group – which seek to increase uptake of cancer screenings for people with learning disability.
There are discrepancies between the screening data available however GP level data suggests the figures shown in the table below.
Figure 24: Percentage of screening uptake in people with learning disabilities by Surrey Heartlands Place
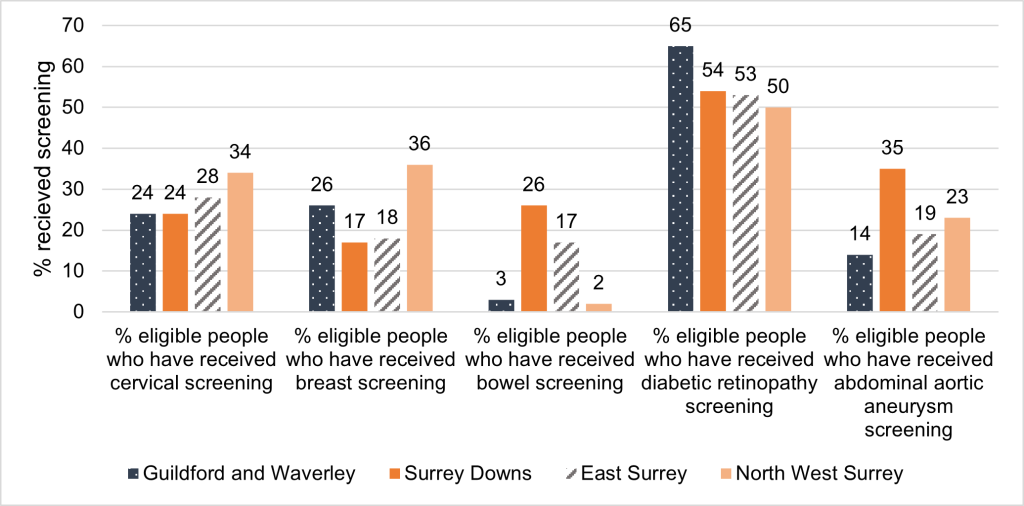
The report also found significant discrepancies between the four places within Surrey Heartlands for uptake of breast and cervical cancer screenings. This remains the case in the data shown above, with all but one of the screening programmes showing less than 40% uptake in people with learning disabilities. The extreme range in bowel screening uptake suggests a possible coding issue with the inputting of bowel screening data which is being investigated further.
Notable discrepancies in 2021/22 were as follows:
- For breast screening, take-up was 36% of the eligible population of people with learning disabilities in North West Surrey, but only 14% in East Surrey
- For cervical cancer screening, take-up was 34% in North West Surrey, but only 23% in Guildford and Waverley
There is some variation looking back over time, but some patterns have remained constant:
- North West Surrey was the place with the highest proportionate take-up of breast screening amongst those eligible over each of the last 3 years
- Guildford & Waverley was the place with the lowest proportionate take-up of cervical screening amongst those eligible over each of the last 4 years
Whilst these patterns have remained consistent for the two individual screening types, there is no consistent pattern across both types of cancer screening over time.
This finding suggests an opportunity to explore possible inconsistencies between place on how cancer screening is offered and promoted.
Table 24: Percentage of patients who are female aged 50 to 69 and received breast cancer screening in the five years leading up to and including 31 March, by year
| Year | Surrey Heartlands ICB with learning disability | Surrey Heartlands ICB without learning disability | Frimley ICB with learning disability | Frimley ICB without learning disability |
| 2019/20 | 52.50% | 74.10% | 52.70% | 71.60% |
| 2020/21 | 48.80% | 71.60% | 49.70% | 69.50% |
| 2021/22 | 48.49% | 70.47% | 48.30% | 71.53% |
| 2022/23 | 48.39% | 69.56% | 41.94% | 68.64% |
| 2023/24 | 48.45% | 67.40% | 33.33% | 68.87% |
Source: Health and Care of People with Learning Disabilities, Experimental Statistics 2023 to 2024 – NHS England Digital
Table 25: Percentage of patients eligible* for cervical cancer screening on whom an adequate cervical smear test has been performed in the three years and six months (for those aged 25 to 49) and in the five years and six months up (for those aged 50 to 64) up to and including 31 March, by year
| Year | Surrey Heartlands ICB with learning disability | Surrey Heartlands ICB without learning disability | Frimley ICB with learning disability | Frimley ICB without learning disability |
| 2019/20 | 27.20% | 71.30% | 26.00% | 71.00% |
| 2020/21 | 24.40% | 70.00% | 24.30% | 69.90% |
| 2021/22 | 26.39% | 73.02% | 27.02% | 72.76% |
| 2022/23 | 26.11% | 72.38% | 27.92% | 71.82% |
| 2023/24 | 28.57% | 72.71% | 30.13% | 72.12% |
** Patient coverage 88.0% for Surrey Heartlands ICB and 94.1% for Frimley ICB
Source: Health and Care of People with Learning Disabilities, Experimental Statistics 2023 to 2024 – NHS England Digital
In order to try to improve the screening uptake across Surrey Heartlands ICB, a system wide screening meeting was set up, with the aim of task and finish groups being set up for each screening programme. The bowel screening task and finish group has made the most progress and have undertaken some work to ensure that the screening hub are sent a list of people with learning disabilities who are due to be invited for screening. This will then allow the hub to send out easy read invite letters and information in advance and enquire about reasonable adjustments that may be required to ensure they can access the screening they require.
Physical activity
We have limited pockets of information about the level of physical activity people with learning disabilities undertake within Surrey.
The commissioned report considered data on interventions for which people with learning disabilities would be eligible, including ‘assessments of diet & exercise’. The proportion of people with learning disabilities receiving assessments of nutritional status, diet and level of physical activity increased between 2018/19 and 2021/22 (24% to 32%) with a corresponding 5 percentage point reduction between 2018/19 and 2021/22 of the proportion of people with learning disabilities with a BMI ≥25 (63% to 58%).
However, for several interventions available to the whole population of people with learning disabilities data from 2021/22 shows that take-up is lower in the 14 to 19 and 20 to 29 age groups than older age groups including assessment of nutritional status, diet and level of activity.
Figure 25: Proportion of people with a learning disability receiving assessment of nutritional status, diet, and level of activity in Surrey by age group, 2021/22
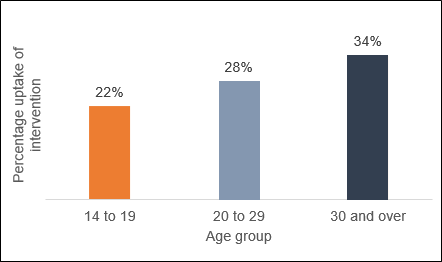
Lifestyle interventions offered via primary care post annual check as an alternative or in conjunction with a medication related intervention were also analysed with physical activity as one lifestyle intervention. The analysis indicated that although the proportion of people in Surrey with learning disability receiving AHCs increased markedly from 48% to 75% between 2019/20 and 2021/22 (a 54% increase) this did not translate into a markedly higher proportion of the population receiving interventions for which they would be eligible. The only marked increase was in relation to the prediabetic cohort of people with learning disabilities receiving a lifestyle intervention.
In response, Surrey County Council’s Public Health team commissioned a ‘Surrey Whole System Approach to Obesity for people with learning disabilities’. This resulted in a 14-point action plan in 2022 including both diet and physical activity. Those that include exercise related actions are:
1. Implement internal Policy for healthy living and eating, across all organisations
3. Generate a recognised Charter for Health – this approach for all employers to adopt their policy on healthy living framework
5. Providers to set service users and staff, healthy lifestyle challenges to create long-term instinctive choices
12. Create a register of county facilities for private use such as the therapy swimming pools for Learning Disabilities & Autism adults not currently using public pools due to social anxiety
Recommendation: Further understanding of the level of physical activity and access (including barriers), interlinked to the Whole System Approach to Obesity for people with learning disabilities and connecting into other initiatives such as Active Surrey and Active Travel.
Recommendation: Health inequalities group to be convened to consider all the health inequalities including wider determinants and supporting the two public health leads in community asset and grass root approaches to the recommendations.
Gender based inequalities within the learning disabilities population
At the time of the commissioned 2020 LeDeR report, the age at death was 11 years younger for men with learning disabilities compared with men in the general population: among women this doubles to 22 years. This was updated in the 2021/2022 LeDeR annual report where women with learning disabilities in Surrey, die 20 years sooner than women who do not have learning disabilities and men with learning disabilities, in Surrey, die 14.7 years sooner than men who do not have learning disabilities.
In addition to a gender-based inequality regarding the mortality gap, women with learning disabilities are also suffering from greater morbidity. The increased prevalence of health issues linked to early death among all people with learning disabilities (diabetes, obesity and hypertension) is greater for women with a learning disability.
According to recent national research presented to the House of Commons, men in the general population were 13% more likely than women to have an overweight or obese BMI (≥ 25) [53]. Women in Surrey with learning disabilities, however, were 16% more likely than men with learning disabilities to be overweight or obese. This pattern of increased likelihood holds across each of the last 4 years and can be observed across the majority of age groups (with the exception of 60 to 69 and 80 to 89).
Figure 26: Proportion of men/women with learning disabilities in Surrey who have BMI ≥ 25, 2018/19 to 2021/22
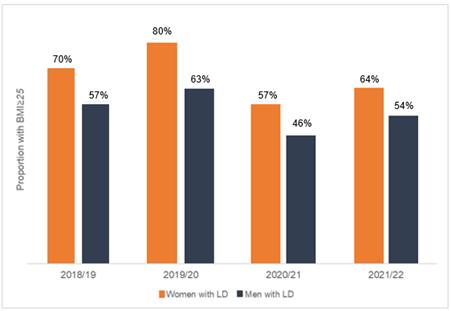
Women with learning disabilities in Surrey are significantly more likely than men to have a BMI ≥25. There is no clear-cut clinical evidence to explain this skew towards women, especially as the inverse applies to people without learning disabilities. One potential explanatory factor is the impact of hormonal imbalances on weight management. This may be particularly relevant to people with learning disabilities where communication challenges can make it difficult to support service users to manage menstrual cycles, to manage conditions which set off hormonal imbalance, and to manage the onset of menopause, an area that remains under-researched [54].
Recommendation: To further understand why women with learning disabilities are more likely to be overweight and design appropriate interventions.
Recommendation: A greater understanding of needs and experiences of women with a learning disability of peri menopause and menopause including but not limited to impacts on weight (including access to support, interventions and mental health impacts).
This finding suggests that BMI-related interventions, such as assessments of nutritional status, diet and level of physical activity, are not working as effectively as they could be, and indicates an opportunity for developing and augmenting weight management-related interventions targeted at women specifically.
For hypertension, the pattern is repeated: men without learning disabilities in Surrey were 2% more likely than women without learning disabilities to be hypertensive, according to 2020/21 data. Women with learning disabilities in Surrey, however, were 33% more likely than men with learning disabilities to have hypertension.
These findings offer a potential explanation for the difference in mortality gap between men and women with learning disabilities: if gender trends for health outcomes are inverted for the population of people with learning disabilities, it is to be expected that the mortality trend whereby women tend to live longer than men in the general population is also inverted. The reasons for which women with learning disabilities might have worse health outcomes than men are less clear: some potential hypotheses are offered alongside the intra-population gender analyses.
The compounded inequality that women are facing needs to be acknowledged and addressed if equality for all people with learning disabilities is to be improved. This finding provides considerable evidence to support related interventions (aimed at improving diet, or levels of exercise, for example) that are specifically targeted at women.
Table 26: Number of patients with a learning disability and without a disability who have an active diagnosis of hypertension, as at the end of the reporting period
| Age groups | Frimley ICB with a learning disability | Frimley ICB without a learning disability | Surrey Heartlands ICB with a learning disability | Surrey Heartlands ICB without a learning disability |
| 0 to 9 | 0 | 20 | 5 | 15 |
| 10 to 17 | 5 | 45 | 10 | 35 |
| 18 to 24 | 10 | 110 | 10 | 115 |
| 25 to 34 | 20 | 900 | 20 | 925 |
| 35 to 44 | 40 | 4,890 | 55 | 4,650 |
| 45 to 54 | 65 | 14,015 | 90 | 14,605 |
| 55 to 64 | 115 | 23,680 | 150 | 27,650 |
| 65 to 74 | 75 | 25,335 | 125 | 31,275 |
| 75 and over | 55 | 34,865 | 80 | 50,020 |
| Total | 385 | 103,860 | 545 | 129,290 |
Table 27: Proportion of male and female patients in the learning disability cohort who have an active diagnosis of hypertension by age group for both Frimley ICB and Surrey Heartlands ICB, as at the end of the reporting period
| Age groups | Frimley ICB males | Frimley ICB females | Surrey Heartlands ICB males | Surrey Heartlands ICB females |
| 0 to 9 | 0% | 0% | 4.35% | 0% |
| 10 to 17 | 1.67% | 0% | 1.56% | 2.50% |
| 18 to 24 | 1.54% | 2.56% | 1.10% | 2.17% |
| 25 to 34 | 2.41% | 3.39% | 2.36% | 1.30% |
| 35 to 44 | 7.84% | 10.81% | 7.50% | 7.81% |
| 45 to 54 | 20.00% | 17.65% | 16.67% | 15.09% |
| 55 to 64 | 32.56% | 28.13% | 25.40% | 26.42% |
| 65 to 74 | 40.00% | 33.33% | 34.29% | 43.33% |
| 75 and over | 62.50% | 66.67% | 44.44% | 44.44% |
Primary care
The NHS Long Term Plan – Learning disability and autism (section 3.31) states that action will be taken to tackle the causes of morbidity and preventable deaths in people with a learning disability and for autistic people and to help do so the plan including improving the uptake of the existing AHC in primary care for people aged over 14 years with a learning disability, so that at least 75% of those eligible have a health check each year.
In Surrey, there are approximately 21,800 adults with learning disability and/or autism and 7,000 children with additional needs and disabilities (Surrey County Council, JSNA, 2017). Of this overall number, approximately 4,790 aged 14+ are on the primary care GP learning disability register with work underway to improve this number. This number increases to 5,144 on the QOF.
The proportion of people in Surrey with learning disabilities receiving AHCs increased markedly between 2019/20 and 2021/22, from 48% to 75%, which equates to a 54% increase. This is a significant achievement.
Figure 27: Annual Health Checks System Target vs. Actual Trajectory 2021/22
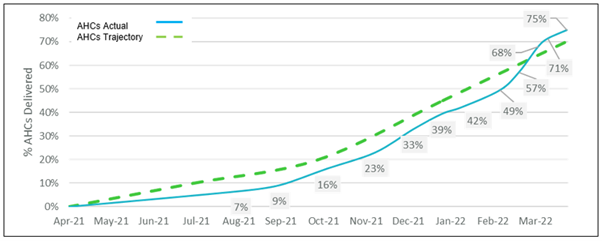
However, the higher number of AHCs did not consistently translate into an increase in the proportion of people with learning disabilities receiving AHC-facilitated interventions for which they would be eligible. The only marked increase was in relation to the prediabetic cohort receiving a lifestyle intervention. Between 2019/20 and 2021/22, there was a decrease in proportionate take-up of the following interventions:
- Blood lipid test
- Assessment of nutritional status, diet and level of activity
- Medication intervention for raised blood pressure
Figure 28: Percentage of people with learning disabilities receiving health checks, blood lipid tests, assessment of nutritional status, diet and level of activity and medication interventions for raised blood pressure (where eligible), 2019/20 – 2021/22
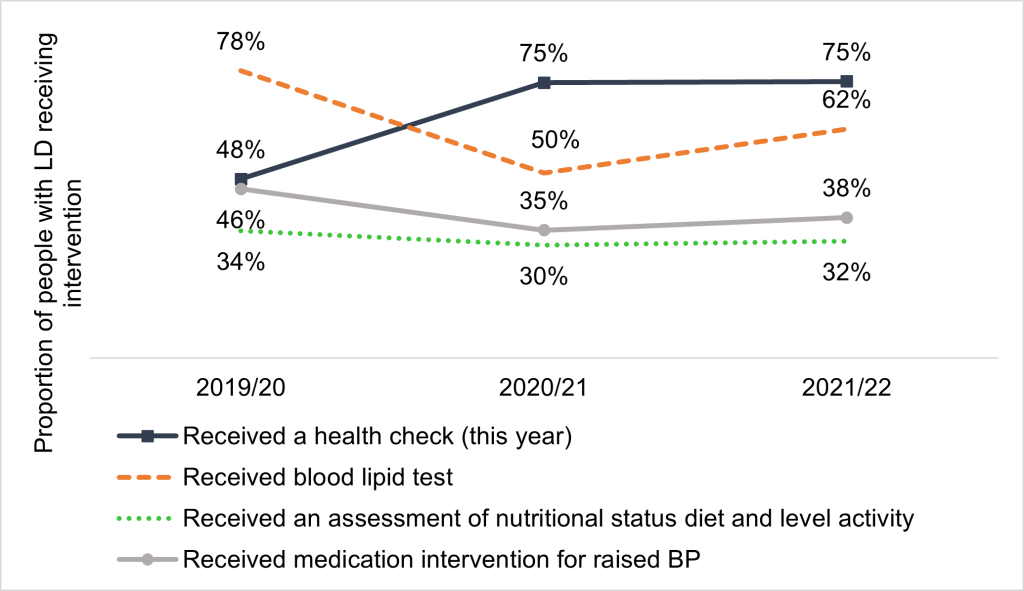
Figure 29: Proportion of people with learning disability in Surrey receiving AHCs by age group, 2021/22
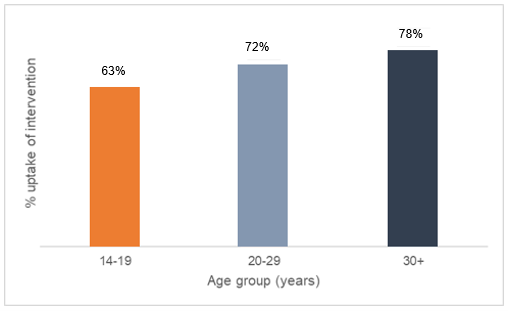
The findings should be viewed in the context of the intense capacity pressures experienced by primary care during the COVID-19 pandemic. Although the number of completed AHCs went up, primary care practitioners may have lacked the capacity to give the time and attention to each AHC required, which might account for proportionately fewer interventions being recommended and received.
Of note is that for several interventions available to the whole population of people with a learning disability, data 2021-22 shows that take-up is lower in the 14 to 19 and 20 to 29 age groups than older age groups including AHCs as above, flu vaccination, assessment of nutritional status, diet and level of activity and blood lipid test.
The views of people with learning disabilities and their experiences of accessing primary care are covered in other sections.
Recommendation: Joint work across the age ranges under the governance of the health inequalities group to consider and address the reasons for low uptake of annual health checks and other interventions for younger people.
This finding indicates an opportunity to focus on both the quantity and quality of AHCs so that they result in the most appropriate interventions for people with Learning Disability in Surrey.
Measures of physical health recorded at a good practice AHC are linked to both respiratory and circulatory disorders (see Table 28). As a result, successful interventions aiming to reduce mortality caused by respiratory disorders, for example, would also have an impact on deaths caused by circulatory disorders.
Table 28: Top causes of mortality for people with learning disabilities in Surrey (2021-22), mapped to corresponding risk factors assessed at AHCs and relevant interventions {i}
| Risk factors | Respiratory disorders | Circulatory disorders | Neoplasms |
| BMI ≥ 25 | Yes | Yes | Yes |
| Current smoker | Yes | Yes | Yes |
| Blood glucose- prediabetic/diabetic | Yes | Yes | No |
| Hypertension | No | Yes | No |
| Heavy alcohol consumption | No | Yes | Yes |
| Interventions relevant to risk factors | Respiratory disorders | Circulatory disorders | Neoplasms |
| Weight intervention | Yes | Yes | Yes |
| Assessment of nutritional status, diet and level of physical activity | Yes | Yes | No |
| Flu vaccination | Yes | No | No |
| Support to stop smoking | Yes | Yes | Yes |
| Intervention or referral for diabetes (lifestyle, referral or medication) | Yes | Yes | No |
| Intervention for blood pressure (lifestyle or medication) | No | Yes | No |
| Alcohol intervention | No | Yes | Yes |
| Blood lipid test | No | Yes | No |
| Breast/cervical/colorectal screening | No | No | Yes |
*Yes indicates if a risk factor or interventions relevant to risk factor correspond with the top causes of mortality
Source: Surrey Heartlands AHC
These overlaps validate that those health outcomes and interventions that are currently assessed and facilitated at AHCs are highly relevant to the most common causes of death amongst people with Learning Disability. This is an encouraging picture, suggesting that improvement of current interventions and AHCs should constitute a significant element of any effort to reduce the mortality gap for people with Learning Disability.
Variations in physical health between Surrey Heartlands Four ‘Places’
BMI≥25 was the health outcome with the highest degree of variation observed across Place in Surrey. The variation across Place for the percentage of people with a BMI≥25 was the highest of all health outcomes for all 4 years of data – with this being a statistically significant finding in 2018/19, 2019/20 and 2021/22.
Table 29: Percentage of people who have a learning disability in Surrey with a BMI of 25 or higher, 2018/19 to 2021/22
| Year | East Surrey- % with BMI ≥25 | Guildford & Waverley- % with BMI ≥25 | North West Surrey- % with BMI ≥25 | Surrey Downs- % with BMI ≥25 | Standard deviation across Place |
| 2018-2019 | 64% | 54% | 68% | 66% | 5.5% points |
| 2019-2020 | 74% | 63% | 70% | 73% | 4.0% points |
| 2021-2022 | 52% | 59% | 63% | 59% | 3.8% points |
For comparison, the next highest measure of standard deviation across place in both 2018/19 and 2019/20 was 3.3% points (for the proportion of people with learning disabilities at high risk of being diabetic or being pre-diabetic). In 2021/22, the next highest measure of standard deviation across place was 1.6% points, for the proportion of people with learning disabilities who were diabetic.
This finding indicates a notable degree of geographical variation for BMI≥25 relative to other health outcomes and suggests an opportunity to explore the reasons underlying this.
North West Surrey is also the lowest performing on several health outcome measures in 2021-22, recording the lowest performance across Place on the outcome measures presented in Table 30. It is not known if this is replicated in the wider population.
Table 30: North West Surrey outcome performance for people with learning disability 2020/21
| Outcome for people with learning disability in 2021-22 | North West Surrey performance | Gap to highest performing Place |
| Proportion with BMI≥25 | 63% | 17% |
| Proportion who are diabetic | 11% | 39% |
| Proportion who are pre-diabetic/high risk | 10% | 34% |
| Proportion who are current smokers | 11% | 37% |
This pattern was replicated in part over previous years. In the previous 3 years before 2021/22, North West Surrey was the place with the highest proportion of those with diabetes and the highest proportion of those who were current smokers. It was also the place with the highest proportion of those with BMI ≥25 in 2018/19.
Recommendation: Work with public health and system clinical leads diabetes leads to ensure support is reasonably adjusted to meet the needs of people with a learning disability and targeted support is offered in North West Surrey ‘place’.
In addition, North West Surrey was the place with the lowest proportion of patients on the learning disabilities Register who had an AHC in 2021/22 and 2020/21, and with the joint-lowest proportion in 2018/19.
Recommendation: Monitoring on an ongoing basis with both the Surrey Heartlands performance team, primary care liaison service and place-based leads to offer support where needed to ensure North West Surrey has support if needed to offer health checks.
This finding suggests an opportunity to explore the reasons underlying these challenges in North West Surrey, and to consider whether interventions need to be designed or targeted differently.
See also former recommendation: Health inequalities group to be convened to consider all of the health inequalities including wider determinants and supporting the two public health leads in community asset and grass root approaches to the recommendations.
Dental outcome [55]
National and international research, summarised by the UK Health Security Agency (UKHSA) shows that people with learning disabilities have poorer oral health and more problems in accessing dental services than people in the general population. People with learning disabilities may often be unaware of dental problems and may be reliant on their carers/paid supporters for oral care, who are rarely trained for this and may not see oral care as a priority so not initiate dental check ups. Evidence consistently shows that people with learning disabilities have poorer access to dental services, less preventative dentistry so greater unmet oral health needs:
- higher levels of gum disease
- greater gingival inflammation
- higher numbers of missing teeth
- increased rates of toothlessness
- higher plaque levels [56]
Dental care is available from general dental practices (high-street practices) for all residents. Those who cannot be treated safely in general dental practice, because they need specialist skills or facilities, can access dental care from community dental service clinics. It is not known how many people with learning disabilities require specialist or indeed how many access either mainstream or specialist care. Feedback from carers to commissioners is that those with accompanying sensory needs (including those autistic people with learning disabilities) find the whole dental experience incredibly challenging. There is no performance data specifically on dental care for patients with learning disabilities as this data is not collected from patients. As such, there is no way of assessing the care given to dental patients with learning disabilities.
NHS commissioning bodies are responsible for NHS dental services – NHS England and NHS Improvement (NHSE/I) are working with Integrated Care Systems (ICSs) in the South-East to delegate commissioning responsibilities for dental services to ICSs. Currently the responsibility for commissioning dental services is transitioning from NHSE to Surrey ICB. Surrey ICB will work with local partners including Surrey County Council and NHSE to identify any amendments needed to ensure appropriate models of care for vulnerable groups.
Surrey and Sussex NHS Trust provide Special care dentistry to people including those with learning disabilities in Surrey. Together with dental specialty colleagues in their Oral & Facial Unit, they provide comprehensive dental advice and treatment, including sedation or general anaesthesia, including domiciliary care where appropriate. Assessment of patients generally takes place at East Surrey Hospital. Treatment is carried out at East Surrey and Caterham Dene Hospitals. They offer ongoing general dental care for those patients who need it long-term. GPs, dentists, community nurses or care workers can refer patients direct to this department. ‘HCRG Care Group’ offer the service that covers the west of Surrey [57]
Recommendation: As specialist dentistry commissioning becomes delegated to ICBs from NHSE/I, work needs to be undertaken to understand levels of access to dental care of people with learning disabilities and the challenges that may prevent access or lead to a poor experience, triangulating dental service data with that from general practice.
Postural care
People with profound and multiple learning disabilities often sit and lie in limited positions, leading to a high risk of body shape distortion which is not inevitable with the right equipment and positioning techniques helping to protect body shape [58]. Early intervention can prevent the need for surgery and 2018 government guidance recommended that NHS bodies should provide a service that recognises postural care issues and addresses them effectively. The 2018 government guidance recognised that physical, psychological and emotional effects of body shape distortion, and poor postural care can have severe and life-threatening consequences, including premature death. This was also noted in The Confidential Inquiry into premature deaths of people with learning disabilities (CIPOLD) which established the link between a failure to protect body shape and resultant premature death [59].
Postural care refers to ‘an approach that aims to preserve and restore body shape and muscle tone for people with movement difficulties’ and addresses all body positions that an individual adopts over the day and it usually involves a personalised 24 hour programme that includes [60].
- provision of adaptive seating
- positioning equipment to support the person in lying, including at night time
- moving and handling techniques
- advice and training for family carers and professionals across all settings
Respiratory problems are the main reason people with profound and multiple learning disabilities need primary or secondary medical care; pneumonia is the most common cause of death in this group [61]. Some of the risk factors for respiratory problems that can be reduced by good postural management are:
- airway clearance dysfunction
- saliva management difficulties
- immobility
- reflux
- sleep disordered breathing
- thoracic deformity
Other physical health problems associated with body shape distortion include [62]:
- problems with the musculoskeletal system, such as hip dislocation, contractures, curvature of the spine and reduced movement
- difficulties in swallowing and risk of choking
- constipation
- pressure on internal organs
- recurrent pressure sores
Such complications will cause discomfort and possibly severe pain. They will certainly have a negative impact on someone’s quality of life and can lead to emotional and psychological problems including fatigue, depression, isolation and feelings of helplessness.
Figures on how many people with learning disabilities who may require postural care are not available. However, the need for postural care usually occurs for people with profound and multiple learning disabilities. In an ‘average’ area in England with a population of 250,000 the Mansell Report ‘Raising Our Sights’ referenced that ‘researchers suggest this would mean that the number of adults with profound intellectual and multiple disabilities will rise from 78 in 2009 to 105 in 2026, and that the number of young people with profound intellectual and multiple disabilities becoming adults in any given year will rise from 3 in 2009 to 5 in 2026’. Given that the Surrey population is 1.19 million approximately we would expect the numbers to be 500 adults in 2026 increasing year on year as young people become adults by 24 in 2026 [63].
Data specifically on all age profound and multiple disabilities is not collated in Surrey and terminology varies between children and adults. Social care data offers the nearest proxy within adults. The data suggests a lower level of need than research evidence suggests [64].
Table 31: The number of people open to Adult Social Care in Surrey with a PSR and a PCC of physical disabilities or a PCC of learning disability and a PSR of either physical support – access and mobility only or physical support – or personal care support by district and boroughs, excluding unknown address
| D&B or OOC | Adults with Physical Disabilities |
| Elmbridge | 13 |
| Epsom & Ewell | 18 |
| Guildford | 30 |
| Mole Valley | 22 |
| Reigate & Banstead | 32 |
| Runnymede | 10 |
| Spelthorne | 16 |
| Surrey Heath | 16 |
| Tandridge | 17 |
| Waverley | 38 |
| Woking | 19 |
| OOC | 23 |
| Grand Total | 254 |
Numbers or totals may have been slightly altered to avoid disclosure on this or other tables
Figure 30: The number of people open to Adult Social Care in Surrey with a PSR and a PCC of physical disabilities or a PCC of learning disability and a PSR of either physical support – access and mobility only or physical support – or personal care support by district and boroughs, excluding unknown address
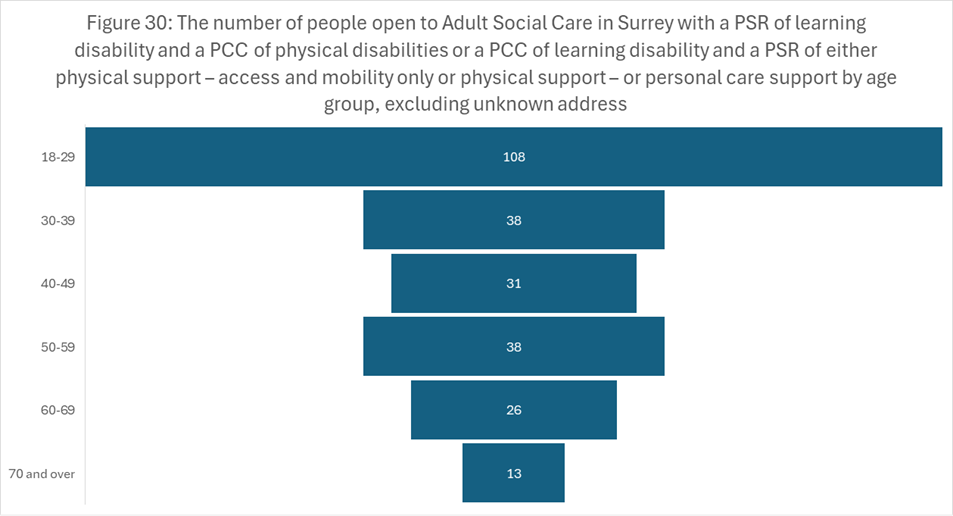
Source: SCC Adult Social Care, November 25
Numbers or totals may have been slightly altered to avoid disclosure on this or other tables
Data indicates there are 106 children and young people with an Education Health and Care Plan and a primary diagnosis of ‘Profound & Multiple Learning Difficulty’.
Table 32: Number of children and young people with an EHCP with primary need of profound and multiple learning difficulties, 2022/23
| Local Authorities | EHCP: Profound & Multiple Learning Difficulty | Total Number of EHCP plans |
| Surrey | 106 | 11,403 |
| Elmbridge | 10 | 1,259 |
| Epsom & Ewell | 6 | 724 |
| Guildford | 16 | 1,337 |
| Mole Valley | 7 | 805 |
| Reigate & Banstead | 14 | 1,524 |
| Runnymede | 9 | 834 |
| Spelthorne | 11 | 1,145 |
| Surrey Heath | <5 | 731 |
| Tandridge | 10 | 849 |
| Waverley | 9 | 1,267 |
| Woking | 10 | 928 |
Aspiration pneumonia accounted for 40% of deaths and pneumonia 10% of deaths in adults as reported in the 2021 LeDeR report. As a result, the LeDeR panel recommended a deep dive into Respiratory / Aspiration pneumonia deaths which include postural care considerations during 2022.
Recommendation: Given the importance of postural care, improved data tracking is required to inform commissioning intentions. This should include reference to postural care in any LeDeR or safeguarding reports.
Dementia and learning disabilities
It is forecast that between 2020 and 2030 the overall number of people with dementia is to increase by 28%, from 17,700 to 22,672. Dementia affects people with a learning disability at a younger age. People with learning disabilities aged over 60 are two or three times more likely to have dementia than the general population.
Combining the Frimley and Surrey Heartlands data, it is estimated that in Surrey there are around 135 people with a learning disability who have dementia. This triangulates with the data within NHS digital, however provider feedback is that these numbers appear low.
Table 33: The number of people with Dementia in Surrey, by age group, for people with a Learning Disability, Down’s syndrome and people without learning disabilities, 2023/24
| Age groups | Frimley ICB with a Learning Disability | Frimley ICB with Down’s Syndrome |
Frimley ICB without a Learning Disability |
Surrey Heartlands ICB with a Learning Disability |
Surrey Heartlands ICB with Down’s Syndrome |
Surrey Heartlands ICB without a Learning Disability |
| 18 to 24 | 0 | 0 | 0 | 0 | 0 | 5 |
| 25 to 34 | 0 | 0 | 0 | 0 | 0 | 10 |
| 35 to 44 | 5 | 0 | 0 | 0 | 0 | 10 |
| 45 to 54 | 10 | 10 | 15 | 10 | 10 | 15 |
| 55 to 64 | 20 | 15 | 95 | 30 | 20 | 105 |
| 65 to 74 | 15 | 10 | 525 | 15 | 10 | 800 |
| 75 + | 10 | 5 | 5,035 | 20 | 5 | 7,795 |
| Total | 60 | 40 | 5,670 | 75 | 45 | 8,740 |
Recommendation: Improved intelligence regarding dementia prevalence should be established, requiring joint work between health and care practitioners, commissioners, providers and the clinical lead. Data reports should include:
- reference to dementia in any LeDeR or safeguarding reports
- the number of people identified on the GP dementia register who have a learning disability or Down’s Syndrome and of those how many have had their dementia review
- the number of people identified on the GP LD register who have dementia and of those how many have had their dementia review
Figure 31: Proportion of Dementia cases for each age group in Frimley ICB and Surrey Heartlands ICB for people with a Learning Disability, people with Down’s Syndrome and people without learning disabilities, 2023/24
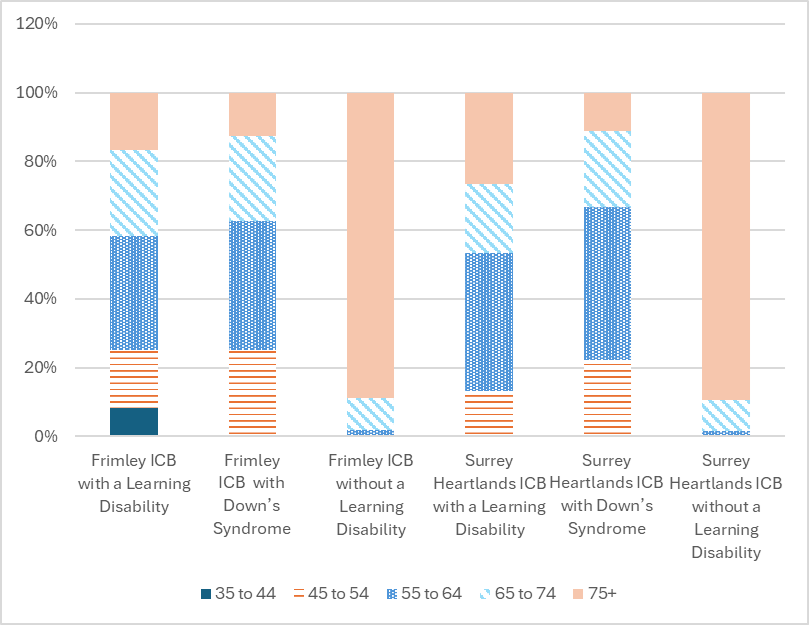
SABP operate a tailored dementia assessment, diagnostic and support service for individuals with Down’s syndrome. The service currently supports 54 adults with Down’s syndrome diagnosed with dementia and a further 32 adults with a learning disability.
There is a post diagnostic pathway for people with a learning disability that offers support to the person, their carers/ staff through to end of life, via a minimum of a 6-month brief review and an annual review, with other interventions including cancer screening programmes available as required.
The UK’s longest running (20+ years) Down’s Syndrome and Dementia longitudinal study includes a database of services for people with Down’s syndrome who develop dementia. This has had a major impact on clinical practice nationally and resulted in the development of a range of projects, including development of resources, Quality Outcome Measures and the publication of national guidance ‘Dementia and People with Intellectual Disabilities: Guidance on the assessment, diagnosis, interventions and support of people with intellectual disabilities who develop dementia published by the BPS (2009, 2015)’.
The Joint Health and Social Care Dementia Strategy for Surrey 2022 to 2027, available in easy read, identifies specific commitments, including the following that are particularly pertinent to this JSNA:
- Preventing Well: our aim is to continue to raise public awareness and activities around dementia and the actions people can take to prevent dementia
- By April 2022 we will ensure we have accessible material for people e.g., Easy Read or a video to enable people to access the information they require.
- Diagnosing Well: our aim is for people to have equal access to dementia care; understanding where communities may not be accessing dementia diagnosis and post diagnostic support. We will address the inequalities and gaps in service with partners to overcome barriers.
- By April 2022 we will increase access and uptake of baseline assessments for people with Down’s Syndrome.
- Living Well: our aim is to make sure everyone has the opportunity to live life to the full following diagnosis
- By June 2022 we will ensure accessible resources on dementia are available for people with a learning disability
- By November 2022 we will have a young onset dementia accommodation with support offer.
- By April 2023 we will have more dementia day support for those with young onset dementia
- Supporting Well: our aim is to engage with our communities …. to ensure we reach out to people with dementia and their carers
- By April 2023 we will improve the accommodation with care and support offer to have small scale specialist dementia residential and nursing care available to meet a range of needs.
- People with a learning disability and dementia may not have access to appropriate care if dementia care homes are not skilled in working with people with a learning disability. Similarly, care homes for people with learning disabilities may not be able to meet needs of their clients if they develop dementia. A person-centred approach should be taken, to allow different options as appropriate e.g., enabling with person with a learning disability to remain in their current home, with extra support if needed.
- Dying well: our aim is to make sure care is coordinated to enable the person with dementia to live their life as independently as possible until their death.
Recommendation: Data regarding prevalence of dementia among people with learning disabilities and Down’s syndrome and use of services must be included in strategic planning going forward under the Dementia Strategy.
People with learning disabilities and ageing
People with learning disabilities are living longer. It is estimated that by 2030, there will be a 30% increase in the number of adults with learning disabilities aged 50+ using social care services, with an estimated 164% increase in adults with learning disabilities over 80 using social care [65].
As can be seen from Table 3 (in the section around population projections) the number of people with learning disabilities aged 65+ in Surrey is estimated to increase between 2023 and 2040 from 4,977 to 6,458. Increased life expectancy intensifies the need for age-specific support, for example on falls and frailty.
Research evidence suggests the majority of determinants of health sit outside health services, and inequalities are the result of the interaction of several factors including increased rates of exposure to common ‘social determinants’ of poorer health (e.g. poverty, poor housing, social exclusion), individual lifestyle factors, barriers to accessing health care and experience of overt discrimination [66].
People as they age may also find themselves becoming carers of their loved ones including their parents, partner and friends and may not know that this brings access to a Carer’s assessment for example and may benefit from an emergency plan, the same as a carer without a learning disability [67].
Recommendation: The wider needs of ageing adults with learning disabilities needs system-wide consideration, building on specifically targeted pieces of work currently underway. This must include but not be limited to NICE health-based guidance and being supported in any caring roles.
Sensory Impairment
Visual impairment
Sight for Surrey, which is commissioned by Adult Social Care to provide services to people with sight and/or hearing loss and services to people who are deaf, has approximately 5348 people with visual impairment on their database. This includes people who are registered as severely sight impaired/blind and sight impaired/partially sighted. Most of the users of this service are aged over 65.
The number of people of working age adults with a visual impairment is expected to remain stable to 2030, but with a 39% increase in prevalence in those over 65. The anticipated 39% increase (from 17,070 to 26,300 people) by 2,030 of people over 65 with a moderate or severe visual impairment is likely to challenge current service provision both in terms of volume and structure.
The Public Health England Guidance ‘Eye care and people with learning disabilities: making reasonable adjustments’ states that:
- Adults with learning disabilities are 10 times more likely to have serious sight problems than other adults and children are 28 times more likely
- People with very high support needs are most likely to have sight problems. They may not know they have a sight problem, and may not be able to tell people – supporters, carers and teachers often think that people can see very well
- 6 in 10 people with learning disabilities need glasses and often need support to feel comfortable to wear them
- Adults should have an eye test every 2 years, sometimes more often, children should have an eye test every year
- Everyone can have a sight test, with the right support
- The biggest single cause of avoidable sight loss across the world is those with very poor eye sight not having glasses
The only data available about people with learning disabilities and eye care is on uptake of diabetic eye screening for diabetic retinopathy, which ranges from 50% to 65% across Surrey Heartlands ICS. Guildford and Waverley place had the highest level of uptake at 65%, followed by Surrey Downs (54%) and East Surrey 53%. The place with the lowest diabetic eye screening uptake was North West Surrey where only 50% of eligible people received the eye screening. National data indicates a much higher uptake within the general population of 80.8% in 2023/24 and around 80% for 2014 to 2019 [68].
Recommendation: Improved data relating to eye health and access to related services should be established, requiring joint work between health and care practitioners, commissioners, providers and the clinical lead.
Hearing loss
Sight for Surrey has approximately 1,398 people living with hearing loss on their database; this includes people who are Deaf and use British Sign Language. Most users of this service are aged over 65.
The number of people of working age with a profound hearing impairment will remain stable over the next 2 years (at some 250 people), with a 15% rise (313 people) in those ages over 65 to 3667 people. This includes people who are Deaf and use British Sign Language.
The numbers of adults with moderate or severe hearing impairment are much greater and the number will increase over the next 20 years at a higher rate.
Sight for Surrey also has approximately 1890 people living with combined sight and hearing loss on their database. [69]
Studies suggest around 40% (exact estimates vary) of adults with a learning disability experience moderate to severe hearing loss [70].
Recommendation: Improved data about hearing, hearing loss and hearing impairment and access to support for people with learning disabilities should be pursued.
Podiatry
The greater prevalence of foot disorders affecting people with learning disability compared with the general population means podiatry is an important offer to this group [71].
In Surrey podiatry services are provided via multiple community health services with varying criteria and there is currently insufficient data about access. There is a specialist LD podiatrist offer in the east of the county only. As of December 2022, they have a current caseload of 92 and a waiting list of 11 including some recent referrals from the West Community Team for people with learning disabilities.
Recommendation: Improved data about access to community podiatry services and the impact of there being a specialist podiatry offer in only half of the county should be pursued.
Sex, sexual health, sexual awareness and sexual expression
The World Health Organization specifies, “sexual health requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences” [72] [73]. Sexual expression, including the right to develop relationships and access sexual health education, is an inherent human right [74].
The wish for a private life including relationships and romance as well as having a child this was raised as important by the Surrey People’s Group who met in December 2022.
The Surrey Heartlands NHS Specification for sexual health services includes the requirement for reasonable adjustments for both people with learning disabilities and autistic people.
See also below in regard to pregnancy and LGBTQ+ recommendations in regard to intersectionality.
Recommendation: A greater understanding of the needs of people with learning disabilities regarding sexual awareness and expression, and access to services should be pursued.
Pregnancy care and outcomes
The national survey of adults with learning disabilities in England (2003/04) found that 9% of women with learning disabilities had a child (2005). There does not appear to be any further UK data on the number of women with learning disabilities who experience pregnancy and childbirth, or UK evidence regarding risk factors for poor pregnancy and birth outcomes for women with learning disabilities. [75] [76]
Research suggests that mothers with Learning Disabilities face the following inequalities:
- More likely to have their children removed and permanently placed outside the family home. [77]
- Higher risk of adverse outcomes, such as pre-eclampsia, low birthweight babies, and more frequent admission to neonatal intensive care. [78]
- Barriers to accessing antenatal care such as difficulties with transport, difficulty remembering appointments and understanding the purpose of the appointment. [79]
- Less satisfaction with their maternity care compared with non-disabled women, particularly interactions with staff. [80]
A qualitative study of the experience of maternity care for women with a learning disability found the following themes:
- desire for greater choice in their care
- need for accessible information and communication
- fear of being judged by professionals
- experiencing safeguarding as discrimination
- need for family and professional support. [81]
Across the four Trusts providing maternity care in Surrey, 3% of pregnant mothers are thought to have a learning disability, however this data is not consistently captured. Acknowledging wider challenges in case finding and under-diagnosis, the true proportion may be higher.
Our local priorities
Within the Surrey Heartlands Local Maternity System Five-Year Perinatal Equity Action Plan, women and birthing people living with a Learning Disability and/or Autism are included as a priority population cohort. Specific deliverables in the first year of the action plan, 2022-2023, are:
- Support Perinatal Mental Health teams to improve access for families with learning disability and autism. Research shows that mothers with autism are significantly more likely to experience both prenatal depression and postnatal depression.
- Use evidence-based, targeted educational materials to support reasonable adjustments.
- Use appropriate and accessible communications to ensure that parents with learning disabilities are aware of their rights, and the support they are entitled to (including from adult social care).
- Where appropriate, ensure links with transition services to provide joined-up support to prospective parents who may be transitioning between children and adult services.
- Support perinatal mental health teams to improve access and support for women and birthing people with a learning disability and/or autism.
- Link into system co-production forums, aimed at people with learning disability and autism and support provision of places for people with learning disability and autism to meet. It is key to hear the voices of service-users within this cohort to drive improvement and aid with the co-design of services.
Future years will focus on further embedding best practice and using captured reasonable adjustment data to support data-driven continuous improvement to accessibility. To measure success and inform data-driven improvement to our priority deliverables, metrics are included within the strategy.
Data is not available on the proportion of pregnant people with autism locally, however noting the national context of an increasing number of adults with autism (either due to late diagnosis, self-diagnosis, or childhood diagnosis), there is a need to ensure equity of access for this group.
As noted above there was very little available (including data) about the experience of people with learning disability being parents including fathers both nationally and within Surrey. The goal of becoming a parent was raised by people with learning disabilities at Surrey People’s Group Event 6th December 2022 (see also later in this document).
Recommendation: Data and insight about the number and experiences of parents within a learning disability will support the delivery of the local priorities identified above and needs to be sourced.
Access to health services
Supporting the access of people with learning disabilities to health care takes many forms within Surrey. This includes, from the NHS Long Term Plan (digital flag and NHS Improvement Provider Standards), various teams to support both those with learning disabilities and health professionals (e.g.) primary and acute liaison teams), dedicated specialist teams and the use of audit and support tools.
Within the NHS Long Term Plan, support to people with learning disabilities was included in chapter 3 (from 3.31). The chapter describes the commitment that the whole NHS will improve ‘its understanding of the needs of people with learning disabilities and autism, and work together to improve their health and wellbeing’ including:
- By 2023/24, a ‘digital flag’ in the patient record will ensure staff know a patient has a learning disability or autism (the work on this to date is referenced The digital flag)
- Over the next five years, national learning disability improvement standards will be implemented and will apply to all services funded by the NHS. These standards will promote greater consistency, addressing themes such as rights, the workforce, specialist care and working more effectively with people and their families.
Digital flag
Given the LTP commitment and the context of the Equality Act, Surrey recognised the requirement to provide reasonable adjustments enabling individuals to access care and treatment. As such Surrey became an Early Adopter of the Reasonable Adjustment Flag, to enable the coding and sharing of reasonable adjustment information with all partners.
The project enabled aspects of technical early adoption including SNOMED code development and developing drop down menus of reasonable adjustments as part of a phased trial linked to the wider digital development of the Surrey Care Record. Longer term work is currently being scoped.
NHS improvement provider standards
The NHS learning disability improvement standards have been developed with a number of outcomes created by people and families — which clearly state what they expect from the NHS. By taking this approach to quality improvement, it places patient and carer experience as the primary objective, as well as recognising the importance of how the NHS listens, learns and responds in order to improve care.
The four standards are:
- respecting and protecting rights
- inclusion and engagement
- workforce
- learning disability services standard (aimed solely at specialist mental health trusts providing care to people with learning disabilities, autism or both)
The standards are intended to help organisations measure quality of service and ensure consistency across the NHS in how we approach and treat people with learning disabilities, autism or both. They are prominent in the learning disability ambitions in the NHS Long Term Plan and included in the NHS standard contract 2019/20. We aim to apply the standards to all NHS-funded care by 2023/24. Each of the acute Trusts and the Mental Health Trust should have completed an annual assessment against the standards that can be used to drive improvements. These are:
- Royal Surrey Hospital
- Frimley Park Hospital
- Epsom General hospital
- East Surrey Hospital
- St Peter’s Hospital
- Surrey and Borders Partnership NHS Foundation Trust
The community health services have not previously completed an assessment but are planning to do so.
Recommendation: to consider using the outputs from all of The learning disability improvement standards for NHS trusts reports in strategic discussions to share good practice and reduce unwarranted variation across Surrey.
Recommendation: Ensure the community health services are offered support to complete The learning disability improvement standards for NHS trusts.
Access to primary care
The Learning Disability Primary Care Liaison Service offers support to adults with a learning disability age 18 and over who are registered with a GP in Surrey.
The team offer the following support to people who have a learning disability and family/carers:
- Generating and providing access to health information that’s easy to read
- Signposting to additional services as appropriate
- Promoting access to NHS screening programmes
- Encouraging participation in AHCs
The Learning Disability Primary Care Liaison Nurses offer the following support to primary care:
- Support to identify which of their patients have a learning disability.
- Provide learning disability awareness training opportunities to GPs and within the wider network
- Provide information and guidance on reasonable adjustments
- Provide advice on the Mental Capacity Act, best interest decisions and Independent Mental Capacity Advocates.
- Provide support and guidance on Annual Health Checks
The team offer time sensitive, intensive pieces of work for two weeks or less and if the intervention is likely to be longer, a referral to the Community Team for People with Learning Disabilities (CTPLD) can be made. They do not case hold.
The team work well within a tight and structured remit but are keen to develop further into ensuring annual health checks are booked, health action plans are good quality and actioned and complete more outpatient work with the acute hospital settings (especially for people not open to the community teams for people with learning disabilities), all of which will require further capacity. Further work is needed within community health to understand access and reasonable adjustments and this team would be well placed to progress this.
Recommendation: Data from this JSNA to inform the upcoming contract review of the specialist learning disability services including the primary care offer.
Access to acute healthcare
The Royal College of Physicians published an ‘Acute care toolkit 16 Acute medical care for people with a learning disability April 2022’ which made the following recommendations:
- Use primary care records / hospital alert system to help identify, on admission, all patients with a learning disability (see below about the ‘flag’).
- The clinical presentation of a person with a learning disability can be highly variable: multiple health conditions and polypharmacy are common at a young age, and people with a learning disability may die of common and preventable conditions. A specific focus on assessing and meeting the care needs of these patients is required.
- Professional uncertainty when faced with complex patients is common, and seeking help is wise and advisable. Use the hospital learning disability team as a resource in guiding decisions around care.
- Involve the person with a learning disability – and, where appropriate, their carers – in decision making as much as possible. Assess mental capacity for each decision.
- The patient is entitled to reasonable individualised adjustments in communication and care.
Hospital learning disability team
Surrey and Borders Partnership NHS Foundation Trust provide an acute liaison service for people with learning disabilities consisting of a number of nurses, including nursing associates, who work within an acute hospital across Surrey:
- Royal Surrey Hospital
- Frimley Park Hospital
- Epsom General hospital
- East Surrey Hospital
- St Peter’s Hospital
Their main focus and role is to ensure equal access for people with learning disabilities to acute services, and assessment in acute services regardless of presenting health needs achieved through a number of ways:
- Flagging – ensuring those with a registered learning disability are flagged on acute services digital records.
- Well co-ordinated care – supporting, monitoring and co-ordinating a learning disability inpatient/outpatient’s hospital visit throughout their hospital stay.
- Care pathways – we are often involved in developing care pathways with inpatient and outpatient services within the acute hospital, specifically for P learning disability
- Planned admission – supporting and co-ordinating planned admissions with inpatient/outpatient service
What they do:
- Discharge planning – supporting discharge planning involving all those involved in the individual’s care.
- Outpatients’ appointments – ensuring reasonable adjustments are in place, and that people with learning disabilities have the right support when accessing outpatient appointments.
- Preventing harm and monitoring incidents – monitoring, logging and reporting incidents identified within the acute hospital. To identify common themes experienced by people with learning disabilities and sharing with senior acute colleagues and the commissioners.
- Communication – ensuring people with learning disabilities have access to relevant health information, through use of easy read documents, interpreters etc.
- Understanding individual communication needs – ensuring individuals with a learning disabilities’ communication needs are understood and acknowledged when accessing inpatient/outpatient services.
- Patient passports – ensuring acute staff have access to hospital care passports and any other relevant documentation to enable them to have a good level of knowledge and understanding of individuals with learning disabilities who use acute services.
- Role of carers – ensuring Acute colleagues and care providers are aware of the role of the carer throughout people with learning disabilities’ hospital stay. Reviewed on a case-by-case basis depending on the presenting needs of the individual with a learning disability.
- Ward resource folder / Intranet resources – ensuring all acute services have access to useful learning disability resources, e.g. ensuring the acute intranet has useful learning disability resources that can be utilised.
- Consent and best interest decision making – supporting acute colleagues to ensure they follow MCA/BI guidelines.
- Mental capacity act – supporting the completion of capacity assessments and ensuring acute staff complete and record this accurately as per the MCA.
- Needs of people with a learning disability – completing person-centred support plans and risk assessments for individuals with a learning disability on a case-by-case basis.
- Communication – we support the person to communicate with those caring for them and liaise between them and their supporters. We create easy read information for patients to help them understand their health conditions and treatment plan.
- Resolution of disputes & Complaints – monitoring and logging of disputes and complaints from people with learning disabilities, and care providers.
- Signposting – signposting individuals with learning disabilities and acute colleagues to relevant services e.g. CTPLD, mainstream MH services, community therapists, social services etc.
- Induction and bespoke learning disability training – providing mandatory learning disability awareness training to a range of healthcare professionals in the acute setting, as well as providing bespoke learning disability training to specific inpatient and outpatient services.
As can be seen from the above, the team offer and cover the vast majority of the recommendations from the toolkit. Some hospitals have sought to extend the service offer further to make this all age/ inclusive of autism for example.
Recommendation: The findings of this JSNA to inform the upcoming contract review of the specialist learning disability services, include the acute liaison service.
The Acute Liaison service continues to support people admitted into hospital, whether that be a planned or urgent admission or as an outpatient appointment (Table 34)
Table 34: Acute liaison service support admissions, April – September 2021
| Month | Royal Surrey Hospital | St Peter’s Hospital | Frimley Park Hospital | Epsom General hospital | East Surrey Hospital |
| Apr-21 | 22 | 23 | 23 | 26 | 17 |
| May-21 | 23 | 19 | 31 | 26 | 18 |
| Jun-21 | 29 | 21 | 28 | 10 | 21 |
| Jul-21 | 36 | 28 | 17 | 11 | 17 |
| Aug-21 | 27 | 25 | 21 | 30 | 14 |
| Sep-21 | 26 | 29 | 18 | 8 | 25 |
| Total | 163 | 145 | 138 | 111 | 112 |
The following tables show the access to primary and acute care for people with a learning disability living within the Surrey Heartlands area of Surrey.
Table 35 shows the utilisation by people with learning disabilities spilt by user type (from healthy to high) of both acute and primary care. 21% of people with learning disabilities are ‘high’ or ‘very high’ users compared to only 7% of the general population.
Table 35: Resource utilisation band* for learning disability cohort, rolling 12 month snapshot by place; 11 November 2022
| Resource utilisation Band | East Surrey | Guildford & Waverley | North West Surrey | Surrey Downs | Grand Total |
| 1- Healthy users | 137 | 46 | 84 | 83 | 350 |
| 2- Low | 114 | 83 | 167 | 146 | 510 |
| 3- Moderate | 689 | 572 | 692 | 655 | 2,608 |
| 4- High | 235 | 179 | 177 | 167 | 758 |
| 5- Very high | 39 | 42 | 33 | 69 | 183 |
| Grand Total | 1,214 | 922 | 1,153 | 1,120 | 4,409 |
| % in high or very high band | 23% | 24% | 18% | 21% | 21% |
Source: Surrey Heartlands ICB
Table 36: A&E, inpatients and GP encounters for learning disability cohort, rolling 12 month snapshot by place; 11 November 2022
| Values | East Surrey | Guildford & Waverley | North West Surrey | Surrey Downs | Grand Total |
| Inpatient Activity | 119 | 247 | 231 | 154 | 751 |
| Inpatient Emergency | 24 | 48 | 86 | 86 | 244 |
| A&E Total | 452 | 131 | 317 | 441 | 1,341 |
| GP Encounters | 39,262 | 30,755 | 37,608 | 34,761 | 142,386 |
This is broken down by age and gender (Figure 32) across the Surrey Heartlands system and by place and ethnicity categories (Table 37):
Figure 32: The number of individuals with a learning disability accessing primary and acute care, by age and gender – 11 November 2022.
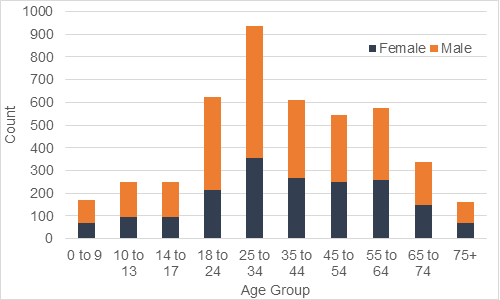
Table 37: The number of people accessing primary care or acute care by recorded ethnicity and place; 11 November 2022
| Ethnicity | East Surrey | Guildford & Waverley | North West Surrey | Surrey Downs | Grand Total |
| British | 952 | 706 | 792 | 716 | 3,166 |
| Refused or Not Stated | 81 | 57 | 59 | 100 | 297 |
| Any other group | 25 | 32 | 46 | 71 | 174 |
| Other White | 15 | 24 | 50 | 29 | 118 |
| English | 11 | 12 | 33 | 58 | 114 |
| Other White European | 21 | 21 | 12 | 20 | 74 |
| Pakistani or British Pakistani | 7 | <5 | 55 | <5 | 66 |
| Indian or British Indian | 10 | 6 | 19 | 13 | 48 |
| Other Asian including British Asian | 10 | <5 | 17 | 11 | 40 |
| (blank) | 5 | 9 | 6 | 16 | 36 |
| Any other white background | 6 | 7 | 10 | 9 | 32 |
| African | 8 | <5 | 8 | 10 | 30 |
| Other Mixed | 8 | <5 | 9 | 5 | 26 |
| Caribbean | 11 | <5 | <5 | 8 | 21 |
| White and Black African | 6 | 5 | <5 | 6 | 20 |
| Irish | <5 | <5 | 6 | 6 | 19 |
| White and Asian | 5 | 8 | <5 | <5 | 17 |
| Chinese | <5 | <5 | <5 | 5 | 16 |
| White and Black Caribbean | 6 | <5 | <5 | <5 | 15 |
| Bangladeshi or British Bangladeshi | <5 | <5 | 5 | <5 | 14 |
| Other Black in Black British | 6 | <5 | <5 | <5 | 13 |
| Any other ethnic group | <5 | <5 | <5 | 6 | 12 |
| Any other Asian background | <5 | <5 | <5 | <5 | 7 |
| Middle East | <5 | <5 | <5 | <5 | <5 |
| Turkish | <5 | 0 | <5 | <5 | <5 |
| Arab | 0 | 0 | <5 | <5 | <5 |
| Asian and Chinese | <5 | 0 | <5 | 0 | <5 |
| Any other mixed background | <5 | 0 | 0 | <5 | <5 |
| Chinese and White | 0 | <5 | <5 | <5 | <5 |
| Greek | 0 | 0 | <5 | <5 | <5 |
| Mediterranean | 0 | 0 | 0 | <5 | <5 |
| Any other Black background | 0 | <5 | 0 | <5 | <5 |
| Black and White | <5 | 0 | 0 | <5 | <5 |
| Welsh | <5 | 0 | 0 | <5 | <5 |
| Black and Asian | 0 | 0 | 0 | <5 | <5 |
| Africa- colour not defined | <5 | 0 | 0 | 0 | <5 |
| Scottish | <5 | 0 | 0 | <5 | <5 |
| Kashmiri | <5 | 0 | 0 | 0 | <5 |
| Grand Total | 1,214 | 922 | 1,152 | 1,120 | 4,409 |
Recommendation: More data is needed to understand the difference between people with and without learning disabilities and their use of primary and acute care to ascertain if there is inequity of access.
Recommendation: Further analysis of data related to access to services by people with learning disabilities to clarify the number of unique people represented as opposed to repeat contacts, as the data might not be representative of access across the whole population access).
Recommendation: Intervention is needed to improve recording of the ethnicity of people with a learning disability using primary and acute services to improve data quality and insight into need.
Finally, the data in Table 38 shows if the person accessing primary care or acute care is in a care home or not, by place. Frimley data will need to be sourced.
Table 38: The number of people accessing primary care or acute care if resident in a care home or not, by place; 01 November 2022
| Place | East Surrey | Guildford & Waverley | North West Surrey | Surrey Downs | Grand Total |
| Not residing in a care home | 806 | 649 | 957 | 765 | 3,177 |
| Residing in a care home | 408 | 273 | 196 | 355 | 1,232 |
| Grand Total | 1,214 | 922 | 1,153 | 1,120 | 4,409 |
| % residing in a care home | 34% | 30% | 17% | 32% | 28% |
Data for people accessing community health services is only available in totality and currently cannot be drilled down into access by people with learning disabilities
Recommendations: The following two sets of data are needed to understand community health service access for those with a learning disability Surrey wide:
- Data for those who live in Frimley.
- Data across the whole of Surrey for people with learning disabilities accessing community health services (which may need to wait until the roll out of the learning disability and autism Flag)
Specialist Health Care support
The Surrey and Borders Partnership Trust (SABP) Learning Disabilities Health services portfolio support people with a Learning Disability who are registered with a GP within Surrey and North East Hants and Farnham and are over the age of 18, where their primary need is for a specialist learning disability service. The services work in conjunction with other stakeholders to offer support and treat as appropriate.
To be eligible for services the following criteria applies:
- Significant impairments in intellectual functioning (IQ below 70)
- Significant impairment of social or adaptive reasoning. The person requires support to achieve their survival needs i.e. eating, drinking, planning, appropriate clothing for weather etc. and with social problem solving and reasoning
- Impairment of onset before 14 years old.
The Specialist Health service portfolio includes:
- Acute and Primary Care Liaison Services
- West Surrey and NE Hants CTPLD
- East Surrey CTPLD
- Intensive Support Service – (ISS) which includes the Intensive Support team in the Community and the Intensive Support beds in the Deacon Unit.
The Acute and Primary Care Liaison Services and Intensive Support Service including the Deacon are included here.
The Community Team for PLD are divided into two teams, the East and West. The services have 5 core functions based on the National Learning Disability Professional Senate recommendations which include [82]:
- Mainstreaming
- Specialist assessment
- Specialist intervention
- Intensive support
- Quality assurance
This is delivered via a large Multi-Disciplinary Teams working with individuals with a learning disability and a health care need for an episode of care. They offer direct clinical therapeutic support including groupwork, Positive Behaviour Support, autism diagnosis (where there is a health need), pre and post dementia diagnosis, joint working with the Intensive Support Service and the local inpatient specialist service, the Deacon. There is equity of service as far as possible across East and West Teams.
Since the pandemic:
- Leadership in both teams has changed
- There has been an increased numbers of referrals
- Referrals are triaged by all professional groups
- Waiting lists are reviewed every 12 weeks and referrals are risk assessed as part of this process.
As demonstrated below, referral rates for the Community Learning Disability Teams have increased year on year for the past 4 years.
Table 39: Number of referrals to the Community Team for people with learning disabilities, 2021 to 2024
| Year | Total number of referrals received by the CTPLD’s |
| 2021 | 1,845 |
| 2022 | 1,831 |
| 2023 | 1,971 |
| 2024 | 1,947 |
In October 2025, Surrey & Borders Partnership NHS Foundation Trust Adult Learning Disability Services received 182 referrals. This equates to 15 referrals per 100,000 registered population.
Whilst referral rates for the CTPLD’s have continued to rise, the intensive and joint work by both the CTPLD’s and the ISS has meant that the actual referral rates for the ISS have decreased as demonstrated in Table 40.
Table 40: CTPLD referrals over time.
| Period | Referral received | Admissions prevented | Placement maintained |
| April 2019- April 2020 | 85 | 78 (91%) | 68 (80%) |
| May 2020- February 2021 | 56 | 54 (96%) | 44 (78%) |
| April 2024- March 2025 | 67 | 53 (79%) | 56 (83%) |
Overall increasing referral rates and complexity of individuals is meaning that waiting times are increasing and learning disability health services are struggling to support people in as timely fashion as desired. Although waiting lists and risk are regularly reviewed and every attempt is made to support a person as soon as possible it is noticeable how much resource is required for many individual complex cases. Many care organisations are accepting to support individuals with complex needs but very quickly realise that they are unequipped to support in the appropriate way. Therefore, there is an immediate reliance on the learning disability health services to avoid any placement breakdown and identify how best to support the individual. Learning disability health services also support anyone who is registered with a Surrey or North East Hampshire GP, and many people are not commissioned/ placed by Surrey but come from neighbouring boroughs or counties.
Learning disability health services have positively attempted to adapt to these demands by streamlining their referral processes, introduced increased group work when appropriate and introduced time limited clinical sessions.
Access to the CTPLD by age is shown to be broadly representative of the GP learning disabilities register.
Following the first health inequalities report looking at data, a second was commissioned to consider other aspects including access to CTPLD’s, which is drawn out below.
Figure 33: Demographic breakdown by age of CTPLD service users against the Surrey learning disabilities register
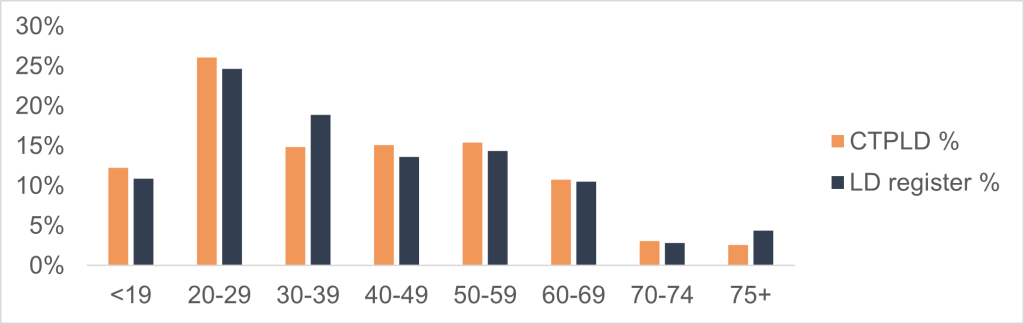
Analysis on age shows that the group of learning disabilities people served by CTPLD aligns closely to the age demographics of the learning disabilities register.
Access to CTPLD by sex is also broadly representative of the learning disabilities register.
Therefore, gender and age do not appear to be a barrier to accessing services.
Figure 34: Demographic breakdown by sex of CTPLD service users against the Surrey learning disabilities register
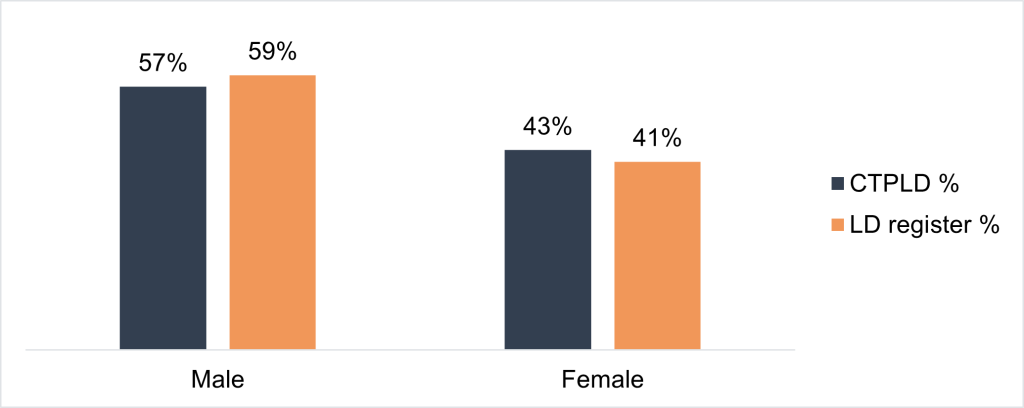
Engagements with CTPLD staff focused on challenges face by the service, of which themes around crisis management arose. A key insight was in relation to the volume of crisis management work. CTPLD tend to have the most impact with learning disabilities people living independently. These people tend to suffer from mental illnesses more often in relation to social impairment and isolation which over time can translate to crisis episodes. As a result, crisis management takes up the majority of CTPLD resources, leaving less opportunities to conduct preventative and proactive health management work.
Specific initiative undertaken to develop the offer include:
- Positive Behaviour Support has become more embedded as a Multi-Disciplinary Team pathway
- Neurodevelopmental pathway
- Service user feedback
- Healthy lifestyle group – joint group between dietetics and occupational therapy
- Increased our resource libraries for people we support e.g. meaningful engagement leaflet and COVID support videos
- Dementia training package developed
Future plans to develop the offer include:
- Increased partnership working with our Children’s services to ensure safe, effective transition between services
- Re-introduction of more in-person training packages
- Obesity Project to develop the work of the Healthy Life-Style group
- QNLD standards accreditation
- Digital referral forms
- Accessible Care Plans – outcomes, feedback from individuals and support network
- Obesity projects with SABP Health Tech team and Convenor as part of the Whole System Approach to Obesity for people with learning disabilities
See previous Recommendation: Data from this JSNA to inform the upcoming contract review of the specialist learning disability services
Mental health and outcomes, including inpatient admissions
Prevalence
Evidence suggests that mental health problems may be higher in people with a learning disability than in those without a learning disability. The estimated prevalence of mental health disorders range from 15% to 52%, depending on the diagnostic criteria used [83].
Applying these research statistics to the prevalence numbers of 23,019 adults in Surrey with a learning disability (including 50% with autism), the number with mental health disorders ranges between 3,453 to 11,510 [84] .
Local data is regarding diagnosis of severe mental illness available through the patient coverage by Integrated Care System. For Surrey Heartlands ICB there was 89.33% coverage and 94.45% coverage for Frimley ICB and suggests a significantly higher prevalence of severe mental illness among the adult population with a learning disability compared with people in the general population.
Figure 35: Percentage of patients in Surrey Heartlands ICB with a diagnosis of severe mental illness as at 31 March 2024, by age band
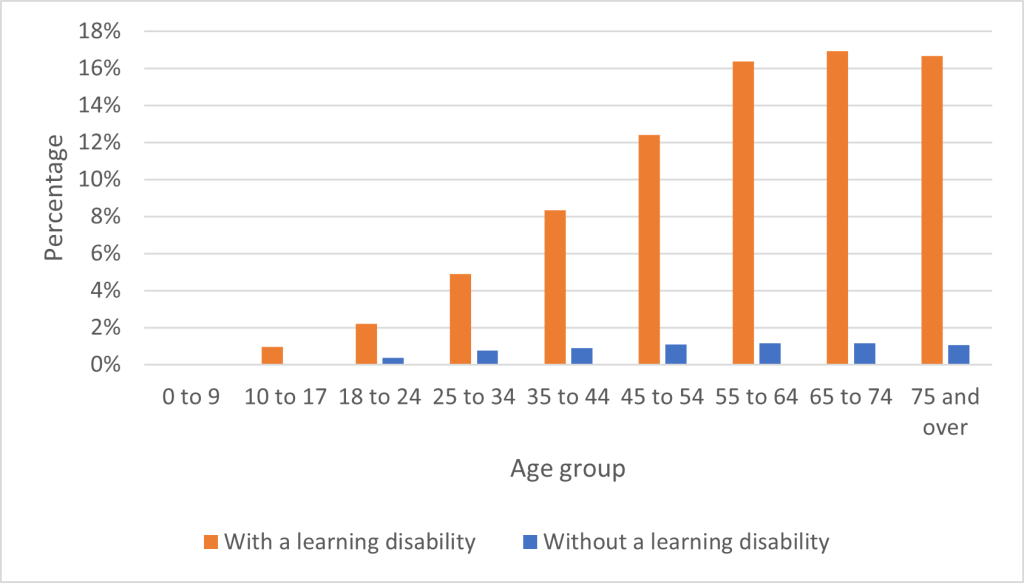
Figure 36: Percentage of patients in Frimley ICB with a diagnosis of severe mental illness as at 31 March 2024, by age band
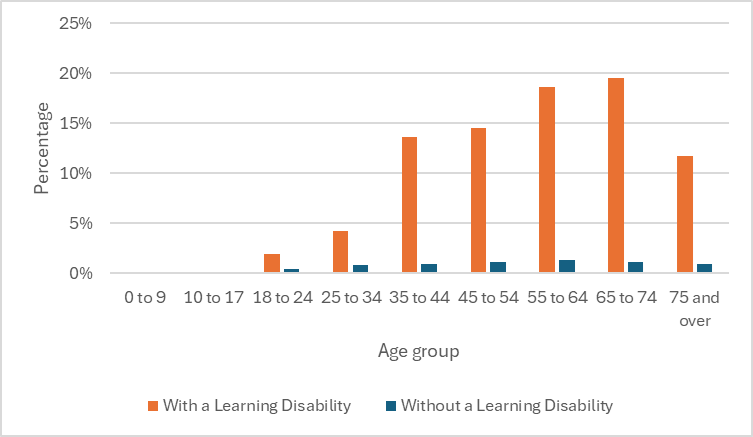
People with a learning disability can access either mainstream mental health services or if their needs are more specialist, they can access the psychologists within the CTPLD as well as a range of other therapies including art, drama and music therapy.
The West CTPLD has seen a steady continual flow of external referrals since 2020. The East has seen a doubling of the waiting list prior to COVID-19 due to staff loss, but with intensive working the waiting times are being managed.
The psychologists within the team also complete ‘unseen’ work in supporting colleagues in other disciplines with named individuals and complex risk.
There is currently no data including reasonable adjustments for people accessing mainstream mental health services who have a learning disability – this would typically be gathered and monitored and improved using the Green Light Toolkit. The goal of the Green Light Toolkit is to support mental health services as they work on improving their response to three groups of people. The three groups are:
- People with learning disabilities
- Autistic people
- Autistic people who have learning disabilities.
People in each of these three groups have the same rights to good care from mental health services as any other citizen which they do not always get.
The Green Light Toolkit has a long history. The 2022 version has been comprehensively updated to reflect changes in understanding, policy and practice.
This is not a tool in current use in Surrey and as a result we have very little insight into access and reasonable adjustments in mental health services.
Recommendation: Urgent consideration to be given for the roll out of the Green Light Toolkit by the six-monthly Strategy group within Surrey.
STOMP and STAMP (STopping Over Medication of people with a learning disability, autism or both with Psychotropic medicines)
The purpose of the STOMP programme is to help people to stay well and have a good quality of life. Surrey Heartlands ICS funded a Specialist Pharmacist to provide a medicines optimisation service to care homes for people with learning disability who identified STOMP as a priority to implement. ‘STOMP- learning disability’ aimed to implement Specialist Pharmacist led STOMP- learning disability medication reviews in primary care residential homes within Surrey Heartlands.
The study concluded that deprescribing can be completed in primary care without the need for referral to secondary care. A proposed integrated model of delivery of screening in primary care, with specialist pharmacist support to review and deprescribe, could ensure better use of time and is in line with recent mental health transformation plans. This requires multiple stakeholder involvement, planning, time, resources, and alternative support to implement successfully.
STAMP stands for Supporting Treatment and Appropriate Medication in Paediatrics. Work on STAMP has paused pending resources.
Recommendation: Consider resource requirements for STAMP.
Recommendation: Consider increasing training in primary care for STOMP/STAMP
Recommendation: Consider models of social support offered to patients and families while stopping medications (e.g. as stopping some of these medications might result in decreased sleep and increased behaviour that challenges and so shouldn’t be left unsupported)
Inpatient use
Those experiencing mental ill health are at risk of admission to inpatient settings for treatment including where the challenging behaviour maybe an expression of mental ill health (please see section challenging behaviour).
The NHS Long Term Plan (2019), Chapter Three, sets the NHS’s priorities for care quality and outcomes improvement for the decade from 2019 which includes people with learning disabilities living fulfilling lives in the community with reduced reliance on inpatient provision:
- By March 2023/24, inpatient provision will have reduced to less than half of 2015 levels (on a like for like basis and taking into account population growth).
- For every one million adults, there will be no more than 30 people with a learning disability and/or autism cared for in an inpatient unit.
- For children and young people, no more than 12 to 15 children with a learning disability, autism or both per million, will be cared for in an inpatient facility.
- For Surrey Heartlands that inpatient 2023/24 target is 24 adults (at 30 per million population) and 3 children (at 15 per million).
- Surrey Heartlands has a total of 2 Children / Young People in inpatient settings and a total of 21 Adults in inpatient settings as of October 2022 both of which are below the 2023/24 targets.
- 6 out of 42 integrated care systems (ICSs) have already met the 2023 to 2024 NHS Long Term Plan target. We are one of those currently.
A deep dive was completed in Surrey Heartlands to inpatient use up to the end of Quarter two 2022 which indicated the following:
Adults
- There are 7 adults in Integrated Care Board commissioned beds, typically beds for treatment of mental illness (including Specialist Learning Disability and working age adult Mental Health Units)
- Year to date activity indicated 9 admissions and 16 discharges
- This includes people with learning disabilities, people with learning disabilities and autism and autistic people (numbers)
Children
- There are less than 5 children/ young people in Integrated Care Board commissioned beds via the Children and Young People Tier 4 Provider Collaborative hub
- Year to date activity indicated less than 5 admissions and discharges
Preventing admissions
There are a number of ways the Surrey system works to prevent unnecessary admissions.
Dynamic Support Register
There is a requirement for integrated care boards (ICBs) to develop and maintain registers to identify people of all ages with a learning disability, autism or both who display, or are at risk of developing, behaviour that challenges or mental health conditions who were most likely to be at risk of admission.
As with most systems the Surrey Dynamic Support Register took the form of a spreadsheet which was agreed as suboptimal, and we have developed a digital Dynamic Support Register with digital partners and Kent ICB colleagues. We are currently in the mobilisation stage of the digital register.
Integrated Intensive Support Service
The Integrated Intensive Support Service (or ISS) was formed in late 2016 in line with guidance from NHS England and Transforming Care principles.
This is a multi-disciplinary team that works in the community, as well as in the specialist inpatient setting, the Deacon Unit. The aim is to:
- Prevent hospital admission
- Prevent placement breakdown
- Reduce length of stay within inpatient settings
- Place the person at the centre to maintain human rights, dignity and compassion
- Work flexibly across ISS and Assessment and Treatment Unit and across roles
- Work closely as a team, sharing expertise and reaching joint decisions
- Work closely with the Community Team for People Learning Disabilities who continue to provide care co-ordination
The service is not a seven-day specialist multidisciplinary service or crisis care offer, as indicated in the NHS long term plan.
Table 41: The intensive support service statistics 2021/22
| Period | Referrals Received | Admissions Prevented | Placement Maintained |
| April 2021-March 2022 | 69 | 56 (80%) | 62 (89%) |
Recommendation: Consideration in the ISS contract review as to whether there is a need for a seven-day specialist multidisciplinary service or crisis care offer
LAEP meeting and Care (education) and treatment reviews
Surrey has also implemented Local Area Emergency Protocol or ‘LAEP’ meetings which can stop people needing to go to a specialist hospital quickly and are usually held when there isn’t time for a Care and Treatment review.
Care (education) and treatment reviews (C(E)TRs) are part of NHS England’s commitment to transforming services for people of all ages with a learning disability and autistic people. C(E)TRs are for people who have been admitted to a mental health hospital or for people who are at risk of admission. They are undertaken by commissioners to ensure that people are only admitted to hospital when absolutely necessary and for the minimum amount of time possible. Care and Treatment Reviews (CTRs) are for adults and C(E)TRs are for children and young people.
Within Surrey, the C(E)TR process within 2022 supported in the avoidance of 10 plus admissions and only under 5 led to admissions.
Future considerations for C(E)TRs:
- BTRS action plan chapter one ‘Keeping people safe and ensuring high-quality health and social care’ proposes that recommendations from C(E)TRs, which are carried out within a set period of time after admission, are placed on a statutory footing (commitment 1c). This will mean that responsible clinicians must have regard to recommendations and include them in those patients’ care and treatment plans, unless there are good reasons not to do so.
- There will also be duties on the relevant ICB to have regard to recommendations that relate to services that may be available on discharge, unless there are good reasons not to do so. In chapter ‘2. Making it easier to leave hospital’, plan sets out how this will make it easier for people to leave hospital and ensure that discharge is considered from the outset of planning care and treatment.
The new guidance was published 30 January 2023 to enable systems to prepare for the changes for full implementation by 01 May 2023.
Recommendation: An analysis of the changes to the guidance (now called ‘Dynamic support register and Care (Education) and Treatment Review policy and guide’) to be completed to ensure readiness for implementation by 01 May 2023.
Future considerations for proposed Mental Health Act changes
Chapter 5. of Building the Right Support (BTRS) action plan is ‘Working with changes to the system’ and includes Commitment 5a: Proposal to limit the scope to detain people with a learning disability or autistic people under the Mental Health Act, as part of work to reform the Mental Health Act.
The Government published a white paper on ‘Reforming the Mental Health Act’ on 13 January 2021 containing proposals to reform the Mental Health Act 1983 (as amended in 2007) in England and Wales. The Government subsequently responded to the consultation on the white paper proposals details of the draft Mental Health Bill, published in June 2022, including the inclusion of most of the review 150 recommendations. The Queen’s Speech in May 2022 included an announcement on draft legislation to reform the Mental Health Act. Lord Kamall, The Parliamentary Under-Secretary of State for the Department of Health and Social Care stated that scrutiny would “commence at the earliest opportunity” and the government’s ambition is “to introduce the Bill in the new year on 28th June 2022.
Within the draft Bill are several amendments to the Mental Health Act 1983 it is stated that autism and learning disability would not be considered to be conditions for which a person could be subject to compulsory treatment under section 3. The BTRS action plan states that this is because learning disabilities and autism are conditions that cannot be removed through treatment, although some autistic people and people with learning disabilities may, at times, require treatment for a co-occurring mental illness. Under the proposals, people with a learning disability and autistic people could be detained for assessment under section 2 of the act when their behaviour is so distressed that there is a substantial risk of significant harm to self or others (as for all detentions). The maximum time somebody can be detained under section 2 is 28 days. They will only be able to be detained for treatment under section 3 of the act if a mental health condition that would benefit from hospital treatment is identified. If no mental health condition is identified, then detention will end.
Recommendation: Ensure the impact of the proposed changes to the Mental Health Act outlined in the BTRS Action plan are understood, actioned and planned for including any impact on community accommodation and support and inpatient offer.
Keyworking
The keyworking function has been developed as a response to the NHS England & NHS Improvement Long Term Plan (LTP) commitment that by 2023/24, children and young people with a learning disability, autism or both, with the most complex needs will have a designated Keyworker. Initially, Keyworker support will be provided to children and young people with learning disability, autism or both, who are inpatients or at risk of being admitted to hospital, but it is envisaged that support will also be extended to those who face multiple vulnerabilities such as looked after and adopted children, and children and young people in transition between services.
Surrey Heartlands ICB keyworking service will be offered to children and young people aged 0 to 25 who have Learning Disabilities and / or Autism, with the most complex needs and those who are either at risk of admission or residing in Tier 4 inpatient beds. It will also include those at risk of placement breakdown (school, family or residential placement). Those deemed ‘at-risk’ will be identified as red or amber on the dynamic risk register and assigned a designated keyworker.
The purpose of the keyworking function will be to help families and young people navigate existing social and healthcare services whilst providing personalised care solutions working at a neighbourhood or place level.
The service will be co-terminus with Surrey County Council and will therefore be jointly mobilised with Frimley ICB. System Host agreed to be Children with disabilities under s75 agreement with Surrey County Council.
The Digital Dynamic Risk Register will become the main referral source.
The service is expected to go live in Quarter two of 2023.
Quality of inpatients
The long-term plan also reiterated the need for quality assurance of any inpatient admission. Quality performance metrics relating to the level of performance for mechanisms in place to monitor the quality of care within inpatient settings (Care and Treatment Reviews, 6-8 Week Oversight visits) are collated and reported monthly into the regional NHSE team. ‘Safe and Wellbeing reviews’ were introduced in 2021/2022. Safe and wellbeing reviews were for everyone who was an inpatient on the 31 October 2021 who had a learning disability and any autistic person with or without learning disabilities of all ages and were a national action following the publication on the 9 September 2021 by Norfolk Safeguarding Adults Board (NSAB) of the Safeguarding Adults Review (SAR) into the deaths of three adults with learning disabilities who had been patients at Cawston Park Hospital, an assessment and treatment unit. During the latter part of 2021 and during early 2022, Safe and Wellbeing reviews and the panels to consider the reviews took place.
The Government published a white paper ‘Reforming the Mental Health Act’ in early 2021 containing proposals to reform the Mental Health Act 1983 (as amended in 2007) in England and Wales. The draft Bill proposes several amendments to the Mental Health Act 1983 that directly relate to people of all ages with a learning disability and/or autism, the key message is that both autism and learning disability would not be considered to be conditions for which a person could be subject to compulsory treatment under section 3, I.e. they must have a co-occurring mental health condition in order to be subject to treatment under the Act. A summary can be found in Appendix 6 under resources.
The deep dive completed in regard to inpatient use up to the end of Quarter two 2022 also indicated the following about quality metrics:
- 100% of repeated C(e)TRs were completed on time for those in CYP and ICB commissioned adults settings
- 100% of CYP oversight visits were completed
- 91% of adults commissioned by the ICB oversight visits were completed
Safe and well being review findings
The thematic findings of the safe and well being reviews are included as an appendix. They include good and poor practice identified and thematic review findings regarding a number of areas. The results of the reviews can be found in Appendix 4.
Local inpatient provision
The Deacon unit is a 10 bedded inpatient service for people with a learning disability who require crisis mental health support and is located at Epsom at the St Ebba’s site which operates Surrey wide. 7 beds are block funded for people registered with a GP in the Surrey and North East Hampshire area.
The Service provides seven beds for people registered with a GP in Surrey and North East Hants. It has separate male and female areas to offer 2 gender specific beds away from the other 5, three therapy rooms including a calming zone with a large, wall mounted interactive communication screen and a large garden to the rear and side garden with sunken trampoline. The inpatient pathway includes:
- Physical Health Checks with 24 hours of admission
- Admission Meeting within 7 days of Admission.
- Discharge date set during the admission meeting.
- Access to advocate including the Independent Mental Health Act advocate, Independent Mental Capacity Assessment
- Weekly clinical review
- Therapist Inpatient Pathway
- Case Team Allocation.
- Formulation Meeting
- Placement Specification & ‘All About Me’
- Care and Treatment Review
- Discharge Planning Meeting
Between January and December 2021 there were 5 admissions with an average length of stay of 8.5 months.
People with learning disabilities also can access 9 (approx. given changes) mental health working age adults units within Surrey for which we are host commissioner and, in some cases, out of area beds.
Host Commissioner guidance was published in February 2021. Across England ICSs have now identified a host commissioner for relevant units and identified any specialist mental health inpatient unit, which provides care that is commissioned by ICSs, to people with a learning disability, autism or both. This includes both NHS and Independent Sector provision of Assessment and Treatment Units, Long-Term Rehabilitation Units, and other specialist inpatient units (these may be units that also deliver care to individuals with complex needs, or mental illness).
The Host Commissioner Guidance emphasises the importance of Host Commissioners taking a proportionate and appropriate response to quality/safety issues raised and recommends, utilising the local System Quality Groups (formally Quality Surveillance Groups) to determine appropriate levels of surveillance for inpatient services. This process should be used for NHS and Independent Inpatient providers.
For people in all types of inpatients settings the following community requirements have been collated to enable discharges (both ICB and Provider collaborative commissioning inpatients)
Discharge commissioning arrangements
As of October 2022, there were 22 adults in inpatient settings, 20 of the 22 adults will require Section 117 After Care, these packages of care will be funded on a 50:50 basis. Less than 5 will be commissioned by social care.
Accommodation, care and support needs:
- 14 will require supported living arrangements
- 7 will require supported living and additional support of 1: and above
- Less than 5 will require single accommodation
- 6 can be immediately identified for “Move on accommodation”, others in the medium term. There is a lack of appropriate accommodation in Surrey.
Community Health Service and Social care teams requirements:
- 10 individuals will require support from the Forensic outreach and liaison mental health service provided by SABP, commissioned by the KSS Provider Collaborative. These individuals will receive support from the Specialist Services Social Care team. These teams may need further expansion, to meet the demand
- Less than five will require support from Community Mental Health Teams and the Learning Disability and Autism Social care Team. These individuals have Autism and ongoing mental health needs. Currently there is no community or crisis response service that are able to respond flexibly in the community. (i.e. Community Mental Health Recovery Services & Home Treatment Team for those with Mental Health or CTPLD & Intensive Support Service for those with learning disability and autism). Service enhancements are required but currently impacted by the lack of long-term funding as learning disability and autism service development finding is currently non-recurrent.
- 8 will require support from the CTPLD and the Learning Disability and Autism Social care Team
See prior recommendation on community/ 24/7 crisis response
Wider determinants
As part of the Surrey Health and Well Being Strategy (Surrey Health and Well-being Strategy – update 2022 | Healthy Surrey), Surrey will remain focused on three interconnected priorities supporting people to lead physically healthy lives, have good mental health and emotional wellbeing, and creating the contexts in which individuals and communities can reach their potential with a clearer intent on addressing the wider determinants of health. These priorities adopt a primary prevention (stopping ill health in the first instance) and secondary/tertiary prevention (making sure things don’t get any worse) approach, and focus on providing the right physical, psychological, social and economic contexts for communities that experience the poorest health outcomes to begin to thrive [85].
Map 5: Indices of multiple deprivation in Surrey by LSOA, 2019
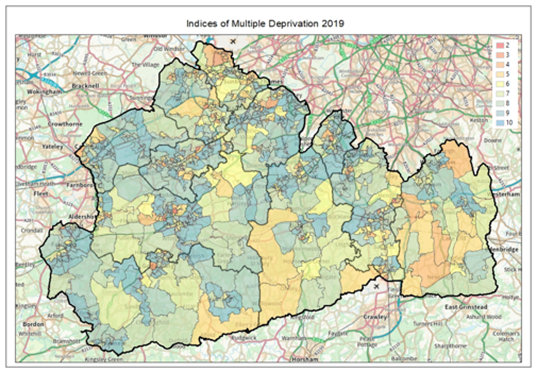
1 = most deprived, LSOA= Lower Super output area
There is a Surrey context chapter of the JSNA for further information: The Surrey Context: People and Place – Surrey-i (surreyi.gov.uk).
Poverty and Health
A follow up report to the aforementioned health inequalities report was commissioned in 2022 to improve understanding and mitigation of the causes of long-term health inequalities faced by people with learning disabilities through the lens of deprivation as well as living circumstances. The overarching question which informed the analysis was:
What is the impact of deprivation and living circumstances on the health inequalities faced by people with learning disabilities, and how could Surrey Heartlands better intervene to combat these inequalities?
Key findings, related to deprivation, living circumstance, rural vs urban environments, and the specialist health offer, the Community Team for people with learning disabilities, are summarised as follows:
- People with learning disabilities from the most deprived deciles suffer notably worse outcomes for smoking, diabetes and vaccination rates as compared to those from the least deprived.
- For every 1% increase in the proportion of students who leave education at 16 in the area covered by a particular GP, people with learning disabilities are 0.86% more likely to be unvaccinated.
- For every kilometre more rural an area in which a person with learning disabilities lives, the probability of them being overweight decreases by 1.7%
- For every kilometre further a person with learning disabilities lived from a fast-food outlet, the probability that that person was overweight decreased by approximately 1%.
- People living in some form of residential care would be more likely to receive an AHC and less likely to engage in potentially risky behaviour such as smoking.
- Analysis on age and gender shows that the group of learning disabilities people served by CTPLD aligns closely to the age demographics of the learning disabilities register.
Two public health leads have been recruited to address the recommendations from this report and the Health Inequalities report.
Surrey County Council published a Cost of Living Directory of Support posted both online and in paper copy across Surrey from the 31 October 2022. This is designed to help people all across Surrey who are feeling the impact of the Cost of Living crisis, by pulling together all the financial and welfare advice on offer in the county.
Recommendation: Further analysis to understand the impact of deprivation including food and fuel poverty is needed.
Accommodation
The Building the Right Support: action plan 2022 includes a chapter on ‘Living an ordinary life in the community’. This plan and chapter are specific to building the right support in the community to reduce reliance on inpatient care in mental health hospitals for children, young people and adults with a learning disability and for autistic children, young people and adults. The commitments within the chapter are:
- Commitment 3a: Embed strategic commitment in all local areas to connect housing with health and care, increase local expenditure on support services and boost supply of supported housing.
- Commitment 3b: Capital funding programmes underway to incentivise new supply of specialist and supported housing.
- Commitment 3c: Commissioning independent research to understand the size, cost and demand of the supported housing sector, including that which meets the needs of people with a learning disability and autistic people.
- Commitment 3d: Provide funding to local areas to deliver the Disabled Facilities Grant.
- Commitment 3e: ADASS, LGA and the Building the Right Support Advisory Group to identify ‘what good looks like’, which will be followed by a report that includes best practice examples, with an emphasis on initiatives that support citizenship and human rights.
- Commitment 3f: NHSE, along with a range of partners, commit to continuing to roll out a programme across England that enables the development of small (supporting less than 30 people with a learning disability and autistic people) community-driven organisations to deliver high-quality, bespoke support wrapped around an individual that promotes choice, control, human rights and citizenship.
- Commitment 3g: Continue to commission funded peer reviews. The programme involves a small group of peers spending time in another area as ‘critical friends’ to support an area to develop and improve service delivery. This process involves a wide range of stakeholders, including people with personal experience, and reflects to the system where they need to focus attention.
An analysis of performance against these commitments is underway within Surrey which should be completed by quarter 4 in 2023.
Accommodation Status
The Adult Social Care outcomes framework has a target of 75% in settled accommodation.
Table 42: The number of people open to Adult Social Care in Surrey with a Primary Support Reason (PSR) or Primary Client Category (PCC) of learning disability by District & Boroughs, excluding unknown addresses, by accommodation status
| D&B or OOC | Settled | Unsettled | Not known |
| Elmbridge | 9 | 8 | 284 |
| Epsom & Ewell | 19 | 34 | 206 |
| Guildford | 12 | 33 | 377 |
| Mole Valley | 18 | 42 | 243 |
| Reigate & Banstead | 21 | 80 | 560 |
| Runnymede | 6 | 22 | 225 |
| Spelthorne | 5 | 10 | 264 |
| Surrey Heath | 5 | 25 | 251 |
| Tandridge | 6 | 36 | 261 |
| Waverley | 15 | 73 | 391 |
| Woking | 5 | 36 | 295 |
| Outside Surrey | 22 | 354 | 189 |
| Total | 143 | 753 | 3,546 |
Numbers or totals may have been slightly altered to avoid disclosure on this or other tables
Map 6: People with learning disabilities funded by Adult Social Care living in residential care, supported living, or living alone or with family / friends summarised by 2025 ward boundaries
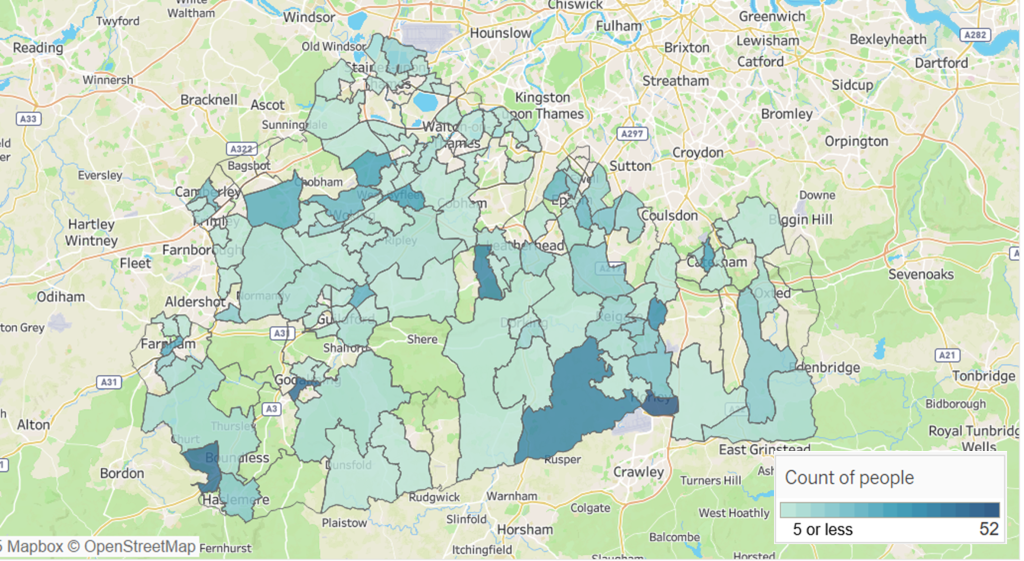
*excludes people with an unknown status or address. Includes only people living within Surrey
Figure 37: Proportion of working-age adults (18 to 64 years) with a learning disability who live in stable and appropriate accommodation, National, Regional and CIPFA nearest neighbour comparison – 2020/21
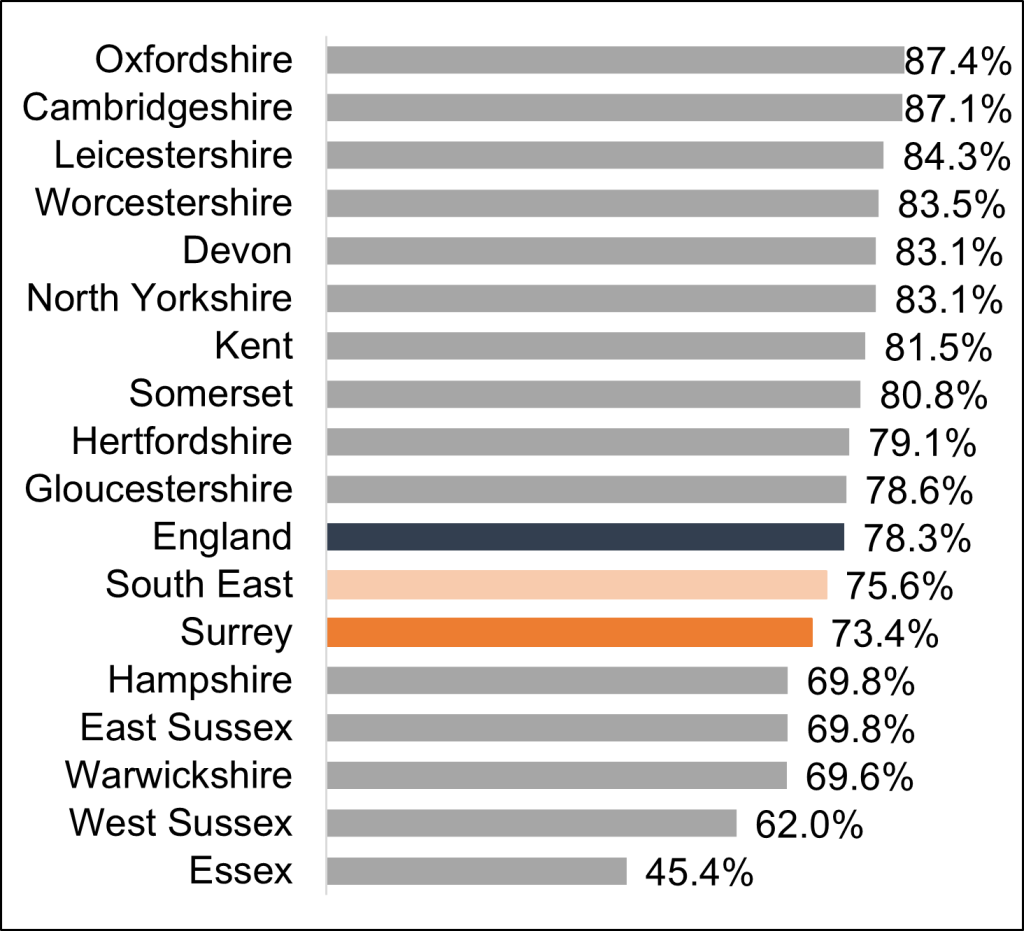
Source: Public health profiles – OHID (phe.org.uk)
Surrey’s action to improve performance
A 5-year Accommodation with Care and Support Strategy is underway in Adult Social Care from 2020-25. The strategy aims to reduce the numbers of people with learning disability and/or autism within institutionalised residential care by 40-50% over the next 5 years. This strategy involves not only the local care market but the 11 District and Borough Council Housing Departments in Surrey working collaboratively to develop Supported Independent Living housing.
Progress to date:
- In October 2019 there were 987 people in residential services.
- In February 2021 there were 961 people in residential services.
- In February 2022 there were 918 people in residential services.
- In December 2022 there were 867 people in residential services.
Employment
The Adult Social Care outcomes framework has a target of 19% of people with learning disabilities in employment or volunteering. The number of adults with a learning disability receiving long-term support from their local social services department who are in paid employment 2019/20, national, regional and CIPFA nearest neighbour comparison:
Figure 38: Percentage of supported working age adults with learning disabilities in paid employment, National, Regional and CIPFA (Chartered Institute of Public Finance and Accountancy) nearest neighbour comparison 2019/20
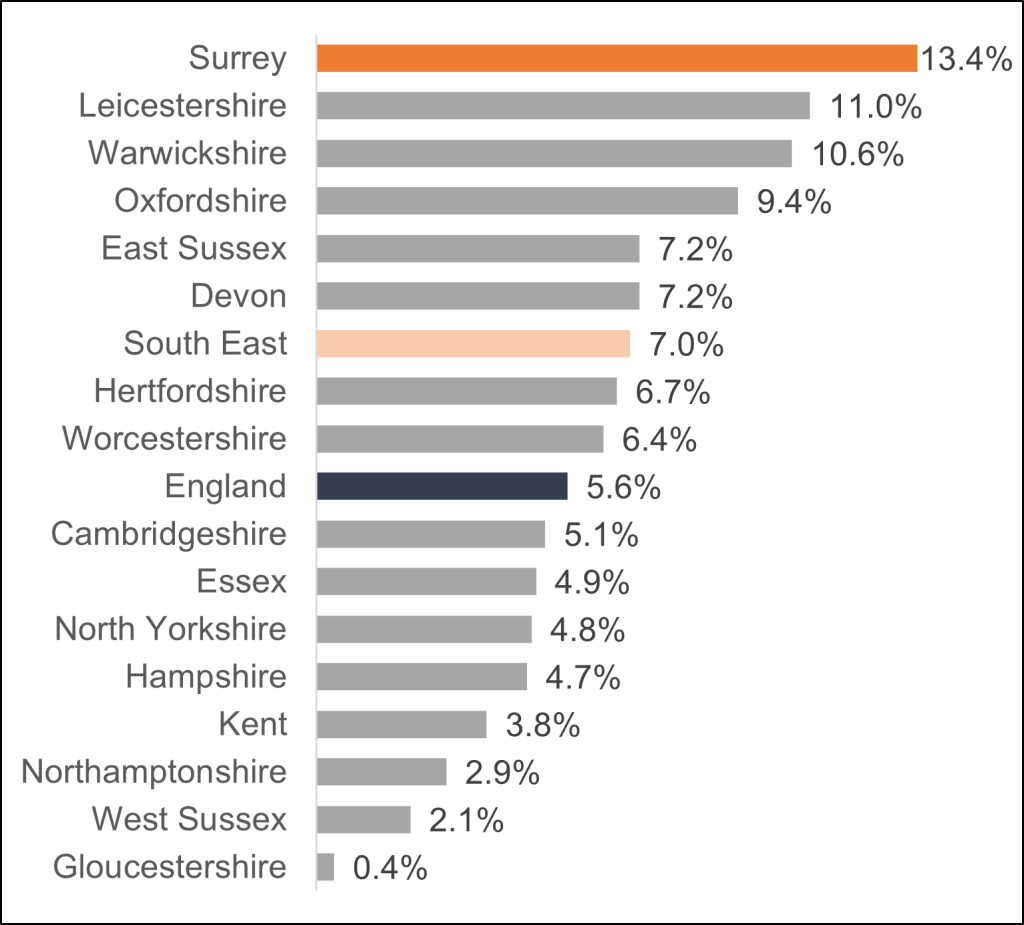
The trend shows that Surrey saw a general increase in employment rate, from 2014/15 at 7.7% to 2019/20 at 13.4% (Figure 39).
Figure 39: Proportion of supported working age adults with learning disabilities in paid employment trends over time 2014/15 to 2019/20
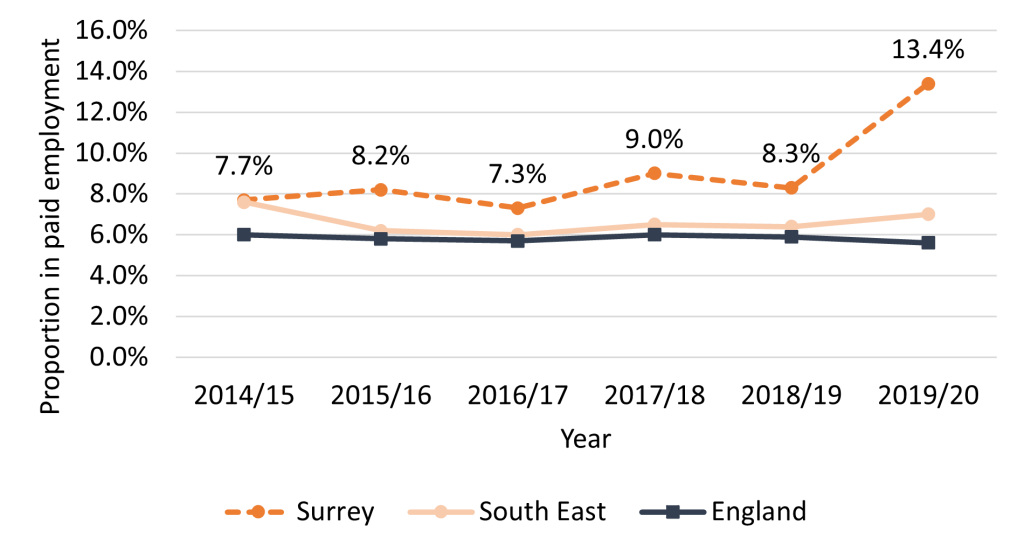
Figure 40 presents a comparison of the employment rate of people in receipt of long-term support for a learning disability (aged 18 to 64) with the overall employment rate, as shown below reinforces that Surrey is doing well.
Figure 40 : The percentage point gap in the employment rate between those who are in receipt of long term support for a learning disability (aged 18 to 64) and the overall employment rate, 2022/2023, National and South Eastern Region
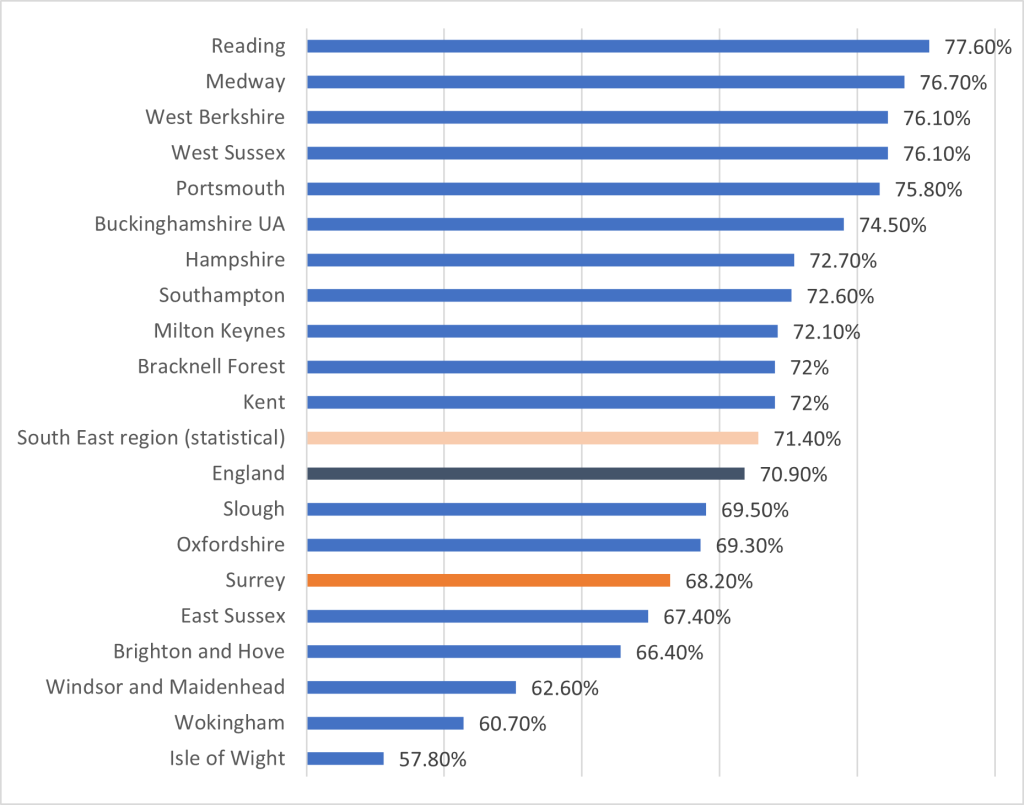
In 2021 the gap in the employment rate between those who are in receipt of long-term support for a learning disability (aged 18 to 64) and the overall employment rate was 67.5% in Surrey. This is lower than the gap nationally (70.0%) and regionally (71.1%) (OHID). The percentage point gap is between the percentage of working age learning disabled clients known to Councils with Adult Social Services Responsibilities (CASSRs) in paid employment (aged 18 to 64) and the percentage of all respondents in the Labour Force Survey classed as employed (aged 16 to 64).
Surrey County Council collect data under ASC14c, percentage of adults in employment or volunteering and report under the primary client category of learning disability. The target the council has set is 20% and performance against this is typically 19% or above for adults and lower for the transition service as the majority of individuals are in education.
Table 43: Number of people open to Adult Social Care in Surrey with a Primary Support Reason (PSR) or Primary Client Category (PCC) of learning disability by District & Boroughs, excluding unknown addresses, by employment status, split by paid and unpaid
| D&B or OOC | Not Known | Employed & Voluntary (Paid) | Employed & Voluntary (Unpaid) | Unemployed |
| Elmbridge | 13 | 53 | 17 | 218 |
| Epsom & Ewell | 6 | 34 | 16 | 203 |
| Guildford | 35 | 61 | 35 | 291 |
| Mole Valley | 12 | 33 | 34 | 224 |
| Reigate & Banstead | 24 | 68 | 39 | 530 |
| Runnymede | 19 | 23 | 9 | 202 |
| Spelthorne | 22 | 40 | 12 | 205 |
| Surrey Heath | 31 | 37 | 21 | 192 |
| Tandridge | 9 | 26 | 26 | 242 |
| Waverley | 56 | 65 | 30 | 328 |
| Woking | 19 | 43 | 23 | 251 |
| Outside Surrey | 13 | 22 | 22 | 508 |
| Total | 259 | 505 | 284 | 3,394 |
Numbers or totals may have been slightly altered to avoid disclosure on this or other tables
Table 44: Number of people open to Adult Social Care in Surrey with a Primary Support Reason (PSR) or Primary Client Category (PCC) of learning disability by age, excluding unknown addresses, by employment status with split of paid and unpaid
| Age Group | Not Known | Employed & Voluntary (Paid) | Employed & Voluntary (Unpaid) | Unemployed or retired |
| 18 to 29 | 111 | 122 | 97 | 1,253 |
| 30 to 39 | 39 | 156 | 60 | 683 |
| 40 to 49 | 29 | 76 | 54 | 384 |
| 50 to 59 | 30 | 85 | 34 | 406 |
| 60 to 69 | 26 | 42 | 28 | 411 |
| 70 and over | 24 | 24 | 11 | 257 |
| Grand Total | 259 | 505 | 284 | 3,394 |
Numbers or totals may have been slightly altered to avoid disclosure on this or other tables
Recommendation: Annual social care reviews should routinely include the collection of this data, to reduce the number for whom employment status is unknown.
Employment provision in Surrey
One of the twelve workstreams in Surrey’s learning disability and autism Programme Board delivery plan 2021 to 2024 focuses on ‘Day Opportunities / Employment / Community Inclusion’.
Employment is also referenced in community infrastructure and services and young people and transition ‘Increase the work experience and employment opportunities for young people aged 16 or over, with the aim of an additional 80 people benefitting from supported internships and supported employment.’
Workstream 5 of the All Age Autism Strategy 2021 – 2026 is employment and Surrey benefits from a vibrant ‘No One left Behind skills and employment network’ that is fully inclusive.
Surrey has a mixed offer of employment support types to cover a range of needs including:
- Supported employment: available for all adults aged 18 and over and comprises career advice, job searching, interview support, job coaching, in work support and job maintenance.
- Supported Internships with employers: targeted at 16 to 24 year olds and linked to interests and skills. Offered in the final year of education leading to work or job seeking.
- Work experience, volunteering opportunities targeted for 16 to 24 year olds, ideal for those not attending college
Supported Internships
The headlines for 2021/22 Supported Internships
- 14 young people undertook supported internships
- 93% completed their supported internships
- 43% achieved paid outcomes
- 43% are actively job seeking
- 86% continuing with vocational options at end of year (e.g., paid work, volunteering, job seeking)
Commissioning activity
There is a strategic review of Surrey’s current offer of day and evening opportunities underway which includes a review of the employment support available. This aims to:
- Identify gaps in the current provision
- develop a wider menu of options that facilitates choice and independence
- develop greater transparency and equity across the market
The review will result in a refreshed commissioning strategy. It aims to report in Summer 2023.
Community Inclusion
A community inclusion strategy is to be developed during 2023. This will be aligned to the joint Autism Strategy and a post for a dedicated commissioning manager to progress Community Inclusion has been established.
Hate and mate crime
The number of Safeguarding referrals that were started between 01 September 2021 and 30 August 2022 and linked to people with a PSR or PCC of Learning Disability, which resulted in a Section 42 Enquiry which were flagged as a Mate Crime was 8.
There is also the experience of anti-social behaviour which appears to happen more to people with disabilities as is shown below and is defined as:
“Anti-social behaviour is any behaviour that causes people nuisance, annoyance, alarm or distress. This can include behaviours that are aggressive or intimidating or that impact upon a person’s quality of life”.
Figure 41: Proportion of adults experiencing any anti-social behaviour in the last year by disability status, England and Wales, for year ending March 2025
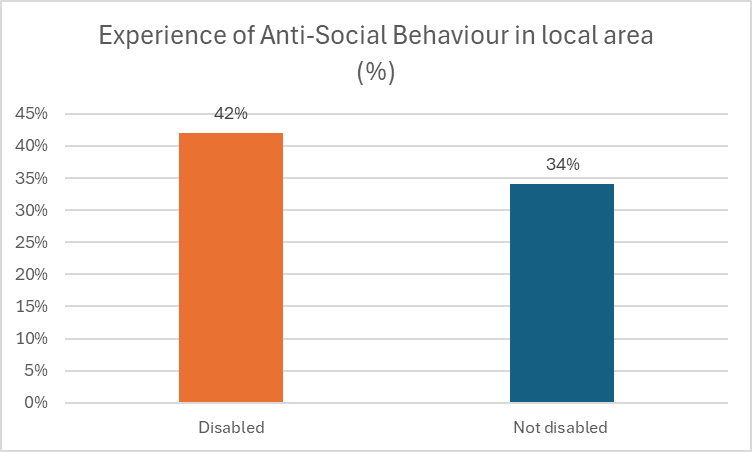
Figure 42: Proportion of adults experiencing any anti-social behaviour in the last year by disability status, and age group, England, for year ending March 2020
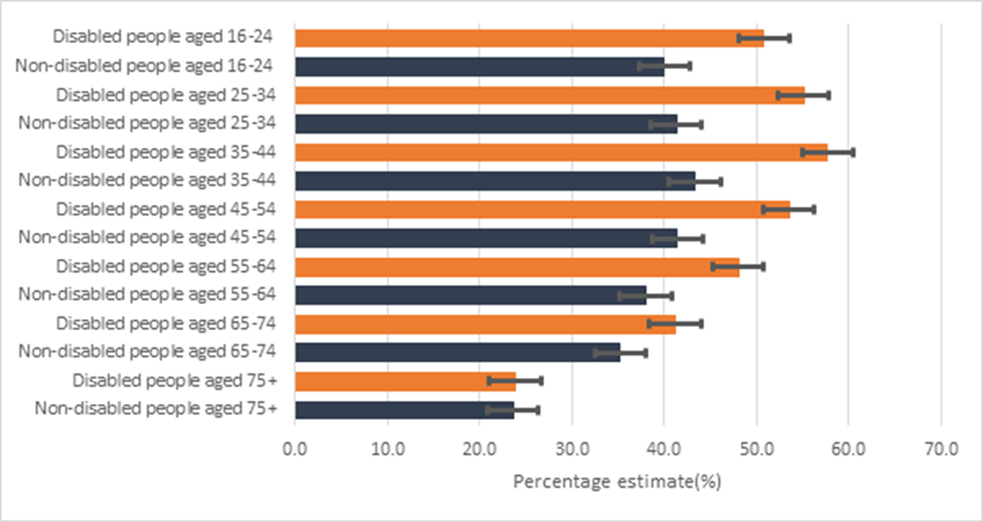
Domestic Abuse
People with learning disabilities, autism or both are thought to experience domestic abuse at about three times the rate of the general population [86]. Around 1 in 10 (9.2%) disabled people aged 16 to 59 years in England and Wales experienced domestic abuse in the year ending March 2020, compared with about 1 in 20 (3.9%) non-disabled people; disabled women (12.7%) were more than three times as likely to experience domestic abuse than non-disabled women (4.7%) [87].
A Marac (Multi-Agency Risk Assessment Conference) is a meeting where information is shared on victims at the highest risk of serious harm or murder as a result of domestic abuse. It is attended by representatives of local agencies such as police and health. In Surrey, the number of domestic abuse cases discussed at MARAC in the year ending March 2025 was 1,868. Of these, 0.5% of cases the victim had a disability. This proportion is lower than what was seen in England (11.2%) and the South East (8.2%)[88].
Recommendation: The number of people with learning disabilities experiencing domestic abuse and accessing support is not well understood within Surrey. This needs to be understood to ensure the support offers are reasonably adjusted.
Crime, concerning behaviour
Across the Criminal Justice System (police, courts, prison and probation) work needs to be done to ensure that people with learning disabilities and/or autism are identified routinely, and supported [89] [90] [91]. Within Surrey, most is known about people who have been diverted into forensic inpatient beds as this is part of the NHS England Long Term plan commitment to reducing the use of inpatient beds and inpatient use trajectories (see below).
Police and Court
Access to and experience of the police and court system by people with learning disabilities is not deeply understood so it is not clear in Surrey if people with learning disabilities and/or autism are identified routinely and supported. Data is not currently available regarding access to the police service.
Recommendation: Data is required to understand quality of access to the police service by people with learning disabilities.
Prison
Two studies estimated the prevalence of learning disabilities among prisoners at 7% [92] [93] so despite varying prevalence statistics (e.g. proportion of people known to adult services as having learning disabilities is 0.6% although, actual prevalence is likely higher) it can be concluded that people with learning disabilities and/or autism are likely to be over-represented in the Criminal Justice System.
From April 2019 prisoners are screened for learning difficulties and/or disabilities on first reception into the educational services of all adult prisons across England [94] [95]. Prison and probation use IQ below 70 as the benchmark for ‘learning disabilities’. They label those with IQ between 70 and 80 as having ‘borderline intellectual functioning’. These groups are described as having ‘learning disability and/or learning challenges’ and they are entitled to additional support [96].
There are five prisons situated within Surrey:
- HMP & YOI Bronzefield: a privately run female prison in Ashford.
- HMP Coldingley: a prison for adult men in Woking.
- HMP & YOI Downview: a prison and young offender institution (YOI) in Sutton, for women aged 18 and over.
- HMP High Down: a men’s prison and young offender institution (YOI) near Sutton.
- HMP Send: a women’s prison in Woking.
The numbers screened for learning difficulties and/or disabilities in prisons in Surrey is unknown.
Recommendation: The quality of data regarding people in prison who have learning disabilities is required, ensuring they have access to the support they need. It is understood that HMP SEND now has a Neurodiversity Office, contact to be made and joined up discussion to review the impact of this role.
Inpatient bed use
Secure mental health services provide accommodation, treatment and support for people with severe mental health problems who pose a risk to the public. Secure services work predominantly with people who have been imprisoned or admitted directly to hospital following a criminal offence. This can and does include people with learning disabilities.
For Surrey we have data pertaining to people who have been diverted into hospital treatment as this cohort are included within the reduction of use of inpatient beds. The inpatient trajectory key performance indicators to bring inpatient numbers down to below per 30 million of population as specified in the NHS Long Term Plan is inclusive of this population as well as offering them the same quality assurance process such as commissioner visits, CTR/ CETR and safe and wellbeing reviews as those who are inpatients for their mental health needs.
Commissioning arrangements for secure mental health services are via the Kent, Surrey and Sussex Provider Adult Secure Provider Collaborative which is a coalition of three NHS Trusts and five independent sector providers that deliver low and medium secure hospital care for adults (with high secure care commissioning remaining with NHS England). Provider collaboratives represent a shift from national to local commissioning. There are 46 in England and Wales.
How provider collaboratives work:
- Single point of contact for referrals
- Only admit people who require a secure hospital environment
- Source and pay for an appropriate hospital placement
- Monitor and drive up the quality of hospital treatment and care
- Undertake CTR’s (Care and Treatment Reviews)
- Work with hospital teams to ensure least restrictive options are chosen.
- Work closely with community teams to ensure timely discharges
As of November 2022, 14 people were in Provider collaborative commissioned beds, which contributed to Surrey Heartlands Integrated Care System having reaching their 2022/23 target of 21 adult inpatients in total.
- The average length of stay for these patients was 6 years and 6 months.
- 12 of the 14 were out of their integrated care system geography
- 5 are ready for or planning for discharge in 2022/23 with 10 expected for discharge 2023/2024+
- Under 5 are considered delayed transfers of care
- 6 can be immediately identified for “Move on accommodation”, others in the medium term.
Quality
- Under 5 people were in CQC rated inadequate services and under 5 in CQC rated ‘requires improvement’.
- 73% of repeated C(e)TRs were completed on time
- 79% of oversights visits were completed bearing in mind patients can decline
- In March 2022 all received a safe and wellbeing review
Safe and wellbeing reviews
The thematic findings of the safe and wellbeing reviews are included as an appendix. They include good and poor practice identified and thematic review findings regarding a number of areas.
Community Support
The KSS provider collaborative have a commitment to ensure community forensic services (FOL’s) exist for learning disability and autism as well as Mental Health. A work programme designed to reduce length of stay, prevent avoidable admissions and safely manage risk in the community has been instigated by the provider collaborative alongside community partner trusts.
Children’s inpatient services are commissioned via the Tier four provider collaborative
CAMHS Tier 4 Provider Collaborative (PC) involves providers of specialist mental health and care services working together to continuously improve patient experiences. The PC is responsible for planning and commissioning specialist mental health and learning disability services to meet the needs of our local communities. All referrals for CAMHS Tier 4 services come through the PC to ensure that all alternatives to a hospital admission have been considered. Once a decision to admit has been agreed, the PC is responsible for finding and commissioning a suitable placement for the young person. Throughout the young person’s admission, the PC maintain quality oversight of the care provided by visiting the young person regularly and scrutinising care and treatment plans. The PC works closely with community teams in working towards discharge and unblocking any barriers.
There are currently no Surrey based beds for CYP. They are in development.
Community voice
Local infrastructure
There are mechanisms in place to ensure that people with learning disabilities themselves shape service design and delivery. A ‘governance chart’ that shows how these relate is included in the JSNA as appendix 3.
Learning Disabilities and Autism Partnership Board
The Government in 2001 asked that partnership boards were setup across the country to make sure that the white paper, Valuing People: A New Strategy for Learning Disability for the 21st Century, was put into action.
The Surrey Learning Disability Partnership Board was established in 2001 and Autism Partnership Board was established in 2011 to prepare for launch of National Strategy in 2012. Their purpose, as decided by members of the Boards, is that people work together, so that people with a learning disability and/or autism can have a voice, make change happen, live in the community, be informed, be safe, remain healthy and confident to be part of their community
The following “I principles” apply to Partnership Board
- I have choice and control over my life.
- I have a voice
- I live in the community with support from my family and carers.
- I have a fulfilling and purposeful everyday life.
- I get good care from all health services.
- I can access extra health and social care support when needed.
- I am supported to stay safe.
The Boards are co-chaired by an individual with learning disability or autism. Members of the Boards are all key people (stakeholders), who can bring about change, they are people with learning disabilities, their families, professionals, and voluntary organisations.
The Surrey Autism Partnership Board has meetings four times every year. It is for autistic adults, family carers, and people who work supporting autistic people. Members share their work and talk about questions or worries they have. The board makes sure the Surrey All-Age Autism Strategy and the National Autism Strategy works for autistic adults in Surrey. It also has a reference group of autistic adults.
Surrey is a large county so there are four Valuing People groups to ensure everyone has a voice at a local level. The chairs and co-chairs from these groups and another member of the local group will sit on the partnership board. The four Valuing People groups are:
East Surrey
- Reigate and Banstead
- Tandridge
North West Surrey
- Runnymede
- Spelthorne
- Woking
South West Surrey
- Guildford and Waverley
- Surrey Heath
Mid Surrey
- Epsom and Ewell
- Mole Valley
- Elmbridge
The Boards and Local Valuing People Group are supported by an Engagement and Partnership Officer and the chairs of the Valuing People group will meet regularly to talk about agendas and feedback what is happening locally and nationally.
In conjunction with meetings a central email address has been established and an information hub has been developed to ensure information is available to all.
Please visit the Surrey Learning Disability Partnership Board Website.
Recommendation: Ensure that these forums offer people with learning disabilities a range of opportunities to have their voices heard and to shape service design and delivery. These need to be separate from partnership meetings, which could result in their voices being unheard.
Recommendation: Ensure that these forums offer carers of people with learning disabilities a range of opportunities to have their voices heard and to shape service design and delivery. These need to be separate from partnership meetings, which could result in their voices being unheard.
Surrey Peoples Group
The Surrey People’s Network is a Surrey-wide group for people with a learning disability, autism, and acquired brain injury.
The group is set up to give people a voice, find opportunities, and encourage positive change. Meeting once a month on the first Wednesday of the month for an hour and a half. Members suggest topics for the agenda and talk about things important to them. These have included independence, community inclusion, health inequalities, and other projects people care about. The group is growing and always welcomes new members.
The group has been promoted the group via the Surrey Care Association Network, Surrey County Council integrated website and networks as well as social media and reaching out to a wide range of social care and charity organisations and health partners. To engage more widely the group is also in contact with Learning Disability England, a national advocacy and campaigning organisation.
The Surrey People’s Group video was recorded in 2021 during the COVID-19 pandemic to share with people how to get involved and make change happen. In 2021 the Surrey Peoples Group were selected as a finalist for Learning Disability and Autism Leaders Award.
Members have been paid to participate in interviewing for the Council, have led presentations to health professionals, and have checked easy read materials and have made explainer videos [97].
During 2021/2022, the group established four discussion groups on topics that users of services identified to be of concern to them. Key messages are set out below
Transport
- Public transport is the preferred form of transport, in particular buses as trains can be too challenging, both in terms of journey planning and accessibility. Some people are eligible for pass bases and a number of them for carers passes, though these can be challenging to secure.
- Bus passes cannot be used before 9:30 am (during peak times) so can be restrictive for appointments e.g. with the doctor and as a result alternative methods of transport often have to be used. These can be significantly more costly.
Feeling Safe in the Community
- Most members in the group feel safe in their local neighbourhoods and were able to walk at night with street lighting and CCTV.
- Members knew how to contact emergency services if they needed to, and, what to do if they needed help, although the majority in the groups did not know who their community support officers were.
- Many of the group did not know nor communicate with their neighbours.
- Technology can be used to support people more than is currently the case.
Being in the Community
- The following activities are easily accessible and local: countryside walks and parks, shopping, swimming/ leisure centres and cafes/ dining out. It was agreed that these activities had easy wheelchair access too.
- People had to look outside of Surrey to access some places of worship them. For example, the nearest Sikh temple can be found in Crawley in West Sussex.
- Activities such as bowling and going to the theatre are equally difficult to find, and people had to look outside of Surrey.
- Some members are even involved in voluntary work, such as their local food bank, church groups and local charities. This gave members a sense of purpose as well as the ability to socialise with the public.
Money
- People need support managing their money and with utility bills.
- Benefit support: Benefit support was suggested as this is something that isn’t as prominent as budget support. Many of the members are either unemployed or doing unpaid work e.g., volunteering, therefore, income maximisation would be very favourable for them. Support here, would allow them to know what they are eligible to receive.
- Do you know where to get help if you need it? Many members do not know where their local foodbank is or where their community fridges are. The point of sign posting these services more was raised and should be taken into consideration given the current economic climate.
- Citizens Advice Bureau (CAB) – not many are familiar with CAB and what kind of support they offer, or even where their nearest CAB is. Again, sign posting for this is needed.
- The group campaigned for easy read resources on Cost of Living, and these were produced in November and have been circulated to stakeholders, social workers and providers so that people can get advice and support they require.
Next Steps
Following a presentation to Royal Surrey Hospital on challenges faced by people with learning disability using their service, Royal Surrey are working with an individual to make reasonable adjustments and sign posting.
The Surrey People’s group are setting up a series of regular workshops across Surrey to ensure they capture people’s views and feedback to Partnership Board to make change happen and improve lives.
Membership and minutes from the meetings can be found on Surrey People’s Network – having a voice – Surrey County Council (surreycc.gov.uk)
Surrey People’s Group held an event on the 6th December 2022 and talked about the following topics: home, travel, friendships and health. There was also included discussion on ‘things you have done you are proud of’, ‘what makes it hard to live your life’ and ‘hopes and dreams for the future’. Each produced a word cloud.
The biggest words in the word cloud for each topic are as follows.
- Home: needs fixing, shared house, supported living, I can stay out late
- Travel: expensive, safety worries, timetables, no bus passes
- Friendships: nice to see people today, nice friends, friends visit, social media
- Health: had my check, hospital passport, reasonable adjustment, struggle with GP
- Things you have done you are proud of: having a job, living an independent life, special friends
- What makes it hard to live your life: Cost of living, health, getting work, being myself
- Hopes and dreams for the future: having my own flat, getting married, having a child, romance
The full word cloud outputs are included in appendix 5.
The group said that:
- Health feedback has been sent to the liaison nurses and other health colleagues
- Travel feedback has been sent to commissioning who are working on the transport consultation
- Presentation to the Learning Disability Partnership Board – where we agreed this would part of this section of the JSNA
- Use feedback to work out what to work on in 2023
- Develop a strong planning / advisory group
- Have regular events to involve more people
Experience of COVID-19
Lived experience during the first year of the pandemic of those with a learning disability, who receive day to day support, and staff, was fed back through focus groups organised by Surrey People’s Group. The aim was to better understand the experiences of the COVID-19 pandemic.
For those with a learning disability
Feedback of the overall experience of COVID-19 was negative. Having to continually stay indoors and not being able to go out to see friends, family, and going to day services was commented on repeatedly. Mask use was also mentioned, with them making it more difficult to understand people.
The focus groups were asked about what the best thing about COVID-19 had been. Different activities such as cooking/baking, zoom film nights, learning to knit, and playing games with staff, were identified as positives. As was having the vaccine.
When asked what helped during the pandemic, staff support was repeatedly reported, this included helping with tests, explaining what was going on to help with understanding of the situation. Those that the people lived with were also mentioned.
For staff
There were high levels of anxiety felt, with concerns around taking the virus into the workplace or back home to their own families. Staff also felt guilty if they had to work from home, tested positive, or were shielding.
Adult Social Care Survey England- 2023/24
The Adult Social Care survey is a national survey that is conducted by CASSRs. It seeks the opinions of service users aged 18 and over in receipt of long-term support services funded or managed by social services and is designed to help the adult social care sector understand more about how services are affecting lives to enable choice and for informing service development.
The ASC Survey for 2023/24 can be filtered on people with a Primary Support Reason of Learning Disability. Although the survey overall gave some very positive messages, there are important ones that need to be progressed:
- 43.6% selected ‘I have adequate control over my daily life’
- Only 63% of responses were positive selecting the statement ‘I have as much social contact as I want with people I like’
- Only 24.1% of responses stated information or advice was easy to find
- 28.4% stated they ‘have moderate pain or discomfort’.
- 34.9% selected ‘I am moderately anxious or depressed’.
The full survey results are available in Appendix 2.
Recommendation: These findings, particularly regarding control, social contact, pain and mental health, need to shape commissioning intentions for all types of support.
Recommendation: Surrey County Council is currently developing a Direct Payments Strategy, which highlights that there is no Individual Service Fund offer in Surrey and commits to exploring whether one should be developed within the first year of the Strategy being Published in June 2023.
Carer voice
Family Carers are key members of The Learning Disability Partnership Board and the Local Valuing People Group and contribute to shaping development of services.
The Carers Partnership Board was significantly refreshed in April 2022 and a Disabilities Sub Group is planned. This responds to a concern that the voices of people with disabilities and those of their carers were being conflated.
Provider voice
There is a learning disability and autism Network of Surrey Carers Association (SCA) members explore how they can offer the best possible services to the people they care for and support. Representatives from the network attend the Learning Disability Partnership Board and providers sit on the local valuing people groups.
Separately from this, the Commissioning Team support a Provider Forum to establish dialogues with providers of support to people in Surrey with a Learning Disability and Autism regarding issues related to commissioning. This has explored the commissioning of particular models of care, including day opportunities (including outreach and employment support), supported living and short breaks.
Providers are represented on the Partnership Board, on the Programme Board and attend the Strategic Forum. A learning disabilities and autism governance chart that sets out how these relate can be found as appendix 3.
Evidence base, what works
Prevention and interventions for people with learning disabilities with behaviour challenges
Evidence from multi-component health promotion programs (e.g. Health Matters: The Exercise, Nutrition and Health Education Curriculum for People with Developmental Disabilities) indicated that they can result in positive physical, health behaviour, and psychosocial outcomes.
In older adults with a learning disability, health promotion and disease prevention strategies should be tailored to the individual’s health risks and should include cognitive, mental and physical health, accommodations, workplace considerations, assistive technology, recreational activities, and nutrition to address need [98]
Key guidance and resources
National Institute for Health and Care Excellence (NICE)
NICE has published an impact report reviewing how its guidance has been used to improve the health and care of people with a learning disability. Based on this report NICE has developed, three quality standards and one advice product. The following key priority areas were identified by the stakeholders involved in the guidance:
- The uptake and quality of annual health checks
- Reasonable adjustments and accessible communication
- Providing personalised care and supporting people to live independent lives in the community
- Integrated local commissioning of health, social care and education services
- Health and social care workforce development
- Reducing healthcare inequalities
Research has shown that, compared with the general population, people with a learning disability were three to four times as likely to die from an avoidable medical cause of death. Most of the avoidable deaths in people with a learning disability were because timely and effective treatment was not given.
NICE has provided a number recommendations which can help with reducing the health inequalities facing people with a learning disability. These recommendations related to
- Annual Health checks
- Cancer screening
- Health action planning
Recommendations on annual health:
- To help increase access to healthcare, NICE guideline on challenging behaviour and learning disabilities recommends that people with a learning disability should be offered an annual health check.
- NICE guidance on mental health problems in people with learning disabilities sets out how the annual health check should identify physical and mental health problems.
- Health checks should be undertaken by an appropriately trained provider. The NICE quality standard on learning disability: care and support of people growing older sets out the minimum elements that should be included in health check protocols.
Recommendations for cancer screening:
Evidence shows that the rate of cancer screening uptake by people with a learning disability is lower than the general public. The latest report by NICE showed that in the previous five years, the proportion of women aged 50 to 69 with a learning disability who received breast cancer screening was 51%. This compares to 65% of women in the same age group without a learning disability. Therefore, NICE also recommends that other routine healthcare such as cancer screening form important element of the annual health checks. therefore, the NICE guideline on care and support of people growing older with learning disabilities recommends that older people with a learning disability should be offered the same routine screening as older people without a learning disability.
Recommendations for health action plan:
- The health action plan should be developed by the person with a learning disability with their practitioner to stay healthy.
- The guideline on care and support of people growing older with learning disabilities recommends that any actions identified by the annual health check are recorded in the person’s health action plan and in an accessible way for the person.
2. Helping people accessing care and support
Reasonable adjustments are also important and there is a legal requirement to make sure services are accessible to all people with protected characteristics under the Equality Act 2010. The NICE guidance on care and support of people growing older with learning disabilities states that service providers must make these reasonable adjustments.
Adjustments may also be needed so that people with a learning disability can access work. The guidance on mental health problems in people with learning disabilities says adults with a learning disability (with or without mental health issues) interested in accessing paid or unpaid work should be supported.
3. Reducing overmedication and long-term hospital care
Reducing overmedication
There are between 30,000 to 35,000 adults with a learning disability in England who are taking psychotropic medicines without a relevant diagnosis. Guidance from NICE on challenging behaviour and learning disabilities says that antipsychotic medication should be considered only in very limited circumstances. And always offered in combination with psychological or other interventions.
As per The NICE quality standard on learning disability: behaviour that challenges antipsychotic medication should be reviewed 12 weeks after starting treatment and then at least every six months.
Some studies have suggested that community pharmacists may be able to play a positive role in improving the quality of the medication use process, in collaboration with other healthcare professionals, carers and patients with a learning disability (O’Dwyer et al., 2015).
Long-term hospital care
Preventing admission: NICE recommends assessment to identify possible triggers for admission and access to specialist behavioural support in the community. Access to mental health services should including crisis support, should be available when needed (Overview | Service user experience in adult mental health: improving the experience of care for people using adult NHS mental health services | Guidance | NICE)
Upon admission: the hospital and community learning disability team should work together with the person to develop a discharge plan. Links with home community, including relationships, employment and education, should be maintained (Recommendations | Transition between inpatient mental health settings and community or care home settings | Guidance | NICE.)
4 Support and future planning of people with a learning disability
The NICE report highlighted that, in 2019/20, adults using learning disability support services had satisfactory experiences of care. 97% said that support services improve their quality of life and 81% feel as safe as they want. 72% of adults said they are extremely or very satisfied with the care and support they receive. Only 41% say they have as much control over their daily life as they want.
The wider needs of people with a learning disability also need to be considered including housing and opportunities for social interaction. Two-thirds of adults with learning disabilities live with their families, usually their parents, according to Mencap’s Housing for people with a learning disability. Eventually, ageing family carers may reluctantly explore alternative care arrangements when they are no longer able to provide long-term care. The death or serious illness of a parent may result in unplanned or multiple moves in accommodation for people with a learning disability.
Thinking about the future is an important aspect of person-centred planning. As per guidance on care and support of people growing older with learning disabilities, health and social care practitioners should use strengths and asset-based approaches to conversations with people growing older with learning disabilities to address their changing needs, wishes and capabilities and promote their independence for by connecting them with social clubs, community gardens, faith and cultural groups, user-led social groups).
Person-centred approach also includes building on the person’s strengths and skills and consider how to meet their changing needs and preferences to promote independence. This should include empowering people to build and maintain relationships to reduce isolation.
Social Care Institute for Excellence (SCIE)
SCIE’s ‘Tackling inequalities in care for people with learning disabilities and autistic people’ project explored the inequalities faced by people living with learning disabilities and autistic people. A guidance document has been produced which brings together learning from discussions and work with commissioners, service providers and people with learning disabilities.
Workforce development
Health Education England and Skills for Care are co-ordinating the development of the Oliver McGowan Mandatory Training in learning disability and autism for all health and social care staff. This includes tiers 1 and 2 of the core capabilities framework, which is underpinned by the NICE guidance.
Recommendation: Roll out of Oliver McGowan Mandatory Training.
Summary of Recommendations
Legislative / Policy Framework
Recommendation: Following the publication of the evidence we will review whether the detail of Down Syndrome Act is already in place and consider the impact of the Act and subsequent guidance both on this community and the wider community of people with learning disabilities.
Recommendation: Use the outputs from all of the reports of The learning disability improvement standards for NHS trusts in strategic discussions to share good practice and reduce unwarranted variation across Surrey.
Recommendation: Joint work across health and social care system leaders, including leaders at ‘place’, to ensure that the full benefits of the Fuller Stocktake are fully realised for people with a learning disability.
Primary care, all-age learning disability registers
Recommendation: Surrey all-age system leaders need to consider what diagnostic processes are in place and, depending upon the findings, consider if access to services in the future will not be diagnostic dependent.
Recommendation: Surrey all-age system leaders need to consider how best to provide clarity regarding terminology and ensure that necessary differences does lead to poor access or the robustness of intelligence.
Recommendation: To increase the number of people of all ages with a learning disability on the GP Register, paying particular attention to those from minority groups. There is no available breakdown by ethnic group. This is a symptom of a broader lack of routine ethnic monitoring in General Practice that needs to be addressed.
Learning disability population projections
Recommendation: Given that the predicted rate is likely to be lower than the actual rate, the numbers of people presenting with challenging / distressed behaviours and behaviours of concern will need to be kept under review including via the dynamic support register.
Recommendation: Data on all underrepresented groups within Surrey will need to be gathered, including the GRT community using the more distinct categories for these communities that are under development. This data can then be used to consider raising awareness and offering support to members of under-represented communities with a learning disability.
Recommendation: Data to be gathered within Surrey and consideration given to understanding the numbers and experiences of people with a learning disability identifying as LGBGTQ+ in order to ensure barriers to expression are tackled and equity of access to services and support.
Number of adults with a learning disability open to Social Care
Recommendation: Seek to understand this increase, including if the higher rates of identification of more severe forms of intellectual disability are recorded among children of Pakistani and Bangladeshi heritage.
Recommendation: Ensure commissioning strategies and services are able to meet cultural needs, working with the VCSE (including Surrey Minority Ethic Forum).
Safeguarding
Recommendation: Safeguarding data needs routinely to be benchmarked, themes from enquiries highlighted and preventative action undertaken.
Prevalence of behaviour risk factors
Recommendation: Ensure smoking cessation support is reasonably adjusted to meet the needs of people with a learning disability and that targeted support is offered in North West place.
Physical health outcomes
Recommendation: Sustain the deep dive into respiratory deaths in order to better understand how these can be reduced, as recommended by the LeDeR review.
Recommendation: Ensure that the ‘lessons learnt’ review of experience in the pandemic incorporates the views of the provider sector e.g. access to PPE.
Recommendation: Ascertain if mass vaccination centres can use the learning disability flag and routinely offer reasonable adjustments.
Recommendation: Work with public health and system clinical leads to ensure that:
- weight management support is reasonably adjusted to meet the needs of younger people with a learning disability
- targeted support is offered to try to reduce the proportion of young people becoming obese.
Recommendation: Further understanding of the level of physical activity and access (including barriers), interlinked to the Whole System Approach to Obesity for people with learning disabilities and connecting into other initiatives such as Active Surrey and Active Travel.
Recommendation: Health inequalities group to be convened to consider all of the health inequalities including wider determinants and supporting the two public health leads in community asset and grass root approaches to the recommendations.
Gender based inequalities within the learning disabilities population
Recommendation: To further understand why women with learning disabilities are more likely to be overweight and design appropriate interventions.
Recommendation: A greater understanding of needs and experiences of women with a learning disability of peri menopause and menopause including but not limited to impacts on weight (including access to support, interventions and mental health impacts).
Primary Care
Recommendation: Joint work across the age ranges under the governance of the health inequalities group to consider and address the reasons for low uptake of annual health checks and other interventions for younger people.
Variations in physical health between Surrey Heartlands Four ‘Places’
Recommendation: Work with public health and system clinical leads diabetes leads to ensure support is reasonably adjusted to meet the needs of people with a learning disability and targeted support is offered in North West Surrey ‘place’.
Recommendation: Monitoring on an ongoing basis with both the Surrey Heartlands performance team, primary care liaison service and place-based leads to offer support where needed to ensure North West Surrey has support if needed to offer health checks.
Dental outcome
Recommendation: As specialist dentistry commissioning becomes delegated to ICBs from NHSE/I, work needs to be undertaken to understand levels of access to dental care of people with learning disabilities and the challenges that may prevent access or lead to a poor experience, triangulating dental service data with that from general practice.
Postural care
Recommendation: Given the importance of postural care, improved data tracking is required to inform commissioning intentions. This should include reference to postural care in any LeDeR or safeguarding reports.
Dementia and learning disabilities
Recommendation: Improved intelligence regarding dementia prevalence should be established, requiring joint work between health and care practitioners, commissioners, providers and the clinical lead. Data reports should include:
- reference to dementia in any LeDeR or safeguarding reports
- the number of people identified on the GP dementia register who have a learning disability or Down’s Syndrome and of those how many have had their dementia review
- the number of people identified on the GP LD register who have dementia and of those how many have had their dementia review.
Recommendation: Data regarding prevalence of dementia among people with learning disabilities and Down’s syndrome and use of services must be included in strategic planning going forward under the Dementia Strategy.
People with learning disabilities and ageing
Recommendation: The wider needs of ageing adults with learning disabilities needs system-wide consideration, building on specifically targeted pieces of work currently underway. This must include but not be limited to NICE health-based guidance and being supported in any caring roles.
Sensory Impairment
Recommendation: Improved data relating to eye health and access to related services should be established, requiring joint work between health and care practitioners, commissioners, providers and the clinical lead.
Recommendation: Improved data about hearing, hearing loss and hearing impairment and access to support for people with learning disabilities should be pursued.
Podiatry
Recommendation: Improved data about access to community podiatry services and the impact of there being a specialist podiatry offer in only half of the county should be pursued.
Sex, sexual health, sexual awareness and sexual expression
Recommendation: A greater understanding of the needs of people with learning disabilities regarding sexual awareness and expression, and access to services should be pursued.
Pregnancy care and outcomes
Recommendation: Data and insight about the number and experiences of parents within a learning disability will support the delivery of the local priorities identified and needs to be sourced.
Access to health services
Recommendation: To consider using the outputs from all of The learning disability improvement standards for NHS trusts reports in strategic discussions to share good practice and reduce unwarranted variation across Surrey.
Recommendation: Ensure the community health services are offered support to complete The learning disability improvement standards for NHS trusts .
Recommendation: Data from this JSNA to inform the upcoming contract review of the specialist learning disability services including the primary care offer.
Recommendation: The findings of this JSNA to inform the upcoming contract review of the specialist learning disability services, include the acute liaison service.
Recommendation: More data is needed to understand the difference between people with and without learning disabilities and their use of primary and acute care to ascertain if there is inequity of access.
Recommendation: Further analysis of data related to access to services by people with learning disabilities to clarify the number of unique people represented as opposed to repeat contacts, as the data might not be representative of access across the whole population access).
Recommendation: Intervention is needed to improve recording of the ethnicity of people with a learning disability using primary and acute services to improve data quality and insight into need.
Recommendations: The following two sets of data are needed to understand community health service access for those with a learning disability Surrey wide:
- Data for those who live in Frimley.
- Data across the whole of Surrey for people with learning disabilities accessing community health services (which may need to wait until the roll out of the learning disability and autism Flag)
Mental health and outcomes, including inpatient admissions
Recommendation: Urgent consideration to be given for the roll out of the Green Light Toolkit by the six-monthly Strategy group within Surrey.
Recommendation: Consider resource requirements for STAMP.
Recommendation: Consider increasing training in primary care for STOMP/STAMP
Recommendation: Consider models of social support offered to patients and families while stopping medications (e.g. as stopping some of these medications might result in decreased sleep and increased behaviour that challenges and so shouldn’t be left unsupported)
Integrated Intensive Support Service
Recommendation: Consideration in the ISS contract review as to whether there is a need for a seven day specialist multidisciplinary service or crisis care offer
LAEP meeting and Care (education) and treatment reviews
Recommendation: An analysis of the changes to the guidance (now called ‘Dynamic support register and Care (Education) and Treatment Review policy and guide’) to be completed to ensure readiness for implementation by 01 May 2023.
Future considerations for proposed Mental Health Act changes
Recommendation: Ensure the impact of the proposed changes to the Mental Health Act outlined in the BTRS Action plan are understood, actioned and planned for including any impact on community accommodation and support and inpatient offer.
Poverty and Health
Recommendation: Further analysis to understand the impact of deprivation including food and fuel poverty is needed.
Employment
Recommendation: Annual social care reviews should routinely include the collection of this data, to reduce the number for whom employment status is unknown.
Domestic Abuse
Recommendation: The number of people with learning disabilities experiencing domestic abuse and accessing support is not well understood within Surrey. This needs to be understood to ensure the support offers are reasonably adjusted.
Crime, concerning behaviour
Recommendation: Data is required to understand quality of access to the police service by people with learning disabilities.
Recommendation: The quality of data regarding people in prison who have learning disabilities is required, ensuring they have access to the support they need. It is understood that HMP SEND now has a Neurodiversity Office, contact to be made and joined up discussion to review the impact of this role.
Community voice
Recommendation: Ensure that these forums offer people with learning disabilities a range of opportunities to have their voices heard and to shape service design and delivery. These need to be separate from partnership meetings, which could result in their voices being unheard.
Recommendation: Ensure that these forums offer carers of people with learning disabilities a range of opportunities to have their voices heard and to shape service design and delivery. These need to be separate from partnership meetings, which could result in their voices being unheard.
Adult Social Care Survey England – 2023/24
Recommendation: The findings, particularly regarding control, social contact, pain and mental health, need to shape commissioning intentions for all types of support.
Recommendation: In relation to the message in the responses to the survey regarding control, Surrey County Council is currently developing a Direct Payments Strategy, which highlights that there is no Individual Service Fund offer in Surrey and commits to exploring whether one should be developed within the first year of the Strategy being Published in June 2023.
Workforce development
Health Education England and Skills for Care are co-ordinating the development of the Oliver McGowan Mandatory Training in learning disability and autism for all health and social care staff. This includes tiers 1 and 2 of the core capabilities framework, which is underpinned by the NICE guidance.
Recommendation: Roll out of Oliver McGowan Mandatory Training.
Appendices
Appendix 1: Definitions
Autism
While autism is not a learning disability, around 4 in 10 autistic people have a learning disability. According to the national Autism Strategy, autism is ‘a lifelong developmental disability that affects how an estimated 700,000 autistic adults and children in the UK (approximately 1% of the population) perceive, communicate and interact with others’. A separate Joint Strategic Needs Assessment that focuses on Neurodiversity will be produced in 2023.
Learning disability – Autism | Autistica | Autistica
Cerebral Palsy
Cerebral palsy as the name for a group of lifelong conditions that affect movement and co-ordination. It’s caused by a problem with the brain that develops before, during or soon after birth (NHS). Cerebral palsy is a condition that affects muscle control and movement. It affects about 1 in every 400 children in the UK, usually caused by an injury to the brain before, during or after birth, but there may be no obvious single reason (Scope)
COVID
Coronavirus disease (COVID-19) is an infectious disease caused by the SARS-CoV-2 virus. Most people infected with the virus will experience mild to moderate respiratory illness and recover without requiring special treatment. However, some will become seriously ill and require medical attention.
Down’s Syndrome
Down’s syndrome is caused by having an extra copy of chromosome 21. People with Down’s syndrome will often have varying degrees of intellectual disabilities (mild to moderate), physical disabilities and other associated medical issues which will be different for each person. The Down Syndrome Act (outlines that there are currently estimated to be around 47,000 people living in the UK with Down’s syndrome (Trisomy 21).
People with Down’s syndrome are living longer. Their average life expectancy is now 60 years, which has significantly increased in recent years. With the right support, people with Down’s syndrome can live more independently, gain employment and contribute to their communities. However, we know that people with Down’s syndrome can have poorer health outcomes compared with the general population and other people with a learning disability. People with Down’s syndrome and their families and carers can often struggle to access services such as speech and language therapy, additional educational support and appropriate levels of social care support.
Fragile X Syndrome
Fragile X syndrome (FXS) is a genetic condition, affecting around 1 in 4000 males and 1 in 6000 females. It can cause a wide range of difficulties with learning, as well as social, language, attentional, emotional, and behavioural problems. Some may experience connective tissue issues such as difficulty breast-feeding, hypotonia, hyperflexibility, flat feet, recurrent ear infections and mitral valve prolapse. FXS is the most common inherited cause of learning disability. (Fragile X Society UK)
Williams Syndrome
Williams Syndrome is a rare congenital disorder caused by a small deletion of part of chromosome 7 that occurs randomly and affects around 1 in 18,000 people in the UK. Williams Syndrome is not a learning disability itself, however around many people with Williams Syndrome have a learning disability . It is non-hereditary and causes distinctive facial characteristics and a wide range of learning difficulties. Infants often have delayed development and can develop physical and mental health problems, including anxiety and depression in later life. People with Williams Syndrome tend to be talkative and excessively friendly towards adults. (Williams Syndrome Foundation)
Appendix 2: Adult Social Care Survey England, 2023/24
The ASC Survey for 2023-24 can be filtered on people with a Primary Support Reason of Learning Disability. The responses to the following questions is as follows:
Q1 – Overall, how satisfied or dissatisfied are you with the care and support services you receive? – 68.2%% of responses were positive stating they were extremely or very satisfied with the care and support they receive and a further 22.4% stated they were quite happy with the way staff help them.
Q2 – Thinking about the good and bad things that make up your quality of life, how would you rate the quality of your life as a whole? – 40.5% of responses were positive stating ‘their life is so good, it could not be better or very good’, and a further 39.6% stated life is good.
Q3a – Which of the following statements best describes how much control you have over your daily life? – 45.5% of responses were positive selecting the statement ‘I have as much control over my daily life as I want’ and a further 43.6% selected ‘I have adequate control over my daily life’.
Q4a – Thinking about keeping clean and presentable in appearance, which of the following statements best describes your situation? – 75.9% were positive stating they feel clean and are able to present themselves the way they like and a further 20.5% stated they feel adequately clean and presentable.
Q5a – Thinking about the food and drink you get, which of the following statements best describes your situation? – 73.6% of responses were positive stating they get all the food and drink I like when they want and a further 26.4% stated they get adequate food and drink at OK times.
Q6a – Which of the following statements best describes how clean and comfortable your home is? – 34.3% of responses were positive selecting the statement ‘My home is as clean and comfortable as I want’ and a further 25.9% selected ‘My home is adequately clean and comfortable’.
Q7a – Which of the following statements best describes how safe you feel? – 78.6% of responses were positive selecting the statement ‘I feel as safe as I want’ and a further 18.8% selected ‘Generally I feel adequately safe, but not as safe as I would like’.
Q8a – Thinking about how much contact you’ve had with people you like, which of the following statements best describes your social situation? – 63% of responses were positive selecting the statement ‘I have as much social contact as I want with people I like’ and a further 28.7% selected ‘I have adequate social contact with people’
Q9a – Which of the following statements best describes how you spend your time? – 67.0% of responses were positive selecting the statement ‘I’m able to spend my time as I want, doing things I value or enjoy’ and a further 24.8% selected ‘I’m able to do enough of the things I value or enjoy with my time’.
Q10 – Which of these statements best describes how having help to do things makes you think and feel about yourself? – 81.8% of responses were positive selecting the statement ‘Having help makes me think and feel better about myself’ and a further 14.5% selected ‘Having help does not affect the way I think or feel about myself’.
Q11 – Which of these statements best describes how the way you are helped and treated makes you think and feel about yourself? – 77.8% of responses were positive selecting the statement ‘The way I’m helped and treated makes me think and feel better about myself’ and a further 20.4% selected ‘The way I’m helped and treated does not affect the way I think or feel about myself’.
Q12 – How often do you feel lonely?- 38.9% of responses were positive reporting they ‘never feel lonely’ and 15.7% said they ‘hardly ever’ felt lonely.
Q13- In the past year, have you generally found it easy or difficult to find information and advice about support, services or benefits? – 24.1% of responses were positive stating it was very easy to find and a further 26.9% stated it was fairly easy to find. 34.3% of responses stated that they never tried to find information or advice.
Q14 – How is your health in general? – 39.6% of responses were positive stating it was very good and a further 28.8% stated it was good.
Q15 – By placing a tick in one box in each group below, please indicate which statements best describe your own health state today.
- Pain or discomfort – 67.9% of responses were positive selecting the statement ‘I have no pain or discomfort‘ and a further 28.4% selected ‘I have moderate pain or discomfort’.
- Anxiety or depression – 62.4% of responses were positive selecting the statement ‘I am not anxious or depressed’ and a further 34.9% selected ‘I am moderately anxious or depressed’.
Q18 – How well do you think your home is designed to meet your needs? – 73.8% of responses were positive stating their home meets their needs very well and a further 16.8% stated their home meets most of their needs.
Q19 – Thinking about getting around outside of your home, which of the following statements best describes your present situation? – 60.6% of responses were positive selecting the statement ‘I can get to all the places in my local area that I want ‘and a further 25.7% selected ‘At times I find it difficult to get to all the places in my local area that I want’.
Appendix 3: Governance Chart
People with a learning disability having a voice – structure
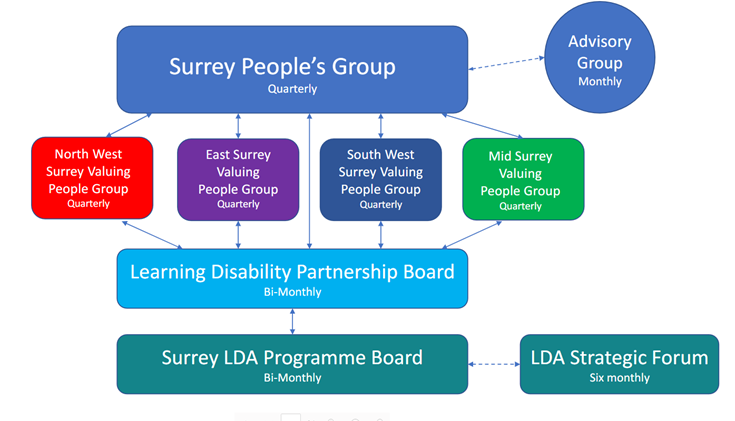
Appendix 4: Safe and well being review findings
Twenty-five reviews were completed overall. Of these 25, 10 were in ICB commissioned adults’ settings. Thematic feedback was prepared and submitted to NHSE. The reviews panel feedback outlined:
- Good practice
- Poor practice
- Thematic Review of Family/Advocacy Feedback
- Thematic Review of findings around Individual’s Safety
- Thematic Review of findings around Individual’s Physical Health Assessment and Treatment
- Thematic Review of findings around Individual’s Mental Health Assessment and Treatment
- Thematic Review of findings around Individual’s Quality of Life
- Thematic Review of findings on how the needs of Children and Young People are being met
- Thematic Review of the Individual’s Feedback
- Thematic Review of the findings around the Individual’s Environment
- Expert by Experience comments of review findings
- Clinical Expert comments of review finding
The following is an overview relating to adults in ICB commissioned beds with learning disabilities and learning disabilities and autism. For CYP the numbers were too small to go into detail.
Good practice:
- Trauma informed approaches referenced
- Calm cards, self-regulation cards, communication passports and zones of regulation cards in specialist environment.
- Within the specialist learning disability environment included: active engagement, verbal de-escalation, arousal ladder, exercise and going out, drama therapy, therapy assisted gardening group, trampoline.
- Evidence of non-pharmacological interventions in preference to medication in line with specialist STOMP guidance within specialist learning disability environments.
- Use of social stories
- Proactive participation in clinical reviews/ CPAs including by the person and their families.
- Multiple examples of positive weight management evident
Poor practice:
- Care planning not being updated/ relevant to current service/ cut and pasted so containing other people’s information
Thematic Review of Family/Advocacy Feedback for those with learning disabilities in specialist learning disability units:
- Vulnerability on discharge (multiple admissions)
- Benefits of hospital environment, full support
- Active support for physical health
- Structure
- Excellent communication between the ward and families
- Negative comparators between independent sector and NHS units featured.
There were no themes from people with learning disabilities in working age adult mental health wards.
Thematic Review of findings around Individual’s Safety for those with learning disabilities in specialist learning disability units:
- People were safe and felt safe.
Thematic Review of Family/Advocacy Feedback
For those with learning disabilities in specialist learning disability units:
- Vulnerability on discharge (multiple admissions)
- Benefits of hospital environment, full support
- Active support for physical health
- Structure
- Excellent communication between the ward and families
- Negative comparators between independent sector and NHS units featured.
Thematic Review of findings around Individual’s Physical Health Assessment and Treatment for those with learning disabilities in specialist learning disability units
- People had high weights and wards had proactive responses
Thematic Review of findings around Individual’s Mental Health Assessment and Treatment for those with learning disabilities in specialist learning disability units
- Positive Behaviour Support strategies and psychology was evident including some good practice within the specialist learning disability environment including active engagement, verbal de-escalation, arousal ladder, exercise and going out, drama therapy has started, therapy assisted re gardening group, trampoline.
- Predominantly medication reviews were in place with good involvement from the person themselves and families.
- Side effect scales were in evidence and some de-prescribing.
- Medication prescription was predominantly for mental illness, with some good practice evidence of non-pharmacological interventions in preference to medication in line with specialist STOMP guidance.
Thematic Review of findings around Individual’s Quality of Life
- The panel considered that there was a mixed level of confidence in regard to quality of life between confident and somewhat confident
- No one had a ‘life plan’ in the formal sense, although some people in specialist wards were completing equivalent such as a ‘life book’.
- Advocacy was on offer within all settings with varied uptake due to self-advocacy and family advocating for their loved one.
- Care plans were person centred and strongly reflected the individuals. Good practice examples of proactive participation in clinical reviews/ CPAs including by the person and their families were also in evidence.
- People did spend time doing things they enjoyed but spending more time out was a key theme for all inpatient settings. People were enjoying their own pursuits as well as learning new ones in the specialist units such as gardening and riding a tricycle. Some frustration was expressed that Covid had impacted eternal activities.
Thematic Review of the Individual’s Feedback from those with learning disabilities in specialist learning disability units:
- Similar feedback to families – largely positive
- Reduction in activities due to Covid and staff shortages
Thematic Review of the findings around the Individual’s Environment
- Specialist learning disability units were clean and smelt fresh. Despite variation in environments, all reviews stated they were appropriate and accessible (including physical mobility aids/ tough furniture), maintained well.
- Unit atmospheres were stated as relaxed. Calmness and space was noted as being down to the unit only having two patients (with a 10 bed occupancy).
Expert by Experience comments of review findings
- Names on the reviews: proforma space for family name.
- Terminology used like self segregation’ , ‘avoidant strategies’ – staying in bed, signs of hopelessness which indicate unmet needs and ‘engagement issues’.
- Concern that people being contained for long periods of time with no treatment
- Hospitals not suitable environments
- Hospitals need to engage with the person’s special interests/ therapies being offered in groups not tolerable for all autistic patients
- Importance of planning discharge
- Far from families
Clinical Expert comments of review finding
- To ensure safe and effective discharges the devil will be in the detail of discharge planning
- Barrier to discharge is good step down in Surrey
- Diagnostic formulation and confusion around people’s diagnoses prevalent and differential diagnosis is very important, as labels are detrimental to a person’s assessment and treatments
- Concern re. accuracy of diagnoses and therapeutic response including a PRN and a ‘soothing’ not treatment oriented offer
- Where expertise isn’t available bring this in via other trusts/ third sector
- Young people as inpatients /link to LAC team to learn from their experience
- Model of support including crisis offer needed within Surrey to prevent admissions including reasonable adjustments to preventative mental health services
Risks / Gaps / Issues
- Expertise was required for (under) 5 (suppressed) people that the system did not readily have access to.
- Social care support and provider market development needed to meet the needs of people with complex circumstances.
- Ordinary Residency disputes featured.
- Concerns regards access to lifelong learning including online within inpatient settings.
- Length of time for Court of protection proceeding if lack capacity.
There were no thematic review of findings on how the needs of Children and Young People are being met due to low numbers.
Safe and well being reviews
Forensic services
Good Practice:
- Use of social stories for life planning.
- Proactive participation in clinical reviews/ CPAs including by the person and their families.
- Multiple examples of positive weight management evident e.g. Dietitian in place and OT support with own/ healthy cooking and menu planning, positive weight loss example, monthly primary nurse sessions to discuss care plans and regular IT sessions, small changes encouraged such as sweetener instead of sugar, supported food choices e.g. veganism, menus RAG rated to highlight healthy choices, high fat / sugar food.
- Friends and Family toolkit within forensic services (consider wide adoption)
Poor Practice
- Staff not being available to meet specific needs relating to trauma (gender/ 1:1)
- Lack of understanding and support for sensory food needs
- Autistic people and inappropriate sensory environments
- Autistic people being offered only group therapies/ activities
- Expertise in autism and eating disorders co-occurring not apparent.
- Refusal of health monitoring not being risk managed well.
- Care planning not being updated/ relevant to current service/ cut and pasted so containing other people’s information
Themes from family members whose loved ones were inpatients in forensic services:
- Communication
- Changed diagnosis
- Contact and visits
- Group activity access for autistic people who were inpatients
- Health
- Staff
- Activity offer (related to staff)
- Discharge
Themes about safety for those inpatients in forensic services:
- Patients said they felt /staff protect them.
- Positive Behaviour Support plans in place
- Some references to the availability of trauma informed care.
- Reported nil/ low PRN prescribing and use under STOMP
- Minor to low physical intervention use/ rare use of seclusion.
- Few incidents of abuse and being perpetrators of abuse to others (staff and patients) (with completed safeguarding referrals).
- Two self-imposed self-segregation both by autistic patients; POSI referral
- A small number of safeguarding referrals and A&E attendances related to self-harm.
Physical Health Assessment and Treatment for those inpatients in forensic services:
- Weight issues/ high BMI’s (up to 41) – varying responses / care planning was not consistent / some good practice
- Some section 17 conditions posed restrictions on accessing health professionals and physical activity.
- Co-occurring eating disorders and autism were not well managed.
- Expected processes and tools to support people with learning disabilities were not consistently evident e.g. Annual health checks, comprehensive health action plan, hospital passport
- Bowel monitoring was lacking
Thematic Review of findings around Individual’s Mental Health Assessment and Treatment for those inpatients in forensic services:
- Confidence levels varied widely.
- Reasonable adjustments were in place e.g. in care plans, including where working diagnosis of autism were in place including adapted treatment programme.
- Communication and sensory needs assessment were not detailed as widespread and absent in one case.
- Non drug methods were on offer including Positive Behaviour Support and psychology, but a theme was an absence of forensic psychologists.
Thematic Review of findings around Individual’s Quality of Life for those inpatients in forensic services:
- The panel considered that there was a mixed level of confidence in regards to quality of life between confident and somewhat confident.
- No one had a ‘life plan’. DEFINE
- Advocacy was on offer with varied uptake due to self advocacy and family advocating for their loved one.
- People did spend time doing things they enjoyed but spending more time out was a key theme for all inpatient settings. People were enjoying their own pursuits as well as learning new ones in the specialist units such as gardening and riding a tricycle. Some frustration was expressed that Covid had impacted eternal activities.
Individual’s Feedback from inpatients in forensic services:
- Limited offer of activity
- Repetition of activities or lack of activity (especially weekends where boredom sets in) with some concern for activities being offered in groups and not suitable/ accessible for autistic people (and activity positively correlating to community leave and discharge planning)
- Size of units /noise within units (again with reference to autistic people)
- Sleep issues (due to mental health/ boredom)
- Being granted and accessing leave (and more leave) with regard to accessing the community
- Health and exercise
- Varied food quality and healthiness /access to cooking.
Thematic Review of the findings around the Individual’s Environment for those inpatients in forensic services:
- Forensic environments and facilities were wide ranging both internally and externally.
- Internally most wards had ADL kitchens.
- Externally the offer ranged widely to include outdoor gyms, clubs, football pitch, exercise equipment, well-maintained gardens, a music shed for listening to, composing and playing music and goats, sports hall, fishing lake, nature trails, cafes and shops.
- The majority of forensic wards including communal areas, bedrooms and other buildings such as activity rooms were clean and well maintained.
- A minor theme of tired looking communal areas which benefit from decorating and refurbishment to modernise including replacing worn down furniture and rugs emerged for two wards.
- Some repairs issues were noted during the observations such as individual rooms e.g. bathroom. One major concern with ongoing smaller maintenance issues arose – a safeguarding alert was potentially being raised in regard to environment (water temperature, draining issues and issues with responsiveness of estates team); host commissioner informed.
- Forensic wards predominantly smelled fresh with cleaners being apparent during observations on many wards.
- During one visit a lower section of a ward was closed as a result of drainage issues and it was reported that there was faeces and water on the floor and therefore closed to all staff, patients and visitors.
- Bedrooms seen were personalised with posters and possessions evident and, in some cases, limited ‘due to the nature of the service’. Consent as not consistently given by all those reviewed usually due to ‘their bedrooms not having been tidied.’
- Environments varied as did the accessibility and signage accessibility all the way from closed ward areas to wide corridors and accessible posters including some patient artwork, festive decorations and notices. In some units (but not consistently) feedback was displayed on walls along with essential information such as how to complain how to access advocacy, information on sepsis, Covid and smoking cessation in easy read formats, how to contact the CQC, take away night menus and notice boards celebrating patient achievements. One unit had rooms with laminated cards identifying preferences and dislikes of the occupying patient.
- One concern was lighting and noise for autistic patients without and with learning disabilities.
- Another concern was a unit with bedroom areas locked off for large part of the day due to two storey environment presenting challenges for observation.
- Forensic wards appeared in the main to be calm and quiet. The calm environment seems to stem from two major themes drawn from activity levels – so wards were calm if patients and staff were engaged in activities (and this was predominantly the case) or if there were no activities and boredom was apparent with minor altercations between staff and patient and lunch punctuating boredom.
- Some concerns with activity levels were reported as staff shortages, lack of initiation by staff. Activities were almost consistently available and wide ranging, e.g. Chess Board, art room, TV lounge, games console, magazines, outdoor gym equipment. OTs present on wards were leading activities.
- In some cases, setting on sites external to wards, both patients and staff were relaxed and enjoying themselves.
- When wards were not observed as calm with a good atmosphere this was due to minor altercations (due to boredom/ waiting), when noise and behaviours from a patient the service found challenging impacting on other patients and significant lack of staff.
Risks / Gaps / Issues
• Expertise was required for (under) 5 (suppressed) people that the system did not readily have access to.
• Social care support and provider market development needed to meet the needs of people with complex circumstances.
• Ordinary Residency disputes featured. Input from social care was raised particularly for those within a forensic setting and due for discharge.
• Concerns regards access to lifelong learning including online within inpatient settings.
• Length of time for Court of protection proceeding if lack capacity.
Appendix 5: Surrey Peoples Group feedback
Questions were asked to the participants of the Surrey Peoples group around a number of topics, word clouds were produced around the feedback.
Friendships:
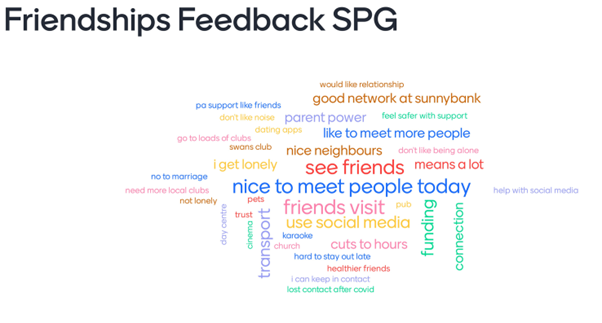
Health:

Home:

Travel:
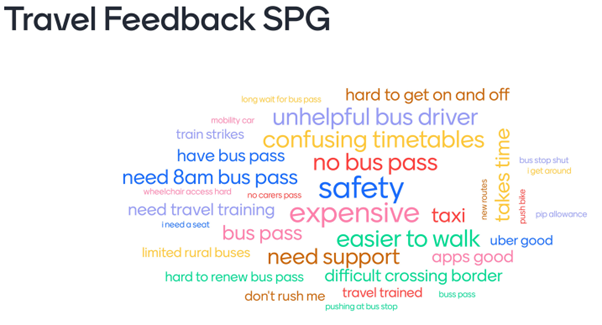
Things you have done that you are proud of:

What makes it hard for you to live the life you want
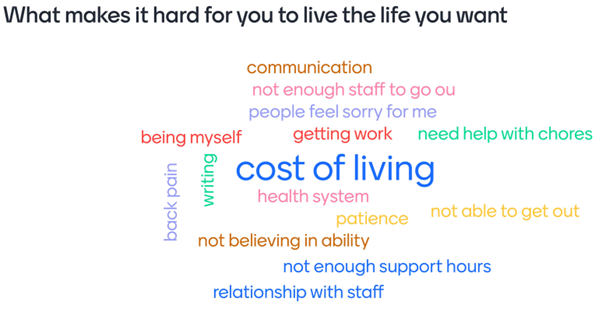
Your hopes and dreams for the future:

Appendix 6: Resources
Access to adult learning
Surrey Adult Learning (SAL) provides inclusive opportunities to promote learning, health and wellbeing. There are seven dedicated adult learning centres in North and South West Surrey:
- Camberley
- Esher
- Guildford
- Molesey
- Sunbury
- Woking
In addition, there are nearly one hundred community venues and an extended online programme.
The courses on offer through Surrey Adult Learning include:
- Creative Art and Craft, Textiles, Mosaics
- Dance, Exercise and Performing Arts
- English and Maths
- ICT, Media, and Photography
- Independence Skills and Healthy Living
- Work Skills.
Supported Learning team offers an entry-level programme of courses for adults with learning disabilities. The courses are designed to:
- improve communication, reading, writing, number, and ICT skills
- promote community participation, engagement, and social inclusion
- enable independence
- develop confidence
- enhance employability skills
- provide opportunities to maintain physical and mental wellbeing.
Some of the courses are free to learners who meet the eligibility requirements. They are also able to offer bespoke courses to organised groups.
Mental health legislation
The Government published a white paper on ‘Reforming the Mental Health Act’ on 13 January 2021 containing proposals to reform the Mental Health Act 1983 (as amended in 2007) in England and Wales. The Government subsequently responded to the consultation on the white paper proposals details of the draft Mental Health Bill, published in June 2022, including the inclusion of most of the review 150 recommendations. The Queen’s Speech in May 2022 included an announcement on draft legislation to reform the Mental Health Act. Lord Kamall, The Parliamentary Under-Secretary of State for the Department of Health and Social Care stated that scrutiny would “commence at the earliest opportunity” and the government’s ambition is “to introduce the Bill in the new year on 28th June 2022.
Within the draft Bill are several amendments to the Mental Health Act 1983:
- Autism and learning disability would not be considered to be conditions for which a person could be subject to compulsory treatment under section 3.
- Changes to the criteria for detention by setting out two new tests with a higher risk threshold
- A new definition of “appropriate medical treatment” to require that the treatment must have a reasonable prospect of alleviating, or preventing the worsening of, the patient’s mental disorder.
- A new duty on the clinician in charge of the patient’s treatment to consider certain matters and take a number of steps when deciding whether to give treatment to a patient under Part IV of the Act.
- A requirement for the clinician responsible for overseeing the patient’s care as a community patient, to be involved in decisions regarding the use and operation of the CTO.
- A new power for Mental Health Tribunal to recommend that the Responsible Clinician reconsider whether a particular CTO condition is necessary, in cases where the Tribunal has decided not to discharge a person from a CTO.
- A new statutory role, the nominated person to replace the current Nearest Relative role in the Act.
- Quicker expiry of the initial detention period under the Act and more frequent review and renewal of the detention.
- Extend the amount of time patients can apply to the Mental Health Tribunal and make automatic referrals more frequent.
(the above taken from: CBP-9132.pdf (parliament.uk))
NHS Long Term Plan » Learning disability and autism
Voluntary sector resources
Accommodation, support, and care
There are many voluntary sector organisations providing a wide range of accommodation, support and care across Surrey, including organisations such as Avenues, The Grange, The Meath, Active Prospects, Whitmore Vale and Dimensions. These organisations tend to offer added value with their ability to fundraise and greater use of volunteers.
Leisure opportunities
Voluntary sector organisations offer a large variety of leisure activities for people with learning disabilities across Surrey. These include, and are not limited to, community choirs, arts and drama clubs, befriending services, and therapeutic gardens. Although such clubs and activities can be found widespread across the county, there is a higher concentration of voluntary sector organisations offering these services in North-West Surrey and Guildford.
Life skills
This category encompasses voluntary sector organisations that provide any form of educational and independent skills support. Services available for people with learning disabilities range from cooking classes to employment support and vocational opportunities. Although some voluntary sector organisations offer life skills support across the county, there is a high concentration of such services in Tandridge, Woking, and Guildford.
Physical exercise
There are many voluntary sector organisations offering opportunities for people with learning disabilities to take part in physical activity. These include walking football, Boccia, swimming, and dancing. Most of these clubs can be found across Redhill and Waverley but some are available in other areas of Surrey.
Transport
Availability of transport services for people with learning disabilities is limited. Some voluntary sector organisations do address this by offering free taxi services, pick up from home to local amenities and shuttle bus transportation across the county, however the general prevalence of such services is low. The biggest concentration of voluntary sector transport services is offered across North West Surrey.
Supporting People’s Voices
There are several user-led and peer facilitated Voluntary sector organisations, enabling people with lived experience to develop and offer training, research input, quality checking, expert by experience policy development.
Surrey Choices
EmployAbility 2021/22
- 468 supported adult job seekers
- 349 young people in education to support in their employment journey
- 508 Keep in Touch (KIT) – people supported to keep their jobs (344 paid jobs, 164 voluntary)
- Worked with 644 Employers across Surrey
- 12.6% of people with LD known to adult social care in work (ASCOF) – average in the UK =5.1%
Future Choices
- 27 young people took part (20 Sept 21 and 7 Jan 22)
- 93% retention and engagement on Future Choices
- 81% attendance on timetabled sessions
- 37% achieved paid outcomes (13 paid jobs found)
- 60% paid outcomes for Autumn 21 starts
- 73% continuing volunteering in their local communities (19 voluntary placements kept)
- 85% continuing with vocational options at end of year (e.g., paid work, volunteering, Supported Internship or supported employment)
- 100% achieved additional personal
Halow
Based in Guildford and Woking, contact [email protected] 01483 447960.
| Service name | Offer | Numbers | LD/A and ages | Innovation/ value /grants |
| Halow’s Social Activities |
Large variety of regular and one-off social activities; in or leaving from Guildford. Subsidised, affordable costs. Some age specific (e.g. 16-21 youth club) and others for all ages. | Variable by activity- ranging from 6 to 40 | LD & A | Includes focus on coproduced core needs, with related funding e.g. sports group. |
| Halow’s Building Futures |
An innovative fulltime community-based learning programme that nurtures the independence, enriches the lives, continues the education, and builds the future of young people. Often SEND funded and now available in Guildford and Woking. |
Up to 12 per group. Capacity is 60 young people across 3 progressive year groups. | LD & A Most people are under 30 |
Innovative programme, and genuine alternative to continuing in sixth form / college. Fee is supported by charitable income. |
| Halow’s A Reason To Get Up |
A sequence of 1 day and half day Mon-Fri offers aiming to enrich the lives and continue the education of service users. Sessions are often fitted in a round other life commitments, be it personal, education, work, etc. Mainly in Guildford, with one offer in Woking. |
Up to 12 per group | LD & A | Affordable fee is supported by specific grant income for each session. |
| Halow’s outreach buddy service |
1:1 work largely in the community. | 1:1 or 1:2 based on need. Capacity based on recruitment. There is a waiting list. |
LD & A | – |
The Sunnybank Trust
Are a community based organisation that has grown from the local history of the closure of Epsom’s long stay hospitals. With over 35 years’ experience, we support around 250 adults with a wide range of learning disabilities across North East Surrey.
We support people with LD to have a voice, access social opportunities, clubs, friendships, opportunities and new skills. We put the person at the heart of all we do to ensure that we focus on the person and their needs at all times.
We provide three key services as well as a twice weekly radio show:
Voices: We provide advocacy, both issue based and long term where needed. With over 100 issues per month we have supported on benefits, accommodation, DOLs, best interest meetings, medical and hospital needs as well as social care support to name a few.
Choices: Our activities and clubs include a monthly disco, drama group, gardening and horticulture at our allotment as well as weekly Coffee and Chats, Pub Quizzes and book clubs.
Futures: We provide a person centred transition service for young adults between 18 years – 30 years (we have an older cut off rate as many young adults need more time to develop, matures and process change. We work with the young adult through team and project work, one to one mentoring and peer led activities and projects. Outcomes include employability, independent living, new skills and project/team skills.
The Sunny Sessions Radio Show: Launched in 2020 and in response to Covid, the twice weekly shows, produced for and by people with LD have an average audience of 160 listeners per show. The shows provide an opportunity for information on key services and events that are relevant for the learning disability community as well as providing opportunities to learn radio production and interview techniques by those participating in the production. Increasingly the shows are connecting and working in partnership with other LD organisations such as Halow Trust, Dance Syndrome, the Orpheus Centre, Mencap to name a few. In addition the show connect with other relevant community groups such as Food Bank and the CAB.
Our services are co designed and co-produced with our partners who also support all our peer evaluations and feedback. 18% of the paid staff have a lived experience of LD, with 10% of the trustee board having a lived experience of LD and 20% having a close family member with LD.
Funders include the National Lottery Community Fund, Lloyds Bank Foundation and Mercers trust.
LinkAble www.linkable.org.uk
Contact – [email protected] (different specific individuals for different age groups – happy to provide this is it’s useful
What is offered – LDA – support between 300 and 400 individuals. Centre is in Woking, Under 18s from anywhere in Surrey can attend, Over 18s from anywhere can attend. We work with our clients to develop our services and we are in regular contact with our client group to understand their feedback.
We run different groups on different days and for different abilities – let me know how much more detailed you would like me to be.
Active Prospects www.activeprospects.org.uk
- Led a Whole Systems Approach to Obesity across Surrey – the first time this public health approach has been applied to learning disabilities. The project brought together statutory, private and public sector organisations with experts by experience to identify issues behind higher prevalence of obesity among the LD community, and come up with ideas and a systems action plan to tackle these issues.
- Developed the EASI Cooking webtool in partnership with JP Morgan Chase. EASI Cooking aims to increase cooking skills among people with Learning disabilities through accessible recipes with easy read instructions; and to increase health awareness through a daily nutritional tracker which can be tailored to meet dietary needs. The webtool enables meal planning and automatic upload to an online shopping basket for easy checkout on five supermarket websites.
- Led a Peer Health Champions pilot in partnership with Surrey County Council. The pilot was co-designed with experts by experience supported by Active Prospects, and trained people with Learning Disability to share health awareness and tips with their peers. It is now being rolled out across Surrey.
- Key Role in two research projects (with University of Surrey and Kent Surrey Sussex Academic Health Network) to improve the experiences of people with learning disabilities and/or autistic people when accessing primary care.
Pro-Active Community https://www.proactivecommunity.org.uk
We are experts by experience and many of us have a learning disability, autism or acquired brain injury. The group is open to everyone who lives within Surrey who would like to meet other people to campaign on issues that surround people with a disability and have fun.
Include https://include.org
Include provides community projects, training and consultancy combining music, creativity and fun – to teach people better ways of including and involving people with understanding or speaking difficulties
Include is all about thinking outside the box: music, games, cake and laughter are our tools to bring inclusive communication to life and to take us one step closer to an inclusive world. To Include someone is to unlock their potential and we guarantee you’ll be surprised at what people can achieve.
Chapter Contacts
Please contact [email protected] with any queries or feedback on this chapter.
References
- 1. Department of Health. (2001). Valuing people: a new strategy for learning disability for the 21st century. HM Stationery Office.
- 2. Emerson, E., & Heslop, P. (2010). A working definition of learning disabilities. Durham: Improving Health & Lives: Learning Disabilities Observatory.
- 3. 9780857257093_INTRO_SUPPORT_PEOPLE_WITH_A_LEARNING_DIFFICULTY.indd (nadp-uk.org)
- 4. Learning Disability (datadictionary.nhs.uk)
- 5. NHS Overview Learning Disabilities: Learning disabilities – NHS (www.nhs.uk) accessed August 2022
- 6. People with learning disabilities in England 2015: Main report (publishing.service.gov.uk)
- 7. Hatton C, Bonardi A, Emerson E, Fox MH, Glover G, Krahn GL, et al. Health surveillance and people with intellectual disabilities. In: Hatton C, Emerson E, editors. Health Disparities and People with Intellectual Disabilities. New York: Elsevier; 2015. p. 1-10.
- 8. Learning disability – Autism | Autistica | Autistica
- 9. Research Evidence on the Health of People with Intellectual Disabilities | Intellectual Disability and Health
- 10. Emerson, E (1995), cited in Emerson, E (2001, 2nd edition): Challenging Behaviour: Analysis and intervention in people with learning disabilities. Cambridge University Press
- 11. Royal College of Psychiatrists, British Psychological Society, Royal College of Speech and Language Therapists, (2007), Challenging behaviour – a unified approach.
- 12. (Challenging behaviour and learning disabilities: prevention and interventions for people with learning disabilities whose behaviour challenges NICE guideline (2015)
- 13. Gypsy, Roma and Irish Traveller ethnicity summary – GOV.UK Ethnicity facts and figures (ethnicity-facts-figures.service.gov.uk)
- 14. England and Wales Census 2021 results released, with Roma included for the first ever time | Travellers Times
- 15. Research on learning disabilities in Gypsy and Traveller communities – Friends, Families and Travellers (gypsy-traveller.org)
- 16. Learning Disability Sex and Relationships Research | Mencap
- 17. Robinson ZM, Marsden D, Abdulla S et al (2020) Supporting people with learning disabilities who identify as LGBT to express their sexual and gender identities. Learning Disability Practice. doi: 10.7748/ldp.2020.e2094 Published online: 08 October 2020
- 18. Autistic individuals are more likely to be LGBTQ+ | University of Cambridge
- 19. Social inclusion of LGBTQ and gender diverse adults with intellectual disability in disability services: A systematic review of the literature – Smith – 2022 – Journal of Applied Research in Intellectual Disabilities – Wiley Online Library)
- 20. Condition Prevalence – NDRS (digital.nhs.uk)
- 21. LeDeR programme at UoB 2015-21 | School for Policy Studies | University of Bristol
- 22. Layout 1 (raceequalityfoundation.org.uk)
- 23. Emerson, E., (2010). Self-reported exposure to disablism is associated with poorer self-reported health and wellbeing among adults with intellectual disabilities in England: A cross-sectional. Public Health 124(12), 682- 689.
- 24. FPLD., (2012). Department of Health – Learning Difficulties and Ethnicity: Updating a Framework for Action. www.learningdisabilities.org.uk
- 25. School census – Special educational needs in England: Special educational needs in England, Academic year 2024/25 – Explore education statistics – GOV.UK
- 26. Education Health and Care plans – SEN2 data collection Education, health and care plans: England 2022 – GOV.UK (www.gov.uk)
- 27. EMIS Search from Surrey GP Practice data, 2018/19 to 2021/22
- 28. Office for Health Improvement and Disparities, Tobacco Control Dashboard, 25 November 2022
- 29. NHS Long Term Plan » The NHS Long Term Plan
- 30. https://www.gov.uk/government/publications/nhs-mandate-2022-to-2023
- 31. People with Learning Disabilities in England 2015 – GOV.UK (www.gov.uk)
- 32. Research Evidence on the Health of People with Intellectual Disabilities | Intellectual Disability and Health
- 33. COVID deaths of people with learning disabilities (publishing.service.gov.uk)
- 34. Coronavirus (who.int)
- 35. Watkins A. COVID-19-Related Deaths in Wales amongst People with Learning Disabilities from 1st March to 26th May 2020. Improvement Cymru; 2020. Accessed March 3, 2020. https://phw.nhs.wales/publications/publications1/covid-19-related-deaths-in-wales-amongst-people-with-learning-disabilities/
- 36. Landes SD, Turk MA, Formica MK, McDonald KE, Stevens JD COVID-19 outcomes among people with intellectual and developmental disability living in residential group homes in New York State. Disabil Health J2020;13:100969. doi:10.1016/j.dhjo.2020.100969. pmid:32600948 CrossRefPubMedGoogle Scholar
- 37. Public Health England. COVID-10: deaths of people with learning disabilities. Published November 12, 2020. https://www.gov.uk/government/publications/covid-19-deaths-of-people-with-learning-disabilities
- 38. BMJ 2021; 374 doi: https://doi.org/10.1136/bmj.n1701 (Published 15 July 2021)Cite this as: BMJ 2021;374:n1701
- 39. Health_inequalities_cardiovascular_disease.pdf (surreycc.local)
- 40. Cardiovascular disease – NHS (www.nhs.uk)
- 41. Glover G and others. Mortality in people with intellectual disabilities in England. Journal of Intellectual Disability Research, 2017. 61(1): p. 62-74
- 42. Draheim CC. Cardiovascular disease prevalence and risk factors of persons with mental retardation. Mental Retardation & Developmental Disabilities Research Reviews, 2006. 12(1): p. 3-12
- 43. Carey IM and others. Health characteristics and consultation patterns of people with intellectual disability: a cross-sectional database study in English general practice. British Journal of General Practice, 2016. 66(645): p. e264-e270
- 44. O’Leary L and others. Early death and causes of death of people with Down syndrome: A systematic review. Journal of Applied Research in Intellectual Disabilities, 2018. 31(5): p. 687-708
- 45. Glover G and others. Mortality in people with intellectual disabilities in England. Journal of Intellectual Disability Research, 2017. 61(1): p. 62-74
- 46. Public Health England, Obesity and weight management for people with learning disabilities: guidance (2020). Available online here.
- 47. Hudson, Bob. ‘From Adolescence to Young Adulthood: the partnership challenge for learning disability services in England’, Disability & Society, 18/3 (2003)
- 48. Southward, Philo and Cooper. ‘What Effect Does Transition Have on Health and Well-Being in Young People with Intellectual Disabilities? A Systematic Review’, Journal of Applied Research in Intellectual Disabilities, 30/5 (2017)
- 49. Public Health England, Health Inequalities_Type2_diabetes https://fingertips.phe.org.uk/documents/Health%20Inequalities_Type2_diabetes.pdf
- 50. Dunkley AJ and others. Type 2 diabetes and glucose intolerance in a population with intellectual disabilities: the STOP diabetes cross‐sectional screening study. Journal of Intellectual Disability Research, 2017. 61(7): p. 668-681
- 51. Health and Care of People with Learning Disabilities Experimental Statistics 2020 to 2021 – NDRS (digital.nhs.uk)
- 52. Health and Care of People with Learning Disabilities Experimental Statistics 2020 to 2021 – NDRS (digital.nhs.uk)
- 53. https://researchbriefings.files.parliament.uk/documents/SN03336/SN03336.pdf
- 54. Willis DS. A decade on: what have we learnt about supporting women with intellectual disabilities through the menopause? J Intellect Disabil. 2008 Mar;12(1):9-23. doi: 10.1177/1744629507086604. PMID: 18337298. – https://pubmed.ncbi.nlm.nih.gov/18337298/
- 55. Oral and Dental Health | Surrey-i (surreyi.gov.uk)
- 56. Oral care and people with learning disabilities – GOV.UK (www.gov.uk)
- 57. Surrey Community Dental Service – Surrey Adult Community Services (surreynehantscommunityservices.nhs.uk)
- 58. UK Parliament (2010) Equality Act 2010
- 59. Heslop P, Blair P, Fleming P, Hoghton M, Marriott A and Russ L. (2013) Confidential Inquiry into premature deaths of people with learning disabilities (CIPOLD): Final report. Bristol: Norah Fry Research Centre, University of Bristol (
- 60. Crawford S and Curran A. (2014) 24 hour postural management for community dwelling adults with learning disabilities. Posture and Mobility: The Journal of the Posture and Mobility Group; 31: 15 to 19
- 61. Heslop P, Blair P, Fleming P, Hoghton M, Marriott A and Russ L. (2013) Confidential Inquiry into premature deaths of people with learning disabilities (CIPOLD): Final report. Bristol: Norah Fry Research Centre, University of Bristol
- 62. Hill S and Goldsmith J. (2010) Biomechanics and prevention of body shape distortion. Tizard Learning Disability Review; 15: 15 to 32
- 63. Educating rehabilitation professionals on clinical skills for postural care services: A scoping review – Faye E McGuire, Jennifer Hutson, Hannah Oldenburg, 2022 (sagepub.com)
- 64. Raising our sights: services for adults with profound intellectual and multiple disabilities (mencap.org.uk)
- 65. NDTi-BILD_Supporting_Older_People_Toolkit_2014.pdf
- 66. Emerson, E, Baines, S, Allerton, L and Welch, V (2012) Health Inequalities and People with Learning Disabilities in the UK: 2012. Cambridge: IHAL. http://bit.ly/1euB7jX
- 67. Report to the National Valuing Families Forum (togethermatters.org.uk)
- 68. Public Health Outcomes Framework – Data – OHID (phe.org.uk)
- 69. Adult Social Care Strategy for people with Physical Disability and Sensory Impairment (PDSI) 2022 to 2027 – Surrey County Council (surreycc.gov.uk).
- 70. Hearing loss | Foundation for People with Learning Disabilities.
- 71. Courtenay, Ken & Murray, Anita. (2015). Foot Health and Mobility in People With Intellectual Disabilities. Journal of Policy and Practice in Intellectual Disabilities. 12. 10.1111/jppi.12105
- 72. Sex: What Is the Big Deal? Exploring Individuals’ with Intellectual Disabilities Experiences with Sex Education – Rachelle Hole, Leyton Schnellert, Gloria Cantle, 2022 (sagepub.com)
- 73. World Health Organization (2015). Sexual health, human rights, and the law. World Health Organization. Sexual Health, Human Rights and the Law
- 74. Sex: What Is the Big Deal? Exploring Individuals’ with Intellectual Disabilities Experiences with Sex Education – Rachelle Hole, Leyton Schnellert, Gloria Cantle, 2022 (sagepub.com)
- 75. Public Health England, Health_inequalities_Pregnancy and birth: https://fingertips.phe.org.uk/documents/Health_inequalities_Pregnancy%20and%20birth.pdf
- 76. NHS Digital (2005) Adults with Learning Difficulties in England, 2003-2004
- 77. Tarleton B, Ward L, Howarth J. 2006. Finding the right support. A review of issues and positive practice in supporting parents with learning difficulties and their children. London: Baring Foundation.
- 78. McConnell D, Mayes R, Llewellyn G. 2008. “Women with intellectual disability at risk of adverse pregnancy and birth outcomes.” Journal of Intellectual Disabilities Research 52:529–35.
- 79. Gaudion A, Godfrey C, Cutts H, Homeyard C. 2013. Mothers with learning disability: access, information provision and ongoing engagement with antenatal care. A pilot project developing antenatal recourses. The Polyanna Project.
- 80. Redshaw M, Malouf R, Gao H, et al. 2013. “Women with disability: the experience of maternity care during pregnancy, labour and birth and the postnatal period.” BMC Pregnancy Childbirth 13:174.
- 81. Malouf R, McLeish J, Ryan S, et al. 2017. “‘We both just wanted to be normal parents’: a qualitative study of the experience of maternity care for women with learning disability.” BMJ Open 7:e015526.
- 82. Delivering Effective Specialist Community Learning Disabilities Health Team Support to People with Learning Disabilities and their Families or Carers- 2015
- 83. Hatton C, Emerson E, Robertson J, Baines S. The Mental Health of British Adults with Intellectual Impairments Living in General Households. J Appl Res Intellect Disabil. 2017 Jan;30(1):188-197. doi: 10.1111/jar.12232. Epub 2015 Dec 9. PMID: 26647916.
- 84. Mencap website: Learning Disability and Mental Health – Mental Health Research | Mencap
- 85. Case example – DCLG’s Indices of Deprivation – Office for Statistics Regulation (statisticsauthority.gov.uk)
- 86. Us Too Project: https://arcengland.org.uk/project-resources/the-us-too-project/
- 87. ONS Domestic abuse prevalence and victim characteristics, 27/11/2024. Domestic abuse prevalence and victim characteristics – Office for National Statistics
- 88. Safelives- Latest Marac National Dataset 2024/2025 – https://safelives.org.uk/practice-support/resources-marac-meetings/latest-marac-data
- 89. HM Inspectorate of Probation Criminal Justice Joint Inspection (2014) A Joint Inspection of the Treatment of Offenders with Learning Disabilities within the Criminal Justice System: Phase One from Arrest to Sentence, London: HM Inspectorate of Probation.
- 90. HM Inspectorate of Probation Criminal Justice Joint Inspection (2015) A Joint Inspection of the Treatment of Offenders with Learning Disabilities within the Criminal Justice System: Phase Two in Custody and the Community, London: HM Inspectorate of Probation.
- 91. Talbot, J. (2008) No One Knows: Experiences of the Criminal Justice System by Prisoners with Learning Disabilities and Difficulties, London: Prison Reform Trust.
- 92. Murphy, G.H., Chiu, P., Triantafyllopoulou, P., Barnoux, M., Blake, E., Cooke, J., Forrester-Jones, R.V.E., Gore, N.J. and Beecham, J.K. (2017a) ‘Offenders with intellectual disabilities in prison: what happens when they leave?’, Journal of Intellectual Disability Research, 61, 957– 68. Wiley Online LibraryCASPubMedWeb of Science®Google Scholar
- 93. Murphy, G.H., Gardner, J. and Freeman, M.J. (2017b) ‘Screening prisoners for intellectual disabilities in three English prisons’, Journal of Applied Research in Intellectual Disabilities, 30, 198– 204.
- 94. Ministry of Justice (2019b) Prison Education & Library Services for Adult Prisons in England Policy Framework. Available at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/791622/prison-education-library-services-policy-framework.pdf
- 95. Wakeling, H. and Ramsay, L. (2019) ‘Learning disability and challenges in male prisons: programme screening evaluation’, Journal of Intellectual Disabilities and Offending Behaviour, 11, 49– 59. CrossrefWeb of Science®Google Scholar
- 96. Ramsay, L., Wakeling, H., De Lucchi, R. and Gilbert, H. (2020) ‘Learning disability screening: impact on prison programmes’, Journal of Intellectual Disabilities and Offending Behaviour, 11, 145– 58. CrossrefWeb of Science®Google Scholar
- 97. LeDeR: Learning from lives and deaths of people with learning disabilities and autistic people – Surrey County Council (surreycc.gov.uk)
- 98. Carmeli, E. and Imam, B. (2014). ‘Health Promotion and Disease Prevention Strategies in Older Adults with Intellectual and Developmental Disabilities’. Front Public Health. 2014 Apr 14;2:31. doi: 10.3389/fpubh.2014.00031. PMID: 24783190; PMCID: PMC3995041