JSNA Smoking, Vaping and Tobacco Control
Smoking, Vaping and Tobacco Control Joint Strategic Needs Assessment
Publication date
This chapter was published in July 2024. Data was updated in April 2025.
Contents
- Executive summary
- Introduction
- National and local strategic context
- Adult smoking prevalence in Surrey
- Health outcomes related to smoking
- Smoking in children and younger people
- Other tobacco products
- Vaping
- Economic impact of smoking
- The role of Trading Standards and tobacco control
- Environmental impact
- Stop Smoking Support (SSS) in Surrey
- Resident engagement
- System engagement
- Recommendations
- References
- Acknowledgements
Executive summary
Tobacco Control is an umbrella term often used to describe a broad range of interventions that aim to reduce smoking prevalence, and/or reduce exposure to second-hand smoke and the morbidity and mortality it causes.
This chapter does not consider Cannabis as this is covered under the Substance Misuse JSNA chapter, where it is covered in more detailed as part of the wider treatment programme for adults misusing substances in Surrey. Of all adults in treatment in Surrey, the most common reported substances were opiates, alcohol and cannabis.
Introduction
“Smoking is one of the biggest preventable causes of early death and illness and contributes to the biggest gap in healthy life expectancy between the rich and the poor.”
Smoking causes 78,000 deaths a year in the UK, increases the risk of developing over 50 serious health conditions and leaves countless individuals living with debilitating smoking-related illness.[1] The burden that smoking places on health and care providers in Surrey is significant with 6,331 hospital admissions a year being attributed to smoking.[2]
Health inequalities are preventable, systematic and unfair differences in health outcomes between different population groups. Smoking is the single largest driver of health inequalities in England, particularly influencing the life expectancy gap seen between high and low deprived populations with the more deprived areas typically having higher smoking rates.[3] Spending on tobacco will consume a relatively high proportion of the household income for people with low incomes who smoke. In turn local poverty levels can be attributed to both the cause and an effect of smoking. Those with mental health conditions, substance misuse service users and routine and manual workers also have higher smoking rates than the Surrey average, and due to smoking’s harmful effects, groups with higher smoking rates tend to experience poorer health outcomes.
Children are influenced by what they see around them and where smoking is more visible in home environments, communities and workplaces, there is a greater likelihood that smoking will be taken up by the next generation. Children and young people (CYP) who are from smoking households are up to three times more likely to become smokers themselves compared to their peers who come from smokefree households.[4]
In addition to the impact on health inequalities, smoking brings a huge financial cost to wider society. Action on Smoking and Health (ASH) estimates that each year smoking costs England £46bn and on average £2,486 is spent per smoker on tobacco per year.[5]
National and local strategic context
National strategies
Knowledge, policies and attitudes towards smoking have changed immensely over the past several decades.
In 2017, the Government published its Tobacco Control Plan for England. This contained a vision of a smokefree generation (prevalence of 5% or lower) with a plan for action to reduce both the overall prevalence of smoking and the inequality gap associated with it. Actions included a focus on prevention, supporting smokers to quit, eliminating variations in smoking rates and ensuring enforcement e.g. high duty rates for tobacco products.
The 2019 NHS Long Term Plan contains the following actions relevant to smoking:
- By 2023/24 all persons who smoke that are admitted to hospital should be offered NHS-funded tobacco treatment services.
- Introduction of focused smoking related sessions and treatments for expectant mothers and their partners.
- Introduction of a universal smoking cessation offer amongst specialist mental health services.
In September 2023, the Government published the Major conditions strategy: case for change and our strategic framework, which recognises smoking as one of the principal lifestyle drivers of ill-health and disease. Smoking is also recognised as a risk factor in the six groups of major conditions that are the focus of the strategy: cancers, cardiovascular disease (including stroke and diabetes), musculoskeletal disorders, mental ill health, dementia, and chronic respiratory disease (CRD). The case for change sets out several things the Government is currently doing to address behavioural and other risk factors driving ill health, including a focus on smoking cessation and tobacco control, and several priority areas for ongoing development ahead of publishing the final strategy.
In October 2023, the UK government proposed a new policy change, Stopping the start: The plan to create a smokefree generation. The new legislation proposes a number of changes to further prevent people from becoming addicted to smoking and address the challenge of youth vaping.
The proposals are:
- A smokefree generation: legislation to make it an offence to sell tobacco products to anyone born on, or after 1st January 2009. It will also be an offence for anyone at the legal age to purchase tobacco products on behalf of someone born on, or after 1st January 2009.
- Helping current smokers to quit: increased investment in local authority led local stop smoking services for the next five years; additional money for national anti-smoking campaigns; funding to roll out the new national ‘Swap to Stop’ scheme; funding to provide evidence-based financial incentives to support all pregnancy smokers to quit.
- Protecting children from vaping: ensuring the balance is right between protecting children and supporting adult smokers to quit. The proposal includes restricting flavours, regulating point of sale displays, packaging and presentation.
- Enforcement: increased investment to strengthen enforcement activity to stop underage sales and tackle the import of illicit tobacco and vaping products.
In March 2024, a Tobacco and Vapes Bill was introduced to the Commons, and whilst there is cross party support in favour of this Bill, there are several stages of the process still to take place before it is formalised.
Smoking cessation has also been identified as a key intervention that positively impacts all five clinical areas outlined in the NHS England Core20PLUS5 framework to reducing health inequalities at both national and system level. The below image in figure 1 outlines this framework and associated conditions.
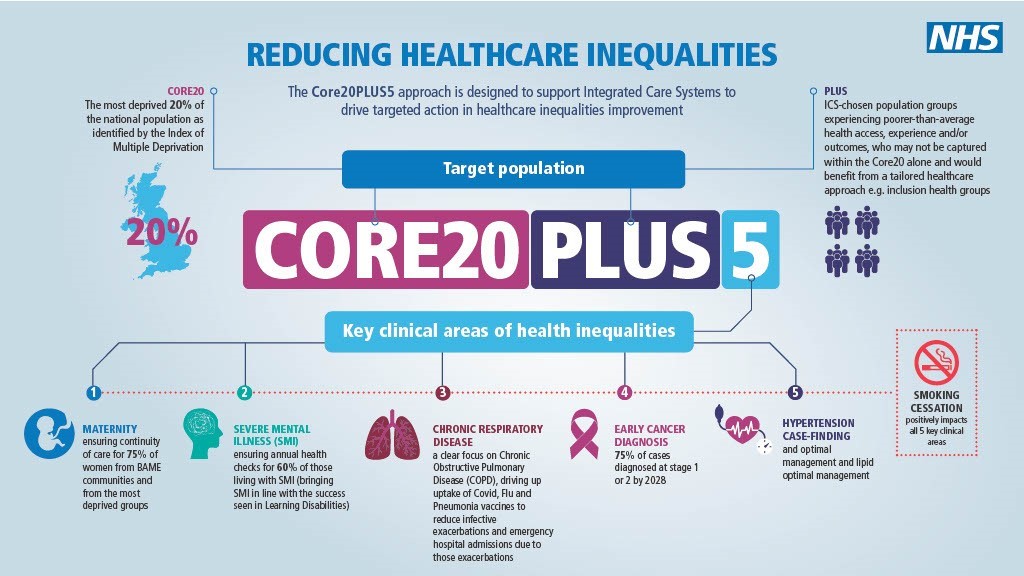
Figure 1: Core20PLUS5 Infographic
Local strategies
Surrey works towards specific strategies which help to align and focus our work alongside national smoking ambitions.
Surrey County Council’s 2023-2028 Organisation Strategy has a purpose “to tackle inequality and make sure no one is left behind”. It sets out four priorities to deliver this with the objective ”tackle health inequality” being one of those priorities and will be delivered through partnerships and service delivery via the Health and Wellbeing Board.
Surrey’s Health and Wellbeing Strategy 2022 specifically addresses smoking under priority one ‘Supporting people to lead healthy lives by preventing physical ill health and promoting physical well-being’, with a key outcome to ensure substance misuse is low, including smoking.
Tobacco smoking has been ”firmly established as the largest cause of health inequality accounting for 50% of the difference between least and most deprived communities.” Providing a way for residents to stop smoking in an effective manner will contribute to the council’s goal of tackling health inequalities.
The Surrey Tobacco Control Strategy 2023-26 was published in Autumn 2023. The strategy sets out why and how Surrey needs to work together to reduce the harmful effects of tobacco. Delivering a high quality, specialist stop smoking service is included in one of the five local priorities. To achieve our strategies ambitions, we have set the following priorities:
- Supporting all tobacco users to quit
- Evidence-based education
- Local regulation and enforcement
- Creating smokefree environments
The commitment in the Surrey Health and Wellbeing Strategy is also reflected in ambition one (Prevention) of the Surrey Heartlands Integrated Care Strategy, which builds on and brings together strategies across the health and care system.
The Surrey Heartlands Joint Forward Plan and Frimley Health and Care Joint Forward Plan, sets out how the local NHS, partner local authorities, voluntary, community and social enterprise (VCSE) sector, Places and Neighbourhoods will deliver their Integrated Care Strategies and NHS Long Term Plan commitments for the local population. Smoking is specifically mentioned in sections on cardiovascular disease, respiratory, and maternity, including the commitment to reduce the prevalence of smoking in Surrey. Specifically in Frimley the Living Well Strategic Ambition, including a commitment to reducing the prevalence of smoking across the Frimley ICS.
The Frimley Integrated Care (ICS) Creating Healthier Communities Strategy
The Surrey Heartlands (ICS) Integrated Care Strategy
Adult smoking prevalence in Surrey
It is estimated by the Department of Health and Social Care that there are around 86,542 smokers in Surrey. Smoking prevalence across Surrey in 2023 was 7.3%, compared to the 2011 value of 14.9%. This demonstrates a decrease of 7.6% over an 11-year period although a similar prevalence of 7.8% was seen in 2021. Surrey’s 2023 smoking prevalence represents a lower value than England (11.6%) and is also below the South East average (10.6%) as seen in figure 2.[2]
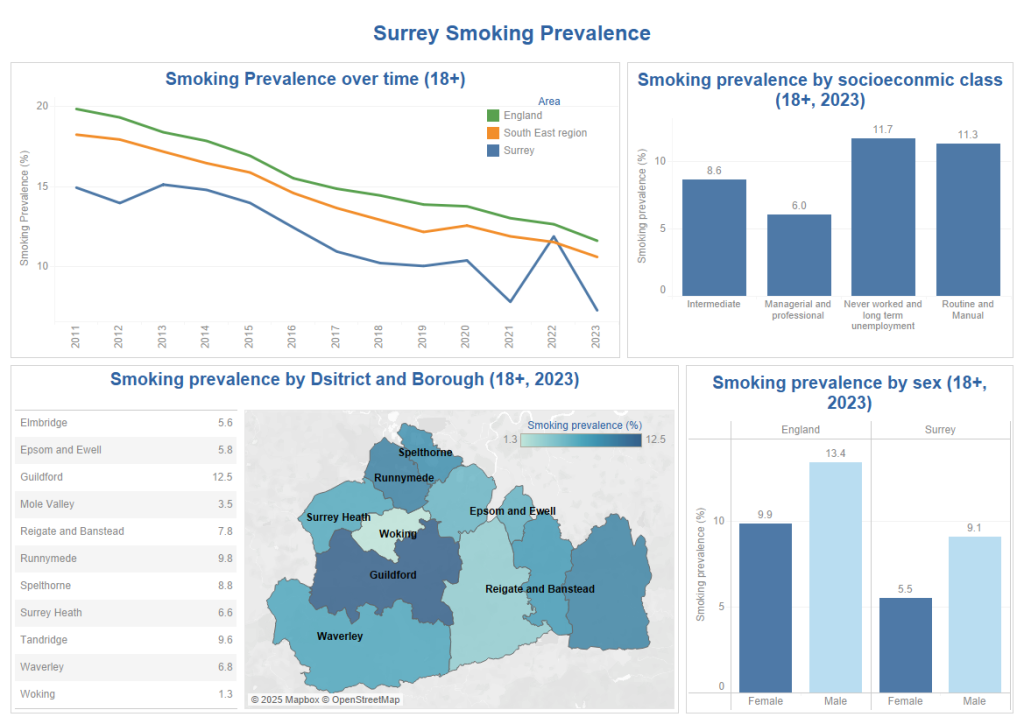
Figure 2: Surrey Smoking Prevalence
Despite gradual declines in the overall smoking prevalence in Surrey over the last 10 years, it is evident that there have been some inconsistencies in reporting over the last three years. Whilst it is difficult to know exactly why there has been a sudden spike in smoking prevalence in 2022, we know there were changes in the way estimates were calculated from 2021. Changes in smoking habits during the pandemic years may also be an influencing factor.
Health inequalities persist in those who smoke.
Smoking by socio-economic status:
Socioeconomic class is a factor that shows major differences in smoking prevalence across Surrey. Around 11.3% of people within a routine and manual socioeconomic class smoke which is nearly two times higher than the prevalence amongst those with a managerial and professional socio-economic class (6.0%).
Smoking by sex:
Looking at sex, male smoking prevalence across Surrey in 2023 was 1.7 times larger than the female smoking rate. This prevalence gap between sexes is similar to England, where the male prevalence is roughly 1.35 times larger than female prevalence.
Smoking by geography:
In figure 2, smoking prevalence by district and borough level across Surrey varies, from the lowest being 1.3% in Woking and the highest of 12.5% in Guildford.[2]
Figures 3 to 8 present the percentage of registered smokers by practice and by NHS Place. This data is based on the Quality Outcome Framework (QOF) indicators and has been pulled from Graphnet and therefore represents a snapshot in time, February 2024.
Practices highlighted in lighter blue represent those that serve the Key 21 Neighbourhood areas. Twenty-three of the practices across Surrey demonstrate more than 10% of their registered patients are smokers, with the highest being 14.9%.
Practices in North East Hants and Farnham and Surrey Heath will show a slightly higher percentage of registered smokers due to palliative care/end of life patients being excluded from the practice totals. This is because the data was gathered using a different methodology than the Surrey Heartlands Practices.
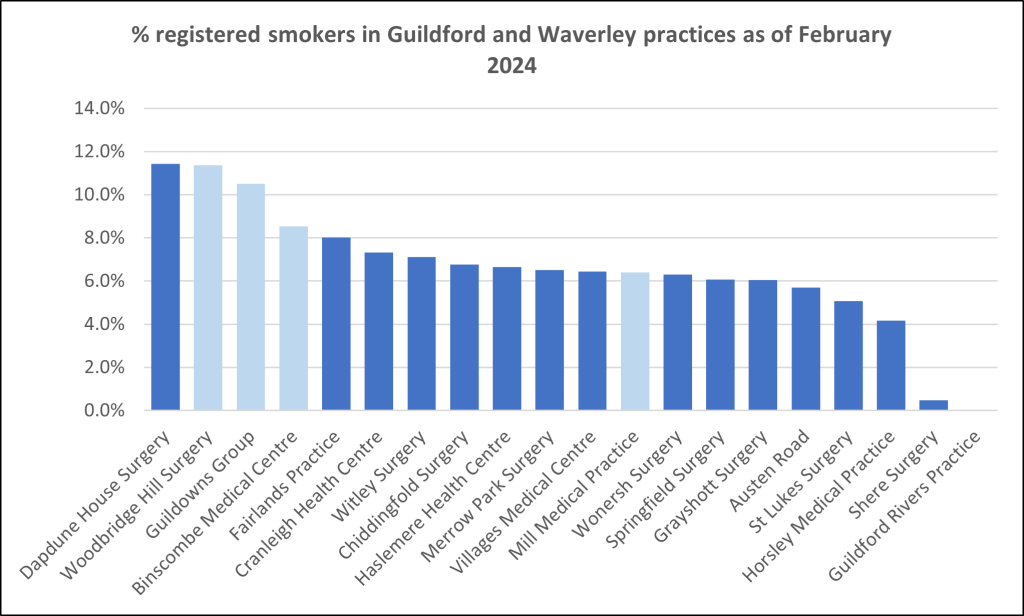
Figure 3: Percentage of registered smokers in Guildford and Waverley with practices highlighted in lighter blue representing those that serve the Key 21 Neighbourhood areas.
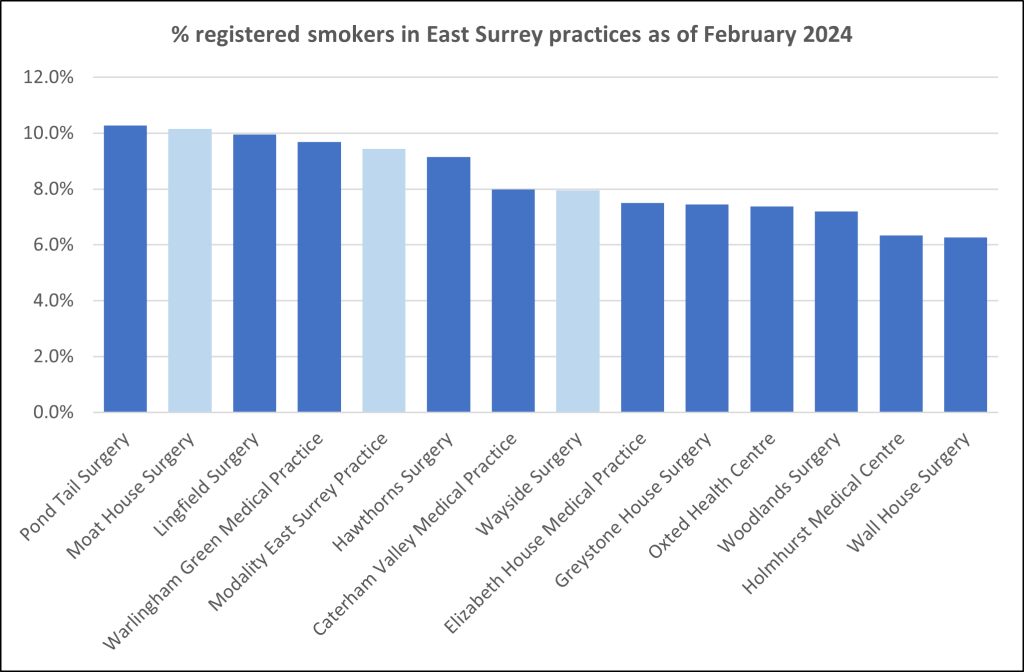
Figure 4: Percentage of registered smokers in East Surrey with practices highlighted in lighter blue representing those that serve the Key 21 Neighbourhood areas.
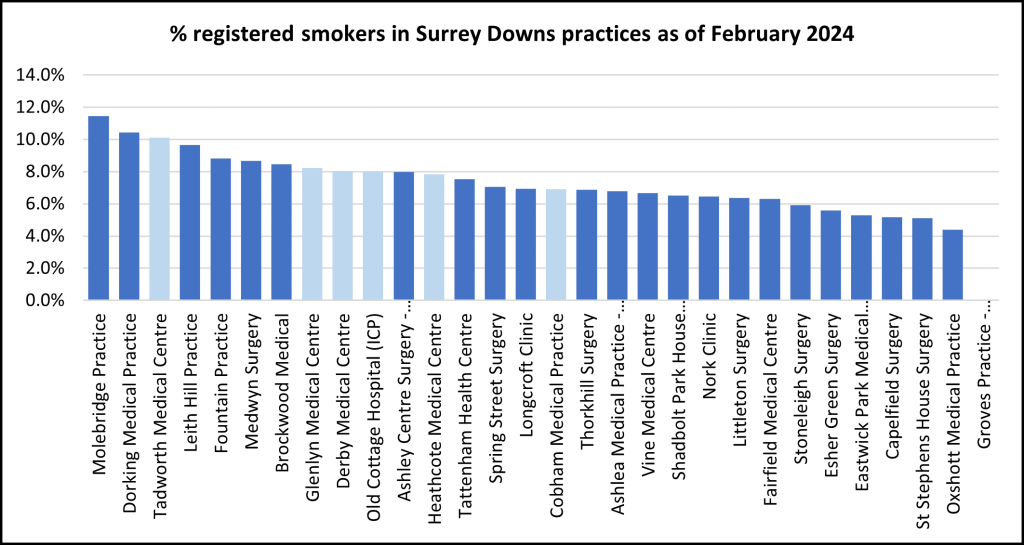
Figure 5: Percentage of registered smokers in Surrey Downs with practices highlighted in lighter blue representing those that serve the Key 21 Neighbourhood areas.
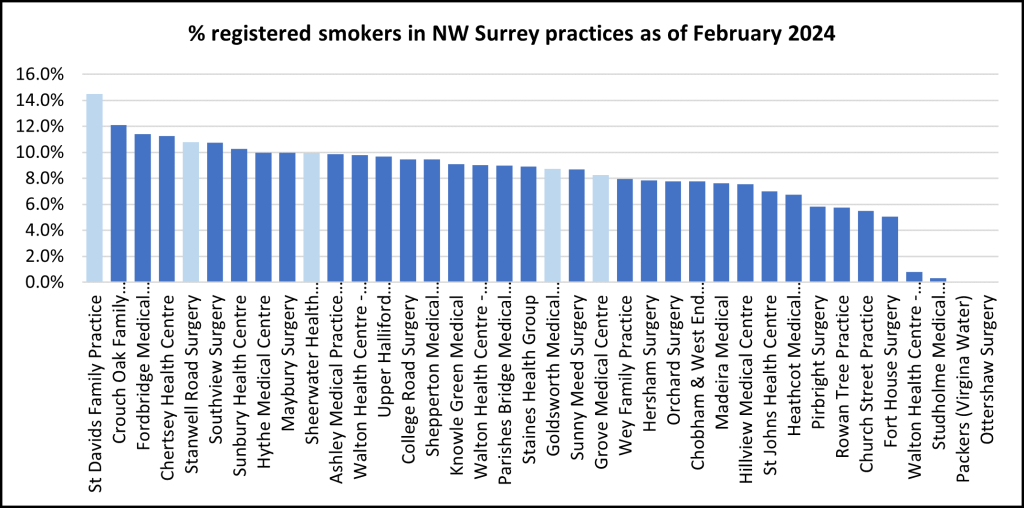
Figure 6: Percentage of registered smokers in North West Surrey with practices highlighted in lighter blue representing those that serve the Key 21 Neighbourhood areas.
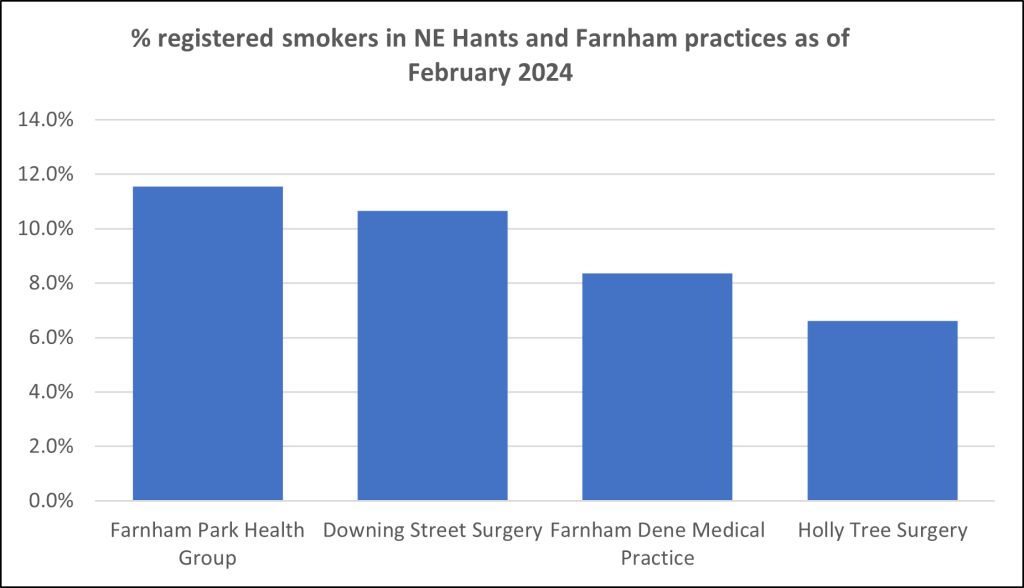
Figure 7: Percentage of registered smokers in North East Hants and Farnham with practices highlighted in lighter blue representing those that serve the Key 21 Neighbourhood areas.
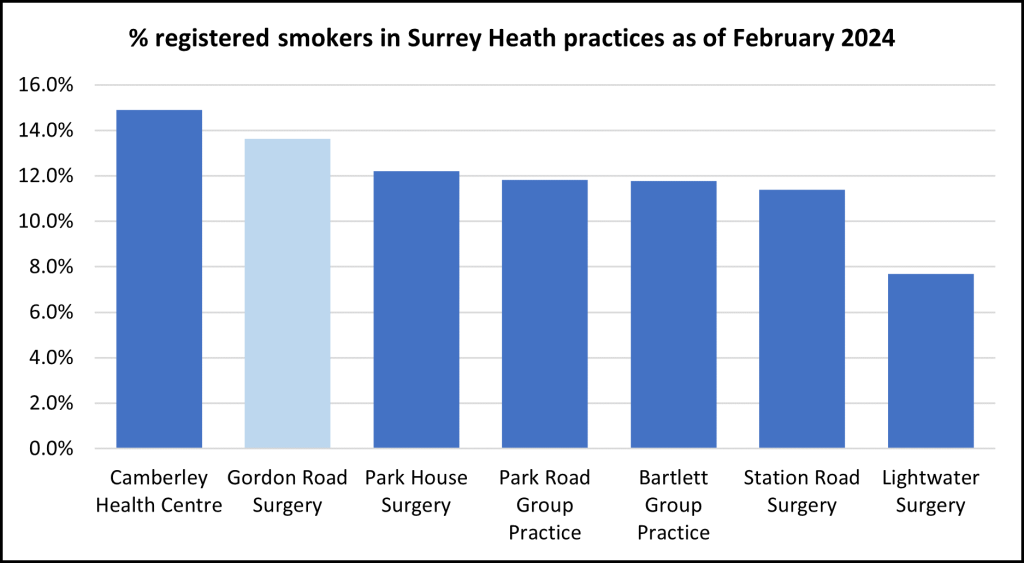
Figure 8: Percentage of registered smokers in Surrey Heath with practices highlighted in lighter blue representing those that serve the Key 21 Neighbourhood areas.
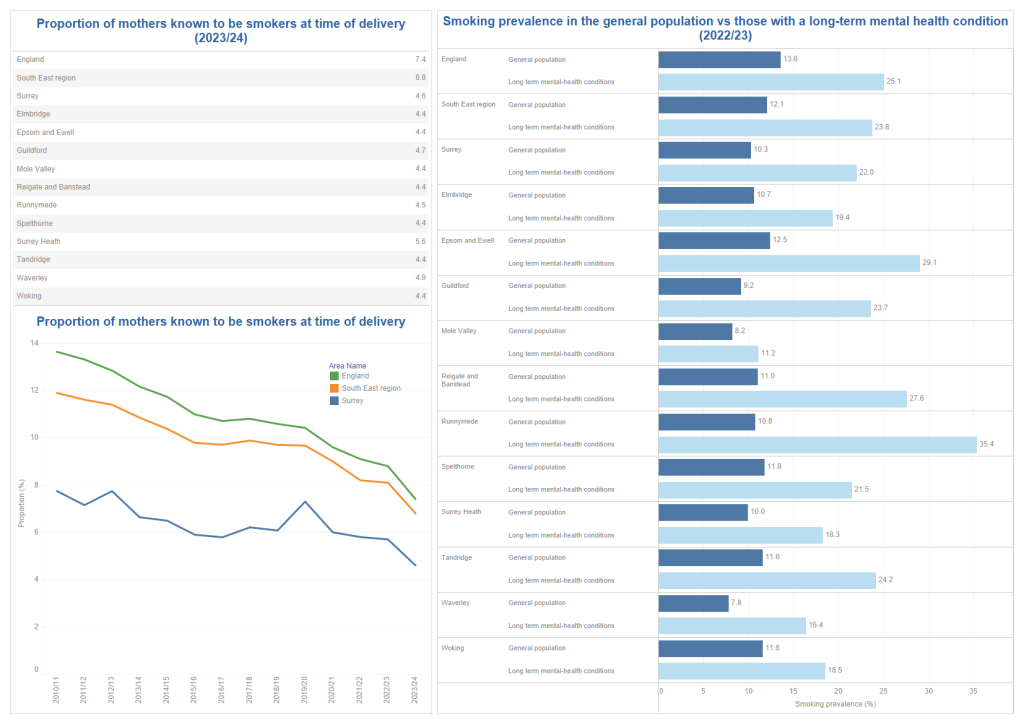
Figure 9: Smoking prevalence in priority populations
Smoking and Mental Health
As seen in figure 9, smoking prevalence amongst those with a long-term mental health condition across England, the South East and Surrey is statistically significantly higher than prevalence amongst the general population (GP Patient Survey (GPPS)). In the 2022/23 financial year (FY) smoking prevalence is roughly 1.8x higher in those with a long-term mental health condition across England (25.1% vs 13.6%) and roughly 2x higher across the South East (25.2% vs 12.1%) and 2.1x higher in Surrey (22% vs 10.3%), than the general population. [2]
Looking within Surrey, the difference in smoking rates between populations varies greatly within district and borough council areas. In Mole Valley, smoking rates in those with long-term mental health conditions are only 1.3x higher (11.2% vs 8.2%) than the general population compared to Runnymede where the prevalence is around 3.3x higher (35.4% vs 10.8%).
Smoking in Pregnancy
Smoking during pregnancy is well known to affect not just the mother but also the development of the baby, along with contributing to complications during pregnancy. As of the 2023/24 FY, 7.4% of mothers in England were known to have been smokers at time of delivery (SATOD), compared to 6.8% of mothers in the South East and 4.6% within Surrey.
There is only small variation in this number across Surrey’s district and borough council areas (figure 9) with the highest rate being in Surrey Heath and Waverley (5.6% and 4.9% respectively) and the lowest in Woking, Tandridge, Spelthorne, Reigate and Banstead, Mole Valley, Epsom and Ewell, and Elmbridge (4.4%).[2]
There has been a steady decrease over the last 10 years in the proportion of mothers known to be SATOD across England, the South East and Surrey. However, over the last 5 years this decrease has slowed, especially in Surrey. Comparing the 2015/16 FY year with the 2023/24 FY, the rate has dropped 3.6% across England, 3.0% across the South East but there has only been a 1.3% reduction in Surrey. This is likely to be due to Surrey’s already low number of women who are still SATOD which is currently around 460. The dedicated tobacco dependency teams within maternity services across Surrey will also be contributing to the low SATOD rates.
Smoking is highly associated with Sudden Unexpected Death in Infancy (SUDI). The Surrey Child Death Review Partnership Thematic Review of Sudden Unexpected Death in Infancy 2014 – 2020, found that of the 20 babies included in the review 60% had a parent or carer who smoked. This is similar to national data. In the report “Sudden and Unexpected Deaths in Infancy and Childhood” the National Child Mortality Database (NCMD) found that smoking in pregnancy was recorded as a modifiable factor in 50% of the deaths in infants under the age of one, whose deaths remained unexplained after investigations.
Smoking in pregnancy was recorded in 50% of the deaths. At a population level, maternal smoking during pregnancy has fallen over recent decades to 11% but is three-fold higher among the families where there were explained deaths in babies and children (32%) and five-fold higher among the unexplained deaths (50%).
Those in treatment for alcohol or drug use
Adults engaged with treatment in Surrey during 2021/22 who smoke tobacco was between 53% (alcohol) and 75% (opiates). This was higher than the national average of 45% (alcohol) to 67% (opiates).
Smoking by ethnicity
Further work is required to understand the level of smoking for different ethnicities within Surrey as data is not currently collected by ethnicity. Ethnicity data is only available for people accessing the stop smoking service.
However, data from the Office for National Statistics (2019)[7] shows that for both men and women, the highest smoking prevalence was seen in the mixed ethnic group with large differences between sexes particularly in Asian (13.9% in men and 2.9% in women), Chinese (12.6% in men and 4.0% in women) and Black (12.9% in men and 6.9% in women) groups.
Health outcomes related to smoking
Action on Smoking and Health have identified the impact of smoking on Core20PLUS5 populations across the NHS Surrey Heartlands Integrated Care Board (ICB) and NHS Frimley ICB footprint. Both figure 10 and 11 highlight that all five clinical areas, maternity, severe mental illness, chronic respiratory illness, early cancer diagnosis and hypertension are impacted by smoking.
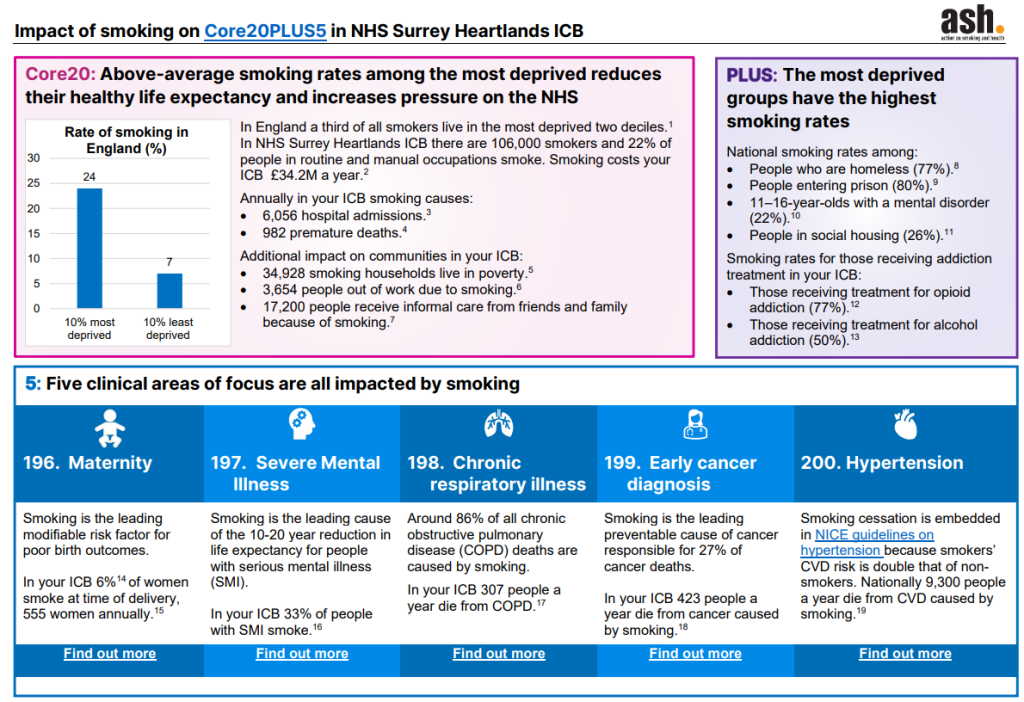
Figure 10: Impact of smoking on Core20PLUS5 in NHS Surrey Heartlands ICB
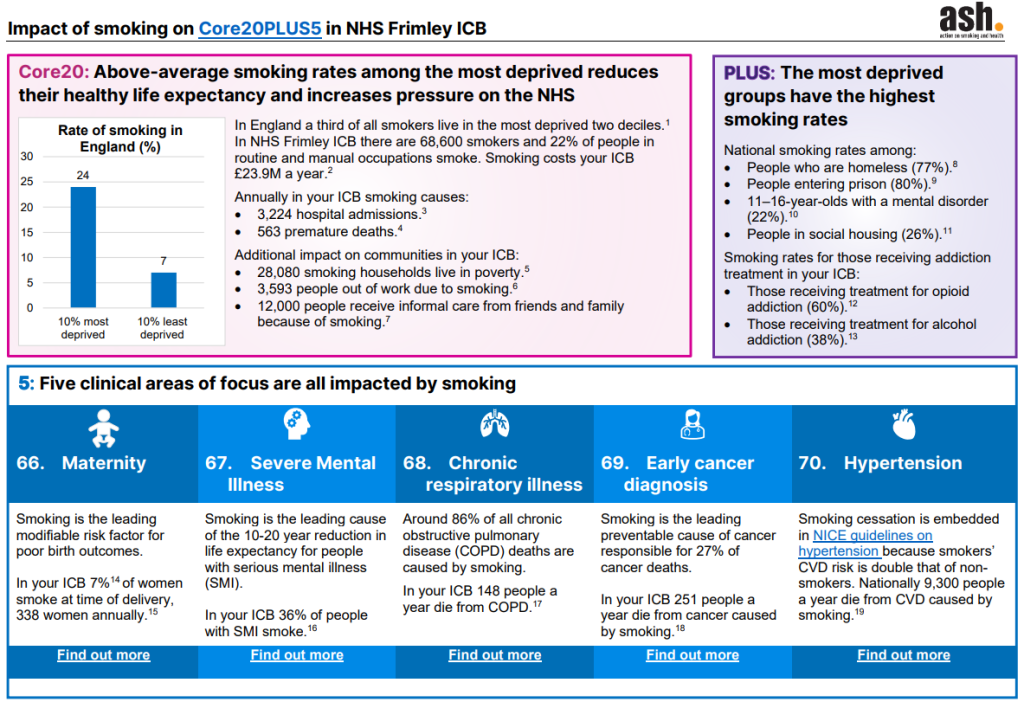
Figure 11: Impact of smoking on Core20PLUS5 in NHS Frimley ICB
Mortality
The impact of smoking on mortality is likely to be as a build up of poor health outcomes over many decades and note should be taken that it is not related to current practices or a reflection on current prevalence rates. The smoking attributable mortality rate per 100,000 population across Surrey was 138.7 per 100,000 for the period 2017 to 2019. This is lower than both the England and South-East values (202.2 per 100,000 and 170.9 per 100,000 respectively) for the same period. Across England there is a clear relationship between deprivation and smoking attributable mortality with the rate in the most deprived areas being roughly 2x that in the least deprived area.[2]
Chronic Obstructive Pulmonary Disease
Smoking is said to be responsible for 9 in 10 diagnoses of COPD. In 2021 to 2023 the rate of COPD attributable mortality per 100,000 population across Surrey was 29.3 per 100,000 which is below both the South East and England values (37.8 and 43.9 per 100,000 respectively)[2]. A lot of variation is seen in COPD mortality looking at Surrey districts and borough council areas. Runnymede has the highest at 41.1 per 100,000 followed by Surrey Heath and Spelthorne with rates of 34.8 per 100,000 and 34.4 per 100,000 respectively. Epsom and Ewell and Mole Valley have the lowest rates per 100,000 at 26.4 and 22.3 respectively.
Cardiovascular Disease (CVD)
Research has clearly established cigarette smoking as a risk factor for cardiovascular disease incidence and mortality, with smoking increasing the risk of death from CVD by up to three times. Smoking can increase your risk of blood clots, an instant rise to your heart rate and blood pressure and reduced the amount of oxygen delivered to the rest of your body.[8]
In England there are 6.4 million people living with CVD, which contributes to around 140,000 deaths each year. It is estimated that 64,000 of these deaths can be attributed to smoking-related causes.[9]
Around 120,000 people are living with heart and circulatory disease in Surrey, 34,000 of those are people living with CVD, causing around 230 deaths each month.
Around 169,000 people have been diagnosed with high blood pressure which is another leading risk factor of CVD.
Cancer
Tobacco is the largest preventable cause of cancer and death in the UK. The link between smoking and cancer is very clear. It causes at least 15 different types of cancer, including two of the most common types: lung and bowel cancer. Other cancers caused by smoking include: nose and sinuses, mouth, larynx (voice box), pharynx (upper throat), oesophagus (food pipe), cervix and ovary to name a few.[10]
Seven in ten cases of lung cancer are said to be caused by smoking. Data from 2021 to 2023 shows the rate of lung cancer attributable mortality per 100,000 population across Surrey was 32.3 deaths per 100,000. This is below both the South East and England values (40.3 and 47.5 per 100,000 respectively). A lot of variation is seen in lung cancer mortality looking at Surrey’s districts and borough council areas. Runnymede has the highest rates at 39.1 per 100,000 compared to Mole Valley with a rate of 25.6 per 100,000. [2]
Asthma
Adult smokers are at higher risk of developing asthma compared to non-smokers. QOF data from 2022/23 shows there are 71,380 people aged 6 and over with asthma in Surrey[2]. Parental smoking is a cause of asthma in children, with a review by the Royal College of Physicians noting that household smoking increases the risk of asthma in children by about 50%[6]. In 2021/22, Surrey’s rate for hospital admissions for asthma (under 19 years) was 84.0 per 100,000, this was below the England average of 131.5 per 100,000.
Pneumonia
Smoking and exposure to tobacco smoke are known risk factors for community acquired pneumonia (CAP). There is evidence that people who smoke are twice as likely as non-smokers to get pneumonia; that smokers are at a higher risk of being hospitalised repeatedly with pneumonia; and that there is a higher risk of respiratory infections in children whose parents smoke and in adults exposed to second-hand smoke.
Ill Health
In the 2019/20 FY, there were 882.7 smoking attributable hospital admissions per 100,000 population across Surrey which is less than both the South East and England values (1,011.5 and 1,398.0 per 100,000 respectively).
The Surrey rate for emergency hospital admissions for COPD (35+) is 177 per 100,000 in 2023-24. This is less than both the South East and England values (260 and 357 per 100,000 respectively).[2]
Smoking in children and young people
“The younger the age of uptake of smoking, the greater the harm is likely to be, because early uptake is associated with subsequent heavier smoking, higher levels of dependency, a lower chance of quitting, and higher mortality. Children and adolescent smoking causes serious risk to respiratory health, short and long term.” [4]
Smoking prevalence in children and young people
It is estimated that each year around 207,000 children in the UK start smoking. Among adult smokers, about two-thirds report that they started smoking before the age of 18.
Figure 13: Smoking prevalence in 11-15 year olds
The proportion of children who have ever smoked continues to decline. In 2021, 12% of 11-15 year-olds (16% in 2018) had smoked at least once (figure 13); the lowest proportion since the survey began in 1982 when 53% had tried smoking. In the past decade the proportion of children who have ever smoked has halved from 25% in 2011 to 12% in 2021. The prevalence of regular smoking also increases with age, from 0.1% of 11-year-olds to 3.3% of 15-year-olds.[4]
Children are also more susceptible to the effects of passive smoking. In 2021, a little over half (52%) of pupils reported having some level of exposure to second-hand smoke (figure 14) with 48% experiencing second-hand smoke in the home (theirs or others’). About one in ten (11%) of all pupils were exposed to second-hand smoke in the home every day or most days. One in five pupils (20%) experienced second-hand smoke in a car.[11]
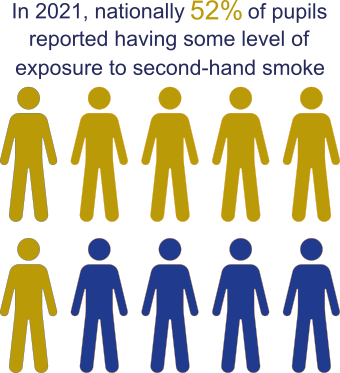
Figure 14: Percentage of pupils exposed to second-hand smoke
Surrey data
In Surrey, smoking prevalence data is available from the health-related behaviour survey (HRBQ).[12] This was conducted during the spring and summer terms of 2022 with 8,197 pupils from 39 primary schools and 11 secondary schools providing a snapshot of what life is like for young people in Surrey. The survey was also conducted in 2019 and comparative data has been provided where possible.
In primary schools:
- One percent of Year 6 pupils have tried smoking in the past or smoke now (this has not changed since 2019).
- Zero percent of Year 6 pupils smoked in the 7 days before the survey.
In secondary schools:
- Ten percent of pupils have smoked in the past or currently smoke (this has reduced from 16% in 2019).
- One percent of pupils responded that they smoke ‘regularly’.
- Of the 22 pupils who smoke regularly, 36% said they would like to give up.
- Two percent of pupils responded that they have smoked in the seven days before the survey.
Other tobacco products
Shisha
Smoking shisha (or hookah) involves burning wood, coal or charcoal to heat tobacco (or flavoured tobacco, ‘maassel’). This produces smoke, which bubbles through a bowl of water or other liquid, into a tube or pipe, and is inhaled through a mouthpiece.
Shisha smoking is a legal activity and is popular in Southeast Asian, Middle Eastern and North African communities. It is increasingly common in England, especially among young people from all ethnic minority backgrounds.
There is currently no available data for shisha smoking prevalence in Surrey.
There is a misconception that because shisha smoke is inhaled through a waterpipe, it is ‘safer’ than traditional cigarette smoking. This is not the case, and evidence shows shisha is not a safe alternative to cigarette smoking. Shisha smokers are at risk of the same kind of diseases caused by cigarette smoking including cancer, heart disease and respiratory disease, as well as adverse effects during pregnancy. During a typical shisha session (which normally lasts 20-80 minutes) a shisha smoker can inhale the same amount of smoke as a cigarette smoker consuming over 100 cigarettes.[13] Shisha is addictive as it usually includes nicotine. The second-hand smoke from shisha pipes is dangerous because it contains harmful substances like carbon monoxide, toxic chemicals and toxic particles.[14]
Smokeless Tobacco
Smokeless tobacco is not safer than smoking cigarettes. It’s a type of tobacco that can either be chewed, sucked, or inhaled without producing smoke
Most smokeless tobaccos have the same amount of nicotine as cigarettes. They can also have more than 25 chemicals that are known to cause cancer. Using smokeless tobacco can also increase your risk of having:
- complicated pregnancies
- mouth and tooth problems
- heart and circulatory diseases.
Smokeless tobacco may also be called snuff, snus or spit tobacco. Some smokeless tobacco products like snus is illegal to sell and buy in the UK.
Current use of smokeless tobacco is also much more common among smokers than non-smokers. Among the South Asian population smokers were nearly four times as likely to be current users of smokeless tobacco than non-smokers.[15] There is no available data for prevalence and understanding behaviours behind smokeless tobacco use in Surrey.
Vaping
What are vapes?
A vape is a battery powered device that heats a solution to produce a vapour. Most vapes contain nicotine and the vapour is inhaled. Along with nicotine the solution usually includes vegetable glycerine, propylene glycol and flavourings. Vapes do not burn tobacco. Vapes do not produce tar or carbon monoxide, two of the most harmful products of smoking tobacco.[16] Manufacturers have developed vapes and the solution they heat to get better at delivering nicotine to the user. Vapes that use nicotine salts enable nicotine to be absorbed faster. Vapers can quickly absorb more nicotine without the harsh effects on the throat that less effective vapes might produce.
Most of the poisonous chemicals contained in tobacco smoke, including tar and carbon monoxide, are not produced by vapes. The chemicals that are in vapour are at much lower levels than in tobacco smoke.
Leading health and public health organisations including the Royal College of Physicians[17], British Medical Association (BMA), Cancer Research UK and the US National Academies of Sciences, Engineering and Medicine; agree that although vapes are not risk-free in the short and medium term, vaping poses a small fraction of the risks of smoking.[18]
For people who smoke, vaping is much safe. People who do not smoke should not vape.[19]
The US National Academies of Sciences Engineering and Medicine reported “Lab tests of vape ingredients, in vitro and short-term human studies suggest that e-cigarettes are likely to be far less harmful than combustible tobacco cigarettes.” People who switch from smoking to vaping are exposed to much lower levels of potentially harmful substances associated with cancer. Currently, there have been no identified risks to bystanders from passive vaping.[16]
National Institute for Health and Care Excellence (NICE) guideline Tobacco: Preventing uptake, promoting quitting and treating dependence (NG209) includes recommendations on the advice that health and care professionals should provide to smokers on using vapes to quit. This is also supported by The Royal College of Physicians who have recognised vapes an effective treatment for tobacco dependency and the need to improve awareness about the safety of vapes compared to cigarettes.[17]
The use of vapes has increased since they became available in the United Kingdom, and they have now become the most popular aid to stop smoking used by people trying to quit.[20]
Evidence to support the use of vapes as an aid to quit smoking is building. The latest Cochrane Review, first published in 2021, has found high certainty evidence that nicotine-containing vapes are more effective than traditional nicotine replacement therapy (NRT) such as patches and gum in helping people quit smoking.[21]
However, there has been some controversy associated with vapes as they have attracted support and criticism from health organisations, health professionals and wider society. This has led to public and professional misunderstanding, where 43% of smokers who have not tried vaping, think that vaping is as harmful or more harmful than smoking tobacco, up from 27% in 2019.[22]
South East Position Statement on Vaping 2024
The South East Tobacco Control Network on behalf of the Association of Directors of Public Health, published the Position Statement on Vaping 2024 to provide consistency and clarity across the South East, assisting with the development of policies and to inform individual practice.
The document outlines the evidence about the relative risk of vaping compared to smoking, recommending trusted sources for more information. The document aims to encourage conversations about vapes and vaping that accurately share the evidence to help people quit smoking.
How are vapes regulated in the UK?
Vapes are not licensed as medicines in the UK, but they are tightly regulated for safety and quality. The Medicines and Healthcare products Regulatory Agency (MHRA) is the competent authority for a notification scheme for vapes and refill containers in Great Britain and Northern Ireland. MHRA provides advice for consumers who want to check whether a vape is legally compliant.[23]
Vaping in Adults
The proportion of the adult population using vapes increased in 2023 to 9.1% from 8.3% in 2022, which equates to 4.7 million people in Great Britain. Fifty-six percent of current vapers are ex-smokers, 37% are current smokers, only 1.1% of individuals who have never smoked are current vapers, and 6.7% of current vapers are never smokers. The proportion of adult smokers who have never tried e-cigarettes is continuing to decline slowly, down to 27% in 2023 compared to 28% in 2022 and 30% in 2021.[24]
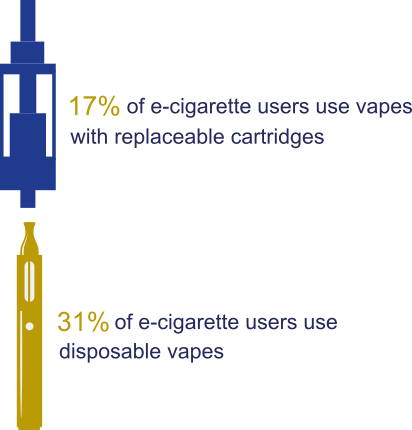
Figure 15: E-cigarette usage among adults
In 2022, the main reason given by ex-smokers for vaping is to help them quit or prevent relapse. Fourteen percent say their main reason for vaping is because they enjoy the experience and 11% to save money. The main reason current smokers vape is to cut down smoking or save money. A third of smokers incorrectly believe vaping is more or equally as harmful as smoking.
The most frequent type of e-cigarette device used remains a refillable tank system, with 50% of current vapers reporting this type as their main device. However, disposable vapes have become more popular in 2023 (31%), compared with 2022 (15%) and 2021 (2.3%). E-cigarettes with replaceable cartridges were used by 17% of vapers (figure 15).
Younger adults are more likely to use disposable e-cigarettes as their main type, with over half (57%) of 18-24 years olds using disposable e-cigarettes as their main type of device in 2023.[24]
Local data on adult vaping behaviours in Surrey is not currently captured.
Vaping in Children and Young People
National data
Vaping in young people is an emerging issue to be aware of. It is an offence to sell vapes to children under 18 in the United Kingdom.
The 2023 ASH Annual YouGov survey of smoking and vaping attitudes and behaviour among 11 to 18 year olds[25] found the following:
- In 2023 20.5% of children had tried vaping, up from 15.8% in 2022 and 13.9% in 2020 before the first COVID lockdown. The majority had only vaped once or twice (11.6%), while 7.6% were currently vaping (3.9% less than once a week, 3.6% more than once a week) and the remainder (1.3% in 2023) saying they no longer vape.
- The 50% growth in experimentation (trying once or twice) from 7.7% in 2022 to 11.6% in 2023 was significant, while the change in current vaping (from 6.9% to 7.6%) was not.
- Since 2021 the proportion of current vaping has been greater than that of current smoking (7.6% compared to 3.6% in 2023).
- The proportion of never smokers who have tried vaping is 11.5%. However, eight out of ten children have never smoked, so this amounts to nearly half (48%) of children who have ever tried vaping. Most (62%) of those who have never smoked but have vaped have only tried once or twice, while most (70%) current vapers have also tried smoking.
- There is an age gradient both for ‘ever’ and ‘current’ vaping. Among 11-15 year olds 15% have ever tried vaping, compared to 34% of 16-17 year olds and 38% of 18 year olds. The figures for current use are 4.6% among those aged 11-15, 15% for 16-17 and 18% for 18-year-olds.
Although some children vaped before they smoked tobacco there is no strong evidence of a causal effect that vaping leads to smoking. In the national data reported from surveys up to 2021, the proportion of 14- year-olds who smoked regularly fell from 7% in 2011 to 1% in 2021; among 15-year-olds, fell from 11% in 2011 to 3% in 2021.[4]
Local data
Data from the 2022 HRBQ survey conducted in Surrey schools[12] found that in secondary schools:
- Six percent of pupils responded that they have “never heard of” electronic cigarettes, while 75% said they have never used them.
- Eighteen percent of pupils had at least tried an e-cigarette which is a drop from 25% in 2019.
- Six percent of pupils responded that they use an electronic cigarette “occasionally” or “regularly”.
Inequalities are apparent in those who have tried vaping. Figure 16 below shows groups of year 10 students who have tried vaping or e-cigarettes. There are noticeably higher scores in those who are disabled, on free school meals, who have long term illnesses or identify as a young carer.
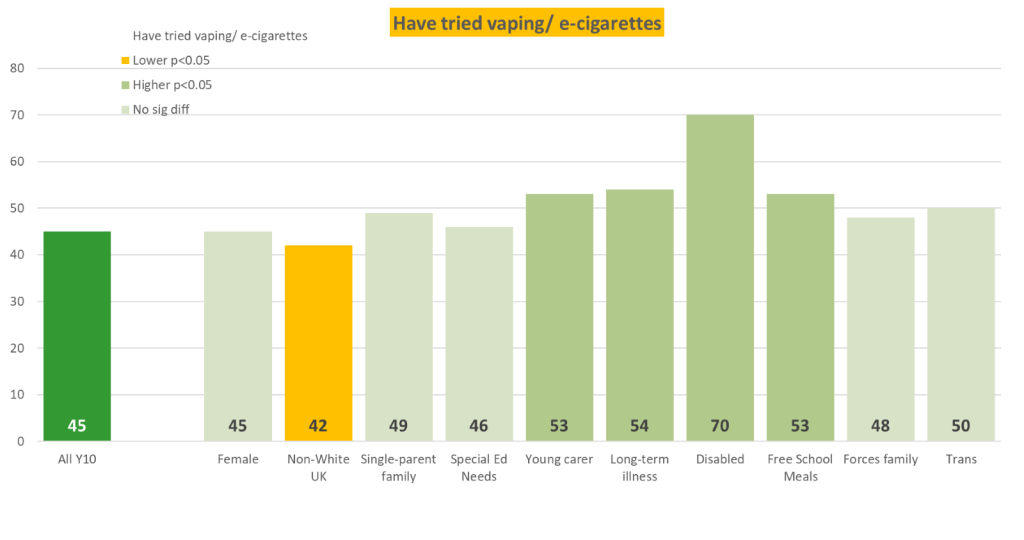
Figure 16: Year 10 students who have ever tried vaping or e-cigarettes broken down by group, HRBQ survey 2022.
It is illegal to sell vapes to children and young people under the age of 18. There are several reasons that may contribute to the rise in demand for vapes from under 18’s including:
- Appealing flavours of vapes such as popcorn, blueberry, mango ice, watermelon-cherry, and bubble-gum.
- Appealing packaging of vapes, with bright colours and interesting imagery.
- The low cost, particularly of disposable e-cigarettes, making them accessible on pocket money. Disposable e-cigarettes can be bought for a little as £2 and are often under £5 (compared to around £15 for a typical packet of cigarettes).
- The addictive nature of nicotine causing children and young people to quickly become addicted.
Economic Impact of Smoking
Action on Smoking and Health (ASH) now estimates that the total costs of smoking in England are £43.7 billion per year. This includes a £27.6 billion loss to productivity per year through smoking related lost earnings, unemployment, and early death, as well as costs to the NHS and social care sector of £1.82 billion and £13.9 billion respectively.
In Surrey, smoking costs £602 million per year [26], with £26.1 million attributed to healthcare costs. These costs are a result of smoking related hospital admissions and the cost of treating smoking related illness via primary care services.
Spending on social care is also huge in Surrey, with approximately £205 million spent on adults aged over 50 because of smoking. It is no surprise that smoking also has a negative costly impact on productivity, affecting earnings and employment prospects. The cumulative impact of smoking related lost earnings, unemployment and early deaths is estimated to be £367 million per year.
It is approximately £403 per quit in Surrey. This is an insignificant sum considering the costs smoking has on the Surrey population.
Source: ASH Ready Reckoner[26] ashresources.shinyapps.io/ready_reckoner/
The role of Trading Standards and Tobacco Control
Buckinghamshire and Surrey Trading Standards is a jointly funded Trading Standards service, hosted by Surrey County Council, to deliver consumer protection services within both authorities. The service uses local intelligence to tackle underage sales, sales of illicit products such as tobacco and non-compliant e-cigarettes as well as ensuring the safety of products such as e-cigarettes.
Summary of the main tobacco related legislation
- Children and Young Persons Act 1933 prohibits the sale of tobacco products to persons under the age of 18
- Tobacco and Related Products Regulations 2016 deal with the manufacture, presentation and sale of tobacco and related products, including herbal products for smoking, vapes and refill containers, as well as smokeless and novel tobacco products.
- The Standardised Packaging of Tobacco Products Regulations 2015 standardise the packaging of certain tobacco products by requiring the removal of all promotional features.
- The Tobacco Advertising and Promotion Act 2002 bans advertising and promotion (including sponsorship) of tobacco products.
- The Tobacco Products (Traceability and Security Features) Regulations 2019 introduced a track and trace system for the supply chain of tobacco products and a system of security features to authenticate tobacco products. This means that each pack of tobacco will carry a unique code to track it from the producer to the retailer, and a label incorporating security features that can be used to check the product is genuine.
Illicit tobacco
Illicit tobacco is a cheap source of tobacco, often with no health warnings in English and not in plain packaging. Illegal tobacco is linked to smoking in young people and those from more deprived groups for whom price affects how much they can smoke, which reflects the national picture.
Illegal tobacco across the country is becoming a significant problem with organised criminal gangs targeting vulnerable people by selling cigarettes and hand rolled tobacco at reduced prices. Surrey is no exception with illicit tobacco being found by Buckinghamshire and Surrey Trading Standards across the county. The availability of cheaper illegal tobacco undermines the efforts of smokers from quitting and instead encourages more smoking among both adults and young people.
There is strong evidence to show that illicit tobacco causes house fires. Illegal cigarettes do not meet the ‘Reduced Ignition Propensity’ safety standard. Since 2011, all cigarettes sold in the UK have to be manufactured to meet this standard which makes sure that cigarettes left unattended go out quickly using fire retardant paper.
Since illegal cigarettes are not manufactured legitimately, safety cannot be assured, leading to cigarettes staying lit and fires occurring.
Common brands of illegal tobacco to look out for include Jin Ling, Raquel, Richman, Platinum, Newman (NZ) and Camelford which cannot legitimately be bought in the UK. However, if tobacco products do not contain health warnings written in English or display the ‘United Kingston (UK) DUTY PAID’ fiscal mark, they are also illegal.
Non-compliant vapes
The introduction of disposable vapes in the last couple of years has seen a rise in problems in the market. These include:
- The safety of the vapes themselves alongside growing evidence there has been a rise in under 18s vaping.
- Compliance issues with vapes include: not being registered with the Medicines and Healthcare products Regulatory Agency (MHRA) for sale in the UK (and therefore there is no assurance about the chemicals they contain and their safety).
- Having a liquid tank size that is larger than the maximum permitted (2ml).
- Nicotine-containing e-liquid for sale in one refill container should not exceed 10ml.
- The nicotine strength of e-liquids should be no more than 20mg/ml
- Having incorrect labelling (often the labelling was designed for a different market than the UK) and counterfeit vapes, again with no knowledge of the chemicals they contain and no assurance that they are safe.
Enforcement in Surrey
In the 2022/23 FY following the gathering of local intelligence, across both Buckinghamshire and Surrey, Trading Standards undertook 17 visits resulting in 4,284 packets of 20 cigarettes, 11,340g of hand rolling tobacco, and 13kg of illicit shisha being seized along with nearly 8000 non-compliant e-cigarettes; which creates issues of where to store these products.
In Surrey, during a 12-month period from January 2023 to January 2024, Trading Standards received 236 reports of underage sales or on illicit tobacco and vape products. Of these 236 cases, 200 were in relation to vape products. This trend was similar by district and borough council areas, shown in figure 17. Guildford, Epsom and Ewell and Spelthorne reported the greatest number of cases with 38, 34 and 32 respectively, compared to Tandridge and Surrey Heath which recorded five and seven reported cases respectively. Most reported cases came from the Police, Citizen’s Advice and the general public.
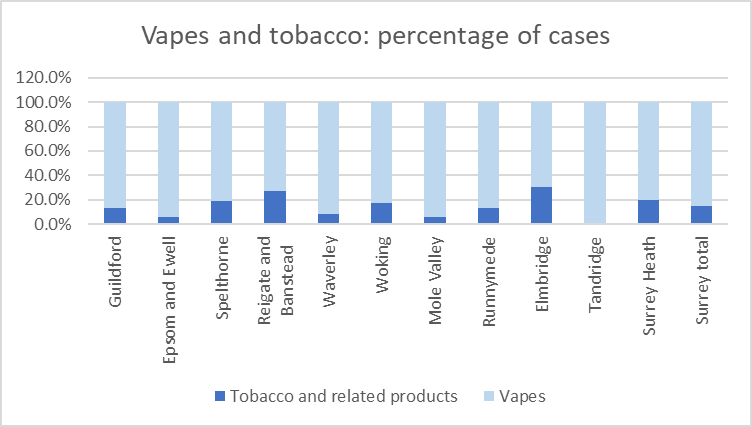
Figure 17: Tobacco and Vape reports to Trading Standards by district and borough.
Regarding underage sales, 73% of all referrals in Surrey related to vaping products, 7% tobacco and 21% for other (i.e. alcohol). Figure 18 shows that underage sales relating to vaping products was greatest across all districts and borough council areas except for Surrey Heath.
It is anticipated that there are more incidences of underage sales and sales of illicit products taking place in Surrey, but the reporting mechanisms are not well known amongst the general public.
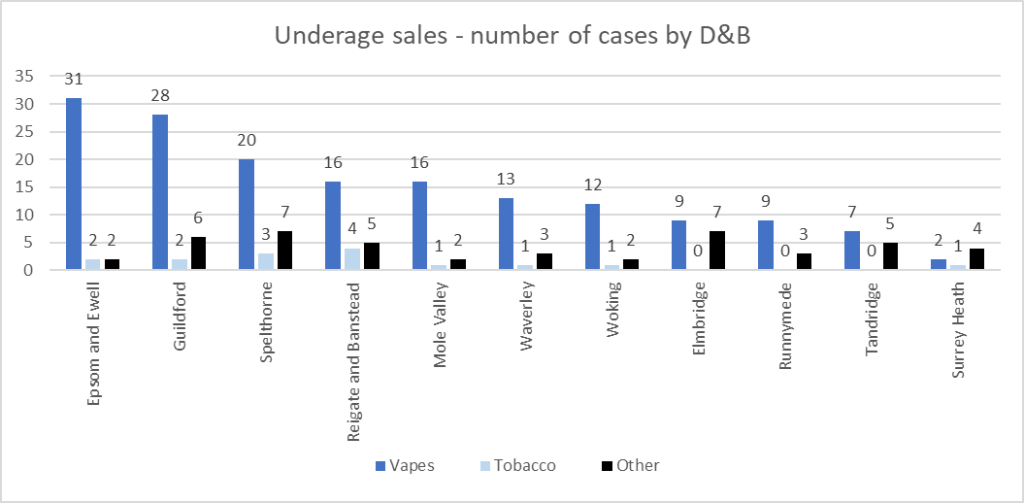
Figure 18: Tobacco, vapes and other underage sales by district and borough
The Police and Trading Standards can investigate and take action against those who import or sell illegal tobacco and vape products and members of the pubic can report any intelligence directly to them via this website.
Environmental Impact
Tobacco and smoking-related products are the most littered items in the UK, with cigarette butts comprising the vast majority of this (66%).[27] Almost all cigarette butts are plastic, and these subsequently degrade into microplastics which leach toxic chemicals into watercourses and soil. Over the last decade, tobacco smoking has decreased throughout the UK, driven in part by the rise of e-cigarettes.
Disposable e-cigarettes are the subject of considerable concern, with 5 million[28] thrown away each week and the significant and sharp increase in the use of disposable e-cigarettes, particularly by children, has driven a debate around the sale and use of these products, culminating in a ban on disposable e-cigarettes from 1 April 2025. The UK government intends to pass this ban into law towards the end of 2024, with a six-month grace period meaning disposable e-cigarettes will not be legally sold from October 2025.
It is unclear what effect this will have on the black market for disposable vapes, however it is likely that some disposable e-cigarettes will still be in circulation after October 2025 and reusable e-cigarettes will not be affected. Both disposable and reusable e-cigarettes are currently classed as Waste Electrical and Electronic Equipment (WEEE), falling under Category 7 of the WEEE Regulations and although legally any establishment selling disposable e-cigarettes must make provision for customers to dispose of them safely, it is unclear the extent to which this happens.
The relatively new product means that consumers are largely unaware of how to dispose of e-cigarettes, resulting in them being placed within normal household or litter bin waste. This waste entering the normal domestic waste is contributing to a significant increase in the number of fires at waste facilities due to their lithium-ion batteries, with instances up 71% since 2022.[29]
The pace at which e-cigarettes have increased in popularity over the previous few years means that although the upcoming ban on disposable e-cigarettes should significantly reduce the amount entering the waste stream, assessments on how to educate the public and mitigate the impact of these items entering the domestic waste stream should continue to be made.
Surrey County Council is working with its waste contractors and partners to develop policy and communications to address the issue posed by e-cigarette waste, and some industries have launched e-cigarette recycling schemes to improve diversion of these from other waste streams. These schemes aim to reduce the risks posed by fire at facilities and recover valuable material within the e-cigarettes. They involve the provision of containers in various retail destinations in which e-cigarettes are deposited then collected for treatment.
The Local Government Declaration on Tobacco Control
The Local Government Declaration on Tobacco Control was developed by Newcastle City Council. It is a statement of a council’s commitment to ensure tobacco control is part of mainstream public health work and commits councils to taking comprehensive action to address the harm from smoking. Surrey County Council signed the declaration in February 2014.
NHS Smokefree Pledge
In January 2018, the Smokefree Action Coalition launched the NHS Smokefree Pledge, updating the NHS Statement of Support for Tobacco Control launched in 2014.
The Pledge is designed to be a clear and visible way for NHS organisations to show their commitment to helping smokers to quit and to providing smokefree environments which support them. Currently no NHS trusts in Surrey have signed the pledge.
Stop Smoking Support (SSS) in Surrey
Relevant NICE guidance
NG209 Tobacco: preventing uptake, promoting quitting and treating dependence
This guidance provides advice, quality standards and information services for health, public health and social care to support the following:
- Support to stop smoking for everyone aged 12 years and older.
- Help to reduce peoples harm from smoking if they are not ready to stop in one go.
- Prevent children, young people and young adults aged 24 years and under from taking up smoking.
The guideline also brings together and updates all NICE’s previous guidelines on using tobacco, including smokeless tobacco. It covers nicotine replacement therapy and e-cigarettes to help people stop smoking or reduce their harm from smoking.
This guidance covers several recommendations such as:
- organising and planning national, regional or local mass-media campaigns
- coordinated approach to school-based interventions
- whole-school or organisation-wide smokefree policies
- support to stop smoking in primary care and community settings
- promoting stop-smoking support
- using medicinally licensed nicotine-containing products
- helping retailers avoid illegal tobacco sales
- supporting people who do not want, or are not ready, to stop smoking in one go to reduce their harm from smoking
- Provide training to health care staff such as train all frontline healthcare staff to offer very brief advice on how to stop smoking and make appropriate referrals to a local stop smoking service.
Smokers are three times more likely to quit smoking for good by using an evidence based local stop smoking service to support them. The Surrey stop smoking service (SSS) follows the NICE guidance on delivery.
Local stop smoking services
The SSS provide a highly cost-effective approach to help people quit smoking. Stop smoking services form a key part in improving people’s health outcomes and reducing health inequalities, as well as significantly increasing people’s chances of quitting smoking for good.
One You Surrey is the Council’s commissioned Adults Healthy Lifestyle service which offers free, evidence-based stop smoking support. The service offers 12 weeks of behavioural support, as well as free access to quitting aids such as NRT and vape starter kits.
During 2022/23 the Surrey SSS supported 2,534 smokers to set a quit date and 1,541 people successfully quit smoking. This is a 60.8% quit rate. The trend is shown below in figures 19 and 20.
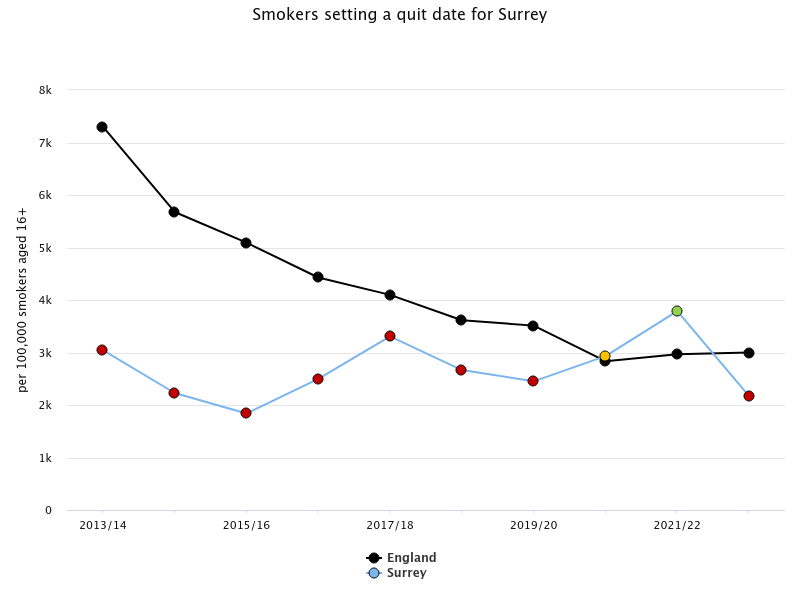
Figure 19: Smokers setting a quit date for Surrey
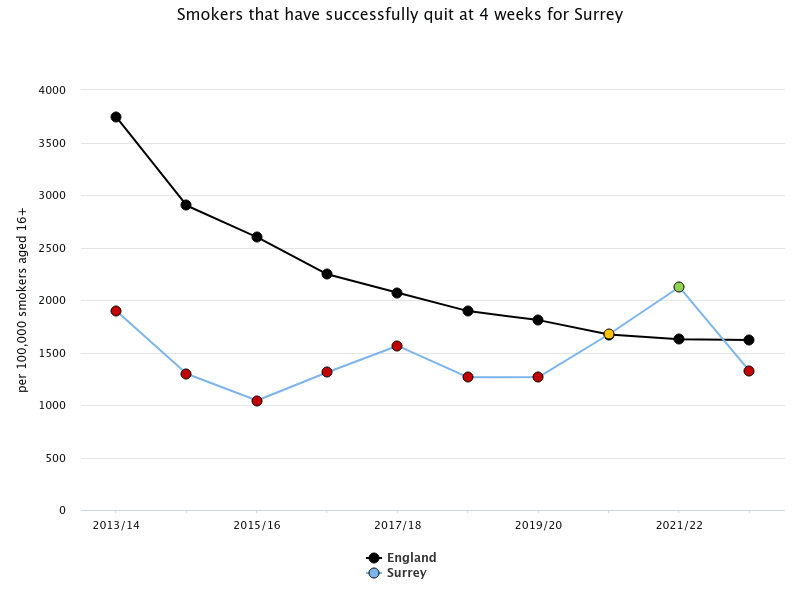
Figure 20: Smokers that have successfully quit at 4 weeks for Surrey
More women successfully quit smoking in 2022/23 than men (833 versus 708 respectively), however fewer men did not quit or were lost to follow up (LTFU) compared to women, 295 (not quit) and 112 (LTFU) versus 441 (not quit) and 145 (LTFU).
There was a 60.8% quit rate overall, 63.5% for men and 58.7% for women. Although more women set a quit date than men, men are more likely to successfully quit in Surrey.[30]
NHS Tobacco Dependency Service
The NHS long term plan ambition aims to support the NHS to ensure that all individuals who are admitted to hospital through acute inpatient or mental health settings, are offered NHS-funded tobacco dependency treatment. This follows the Ottawa model implemented in Canada which has successful outcomes. There is also a maternity pathway to support all expectant mothers through their antenatal care, to ensure newborns go back to a smokefree environment.
Within Surrey Heartlands ICB, there are seven pathways across four trusts which are split between acute inpatient, maternity, and mental health. These are split as follows:
| Trust | Acute Inpatient Pathway | Maternity Pathway |
|---|---|---|
| Royal Surrey NHS Foundation Trust | Yes | Yes |
| Ashford and St. Peter’s Hospitals NHS Foundation Trust | Yes | Yes |
| Surrey and Sussex Hospitals Trust | Yes | Yes |
| Surrey and Borders Partnership NHS Foundation Trust | Yes (mental health inpatients) |
n/a |
| Epsom and St Helier University Hospitals NHS Trust | Yes | Yes |
| Frimley Health NHS Foundation Trust | Yes | Yes |
NICE recommend that all health and social care professionals be trained in very brief advice (VBA) and deliver VBA opportunistically to patients. This is essential for referral generation into the local SSS. VBA on smoking is designed to promote quitting and can be delivered in almost any situation with a person who smokes in less than 30 seconds.
Evidence of effectiveness of the Surrey SSS
In May 2022, the Surrey SSS was evaluated to look at overall performance and how service provision had evolved over the pandemic, to provide insight on the current delivery model and the impact of any changes. Overall, the evidence from the evaluation suggests the service is high quality and performing well, however there are areas for improvement or where the service could develop further, particularly in supporting certain priority groups. Data included in this evaluation was from April 2019 to February 2022, however additional data up until February 2023 has been included in this needs assessment.
Service user experience
The service is rated very highly by service users in the quarterly client satisfaction survey, scoring above 4 out of 5 across all areas (service quality, service accessibility, team knowledge and skills, support received, team friendliness). This survey was completed by approximately 10% of service users during the period analysed. When the additional data was added, the satisfaction survey was completed by 40% of all service users and the service remained at a very high rating (98% of responses for all areas scored above 4 out of 5).
Effectiveness of service delivery model
- It is evidenced based offering interventions that increase the likelihood of individuals successfully quitting smoking.
- National evidence currently suggests telephone and virtual support is less effective than face to face support. This may be due to a lack of evidence however this cannot be assumed. Quit rates have remained in line with bench marking.
- An element recommended in national guidance due to strong evidence of efficacy is group face to face support. Currently the Surrey SSS only offers peer support through a Facebook group because of changes to the service during the pandemic.
- As a result of the pandemic the delivery model changed to be remote and telephone based. Insight from the provider is very positive, the service is more flexible for clients and the provider can see more people.
- However, carbon monoxide (CO) monitoring was significantly reduced and therefore validated quits remain a challenge with the current model. CO monitoring has been seen as a motivating tool for service users and provides evidence base for commissioning purposes.
- Dedicated stop smoking advisors for pregnant women and service users with mental health conditions was positive.
The service has seen 10,031 patients :
- 75% are from a priority group
- 20% are from a target ward
- 5% are pregnant women
- 43% are male
- 22% are routine or manual workers
- 11% are of Black and Asian minority ethnicity
Overall, the service performs well against national benchmarks of abstinence at 4 weeks (55%) and similarly at 52 weeks (11%).
This equates to 1,132 people in Surrey who have quit for at least 1 year between April 2019 and February 2023, this includes both self-reported and CO verified quits. The proportion of quits at 52 weeks has been on a slight decline, however with the service supporting more people, the number of people who have quit at 52 weeks has increased. Only 4% of quits in 2022/23 have been CO verified, therefore additional work needs to take place to restore this.
Vapes were introduced in April 2022 as an additional quit aid to support clients. This was because of the supply issues with Champix. During 2022/23, approximately 66% of clients used a vape to aid their quit attempt, with the vast majority combining their vape with a nicotine patch. Amongst those service users who do use a combined model there has been an observed 4-week quit rate of 65%. This is higher than the overall service quit rate of 60.8%.
Resident engagement
A research brief is currently being scoped to investigate the barriers amongst smokers in Surrey preventing them from accessing the local SSS and what interventions are likely to be most effective in helping smokers overcome capability, opportunity and motivation barriers.
The research and findings will be added to this JSNA chapter when they are available later in the year.
System engagement
As part of the development of the Tobacco Control Strategy which has informed this chapter, there was engagement with a range of stakeholders from across Surrey. These included:
- Public Health, Surrey County Council
- Trading Standards, Surrey County Council
- Surrey Healthy Schools Lead, Surrey County Council
- Environment and Waste Management, Surrey County Council
- NHS Surrey Heartlands ICB
- NHS Frimley ICB
- Primary Care
- Community Pharmacy
- Macmillan
Recommendations
Area 1: Insight and Inequalities
| Recommendation | Rationale |
|---|---|
| 1.1 Further understand the needs of smokers in Surrey and the best way to engage with and promote the benefits of quitting. There should be a particular focus on routine and manual workers and people in treatment for substance misuse. | Limited evidence on the key behaviours which motivate smokers to quit in Surrey as well as what the barriers are smokers face preventing them to access stop smoking services. |
| 1.2 Gather local intelligence about the cultural behaviours in Surrey related to shisha smoking and other tobacco products. | There is currently no local data or insight on these behaviours. |
| 1.3 Gather more intelligence on the smoking and vaping prevalence among children and young people in Surrey | Limited data from the Health-Related Behaviour Questionnaire in Surrey |
Area 2: Stop Smoking Services
| Recommendation | Rationale |
|---|---|
| 2.1 Further understand how SSS can support substance misuse service users, routine and manual workers and people from inclusion health groups. | High smoking prevalence in these populations compared to the general population. |
| 2.2 Adapt current delivery model to include a face-to-face component to include CO validated quits. | CO monitoring was significantly reduced in the pandemic due to remote delivery, and whilst there are benefits to support quit attempts with remote delivery, CO validated quits have not restored to pre-pandemic levels. |
| 2.3 Improve responses to 52-week abstinence data, particularly for mental health and pregnancy service users. Maybe include an incentive for responding. | There has been a decline in the number of 52 week quits, although an overall increase in the number of 4 week quits. |
| 2.4 Improve demographic data completeness particularly for ethnicity. | Limited data on smoking prevalence by ethnicity in primary care so it would be useful to understand quit attempts by ethnicity in the local stop smoking service. |
| 2.5 Enhance partnership working with Surrey Heartlands and Frimley ICBs as the smoking cessation pathways are developed in acute and mental health trusts and maternity units.
Strengthen referral pathways in Outpatient Clinics where smokers are not picked up via the LTP Tobacco pathways. |
As the services reach full establishment, maximising the potential for onward referral at the point of discharge for patients. |
| 2.6 Continue to promote the benefits of swapping to a vape to stop smoking. | High quit rate of 65% from the local stop smoking service using vapes as a quit aid. |
| 2.7 Improve referral pathways to SSS within long term condition specific pathways across Surrey by training frontline staff in Very Brief Advice. | Data demonstrates smoking related ill health such as COPD is greater than England in some district and borough council areas such as Runnymede. |
Area 3: Enforcement
| Recommendation | Rationale |
|---|---|
| 3.1 Increase the awareness of how residents can report concerns of underage sales or sales of illicit tobacco and vape products in Surrey. | Underage tobacco and vape sales are evident in Surrey but are not reflective of the number of young people vaping in Surrey. |
| 3.2 Use intelligence from Trading Standards to target promotion and marketing of the SSS. | Data identifies areas of underage sales and illicit tobacco sales, mapping this with smoking prevalence and stop smoking support could maximise impact. |
| 3.3 Increase the capacity in officers to further investigate cases of underage sales or sales of illicit tobacco and vape products in Surrey. | Staff resources are limited to meet the demands of increased reports. |
Area 4: Environment
| Recommendation | Rationale |
|---|---|
| 4.1 Increase the awareness of e-cigarette recycling schemes to Surrey residents. | Many users of disposable vapes are not aware of the recycling mechanisms in place. |
| 4.2 Work with districts and borough councils and NHS Trusts to develop smokefree policies to demonstrate their commitment to supporting people to quit smoking. | NHS trusts have not signed up to the NHS Smokefree pledge. |
References
[1] Stopping the start: our new plan to create a smokefree generation – GOV.UK (www.gov.uk)
[2] OHID Fingertips: Smoking Profile . Smoking Profile – Data – OHID (phe.org.uk)
[3] Action on Smoking and Health (2019) Health Inequalities and Smoking ASH-Briefing_Health-Inequalities.pdf
[4] Action on Smoking and Health (2024) Young People and Smoking Youth-Smoking-Fact-Sheet-2024.pdf (ash.org.uk)
[5] Action on Smoking and Health: Ready Reckoner Spring 2024 ashresources.shinyapps.io/ready_reckoner/
[6] Royal College of Physicians Tobacco Advisory Group. Passive smoking and children. Royal College of Physicians, London 2010
[7] Office for national Statistics: Adult Smoking Habits in the UK 2021: Adult smoking habits in the UK – Office for National Statistics (ons.gov.uk)
[8] Action on Smoking and Health: Smoking, the heart and circulation 2021: Smoking-Heart.pdf (ash.org.uk)
[9] British Heart Foundation: England CVD Factsheet 2024 BHF England CVD Factsheet
[10] Cancer Research UK: How does smoking cause cancer? | Cancer Research UK
[11] NHS England: Smoking, Drinking and Drug Use among Young People in England, 2021
[12] Health Related Behaviour Questionnaire | Surrey-i (surreyi.gov.uk)
[13] British Heart Foundation: Shisha Shisha – BHF
[14] Local Government Association: Reducing the harm of shisha and the need for better regulation. Reducing the harm of shisha and the need for better regulation | Local Government Association
[15] Action on Smoking and Health: Evidence into practice: Smokeless tobacco products 2020 smokelesstobaccoeip.pdf (ash.org.uk)
[16] South East Tobacco Control Network: Position Statement on Vaping 2024
[17] Royal College of Physicians: e-cigarettes and harm reduction. e-cigarettes-and-harm-reduction_full-report_updated_0.pdf (rcp.ac.uk)
[18] Nicotine vaping in England: 2022 evidence update main findings – GOV.UK (www.gov.uk)
[19] Chief Medical Officer for England on vaping – GOV.UK (www.gov.uk)
[20] NHS (2022) Using e-cigarettes to stop smoking – NHS (www.nhs.uk)
[21] Hartmann-Boyce J, Lindson N, Butler AR, McRobbie H, Bullen C, Begh R, Theodoulou A, Notley C, Rigotti NA, Turner T, Fanshawe TR. Electronic cigarettes for smoking cessation. Cochrane Database of Systematic Reviews. 2022(11). DOI: 10.1002/14651858.CD010216.pub7
[22] Action on Health and Smoking 2023 Addressing common myths about vaping: Putting the evidence in context – ASH
[23] MHRA (2022) E-cigarettes: regulations for consumer products https://www.gov.uk/guidance/e-cigarettes-regulations-for-consumer-products
[24] Action on Smoking and Health Use-of-e-cigarettes-among-adults-in-Great-Britain-2023.pdf (ash.org.uk)
[25] Action on Smoking and Health Use of e-cigarettes among young people in Great Britain – ASH
[26] Action on Health and Smoking Ready Reckoner 2025
[27] Keep Britain Tidy: Litter Composition Analysis 2020
[28] Material Focus: Media release 2023 https://www.materialfocus.org.uk/press-releases/disposable-single-use-vapes-thrown-away-have-quadrupled-to-5-million-per-week/#:~:text=The%20latest%20research%20from%20Material,was%20first%20conducted%20last%20year.
[29] Lets Recycle: Media Release 2024 https://www.letsrecycle.com/news/material-focus-reports-71-increase-in-battery-fires-since-2022/?utm_campaign=letsrecycle.com%20newsletter&utm_medium=email&_hsenc=p2ANqtz-_6dR6AkgNZiMzBMNk6DUkt_14wzX17_G8tlu5n-8Oqm3Jg0SFEzvKFTR-VOvLwnk7Kkd_lQTh1iDxXT7_Sr8Bs7WsbnK21BnVjiKUlS359vghWuzo&_hsmi=307530461&utm_content=307530461&utm_source=hs_email
[30] NHS England Digital: Statistics on NHS Stop Smoking Services in England – April 2022 to March 2023 (Q4, Annual) – NHS England Digital
Acknowledgements
Lead Contributors
| Emma Jones [email protected] |
Public Health Programme Lead, Surrey County Council |
| Rebecca Matthews | JSNA Programme Manager, Surrey County Council |
| Will King | Public Health Programme Lead, Surrey County Council |
| David Pickering | Team Manager, Buckinghamshire & Surrey Trading Standards |
| Adam Watkins | Senior Programme Manager, NHS Surrey Heartlands |
| Nick Wallace Jones | Waste Strategy & Policy Officer Surrey County Council |
| Nicola Munday | Child Wellbeing Professional and Lead for Learning from Child Deaths NHS Surrey Heartlands |