JSNA Tuberculosis
Joint Strategic Needs Assessment: Tuberculosis in Surrey Heartlands
Publication date
This chapter was published in January 2025
Contents
- Introduction
- Summary of findings
- List of recommendations
- National context
- The Surrey context
- Epidemiology of TB in Surrey Heartlands
- TB diagnosis, screening and treatment
- Service provision
- Inclusion health
- Patient perspectives
- Appendix
- Glossary
- References
- Key contacts
Introduction
Tuberculosis (TB) is an infectious disease caused by the Mycobacterium tuberculosis complex. While TB can affect any part of the body, infection of the lungs (pulmonary TB) is most common. Only TB infections in the lungs or the throat (laryngeal TB) can be transmitted to others.
When someone is infected by TB, the bacteria may:
- Be destroyed by the immune system
- Develop into TB disease (‘active’ TB) over a period of weeks or months; or
- Remain in the body in a dormant state causing no symptoms or illness (latent TB infection or LTBI). Infection can remain latent for many years and may or may not ever progress (‘reactivate’) to cause disease.
The World Health Organisation (WHO) have estimated that there were 10.8 million new cases of TB disease and 1.25 million deaths globally in 2023, meaning it was likely to have been the leading cause of death from infectious diseases, after three years of being second to Covid-19 [1].
While TB is relatively rare in England, there was an 11% increase in notifications between 2022 and 2023, followed by a 13.7% increase in the first three quarters of 2024 [2].
TB remains an important public health problem because:
- The wide range of symptoms caused by infections outside the lungs (extra-pulmonary disease) can lead to late presentations to healthcare and delays in diagnosis, longer treatment times and worse patient outcomes.
- Treatment regimens are complex and lengthy (a minimum of six months and often longer), with side-effects that can be difficult to tolerate. Lack of adherence to a full course of TB treatment risks the development of drug-resistant TB.
- Poverty, poor nutrition and inadequate, crowded living conditions are risk factors for TB transmission and for latent TB infection to progress to active disease and can make treatment adherence more difficult.
- Transmission of pulmonary TB disease can lead to clusters or outbreaks, particularly there are delays to patients presenting to healthcare services and starting treatment.
- TB remains heavily stigmatised and can lead to loss of employment or other social costs.
Summary of findings
Surrey has relatively few active TB cases. While this is very welcome, it leads to difficulties in how TB is identified and treated. Most healthcare professionals will seldom see a case of TB, so they may not immediately suspect it as a cause of their patients’ illness and are less likely to know how to appropriately refer them to TB service providers. The national LTBI programme, which identifies people from high incidence countries for testing and treatment, does not operate in Surrey because the rate of active TB is low. Few 6–15-year-olds require tuberculin testing to determine whether they should receive TB vaccines. This means that in some parts of Surrey, the skill set required to carry out tuberculin testing cannot be maintained.
In general, TB services perform well. Almost all patients are treated successfully. However, inadequate staffing and the increasing complexity of cases means that services are coming under pressure and cannot always provide the care that they would like. Some core elements of TB service are not always readily available, such as Directly Observed Treatment. The limited capacity of the TB teams means that outreach services are not provided, and links with other services such as prisons and homeless shelters have not been developed.
In common with the rest of the country, Surrey faces challenges relating to diagnosing and treating TB in refugees and asylum seekers. While some of these are out of the control of the local health system, others, such as the provision of accommodation for TB patients with no recourse to public funds are not.
It is hard to get a clear picture of TB service users’ perspectives as this is not currently routinely recorded by service providers. It should be. However, the limited amount of patient feedback that could be gathered for this needs assessment was overwhelmingly positive about the care that had been provided by their TB team.
List of recommendations
Diagnosis, screening and treatment
To reduce diagnosis times, other service providers should consider adopting Ashford and St Peter’s approach of automatically notifying suspected TB cases to the TB team.
Ensure all services can access Polymerase Chain Reaction (PCR) testing without delay when required.
Royal Surrey to ensure appropriate referral, testing and treatment pathways are put in place from all their relevant departments, including for patients starting biologics and children with both active and latent TB.
Service provision
All TB services to have the national TB service specification included in their contracts.
Services should be sufficiently well-funded that staffing levels can meet Royal College of Nursing (RCN) guidelines and services such as Directly Observed Treatment (DOT) and Video Observed Treatment (VOT) can be provided consistently.
Longer-term solution for tuberculin testing to be developed to enable Bacillus Calmette-Guerin (BCG) vaccination of 6-15 year olds in East Surrey.
Inclusion health
Agree pathways for funding DOT or VOT treatments.
If service providers would like to offer DOT through pharmacies, processes should be agreed in advance with a selection of pharmacies so that patients can rapidly commence treatment.
Services using Video Observed Treatment (VOT) should be informed by their provider as soon as a patient misses a single dose.
Ensure appropriate pathways are in place in all Surrey’s prisons. Build relationships between the prison health teams and the relevant TB services.
Develop pathways for prison patients to get hospital appointments at short notice.
Continue to work with Home Office colleagues to prevent people living in asylum accommodation being moved without enough notice to transfer their medical care.
Extend inclusion health outreach across Surrey, including but not limited to active and latent TB screening and GP registration.
Establish and maintain a shared Surrey-wide list of contacts in support services to meet the wider needs of people in inclusion health groups.
Work across the health system to allow people who are not registered with a GP to access a greater range of services.
Agree a memorandum of understanding on the provision of support for people with active TB who have no recourse to public funds.
Patient perspectives
Service providers should routinely collect patient feedback.
National context
Epidemiology of TB in England
England is a country with low TB incidence. In 2023 there were 8.5 cases per 100,000 people, under the WHO low incidence threshold of 10 per 100,000 [3]. There was a sustained drop in cases between the most recent peak of 8,281 notifications in 2011 and 4,375 in 2022 [3]. However, this was followed by a jump to 4,855 cases in 2023, with a further increase of 498 cases in the first three quarters of 2024 [2].
TB in England is highly concentrated in large urban centres, with London’s incidence of 18.7 per 100,000 in 2023 being five times higher than that of the South West (3.7 per 100,000) [3]. This is a consequence of cases being considerably more common in people born outside the UK (40.1 per 100,000) than in UK-born people (2.1 per 100,000) [3].
TB is closely associated with deprivation and social risk factors than can lead to social exclusion, barriers to access to healthcare and overall poor health outcomes. This includes substance misuse, homelessness, imprisonment, being an asylum seeker and having poor mental health [4].
National strategies
The 2015-2020 Collaborative Tuberculosis Strategy for England, created by Public Health England and NHS England aimed to achieve a “year-on-year decrease in incidence, a reduction in health inequalities and, ultimately, the elimination of TB as a public health problem in England” [5]. Over this five-year period, incidence dropped from 10.5 to 7.3 per 100,000, although it should be noted that 2020 data may have been affected by the Covid-19 pandemic. Outputs of that period included:
- The creation of seven regional TB Control Boards
- The development of a national TB service specification
- The establishment of an NHS England and Improvement funded programme for testing and treatment of Latent TB Infection in migrants in high-incidence parts of England
- The introduction of Whole Genome Sequencing (WGS) for new mycobacterial isolates.
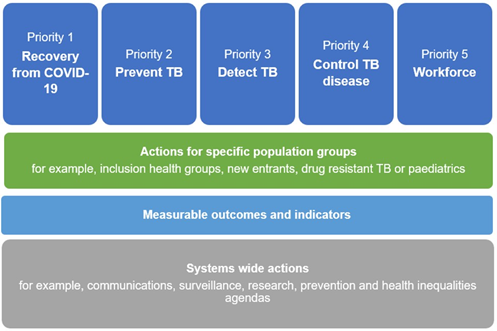
Following on from this strategy, Tuberculosis (TB): action plan for England, 2021 to 2026 is a joint UK Health Security Agency and NHS England publication, with the stated goal of improving the prevention, detection and control of TB in England [6]. As with the 2015-2020 strategy, the action plan aims for a year-on-year reduction in TB incidence and transmission, working towards the World Health Organisation target of reducing incidence by 90% between 2015 and 2035.
The action plan has five priorities (Figure 1) and 79 actions that fall on NHS England, UK Health Security Agency, commissioners, providers, primary care, Integrated Care Systems and Boards, local authorities and the third sector.
Figure 1: Priorities for the TB action plan for England, reproduced from that publication [6].
Selected actions and outcomes that are particularly relevant to this needs assessment include:
- Facilitating technology for appointments and directly observed therapy (DOT)
- Improving the detection and treatment of LTBI in new migrants
- Strengthening prevention, detection and treatment of active TB and/or LTBI in higher risk groups including:
- targeted screening in asylum seekers
- healthcare workers
- the immunocompromised
- the homeless
- those in contact with the criminal justice system
- people newly starting biological therapies
- Reducing delays in diagnosis and treatment
- Increasing culture confirmation rates
- Achieving 90% treatment completion rates by 2026
- Reviewing TB services against the national TB service specification
- Improve education, training and peer support for the TB workforce
- Ensuring the workforce reflects the requirements of local people with TB and the community
Clinical guidelines
The most recent National Institute for Health and Care Excellence (NICE) guidelines on TB were published in 2016 and reviewed in 2024 [7]. They include recommendations on prevention, diagnosis and management of both active disease and latent infection, drug resistant TB, infection prevention and control, case finding and service organisation.
In 2023, the Royal College of Nursing published a complementary case management tool providing guidance for people involved in the care and management of TB patients. It includes recommendations on staffing levels, treatment and contact investigations [8].
NHS England maintain a National TB Service Specification, which provides suggestions around which local specifications should be developed. It includes related services such as pharmacy, social care and psychology.
The Green Book provides guidelines on who should be offered Bacillus Calmette-Guerin (BCG) vaccination against TB [9].
These four documents and the TB Action Plan provide broadly similar recommendations, some of which will be referenced in relevant sections of this needs assessment.
Regional Governance
In line with the recommendation of the 2015-2020 strategy, the South East TB Control Board provides an overarching support structure for TB control in the region, identifying and escalating key issues to national organisations where necessary. It is co-chaired by the UKHSA South East regional director and the NHS England South East medical director, with representation from TB service providers, ICBs and local authorities.
Four local TB networks act as advisory committees, reporting to the South East TB Control Board, including Surrey and Sussex. They:
- Disseminate any changes made to national guidance
- Provide support to organisations to ensure these recommendations and changes
- Provide opportunities to identify issues around TB management and control
- Act as a forum for sharing best practice
In line with NICE and RCN guidelines and the national services specification, there are also quarterly cohort reviews where all cases of active TB in the area are discussed by a multidisciplinary group to review outcomes and identify any issues that have arisen locally.
Within the Surrey Heartlands area, a TB Task and Finish Group has been set up to bring together providers, commissioners, UKHSA and Surrey County Council to progress work towards the TB National Action Plan and resolve any issues that have been identified.
Purpose and methodology of this Health Needs Assessment
This needs assessment was requested by UKHSA and commissioned by the Surrey Heartlands TB Task and Finish Group. The Surrey TB Task and Finish Group has overseen the needs assessment process. The needs assessment was led and written by Dr Tom Irving, Specialty Registrar in Public Health and follows a previous TB Needs Assessment for Surrey and Sussex from 2017 [10].
Quantitative analysis is primarily based on data provided by UKHSA’s Field Epidemiology Service from the National TB Surveillance System (NTBS) and, prior to 2021, two legacy databases (the Enhanced TB Surveillance system and the London TB register). Data were provided for all notifications of active TB disease between 01/01/14 and 31/12/23 for patients whose residence was recorded as being in the Surrey Heartlands ICB area. This is a snapshot of the record as of 22/05/24, rather than the information recorded at the time of diagnosis. It includes patients being treated outside Surrey Heartlands, almost always in London. Data presented here will sometimes be slightly different to that elsewhere, due to small differences in scope, timings and variable definitions. This does not affect the conclusions of this needs assessment.
Other quantitative analysis is based on published data sources as referenced throughout this needs assessment.
Staff members from each TB service provider completed questionnaires, which is given in the appendix.
Qualitative insights also come from interviews carried out with:
- The same TB service staff members who completed questionnaires
- A member of the medical team at HMP Bronzefield
- A GP clinical lead
These took place in July and August 2024 via Microsoft Teams. Interviews were recorded and transcribed.
Service users’ perspectives were captured through telephone interviews with two people who had recently been treated for active TB at one of the local TB services. More details are given in that section.
The Surrey Context
As of 2021, there were 1.2 million people living in Surrey. It is one of the most prosperous parts of the UK, with only small pockets of deprivation.
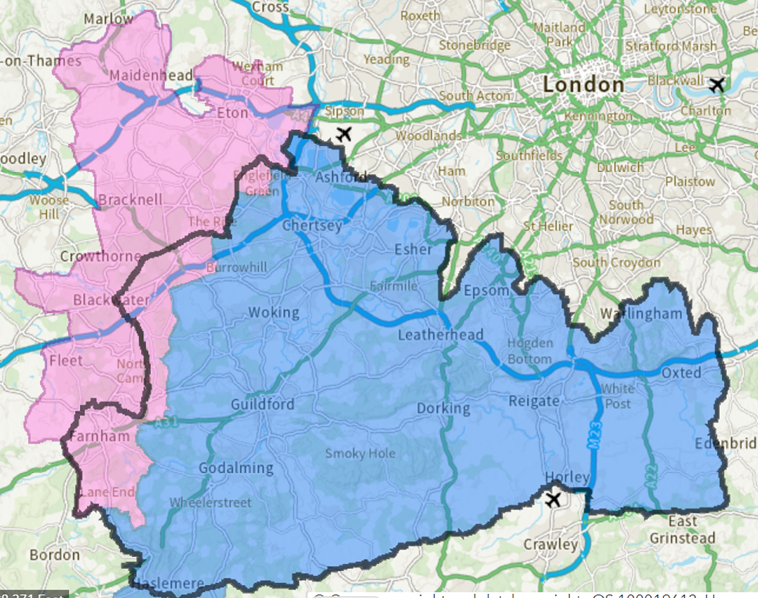
Surrey is served by two Integrated Care Systems (ICSs). Just over a million people (87% of the population) live in the NHS Surrey Heartlands ICS area. The remaining 150,000 people, in Farnham and Surrey Heath, are part of the NHS Frimley ICS area. Frimley also covers parts of Hampshire and Berkshire.
Figure 2: Surrey Heartlands (blue) and Frimley (pink) ICS areas within Surrey (black border). Map from Surrey County Council.
Three hospital trusts are commissioned by Surrey Heartlands to provide TB services:
- Royal Surrey NHS Foundation Trust, at Royal Surrey Hospital in Guildford
- Ashford and St Peter’s NHS Foundation Trust, with services provided at both Ashford Hospital and St Peter’s Hospital in Chertsey
- Surrey and Sussex Healthcare NHS Trust (SASH), with services provided at East Surrey Hospital. SASH also deliver TB care in parts of Sussex. This is separately commissioned by Sussex Health and Care ICB.
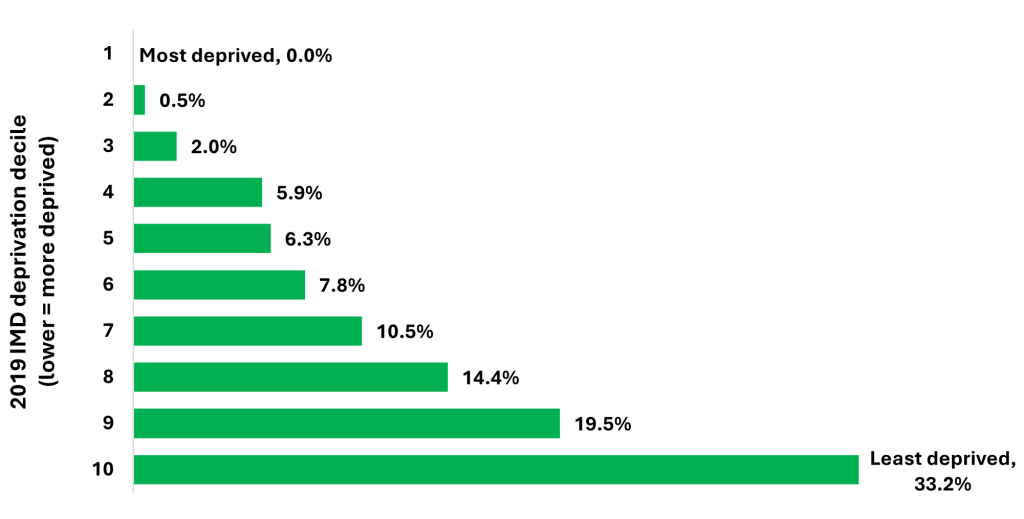
Of Surrey’s 1.2 million residents:
- None live in the most deprived 10% of England’s neighbourhoods
- 6,300 live in the second most deprived 10%
- 23,000 live in the third most deprived 10%
- 393,000 live in the least deprived 10% [11].
Figure 3: The proportion of Surrey’s population in each IMD deprivation decile (lower = more deprived). Data from Surrey’s Joint Strategic Needs Assessment [11].
While Surrey’s deprivation levels are lower than the England average, that is not the case for all risk factors for TB, as summarised in the table below which compares Surrey’s population to that of England overall. This shows that demographics are an important contributing factor to Surrey’s TB incidence being below average for the country.
Surrey’s rates compared to England’s average
| LOWER | SIMILAR | HIGHER |
|---|---|---|
| Deprivation | Birth outside UK | Currently being a prisoner |
| Current opiate usage | Birth in high incidence country | |
| Current homelessness | Refugee or asylum seeker |
17.9% of Surrey’s population were born outside the UK as at the time of the 2021 census [12], around half of whom come from countries that WHO defines as high incidence (>40 cases per 100,000 per year), very similar to the England average [13].
High incidence countries include India (the birthplace of 1.5% of Surrey residents), South Africa (1.4%), Romania (0.7%), Pakistan (0.6%) and the Philippines (0.4%) [12]. 37.9% of Surrey residents born overseas had arrived in the UK in the previous decade [12].
As of the 2021 census, 23.4% of Surrey residents described their ethnicity as something other than White British (similar to the England average of 26.5%), ranging from 12.6% in Waverley to 30.6% in Woking [14].
At that time 2,680 Surrey residents (0.22%) identified as Gypsy or Irish Travellers and 1,675 (0.14%) that they were Roma, compared to 0.12% and 0.18% in England overall [15]. UKHSA do not report data on TB incidence separately for these groups.
As of 30th June 2024, 4,166 people had arrived in Surrey under the Homes for Ukraine programme, 503 residents had arrived under the Afghan Resettlement Programme, and 481 asylum seekers were receiving Home Office Support, of whom 311 were living in contingency accommodation such as hotels (down from 989 in June 2023) [16]. These three groups make up 0.42% of the Surrey population, near-identical to the UK average of 0.41%.
Estimated rates of opiate usage are lower in Surrey (0.42%) than the England average of 0.82%; In 2021/2 there were 118 people who had been identified as being homeless with a drug dependency need in Surrey [17]. 2,178 people were in treatment for alcohol dependence.
Rates of homelessness are also lower in Surrey, at 2.74 per 1000 households, than in England overall (6.08 per 1000) [18].
There are five prisons within Surrey [19]:
- HMP & Young Offender Institute (YOI) Bronzefield
- HMP Coldingley
- HMP & YOI Downview
- HMP High Down
- HMP Send
As of September 2024, these had a combined population of 2,710 [20]. This comprises 3.1% of the English prison population, higher than the 2.1% of England’s overall population that live in Surrey.
Epidemiology of TB in Surrey Heartlands
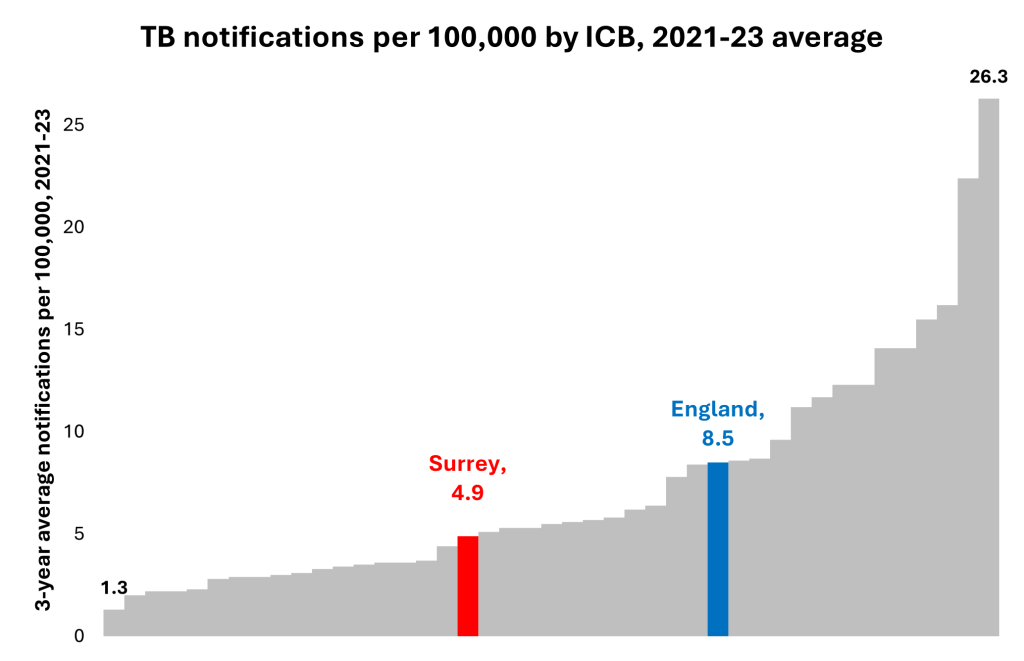
Surrey is a county with low TB incidence. Figure 4 shows that between 2021 and 2023, Surrey Heartlands had well below the overall English notification rate at 4.59 per 100,000. However, because TB is highly concentrated in a few areas, Surrey Heartlands is only just below the median ICB rate of 5.4 per 100,000.
Figure 4: ICB-level average TB notifications per 100,000, 2021-23. England notifications in 2023 included for comparison. Data from “Tuberculosis incidence and epidemiology, England, 2023,”[3].
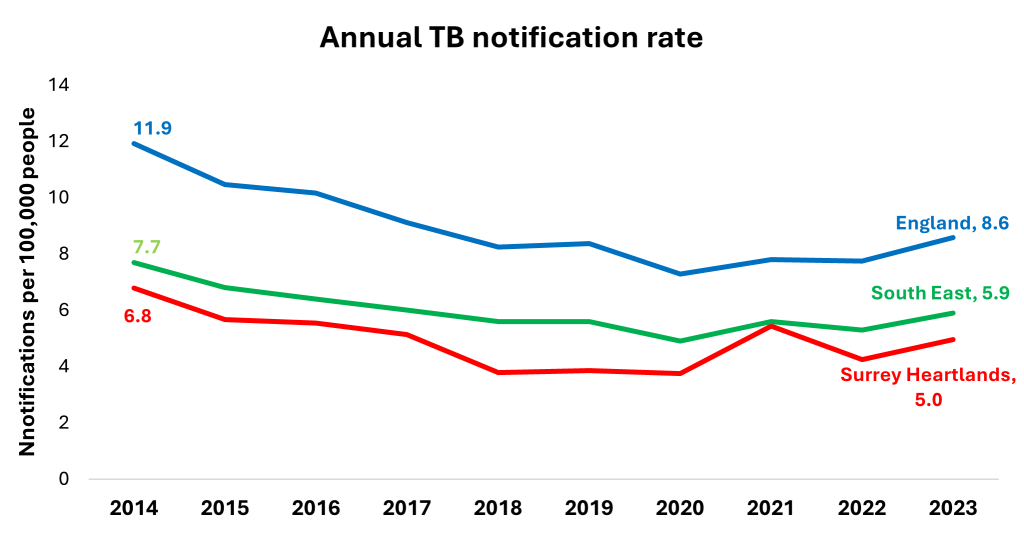
TB in Surrey Heartlands has followed national and regional trends (Figure 5), with the number of active TB cases nearly halving between 2014 (69 cases notified) and 2018 (39 cases notified). This then rose to 53 cases in 2023 (5.0 per 100,000) and 57 between July 2023 and June 2024 (5.3 per 100,000) [2]. While full 2024 data are not yet available, Surrey’s service providers have indicated that they have seen further increases in the second half of the year. Notifications were 13.6% higher in England and 4.9% in the South East in Q1-3 2024 compared to Q1-3 2023 [2].
Figure 5: Rate of TB notifications per 100,000 in England (blue), the South East (green) and Surrey Heartlands (red) since 2014. England and South East data from National quarterly report of tuberculosis in England: quarter 3, 2024, provisional data – GOV.UK [2] and “Tuberculosis in England, 2023 report (data up to end of 2022),”[4].
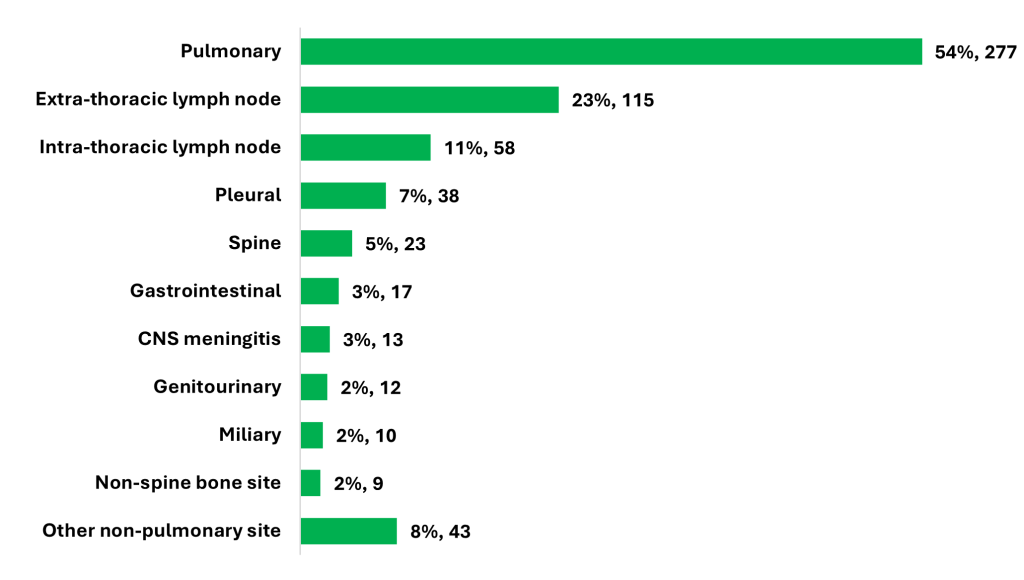
In 2023, 53% of notified active TB cases in Surrey Heartlands were pulmonary and 38% were in lymph nodes. Sites of disease have been broadly constant over the last decade (Figure 6) and are in line with the England averages [2].
Figure 6: Sites of active TB cases notified between 2014 and 2023 in Surrey Heartlands. People may have TB in more than one site, so percentages do not sum to 100.
This masks some clear variations with demographic groups. 74% of UK-born patients presented with pulmonary TB and 15% with lymph nodes TB, but 49% of UK-born patients presented with pulmonary TB and 38% were lymph nodes. Exactly half of cases in people from each of the Bangladeshi, Indian and Pakistani ethnic backgrounds presented with TB in the lymph nodes.
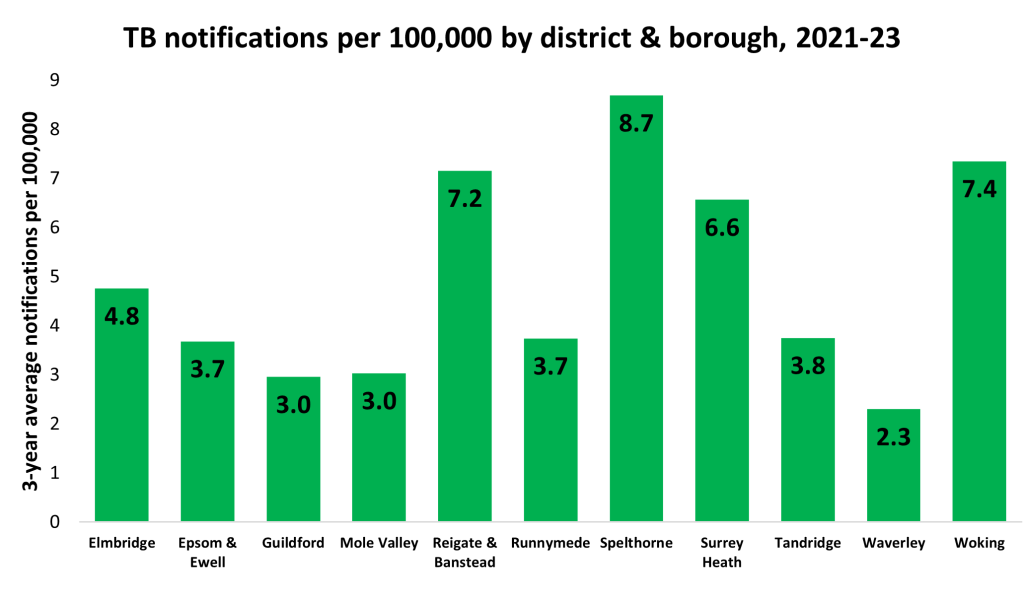
On a district and borough level, in 2021-23 Surrey’s TB notification rates were highest in Spelthorne, Reigate and Banstead and Woking and lowest in Waverley (Figure 7). The relatively small number of cases means that geographical analysis at a more local level did not give any meaningful insights and could have resulted in patients being identifiable. Between 2019 and 2023 no Lower Layer Super Output Area (a geography with between 1,000 and 3,000 residents) had more than five TB notifications. Because cases of TB in Surrey were widely dispersed, the potential benefits of geographically targeted awareness-raising campaigns are limited.
Figure 7: Lower-tier local authority average TB notifications per 100,000 population, 2021-23. Data from “Tuberculosis in England, 2023 report (data up to end of 2022),”[4].
As with England overall [4], in most years there are slightly more notifications for TB in males than females. The proportion of new notification has fluctuated between 49% and 65% over the last decade, sitting at 53% in 2023.
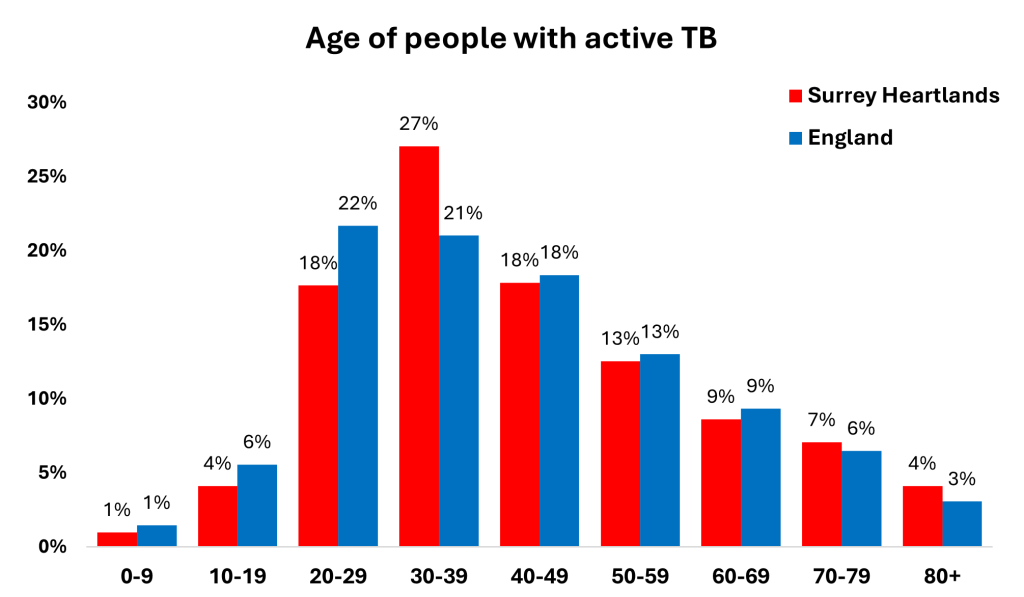
Similarly, the age distribution of cases is similar to the national average in 2022, though with slightly higher proportions in people in their thirties and slightly lower proportions in people in their 20s (Figure 8). Three-quarters being reported in adults between 20 and 59. There are very few cases of active paediatric TB in Surrey Heartlands, with only 13 cases between 2014 and 2023 (2.5% of all cases), compared to 2.9% in England in 2023 and no more than two paediatric cases in any single year.
Figure 8: Age profile of newly notified TB cases in Surrey Heartlands (2023, red) and England (2022, blue).
Between 2019-23, two-thirds of adults with TB were recorded as being employed (excluding the those for whom employment information was unavailable). 7% described themselves as working in IT and 11% were in healthcare; the latter figure has remained broadly consistent over time.
| Status | Proportion of cases in Surrey Heartlands, 2019-23 |
|---|---|
| Employed | 66% |
| Not employed | 17% |
| Retired | 13% |
| Student | 4% |
Throughout the UK, TB is more common in people born in high incidence countries, people from an ethnic minority background and people living in more deprived communities [4]. Surrey is no exception.
While 86% of the population in the 2021 census described themselves as White, only 29% of people diagnosed with TB between 2019 and 2023 did so (Figure 9). Rates of TB were highest in people with Indian, Pakistani and Black ethnic backgrounds (Table 1). There have been too few cases to establish whether there have been any meaningful trends in ethnicity over the last decade.
Figure 9: The ethnicity of people diagnosed with TB between 2019 and 2023 and of Surrey overall in the 2021 census [14]. To prevent disclosure the three sub-categories of Black ethnicity have been combined, as have mixed and other backgrounds. Those with no ethnic group recorded have been excluded.
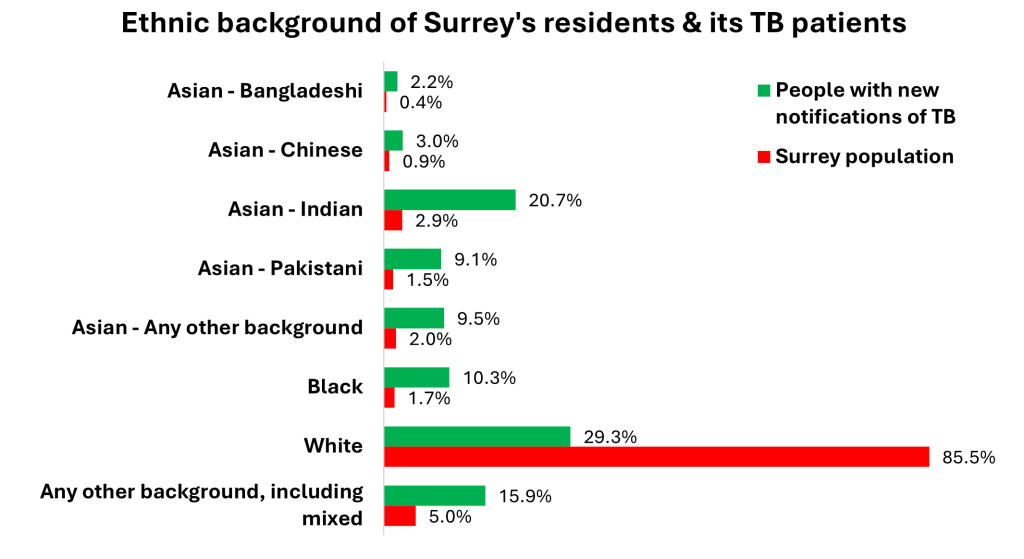
Table 1: Ethnic background of people newly notified as having TB in Surrey Heartlands, 2019-23, and rate per 100,000 population based on the 2021 census.
| Ethnicity | Newly reported TB cases, 2019-2023 | Incidence per 100,000 |
|---|---|---|
| Asian – Bangladeshi | 5 | 96 |
| Asian – Chinese | 7 | 63 |
| Asian – Indian | 48 | 137 |
| Asian – Pakistani | 21 | 117 |
| Asian – Any other background | 22 | 93 |
| Black | 24 | 115 |
| White | 68 | 7 |
| Any other background, including mixed | 37 | 61 |
| Not recorded | 2 | – |
80% of TB cases between 2019 and 2023 were in people born outside the UK, the same as the England average in 2023 [3]. As Table 2 shows, the great majority of cases were in people who had moved to the country many years ago, which would limit the potential for changes to the screening of new migrants to reduce incidence in future. There has however been a recent uptick in the number of TB diagnoses in migrants who have lived in the UK for under two years, from an average of five per year between 2019 and 2022 to 11 in 2023. Five of these 11 people were asylum seekers or refugees.
There was an average of eight cases per year in UK-born people in each of 2022 and 2023, compared to an average of 14 between 2014 and 2019. It is not clear whether this is a fluctuation due to small numbers or a meaningful change.
Table 2: Years of residence in the UK of people newly diagnosed with TB in Surrey Heartlands. Excludes those whose duration of residence is not recorded.
| Years of residence | Proportion of cases 2019-23 |
|---|---|
| UK-born | 20% |
| Under 2 years resident in UK | 14% |
| 2 to 4 years resident in UK | 17% |
| 5 to 9 years resident in UK | 14% |
| Over 10 years resident in UK | 33% |
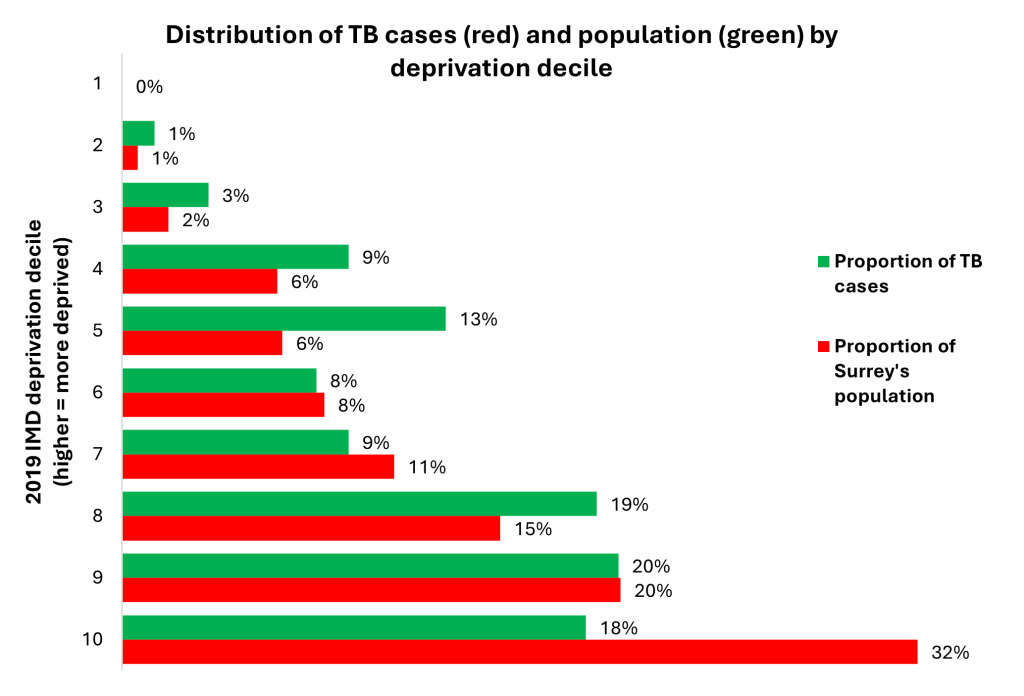
Figure 10 compares the deprivation deciles of the Surrey Heartlands neighbourhoods in which TB patients live (green) with the overall distribution of deprivation in Surrey Heartland’s population (red). As would be expected, rates of TB are highest in the most deprived neighbourhoods. However, because of Surrey’s overall affluence, the great majority of cases are found in less deprived communities. This sits in contrast to England as a whole, where only 13% of cases were found in the three least deprived deciles [3]. This means that even highly-effective awareness-raising measures targeted at GPs working in the most deprived communities could pick up only a small minority of cases.
Figure 10: Distribution of cases of TB in Surrey Heartlands (green) between 2019 and 2023 and Surrey Heartlands’ overall population (red) by Lower Layer Super Output Area neighbourhood IMD deprivation level.
Comorbidities
People infected with TB (whether recently or many years earlier) are more likely to develop active disease if certain underlying conditions are present. Older age, certain medical treatments and serious illnesses such as HIV weaken the immune system and can cause latent bacteria to reactivate or make the immune system unable to kill or contain the bacteria following recent infection. Comorbidities may be related to socioeconomic inequalities and resulting lifestyle factors that already increase the risk of TB, or links to countries where blood borne viruses and TB are more common.
Data on six comorbidities have been collected regularly since 2018. Rates have remained stable over this period, with 31% of patients having had at least one comorbidity recorded in 2023. The proportion of TB patients who are immunosuppressed is noticeably higher than the England average and the diabetes prevalence lower.
Table 3: Surrey Heartlands’ prevalence of comorbidities between 2018 and 2023 and England in 2023, as percentages of those people who had this information recorded. Differences in the way that data are recorded means a direct 2018-23 comparison is not possible. England data from “Tuberculosis incidence and epidemiology, England, 2023,” [3]. Overall England comorbidity data are not published.
| Comorbidity | Surrey prevalence 2018-2023 |
England prevalence 2023 |
|---|---|---|
| Diabetes | 8.9% | 11.5% |
| Hepatitis B | 2.6% | 2.2% |
| Hepatitis C | 1.7% | 1.3% |
| Chronic liver disease | 1.2% | 1.5% |
| Chronic renal disease | 5.1% | 2.8% |
| Immunosuppression | 15.9% | 9.0% |
| At least one comorbidity | 27.1% | n/a |
| More than one comorbidity | 5.3% | n/a |
TB diagnosis, screening and treatment
Time taken to diagnose and start treatment
Rapidly diagnosing and treating people with TB benefits the patient and, for pulmonary disease, also reduces the risk to others.
The TB Action Plan has a target of reducing the average treatment delay in people with infectious or pulmonary TB by 5% each year, from a baseline of 75 days in 2019 to 56 days in 2025-26. In this context, “treatment delay” refers to the time between reported symptom onset date and treatment start date. In 2022, 30.3% of people with TB notified in England took more than four months from symptom onset to treatment start.
Data are available for cases notified since 2018 on the time between:
- Symptom onset and first healthcare presentation
- First healthcare presentation and TB referral receipt
- TB referral receipt and TB service presentation
- TB service presentation to diagnosis
- Diagnosis to treatment start
- Symptom onset to treatment start (available since 2014)
These are summarised for pulmonary TB cases in Table 4. This should be interpreted with caution because the relatively small number of cases of pulmonary TB in Surrey means median durations are volatile, though the drop in 2023 is encouraging and is well below the 56-day target set for 2026 in the TB Action Plan.
Table 4: Annual median times between elements of the journey between symptom onset and treatment start for pulmonary TB cases.
| Year | Symptom onset and treatment start |
Symptom onset and First presentation |
First presentation and TB service referral |
TB service referral and TB service presentation |
TB service presentation and diagnosis |
Diagnosis and treatment start |
| 2014 | 81 | n/a | n/a | n/a | n/a | n/a |
| 2015 | 62.5 | n/a | n/a | n/a | n/a | n/a |
| 2016 | 80 | n/a | n/a | n/a | n/a | n/a |
| 2017 | 83 | n/a | n/a | n/a | n/a | n/a |
| 2018 | 75 | 19.5 | 36 | 0 | 0 | 1 |
| 2019 | 103 | 31 | 18 | 0 | 2 | 1 |
| 2020 | 74 | 29 | 46.5 | 2 | 3 | 3.5 |
| 2021 | 68 | 35.5 | 29 | 0 | 0 | 1 |
| 2022 | 80 | 29 | 13 | 1 | 1 | 2 |
| 2023 | 48.5 | 20.5 | 16 | 1 | 0 | 1 |
Similarly, the proportion of cases that take over 4 months from onset to treatment is highly susceptible to small changes and therefore does not provide much useful insight. It was 29% in 2021, 48% in 2022 and 38% in 2023. While the 2023 figure is higher than the England average of 30%, so was the proportion taking under 2 months, at 50% in Surrey against 40% in England.
In most years, the largest component of the time between symptoms and treatment has been the time taken to present to health services for the first time, followed by the time taken for health services to refer patients to the TB service. By contrast, once pulmonary TB patients are referred to the TB service, they very rapidly start treatment.
This means that efforts to reduce the time in which infectious TB patients are in the community could focus on:
- Encouraging and enabling people to see a primary care provider as soon as possible, although there is a limit to how much this can reduce the time to treatment, given the persistent nature of a cough associated with pulmonary TB
- Increasing awareness of TB among primary and secondary care professionals so that they consider TB as a differential diagnosis alongside more common conditions such as lung cancer.
Diagnosis takes longer for non-pulmonary cases, which is unsurprising given symptoms are less distinctive in some of these sites:
Table 5: Proportion of cases completing this part of the process within a week. Excludes those with recorded times less than zero, indicating that e.g. they were diagnosed before presenting to the TB service.
| Stage | Pulmonary (% taking less than a week for this stage) | Non-pulmonary (% taking less than a week for this stage) |
|---|---|---|
| Referral to TB service presentation | 85% | 84% |
| TB service presentation to diagnosis | 75% | 56% |
| Diagnosis to treatment start | 92% | 79% |
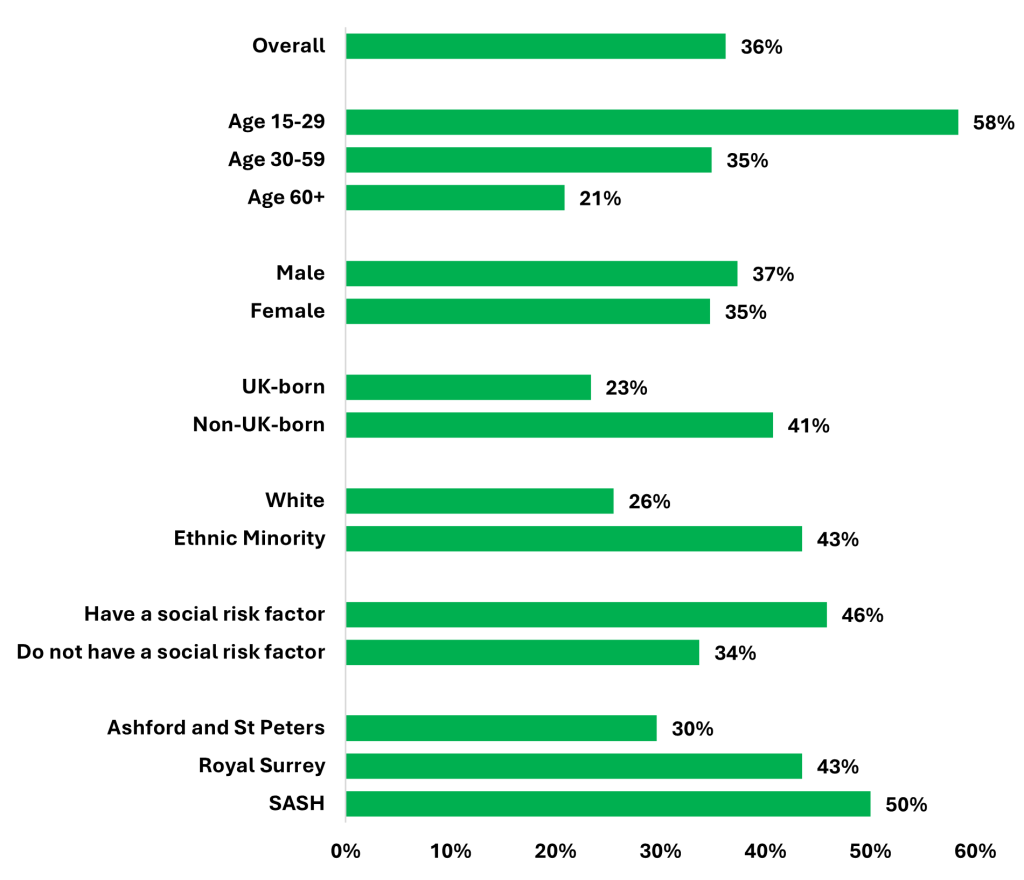
Patients are less likely to start treatment within two months of symptoms starting if they are part of demographic groups where TB incidence are lower (Figure 11). This suggests that GP are less likely to consider TB as a possible diagnosis in patients they see as lower risk.
Figure 11: Percentage of pulmonary TB patients between 2019 and 2023 in Surrey Heartlands who start treatment within two months of symptom onset.
When asked why there are sometimes delays between patients presenting in primary care and being referred to the TB service, interviewees at all TB services thought a lack of awareness of the disease and the relatively low incidence locally means TB is not being considered as a differential diagnosis, particularly in White British patients. In addition, each of these issues were raised by a provider:
- GPs not knowing they should send off sputum samples for testing
- Lack of knowledge of the correct referral pathway
- Language barriers in primary care, with GPs unable to get the right translation services
- Patients not being able to get timely GP appointments
Data on the healthcare settings of first presentation are available for 189 patients since 2018. Of these:
- 80 first presented at their GP (median time between presentation and TB service referral 51 days)
- 56 at A&E (median time between presentation and TB service referral 51 days)
- 9 through contact tracing
- 45 in another setting
This shows the challenge of reducing treatment delays by raising awareness of TB amongst GPs. There are 922 GPs in the Surrey Heartlands area [21]. Given the low incidence of TB, the diversity of settings where patients present and the geographical spread of cases within the county, few healthcare professionals in Surrey will see a patient with TB in any given year. Many of them will already refer rapidly to TB services.
Any attempt to develop a targeted GP awareness-raising campaign is therefore unlikely to be successful. For example, there were 234 cases of TB in Surrey Heartlands between 2019 and 2023. Only 24 were in neighbourhoods (LSOAs) where there had been more than one case in the previous five-year period.
For that reason, targeted awareness-raising work does not form a recommendation in this needs assessment. A more appropriate audience for training would be GP trainees, including making sure that they know how to refer and understand the samples that should be taken. This could include using the Royal College of GPs’ online training resources.
The TB service providers interviewed had had varying experiences of delays in referral or diagnosis relating to secondary care.
- Royal Surrey thought that in instances where TB had not initially been suspected, this was generally for understandable reasons, such as patients being from a low-risk country and having atypical symptoms. They have had issues where patients who have been given bronchoscopies by a non-TB consultant have not had their samples tested for TB. Another concern is an ongoing reluctance of their microbiology department to do PCR tests (described as “dragging their feet”), despite this forming part of the NICE guidelines. This has caused delays in diagnosis. Neither Ashford & St Peter’s nor SASH have had similar problems.
- Ashford & St Peter’s have previously experienced problems with their A&E colleagues not suspecting TB despite the presence of classical symptoms and chest x-rays. They have recently run a training session with A&E staff but say it is too early to tell whether that has been effective.
- SASH have had problems with their imaging colleagues either missing TB cases or not appropriately reporting them to the TB team. They have also had delays in diagnoses due to patients having to wait for bronchoscopies or CT scans.
When asked for an example of what works well within their TB service, Ashford & St Peter’s answered “patients, once we become aware of them are seen very quickly, usually within 24 hours”. SASH said that referral into the service works well.
A TB nurse at Ashford & St Peter’s has recently undertaken a quality improvement project following a patient’s diagnostic delay. Any radiology reports (MRI, CT, X-ray or ultrasound) that mentions potential TB automatically triggers an email to be sent to a pre-configured list of staff including the TB team. The nurse interviewed for this needs assessment described it as:
“very successful and definitely reduces delays in diagnosis. With this system we become aware of the patient as soon as the scan has been reported on and can screen timeously. We call patients on the same day to start the screening process.”
They have subsequently extended this to cover sputum results.
Other than the A&E training at Ashford & St Peter’s, none of the services offer education to other healthcare staff, though all three indicate this is something that they would like to do regularly.
Table 6 shows providers’ responses when asked whether referral pathways exist from different parts of their trust. Royal Surrey do not have pathways in place from some relevant services but are attempting to establish these.
Table 6: Whether pathways exist within trusts for referrals to TB services from each department. From service provider questionnaire.
| Service | Royal Surrey | Ashford & St Peter’s | Surrey and Sussex |
|---|---|---|---|
| A&E | Yes | Yes | Yes |
| Radiology | No | Yes | Yes |
| Microbiology | No | Yes | Yes |
| Histopathology | No | Yes | No |
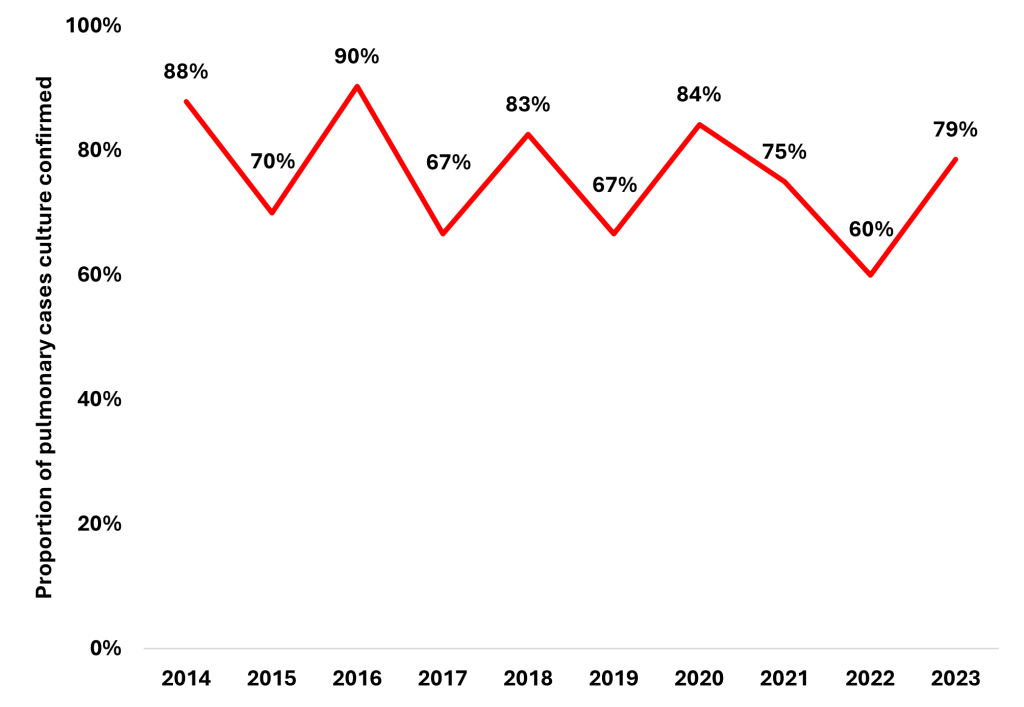
The TB action plan aims to increase the proportion of pulmonary TB cases that are culture confirmed to 80% by 2024. In Surrey Heartlands this has only been achieved in four of the ten years with available data; rates appear to be on a gradual downwards trend (Figure 12).
Figure 12: Culture confirmation rates for pulmonary TB cases in Surrey Heartlands.
Treatment
The vast majority of active TB patients in Surrey are successfully treated. 86% of patients whose cases were notified between 2014 and 2022 had been successfully treated within 12 months and a further 5% were still in treatment. 5% (20 people) had died, 3% (12) were lost to follow up and 1% (4) were known to have not completed treatment. In line with national reporting, treatment outcomes data exclude cases which are MDR or rifampicin resistant and central nervous system, spinal, miliary or cryptic disseminated disease as patients with these forms of disease may have planned treatment for more than 12 months. 2023 data are not included as the 12-month point had not been met for most of these cases at the time of data extraction.
The small number of cases means that one or two people not completing treatment can affect treatment outcome results. This means it is not possible to determine any clear temporal trend in completion rates or between-service variation. The 12-month completion rate of 80% in 2022 was slightly lower than usual and below the South East overall (86%). Over the most recent five years of complete data (2018-2022), no service had more than five patients who did not complete treatment, died or who were lost to follow up.
Five people whose cases had been notified in 2023 had died within 12 months, of whom TB was known to have contributed to the deaths of three patients. This is the first time since 2016 that more than three people notified as having TB had died within a year.
Of the 16 people whose case of TB was notified between 2014 and 2022 and who did not complete treatment or who were lost to follow up (but excluding those who died), 7 (44%) had at least one social risk factor including 6 (38%) who are recorded as having experienced homelessness. Completion rates were similar in UK-born and people born overseas.
Multi-drug-resistant TB (defined as being resistant to at least isoniazid and rifampicin) is extremely rare in Surrey, with only 4 cases between 2014 and 2023 (1.2% of culture confirmed cases). 2.7% of culture confirmed cases in the South East and 1.6% in England in 2022 were multi-drug resistant.
7% of culture-confirmed cases in 2023 were resistant to at least one first-line treatment, well below the South East average of 13.2% and the 2022 England average of 11.9%. Resistance rates have been consistently low, with between one and four cases every year between 2014 and 2023.
Over the 2014-23 period for which data are available, there was only one confirmed case of M. bovis and one of M. africanum, with all other speciated cases being M. tuberculosis.
All service providers said that they very rarely have delays in patients starting treatment following diagnosis of active TB, although as previously mentioned, Royal Surrey’s waiting times for LTBI treatment are around 6-12 months. Getting patients to complete LTBI treatment generally requires more work from the TB teams than active TB, given that they will have previously been asymptomatic but treatment can cause side-effects.
All three services have had problems with medical professionals being referred to them by occupational health with latent TB but not attending their appointments or being reluctant to start treatment, though Royal Surrey said they have seen an improvement in this recently. SASH have been running a clinic in the occupational health department to approve attendance. They are not yet sure whether it has had this effect.
SASH stated that they sometime have delays in getting medication if there are shortages or their pharmacy runs out.
Screening
NICE recommends screening or active case finding for TB is offered to:
- new migrants from high incidence TB countries
- new patient-facing NHS employees
- close contacts of people with pulmonary or laryngeal TB
- homeless people and people who misuse substances in areas of identified need
- new arrivals to prisons and immigration removal centres [7].
Screening of people from high incidence countries
Residents of high TB incidence countries (over 40 cases per 100,000 per year) who apply for a UK visa lasting six or more months are required to be screened for pulmonary TB. The most recent annual report for this screening programme covers 2020. In that year it detected 385 active TB cases (113 per 100,000 applicants). The report does not include any information on the planned place of residence of visa applicants, so it is not possible to determine how effectively this prevents TB in Surrey.
LTBI screening should be offered to new migrants to the UK who present to healthcare services if they are aged 16-35 and from countries with incidence over 150 per 100,000 per year [22].
A national LTBI testing and treatment programme is funded by NHS England to provide this service. It is currently offered to local authority areas with incidence of 20 cases per 100,000, therefore this service is not provided in Surrey.
It is not possible to determine the extent to which GPs offer LTBI testing to migrants when they first register at the practice. However, the GP who was interviewed for this needs assessment considered it very unlikely that many practices do this, given the limited time they have with each new patient.
There is a developing risk nationally around TB in social care staff. While pre-entry screening should prevent new migrants with active TB starting work, they will not be screened for latent infection, leaving a risk of its reactivation and the exposure of vulnerable clients to TB.
Screening of new health and social care workers
Screening of NHS staff is provided by occupational health teams at all three hospital trusts that provide TB services. Reflections on this are given in the treatment section of this report.
Contact management
Contact tracing aims to identify people with undiagnosed active TB or latent TB. In the first instance it is carried out by TB nurses, supported by UKHSA’s Kent, Surrey and Sussex Health Protection Team when the risk to public health is judged to require it.
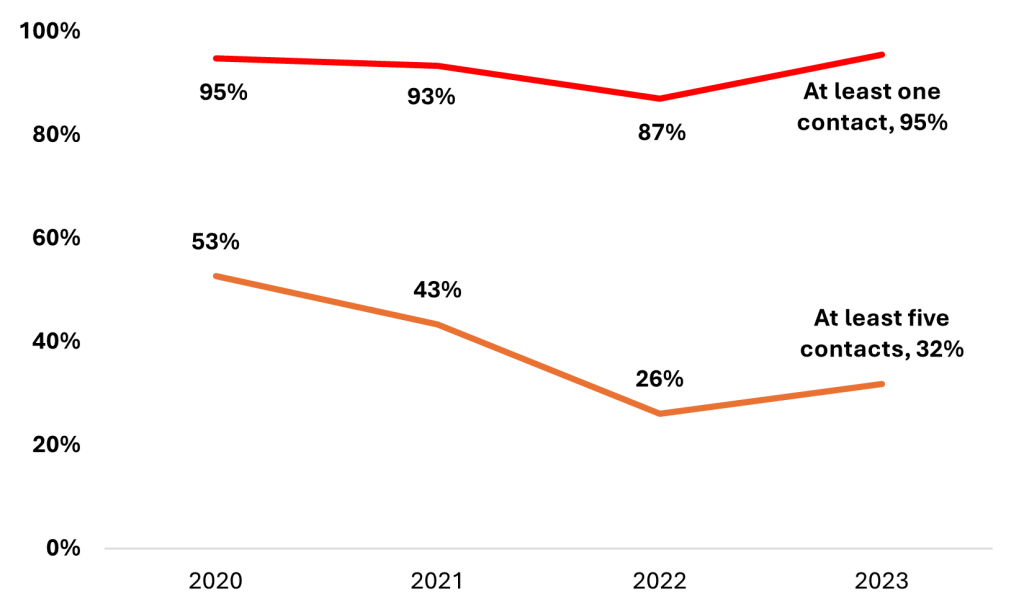
The National Service Specification states that the average number of close contacts traced per pulmonary TB patients should be at least five, “aspiring to 10”. Similarly, the TB Action Plan requires UKHSA to report annually on the target of “90% of pulmonary or infectious TB cases to have a minimum of 5 close contacts (household and non-household) identified and screened” [6]. As of the 2023 annual report, national data are not available on this metric.
Figure 13 shows that the proportion of people with at least five close contacts is well below 90%. Since 2020, 11% of cases have had ten or more identified contacts, with 22 being the highest number traced. The median number of contacts was three, the same as recorded in both England and the South East between July 2023 and June 2024.
There was little variation in the number of contacts traced between the three trusts: over the 2020-23 period, the five-contact target was met 36% of the time by Ashford and St Peter’s, 38% by SASH and 50% by Royal Surrey.
Figure 13: Proportion of pulmonary TB cases in Surrey Heartlands with at least one (red) and at least five (orange) contacts. Excludes a small number of cases for which no contact data were recorded.
Providers were uncertain why so few patients reported five or more contacts. Two thought that an increase in working from home means that there were fewer contacts to be identified. Stigma was also raised, particularly with regards to patients living in shared accommodation. Two providers said they would be able to identify more contacts if they were able to do home visits.
A large majority of contacts of people with infectious TB are willing to be tested for TB, with services’ estimates of attendance ranging from 80%-95%. When asked for the main reasons why some choose not to be tested, all three service providers talked about contacts feeling that it isn’t necessary because they did not have symptoms. Again, one provider raised the stigma of TB. Royal Surrey said that their uptake of screening for medical professionals identified as contacts of infectious patients is much lower, at around 50-60%.
Pre-biologic testing
Use of some biologic therapies increases the risk of reactivation of LTBI [23], with the TB Action Plan including a goal of strengthening prevention in this population. SASH and Ashford and St Peter’s have pathways for this, where Interferon Gamma Release Assay (IGRA) testing is provided by the team who are treating the patient. They then refer to the TB team if positive. Royal Surrey do not have a pathway in place but have indicated they would like to set one up. They would like this to include some awareness raising of the symptoms of TB amongst patients at higher risk of LTBI reactivation who are starting biologics so that they can seek treatment more quickly. This has followed a couple of occasions where people starting biologics have had TB activated despite having either screened negative or been previously treated.
Recommendations
To reduce diagnosis times, other service providers should consider adopting Ashford and St Peter’s approach of automatically notifying suspected TB cases to the TB team.
Ensure all services can access Polymerase Chain Reaction (PCR) testing without delay when required.
Royal Surrey to ensure appropriate referral, testing and treatment pathways are put in place from all their relevant departments, including for patients starting biologics and children with both active and latent TB.
Service provision
Commissioning
The three TB service providers in Surrey are commissioned by Surrey Heartlands ICB. SASH is separately commissioned by Sussex ICB for services in that county, leading to differences in what is provided for patients in the two parts of their patch. TB services are commissioned as part of the standard annual contract with providers and there is no separate funding stream. The national service specification can be included in contracts to set out service expectations and it is recommended that Surrey Heartlands take this approach in the next contract round.
Service mapping
The table below shows a high-level mapping of the services provided by each of the three trusts in Surrey. Information is based on returns to a questionnaire completed by TB service members in July and August 2024. Where relevant, the services are labelled as being recommended by NICE, the UKHSA Action Plan (AP), the National Service Specification (NSS), the Royal College of Nursing (RCN) or the Green Book (GB)
| Service | Royal Surrey | Ashford and St Peter’s | Surrey and Sussex* |
|---|---|---|---|
| Number of clinics | Consultant: one per fortnight Nurse: two phone clinics per week and one in person per fortnight |
Doctor: one per week Nurse: one per week Tuberculin skin test: one per month BCG vaccination one per month Additional weekly clinic run by TB service for patients initiating biologics and with severe asthma. |
Consultant: one per week Nurse: one per week plus one per fortnight One pharmacist, physician associate and consultant clinic per week. Occupational health: one per month |
| Clinic timings | Weekday day times | Weekday day times | Weekday day times |
| Number of patients clinics have capacity for | Consultant: 12 every two weeks Nurse: 10 one week, 16 the next |
Doctor: 30 every two weeks Nurse: eight every two weeks |
41 per week |
| Specific LTBI clinic available | No | No | No |
| Able to see patients or hold clinics in the community. | No | Yes | No (available in Sussex) |
| Home visits offered | No | Yes | No (available in Sussex) |
| Outreach performed in high-risk communities | No | Yes, though limited | No (available in Sussex) |
| Every patient with active TB given a named case manager (NICE, RCN) | Yes | No | Yes |
| Staffing | Consultant 0.2 FTE TB nurse 0.45 FTE Admin staff 0.55 FTE (vacant) Other staff 0 |
1 Consultant Associate Specialist 3 nurses 1.5 FTE 1 admin staff |
Consultant 0.2 FTE 3 TB nurses 2.61 FTE 2 admin staff 1 FTE 1 physician associate 0.2 FTE 1 TB pharmacist 0.4 FTE |
| Active TB cases in children managed by paediatric trained nurses (NSS) | Never | Never | Always |
| Majority of TB nurses competent for phlebotomy (AP) | Yes | Yes | Yes |
| Majority of TB nurses nurse prescribers (AP) | No | No | No |
| Mutual aid arrangement in place with other services | No | No | No (available in Sussex) |
| Sufficient single rooms to isolate all infectious patients (NICE) | Yes | Yes | No |
| Negative pressure ventilation rooms available for suspected or confirmed MDR TB (NICE) | Yes | Yes | Yes |
| Neonatal vaccination available (GB) | Yes, delivered by midwives | Yes, delivered by midwives | Yes, delivered by midwives |
| Vaccination available for 1-15 year olds (GB) | Referred to Ashford and St Peter’s | Yes | See vaccination sections |
| Screening offered to new patient-facing staff (NICE) | Yes, provided by occupational health then followed up by TB team | Yes, provided by occupational health then followed up by TB team | Yes, provided by occupational health then followed up by TB team |
| Involved in screening new asylum seekers | Yes | Yes | Yes |
| Involved in screening other migrants from high incidence countries (NICE) | Yes | Yes | No |
| BCG vaccination provided to new TB team members (GB) | No | Yes | No |
| DOT available (NICE, AP, NSS, RCN) | No | Yes | Not routinely |
| VOT available (NSS, RCN) | No | Yes | Yes |
| Able to provide small incentives to support treatment completion (RCN) | No | No | Occasionally |
| Pathways available for people with MDR or XDR TB | Did not know | Yes, referred to St George’s. | Yes, discussed with St George’s |
| Provide or have access to outreach support services for socially complex cases | No | Don’t know | No (available in Sussex) |
| Induction provided for new starters (AP) | No | Yes | No |
| Student nurse placements provided (AP) | No | Yes | No |
| Access to resources to raise healthcare professional awareness (NICE, AP, RCN, NSS) | No | Yes, leaflets | Yes, posters and e-learning |
| Provide training for other healthcare professionals (NICE, AP, RCN, NSS) | No | Occasionally | No |
| Website to increase awareness of how health professionals can access the service (AP) | No | On their intranet | On their intranet |
| Collect patient feedback | No | No | No |
*Note: Figures for staffing and clinic capacity include Sussex-based patients
Staffing
The representatives of TB teams unanimously thought that they were insufficiently resourced to meet their caseloads, and did not have funding available to increase staffing provision.
“I feel we only provide probably 75% of what an actual specification of a TB service should be and even that I’m struggling to cover” [TB nurse]
The increase in complexity of cases means that more patients require additional services such as home visits, but only Ashford and St Peter’s can currently provide this. The position in Royal Surrey is particularly acute, with only 0.2 FTE of consultant time and 0.45 FTE of nursing time available, and the associated administrative post vacant. This has led to waiting times for LTBI treatment being between 6 and 12 months. This compares to around 4 weeks at SASH and 6 weeks at Ashford and St Peter’s, though staff at the latter say that waiting times at the latter have been increasing recently.
The RCN guidelines on staffing are that services should have one FTE case manager per:
- 40 active TB patients at any time or annually requiring standard case management
- 20 active TB patients requiring ECM
- 80 LTBI patients requiring standard case management
- 40 LTBI patients requiring ECM
Given increases in caseload and complexity that are not yet reflected in the data available for this needs assessment, calculating an appropriate staffing required would be misleading.
In addition to the medical staff, administrative staffing was considered inadequate by representatives from both Royal Surrey (whose 0.55 FTE administrative post is vacant) and Ashford and St Peter’s. SASH’s representative was content with their administrative support.
Providers were all asked whether they offered induction to new staff members and student nursing placements. Ashford and St Peter’s do both, but the other two providers do neither.
Facilities and accessibility of appointments
All service providers said their clinic sites had good transport links. SASH highlighted the difficulty some asylum seekers have faced accessing the site, often not having the money to attend appointments but not informing the TB team of this until they have missed an appointment. The TB team can pay for taxis for patients’ appointments, following a relatively straightforward internal process. Ashford and St Peter’s also said that they can refund the costs of travel for patients who are in receipt of benefits.
SASH were particularly concerned about being able to isolate infectious patients effectively. They do not have a separate outpatient area, so infectious patients need to sit in the main waiting room and they do not have enough negative pressure rooms that are suitable for TB patients. SASH are also unable to induce sputum in hospital, so some patients need to go straight to bronchoscopy.
Ashford and St Peter’s and Royal Surrey both thought they had appropriate facilities for everything they needed to do, although only the former believed they had enough space for their clinics.
Paediatrics
There have been few cases of paediatric patients (those under 15 years old) with active TB in Surrey, with only 13 cases between 2014 and 2023. At 2.5%, the proportion in under 15s is slightly below the 2.9% of TB cases in England. Provision of services for these patients varies considerably.
Paediatric cases in SASH are managed by a separate team that includes a paediatric consultant and a 0.4 FTE specialist paediatric TB nurse. SASH are confident that they have adequate provision to manage more straightforward cases, and that they can get help from St George’s where needed.
The (adult) TB nurses as Ashford and St Peter’s screen children aged one and over and if necessary, refer them to two paediatric consultants for their treatment. In some instances that team has not had capacity to take on patients, in which case they have been transferred to St George’s. While paediatric processes are currently functioning reasonably well, the TB nurse interviewed would like to have had a paediatric nurse to assist them.
In contrast, Royal Surrey have neither a paediatric TB pathway nor paediatric trained TB staff. They have not recently had a case of active TB in a child, and when they have managed cases of paediatric latent TB they have found treatment is often more complicated as it isn’t clear who should do what.
HIV
All active and latent TB patients should be offered a HIV test. In the last 5 years, HIV tests were recorded as having been offered to 96% of people whose HIV status was not already known, of whom 94% accepted the offer. The remaining nine people were not offered a test or had no record of being offered one (including two patients who died within 12 months of notification. It is not possible to determine from the data whether TB was diagnosed post-mortem). 94.4% of all patients in England notified with TB in 2023 with unknown HIV status were offered an HIV test.
Since 2020, none of Surrey’s three TB services have failed to offer a HIV test to more than one patient in a single year.
Vaccination
Vaccination of under ones whose parents or grandparents were born in a country with annual incidence of 40 or more cases per 100,000 are offered BCG vaccination during the Newborn and Infant Physical Examination and receive it in an outpatient setting. Between April and June 2024, BCG uptake in the county of Surrey was 83.3% at three months (England rate 77.4%) and at 83.6% at 12 months (England rate 84.5%) [24]. Unfortunately, data quality issues in previous years mean it is not possible to tell how uptake has changed over time.
Vaccination of eligible children aged 1 – 15 is provided by:
- Ashford and St Peter’s for West Surrey residents
- Frimley Park for Frimley residents
- First Community Health and Care for East Surrey residents.
There are ongoing problems with Mantoux testing for children aged 6-15 in East Surrey. Per the Green Book, this cohort require either a Mantoux or IGRA test to establish that they are tuberculin-negative before vaccination. First Community Health and Care are unable to maintain training and competence for nurses to complete these tests as the number of referrals they receive is too low.
In 2023 a short-term contingency plan was made with primary care and SCC Public Health to fill this gap while longer term solutions are considered. When a referral for BCG is received, First Community Health and Care request an IGRA alternative for the Mantoux skin test from the patient’s GP. If the GP is unable to accommodate the request, First Community Health and Care will link with the Surrey County Council public health team and the ICB Acute Paediatrics and Maternity commissioning team to agree a bespoke approach.
Since this agreement (less than a year) there have been just the referrals to First Community Health and Care, with only one child aged 6-15 requiring BCG after IGRA testing.
Recommendations
All TB services to have national TB service specification included in their contracts.
Services should be sufficiently well-funded that staffing levels can meet Royal College of Nursing (RCN) guidelines and services such as Directly Observed Treatment (DOT) and Video Observed Treatment (VOT) can be provided consistently.
Longer-term solution for tuberculin testing to be developed to enable BCG vaccination of 6-15 year olds in East Surrey.
Royal Surrey to ensure appropriate referral, testing and treatment pathways are put in place from all their relevant departments, including for patients starting biologics and children with both active and latent TB (this recommendation has been repeated from previous section).
Inclusion health
NHS England define inclusion health as “an umbrella term used to describe people who are socially excluded, who typically experience multiple overlapping risk factors for poor health, such as poverty, violence and complex trauma. This includes people who experience homelessness, drug and alcohol dependence, vulnerable migrants, Gypsy, Roma and Traveller communities, sex workers, people in contact with the justice system and victims of modern slavery” [25].
Social risk factors
Data are available in NTBS on whether TB patients:
- Have their ability to self-administer treatment affected by alcohol use
- Have past or current problem drug use
- Are or have been homeless
- Are or have been incarcerated
- Have their ability to self-administer treatment affected by their mental health (collected since 2018)
- Are seeking asylum in the UK (collected since 2021)
- Are in an immigration detention centre (collected since 2021).
Between 2018 and 2023, 14.1% of patients in Surrey with active TB had at least one social risk factor, slightly below the England average of 16.2% between Q4 2022 and Q3 2024. 7.3% had more than one social risk factor.
Social risk factors were more common in men (20%) than women (7%) and overseas-born patients (15%) than UK born (13%). The former trend is also seen in England in 2022 (relative risk ratio 2.52) but the latter is the opposition on the national picture (relative risk rate 1.93 in those born in UK vs those born outside).
Between 2018 and 2023, 7% of Surrey’s patients had experienced homelessness, 5% were problem drug users, 4% were prisoners and 3% had issues with alcohol.
The relatively small number of cases of TB in Surrey means that it is hard to draw clear conclusions from NTBS about how the complexity of cases is changing over time.
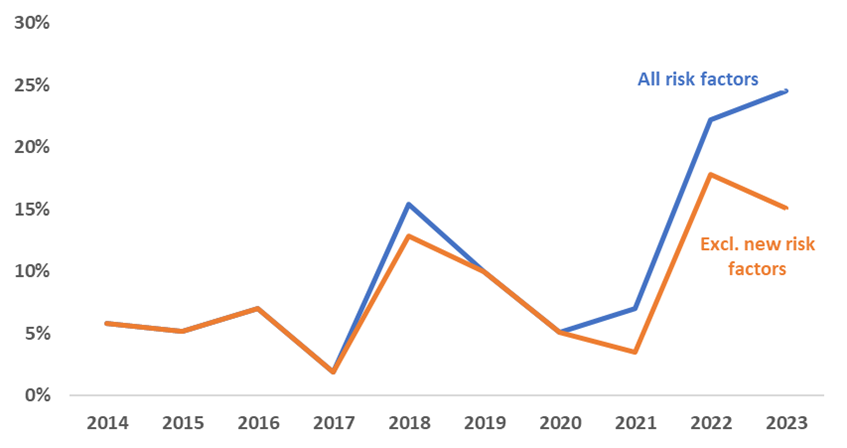
However, there has been a notable uptick in the proportion of cases with social risk factors. Some of this is due to the increase in people seeking asylum, who account for 11% of Surrey cases in the calendar years 2022-23 and the collection of data on immigration and mental health (each had under 5 cases in the calendar years 2022-23). Figure 14 shows that even excluding these newly collected factors, the prevalence of social risk factors was highest in 2022 and 2023, although numbers are too small to determine which individual risk factors have become more common.
Figure 14: The annual proportion of active TB cases in Surrey Heartlands with at least one social risk factor including (blue) and excluding (orange) risks factors which only started to be collected between 2018 and 2021.
The increasing complexity of cases has increased the workload of the acute TB service providers. While Royal Surrey had not noticed a clear increase in complexity, both Ashford and St Peter’s and SASH both had, with more patients requiring enhanced case management (ECM).
“things like drugs, alcohol abuse, imprisonment, homelessness, all those social factors are more at play now than I think they were when I started” [TB nurse]
Both SASH and Ashford and St Peter’s emphasised an increase in patients with drug and alcohol problems and histories of homelessness or imprisonment.
SASH have also had a large increase in the number of asylum seekers; Surrey’s migrant hotels have been disproportionately within their catchment area. These patients are more likely to require interpreters, frequently cannot afford to travel to appointments and can be moved out of the region without notice, making treatment more difficult. Screening for this group can also be more complicated due to their accommodation. SASH have had to screen 300 people in a migrant hotel where there had been ten active cases.
Data on ECM has only been collected relatively recently. 58% of patients notified in 2022 and 51% in 2023 were recorded as needing ECM. Rates were noticeably higher in SASH (70% of all patients in 2022 and 2023) and Royal Surrey (68%) than Ashford and St Peter’s (28%).
Directly observed treatment (DOT) and video observed treatment (VOT)
Guidelines recommend that patients who require extra support in starting and completing treatment are given directly observed treatment (DOT) or video observed treatment (VOT). Eight patients were recorded as having received DOT in 2023, with a further four recorded as having refused it.
Provision of DOT and VOT varies across the Surrey Heartlands area. Royal Surrey offer neither as they do not have the funding for it.
Ashford and St Peter’s offer both, with VOT provided by University College London Hospitals (UCLH). This works well and has been popular amongst the patients who use it. DOT is provided by TB nurses visiting the patients in their homes.
SASH have struggled with the practicalities of getting VOT and DOT set up. This stems in part through a lack of clarity with funding. Before starting each VOT or DOT case they need to go through several approvals, including getting agreement on whether they or Surrey Heartlands ICB will fund it. The approval process for setting up VOT can delay the start of treatment by around 2-3 weeks. An issue they have experienced with VOT is that they are not told by the provider when a patient misses a single dose; they are only informed after a few missed days. SASH have faced similar issues getting DOT set up. They have attempted to deliver DOT through pharmacies, but each of them wants to set it up slightly differently and so a bespoke agreement would need to be set up. They have only managed to treat one Sussex patient with DOT in this way and none in Surrey.
Ashford and St Peter’s are the only service who are able to provide home visits or see patients in the community. In addition to DOT, they collect sputum samples, take blood and can deliver medication or visit unwell patients. In Sussex, SASH have funding for an outreach worker who can provide support to patients at home. This has worked very well, with the outreach worker able to get a rapport with patients. SASH do not have funding for this in Surrey. Those patients either have to call or visit the team in hospital for this.
Refugees and Asylum Seekers
On arrival in the UK, people who cross the Channel to Kent and seek asylum are taken to Western Jet Foil in Dover and then Manston, a processing centre near Ramsgate where immigration documents are issued and initial asylum interviews are held (Unaccompanied asylum seeking children are taken from Western Jet Foil into care with Kent County Council). They are offered a basic health check at Western Jet Foil to identify urgent medical issues [26]. This does not include TB screening but occasionally people with suspected TB are identified at this point. Only acute medical services are available at Manston.
Refugees and asylum seekers living in asylum accommodation provided by the Home Office are supported to register with a local GP, commissioned by Surrey Heartlands ICB [27]. Templates are available to all GP practices (through their online clinical system) that support the full health assessment as outlined by the Home Office.
In addition to the same new patient basic check provided to all patients, it is recommended that migrants be assessed for health needs that relate to their country of origin, prior life experiences and circumstances of their migration, as well as their circumstances in the UK [28]. Many migrants arrive to the UK from countries of high incidence TB, there are country-specific guides to help assessment and guide actions [29]. Those whose country of origin does not have high rates of TB may have been exposed to active TB infection due to the circumstances and nature of their journeys, increasing their risk of TB.
TB screening at new registration initial health checks provided by Surrey Heartlands practices include questions and background of patients. Given the short time given to single primary care consultations, and the likely difficulties encountered during this initial appointment (such as language barriers) it is not possible to determine how effective this assessment is likely to be, nor whether primary care follow the wider health check recommendations. These GPs are not commissioned to deliver screening for Latent TB or active TB infection, or for provision of BCG vaccination.
In four initial accommodation hotels, Surrey Heartlands have commissioned the Refugee and Asylum Seeker Service team from the Alliance for Better Care GP federation. In addition to initial health checks and primary care services, they can provide latent TB screening [27]. However, the Alliance for Better Care representative interviewed for this needs assessment reflected that TB screening is very difficult to the rapid turnaround times for this population. Blood borne virus and TB screening will typically not take place until several months after arrival in a hotel, leaving a high risk of transmission to a large number of people during this time.
The frequent moving of TB patients who are living in asylum accommodation is a result of Home Office policies. While this is not in the control of the Surrey health system, the asylum system is likely to continue to evolve in the coming months. This presents a possible opportunity to work with the Home Office to improve the provision of health services to people seeking asylum.
“The problem is, once the patients move on to another place, we’re not informed or we’re not allowed to be told where they’ve gone. So if you do a test and you get a result [after they have moved], what do you do then?” Alliance for Better Care representative
A related problem is that when people have been required to leave their Home Office-provided accommodation within 28 days of being granted asylum. This has led to an increase in the number of homeless refugees [30]. As a result, on 9th December 2024 the grace period was extended to 56 days [30].
One additional gap identified by Ashford and St Peter’s was for patient information sheets (which are currently provided by TB Alert) to be available in other languages, such as Dari. This issue was also raised by the Alliance for Better Care.
In November / December 2023, the NHS England South East regional public health team undertook a survey of Integrated Care Boards and TB service providers to understand TB screening arrangements in asylum contingency accommodation. This identified several challenges, and the NHSE regional team are working with ICBs to understand these in more detail and support delivery against best practice guidance as documented within “Tuberculosis (TB): migrant health guide” [22].
All the challenges mentioned here were highlighted in Surrey County Council’s Migrant Health Rapid Needs Assessment in 2023 [27] and the Surrey Director of Public Health’s 2024 annual independent report [31]. Further details on migrant health are available in those documents.
No recourse to public funds
A particular challenge is to provide housing for TB patients who would otherwise be homeless so that they are able to complete their treatment, particularly for people who have no recourse to public funds (NRPF).
NRPF is a condition set by the Home Office on those who are subject to immigration control under section 115 of the Immigration and Asylum Act 1999. People with a NRPF condition are not able to claim most benefits or access local authority housing. Most temporary migrants to the UK, and people who are here illegally do not have recourse to public funds. These details are set out under paragraph 6 of the immigration rules and include housing benefit, although there are some circumstances where public funds are available for those with NRPF, such as those with written exemptions [32], [33].
The legal definition of homelessness is a person who has no home in the UK or anywhere else in the world available and reasonable to occupy. A key priority of the TB Action Plan for England is to strengthen the prevention, detection, and treatment of active TB and/or latent TB infection in higher risk groups including the homeless [6]. In addition to the national strategy, for the purposes of TB control, NICE uses a broad and inclusive definition of homelessness that includes the need for secure and private space with the means to store and self-administer medication as well as not being in an enclosed air space with others who are at high risk of undetected infectious TB.
The Care Act (2014) states that local authorities must support adults with care and support needs who are ordinarily resident in their area or present in their area but of no settled residence, even if they have no recourse to public funds [33]. The Act outlines the way in which needs assessments should be carried out, how to determine who is eligible for support (including how charges should be made for residential and community care) and what the local authority obligations are.
If an individual meets the criteria for local authority housing under the Care Act, accommodation should be provided for them. At present, there is no agreement about how and by whom this should be funded in Surrey.
A template memorandum of understanding addressing the provision of housing and financial support to individuals with active pulmonary TB who have no recourse to public funds has been developed by UKHSA for county councils and unitary authorities to adapt and agree with ICBs and TB Services, including housing teams and Adult Social Care. It aims to provide an agreed local pathway for those who:
- have eligible care needs which engage section 18 of the Care Act 2014, or
- do not have eligible care needs but would experience a breach of human rights if homeless which engages section 19(1) of the Care Act 2014 or
- are barred from receiving support under section 18 or 19(1) of the Care Act 2014 due to meeting schedule 54 and 3 of the Nationality, Immigration and Asylum Act 2002 but would experience a breach of human rights if their needs were not met.
Prisons
NICE guidelines state that new prisoners should be symptom screened for TB within 48 hours of arrival [7]. Tuberculin-negative prison staff should be offered BCG vaccination.
Public Health England’s 2013 guidance on managing TB in prison [34] further states that
- prison healthcare teams should, alongside the local TB service, develop care plans for active or latent TB cases in their establishment
- prisoners should be kept in single cells if there is a high clinical suspicion of pulmonary TB, a chest x-ray with suspicion of TB, or confirmed cases of pulmonary disease who are still likely to be infectious.
There are five prisons in Surrey [19]:
- HMP & YOI Bronzefield: a women’s prison in Ashford.
- HMP Coldingley: a men’s prison near Woking.
- HMP & YOI Downview: a women’s prison in Banstead, close to the border with Sutton.
- HMP High Down: a men’s prison in Banstead, close to the border with Sutton.
- HMP Send: a women’s prison in the Borough of Guildford.
In January 2021, health and social care needs assessments were published for each prison by NHS England and NHS Improvement [19]. These reported arrival screening uptake rates of
- Bronzefield 96%
- Coldingley 73%
- Downview 78%
- High Down “three quarters” (exact percentage not stated)
- Send 84%.
Only one case of active TB was identified through this screening, in a patient that has previously been diagnosed in another prison. These needs assessments recommended that High Down increased its screening uptake rates. Send and Coldingley were judged to have had their TB needs met. No comment was made about Downview or Bronzefield.
Ashford and St Peter’s reported that they have strong relationships with the medical team at Bronzefield, whose nurses contact them when they have queries. However, they do not hear from other prisons and don’t know what screening they do.
The nursing team at Bronzefield agreed that relationships with Ashford and St Peter’s TB team are strong. They find possible cases of active TB around every six months, but they are seldom confirmed as TB. They rarely have issues getting people to take part in screening, are able to isolate suspected cases and can provide DOT to all patients. BCG vaccinations for staff are provided by their occupational health teams.
Bronzefield held mass TB screening events in April 2023 and May 2024 as part of a pilot scheme, finding large numbers of latent TB cases both times. This was popular with the prisoners, with 80% uptake at the second event.
The team at Bronzefield reported difficulty providing continuity of care as their average prisoner is only there for around two weeks and they cover a wide catchment area. This means that patients often cannot go back to Ashford and St Peter’s once released or transferred.
A specific issue relating to this is that patients with suspected active TB are isolated for long periods while awaiting diagnosis, with the harms that this causes. They have had difficulties arranging bronchoscopies as prisoners are more likely that usual to not attend planned appointments. The team would like to be able to arrange bronchoscopies at short notice when they are able to bring prisoners to appointments.
Other inclusion health groups
There is no current provision of TB services targeted at other inclusion health groups. A one-off screening project was held in August 2023 for homeless people in Redhill, provided by UCLH’s find and treat service. 37 people were given a symptom screen and x-ray, 18 people received health checks from the Alliance for Better Care and 4 were registered with a GP. No active TB cases were found. This received positive feedback from both those who used it and those who provided it.
The Alliance for Better Care’s equity team are nurses who build relationships over time with inclusion health groups, including in migrant hotels, Gypsy, Rome and Traveller communities, homeless shelters and domestic violence refuges. They perform outreach health and wellbeing checks with a focus on cardiometabolic risk and advice, Make Every Contact Count interactions and Very Brief Interventions and give smoking cessation advice and immunisations. They can support patients with GP registrations and GP appointments for clinical follow up. While they would be able to identify TB symptoms, they are not funded to provide TB-specific services.
The equity team clinical lead strongly recommended outreach teams as the best way to improve detection in people from inclusion health groups. One option for this outreach could be holding workshops with information about TB, followed by then a second visit for testing. This would ideally be as part of an ongoing relationship, rather than as a one-off exercise.
An issue experienced by all three acute service providers and the GP interviewee is that in most instances, people who are not registered with GPs are unable to access other healthcare services including district nursing. This makes identifying and treating cases of TB much more difficult. People in inclusion health groups are more likely to have faced practical, cultural or language barriers to registration, which can be overcome by skilled outreach workers. Others may not be willing to register for reasons including fear or stigma but would still benefit from being able to access health services that support TB care.
Ashford and St Peter’s have occasionally held outreach events at a homeless shelter in Woking, however all acute service interviewees stated that they did not have established relationships with other services such as homeless shelters, drug treatment providers, mental health services or people working on modern slavery that would help support the treatment of patients with complex social needs. A pragmatic solution would be for all system partners to work together to develop a shared list of contacts in these services, so they can be rapidly accessed as soon as they are needed.
Recommendations
Agree pathways for funding DOT or VOT treatments.
If service providers would like to offer DOT through pharmacies, processes should be agreed in advance with a selection of pharmacies so that patients can rapidly commence treatment.
Services using Video Observed Treatment (VOT) should be informed by their provider as soon as a patient misses a single dose.
Ensure appropriate pathways are in place in all Surrey’s prisons. Build relationships between the prison health teams and the relevant TB services.
Develop pathways for prison patients to get hospital appointments at short notice.
Continue to work with Home Office colleagues to prevent people living in asylum accommodation being moved without enough notice to transfer their medical care.
Extend inclusion health outreach across Surrey, including but not limited to active and latent TB screening and GP registration.
Establish and maintain a shared Surrey-wide list of contacts in support services to meet the wider needs of people in inclusion health groups.
Work across the health system to allow people who are not registered with a GP to access a greater range of services.
Agree a memorandum of understanding on the provision of support for people with active TB who have no recourse to public funds.
Patient perspectives
None of the TB services currently actively collect feedback from patients, so there was no existing data that could be analysed for this needs assessment.
All providers were requested to consider asking patients for bespoke feedback through two routes:
- A survey run through Microsoft Forms
- Telephone interviews
One provider agreed to approach suitable patients to seek consent to share their contact details with the HNA authors. The survey was not used.
Two former TB patients were interviewed. As with all qualitative interviews, this cannot give a representative picture of the service’s users. The patients were asked about:
- The early stages of their illness, including healthcare seeking and diagnosis
- The convenience of the service
- Whether they received the information and support they required needed from the service
- General perspectives on their time under TB treatment, including their recommendations for improvement.
Neither patient had had significant delays in seeking healthcare nor in diagnosis. One patient developed symptoms of pulmonary TB while being treated as an inpatient for another condition and was rapidly diagnosed. The other, who had non-pulmonary TB, went to a GP within a week of symptom onset, then took around a month to be diagnosed while other differentials were ruled out. As part of this process, their results were considered by a Multidisciplinary Team meeting; they fed back that she was not given enough information as to why this was needed and therefore was worried that they had another condition.
Both patients were able to start their treatment with the respiratory teams shortly after diagnosis and were able to get to their in-person appointments easily. They reflected that they were able to speak to the team whenever they needed to and were given enough information about their condition and treatment, though one would have liked some written information about how to manage the general recovery from their treatment’s side effects.
In general, both patients were extremely positive about service that they received for their TB and no significant concerns were raised.
Recommendation
Service providers should routinely collect patient feedback.
Appendix: questionnaire completed by TB service provider representatives
1 – Overview of Services
Is your TB service nurse or doctor led?
At which hospital/s does your organisation provide TB services?
Thinking about your TB clinics:
- How many clinics seeing TB patients run each week?
- What days of the week and times do they run?
- Are they TB-specific clinics or general respiratory clinics?
- Are the clinics run by Doctors or TB nurses?
Do you think that you have enough space for your clinics?
Does the clinic site generally have good transport links for patients?
How many TB patients do your clinics have capacity to see in a week?
Does the service see patients or hold clinics in the community?
Does the service offer home visits?
Does the service do other outreach work? Please give details of this work if yes.
2 – Staffing
Is every patient with active TB given a named case manager?
How many Consultants work within the TB service (Full time equivalent, FTE)?
How many Specialist TB nurses work within the service (FTE)?
How many admin staff work within the service (FTE)?
Do you have any other staff working within the service? If so, please give details of their roles and FTE.
Are active TB cases in children managed by paediatric trained nurses?
Are the majority of TB nurses with a caseload competent or qualified to carry out phlebotomy?
Are the majority of TB nurses with a caseload nurse prescribers?
Are there any current vacancies in your staffing? If yes, please give details
Do you think you current clinical staffing levels are sufficient? Please give details if no.
Do you think admin staffing levels are sufficient? Please give details if no.
Are there any cross-cover or mutual aid arrangements with other TB services?
Do you have anything further to add about staffing?
3 – Resources
Does the service have access to laptops and mobile phones for joining meetings and conducting virtual clinics?
Does the hospital have sufficient single rooms to allow all infectious patients to be isolated?
Does the hospital have negative pressure ventilation rooms that you can use for patients with suspected or confirmed multidrug resistant TB?
Does the team regularly use any behaviour or contact tracing toolkits?
Does the team attend any regional TB nurse peer support meetings (not including the Surrey and Sussex TB cohort review)?
Do you feel that you are able to access all appropriate diagnostic tests in a timely manner?
Do you feel that you are able to access all appropriate treatments in a timely manner? If not, please give details.
4 – Referrals
Is there a formal pathway for referrals to the TB service from:
- Primary care
- A&E
- Radiology
- Histopathology
- Microbiology
- Other hospital specialties If yes, please give details of which
Is there a specific referral pathway in place for paediatric TB? If yes, please give details
5 – Delays
What do you think are the main reasons for delays between symptom onset and patients presenting to healthcare services?
What do you think could be done to reduce delays between symptom onset and patients presenting to healthcare services?
What do you think are the main reasons for delays between patients presenting to healthcare services and being referred to the TB service?
What do you think could be done to delays between patients presenting to healthcare services and being referred to the TB service?
Are there frequently significant delays between patients with possible TB being referred to the TB service and having their first appointments with you? If yes, what do you think are the reasons for these delays?
6 – Screening and vaccination
What diagnostic(s) do you use to test for latent TB in contacts of active TB cases?
What diagnostic(s) do you use to test for active TB in contacts of active TB cases?
What proportion of contacts who are eligible for screening attend for testing?
What are the main reasons contacts give for not being tested?
Are unvaccinated, Mantoux-negative contacts of patients with pulmonary or laryngeal TB offered BCG vaccination?
Is there a testing pathway for LTBI for people starting biologics? If yes, how does it work?
Are active and latent TB screening offered to new patient-facing staff working in your trust? If yes, who carries this out?
Is the TB service involved in screening of:
- New asylum seekers If yes, please give details
- Other migrants from high TB incidence countries If yes, please give details
- Occupational health screening If yes, please give details
Is BCG vaccination offered to new TB team members in your trust?
Who provides neonatal BCG vaccinations in your area?
Who commissions neonatal BCG vaccinations in your area?
Who delivers BCG to under 16s (not neonates) at increased risk of developing TB in your area?
Do you have anything further to add about TB screening or vaccination?
7 – LTBI
How many patients have received LTBI treatment from your service in the last year?
What are your LTBI completion/adherence rates over the last year?
Who manages the treatment and follow up for contacts with LTBI?
Is there a specific clinic for LTBI?
What issues tend to arise that mean people with LTBI don’t start treatment?
What do you think could be done to improve LTBI treatment commencement rates?
What issues tend to arise that mean people with LTBI who start treatment don’t complete it?
What do you think could be done to improve LTBI treatment completion rates?
What is the waiting time for people starting treatment for LTBI?
If you have any further comments about your answers, or LTBI services more generally, please answer below
8 – Treatment
Do you offer DOT?
If yes:
- How is DOT funded?
- Who delivers DOT?
- Please give details of how DOT is given.
- How has use of DOT changed before the COVID-19 pandemic?
Do you offer VOT?
If yes:
- How is VOT funded?
- Who delivers VOT?
- Please give details of how VOT is given.
- How has use of VOT changed before the COVID-19 pandemic?
Are you able to provide small incentives to support people in enhanced case management to complete their treatment? If Yes, please give details
What issues tend to arise that mean people with active TB don’t start treatment?
What do you think could be done to improve active TB treatment commencement rates?
What issues tend to arise that mean people with active TB who start treatment don’t complete it?
What do you think could be done to improve active TB treatment completion rates?
9 – High Risk Populations
Are there pathways in place for referrals from:
- Small boat arrival reception centres If yes, please give details
- Migrant hotels If yes, please give details
- Prisons If yes, please give details
- Organisations providing support for homeless people If yes, please give details
Are there specialised pathways in place for treating people in the following groups?
- People seeking asylum If yes, please give details
- People with no recourse to public funds If yes, please give details
- Homeless people If yes, please give details
- People in prisons If yes, please give details
- People with multi or extensive drug resistant TB If yes, please give details
Do you provide or have access to outreach support services (similar to London’s Find and Treat) for socially complex cases such as people experiencing homelessness? If yes, please give details.
What mechanisms (if any) do the service have for linking socially complex cases to other services to help to address needs such as housing, drug use or access to benefits?
10 – Training
Does your TB Service provide an induction programme for new starters?
Does your TB Service offer student nurse placements?
Are there any gaps in training for staff in your service? If yes, please give details
Do you have access to materials and resources for raising awareness of TB amongst other healthcare professionals (posters, e-learning modules etc)? If yes, please give details
Does the TB service provide teaching/training or awareness raising for other health and social care professionals?
If yes:
- How often does this occur?
- Which health professionals is this targeted towards?
- What is the method of the teaching/training?
Does the TB service use a website or any other communication to increase awareness of how health professionals can access the TB service? If yes, please give details:
11 – Service User Perspectives
Does your service collect any insights or feedback from its patients? If yes, please give details
What were the general themes (both positive and negative)
12 – Provider Perspectives
What works well in the TB service?
What are the gaps in the TB service, or significant issues that you think should be addressed for TB services in your local area?
What changes have recently been made to improve your TB service?
What changes are planned to improve your TB service?
13 – Conclusion
If you have anything further to add then please do so here.
Glossary
A&E Accident & Emergency
BCG Bacillus Calmette-Guérin
CT scan Computed Tomography Scan
DOT Directly Observed Therapy
ECM Enhanced Case Management
FTE Full Time Equivalent
GB Green Book
GP General Practitioner
GRT Gypsy, Roma and Traveller
HNA Health Needs Assessment
HPT Health Protection Team
HIV Human Immunodeficiency Virus
HMP His Majesty’s Prison
ICB Integrated Care Board
ICP Integrated Care Partnership
ICS Integrated Care System
IGRA Interferon Gamma Release Assay
IMD Index of Multiple Deprivation
LSOA Lower Layer Super Output Area
LTBI Latent Tuberculosis Infection
MDR-TB Multi-Drug Resistant TB
MMR Measles, Mumps and Rubella
MRI Magnetic Resonance Imaging
MOU Memorandum Of Understanding
NHSE NHS England
NICE National Institute For Health and Care Excellence
NRPF No Recourse to Public Funds
NSS National Service Specification
NTBS National TB Surveillance System
PCR Polymerase Chain Reaction
RCN Royal College of Nursing
SASH Surrey and Sussex Healthcare NHS Trust
TB Tuberculosis
UCLH University College London Hospitals NHS Foundation Trust
UKHSA UK Health Security Agency
VOT Video Observed Therapy
WHO World Health Organisation
YOI Young Offender Institution
References
[1] World Health Organisation, “Tuberculosis.” Accessed: Dec. 10, 2024. [Online]. Available: Tuberculosis
[2] UK Health Security Agency, “National quarterly report of tuberculosis in England: quarter 3, 2024, provisional data,” Oct. 2024. Accessed: Dec. 02, 2024. [Online]. Available: National quarterly report of tuberculosis in England: quarter 3, 2024, provisional data – GOV.UK
[3] UK Health Security Agency, “Tuberculosis incidence and epidemiology, England, 2023,” Dec. 2024.
[4] UK Health Security Agency, “Tuberculosis in England, 2023 report (data up to end of 2022),” Feb. 2024.
[5] Public Health England, “Collaborative TB Strategy for England, 2015 to 2020: End of programme report,” 2021, Accessed: Dec. 16, 2024. [Online]. Available: Collaborative TB Strategy for England, 2015 to 2020: end of programme report
[6] NHS England and UK Health Security Agency, “Tuberculosis (TB): action plan for England, 2021 to 2026,” Mar. 2023, Accessed: Dec. 16, 2024. [Online]. Available: Tuberculosis (TB): action plan for England, 2021 to 2026 – GOV.UK
[7] National Institute for Health and Care Excellence, “Tuberculosis: NICE guideline NG33.” Accessed: Dec. 06, 2024. [Online]. Available: Overview | Tuberculosis | Guidance | NICE
[8] Royal College of Nursing, “A Case Management Tool for TB Prevention, Care and Control in the UK,” May 2023, Accessed: Dec. 10, 2024. [Online]. Available through subscription.
[9] UK Health Security Agency, “Green Book Chapter 32: Tuberculosis.” Accessed: Dec. 10, 2024. [Online]. Available: Greenbook chapter 32 – tuberculosis
[10] Public Health England, “Tuberculosis Health Needs Assessment Surrey and Sussex 2016/17,” Jun. 2017. Accessed: Dec. 10, 2024. [Online]. Available: Tuberculosis Health Needs Assessment
[11] Surrey County Council, “The Surrey Context: People and Place,” 2024. The Surrey Context: People and Place | Surrey-i
[12] Surrey-i, “Estimates of Country of Birth, Nationality, and Migration from the 2021 Census.” Accessed: Oct. 25, 2024. [Online]. Available: Census 2021: Country of Birth, Nationality, and Migration | Surrey-i
[13] UK Health Security Agency, “Tuberculosis by country: rates per 100,000 people.”
[14] Surrey-i, “Ethnic Group from the 2021 Census.” Accessed: Oct. 25, 2024. [Online]. Available: Census 2021: Ethnic Group | Surrey-i
[15] Surrey-i, “Gypsy, Roma, and Traveller populations in Surrey.” Accessed: Oct. 25, 2024. [Online]. Available: Gypsy, Roma, and Traveller populations in Surrey | Surrey-i
[16] Home Office, “Regional and local authority data on immigration groups,” Aug. 2024. Accessed: Oct. 25, 2024. [Online]. Available: Regional and local authority data on immigration groups – GOV.UK
[17] Surrey County Council, “Substance Misuse Joint Strategic Needs Assessment,” Apr. 2024, Accessed: Oct. 25, 2024. [Online]. Available: JSNA Substance Misuse | Surrey-i
[18] Surrey County Council, “JSNA Housing and Related Support,” Jan. 2024, Accessed: Oct. 25, 2024. [Online]. Available: JSNA Housing and Related Support | Surrey-i
[19] Surrey County Council, “HNA Prisons.” Accessed: Oct. 25, 2024. [Online]. Available: HNA Prisons | Surrey-i
[20] Ministry of Justice, “Prison population: monthly prison figures 2024,” Oct. 2024. Accessed: Oct. 25, 2024. [Online]. Available: Prison population: monthly prison figures 2024 – GOV.UK
[21] NHS Digital, “General Practice Workforce, 31 October 2024,” Nov. 2024. Accessed: Nov. 28, 2024. [Online]. Available: General Practice Workforce, 31 October 2024 – NHS England Digital
[22] Office for Health Improvement and Disparities, “Tuberculosis (TB): migrant health guide.” Accessed: Jan. 10, 2025. [Online]. Available: Tuberculosis (TB): migrant health guide – GOV.UK
[23] W. G. Dixon et al., “Drug-specific risk of tuberculosis in patients with rheumatoid arthritis treated with anti-TNF therapy: Results from the British Society for Rheumatology Biologics Register (BSRBR),” Ann Rheum Dis, vol. 69, no. 3, pp. 522–528, Mar. 2010, doi: 10.1136/ard.2009.118935.
[24] UK Health Security Agency, “Quarterly vaccination coverage statistics for children aged up to 5 years in the UK (COVER programme): April to June 2024.” Accessed: Dec. 06, 2024. [Online]. Available: Quarterly vaccination coverage statistics for children aged up to 5 years in the UK (COVER programme): April to June 2024 – GOV.UK
[25] NHS England, “Inclusion health groups.” Accessed: Dec. 04, 2024. [Online]. Available: NHS England » Inclusion health groups
[26] Independent Chief Inspector of Borders and Immigration, “An inspection of the initial processing of migrants arriving via small boats at Tug Haven and Western Jet Foi,” Jul. 2022. Accessed: Dec. 10, 2024. [Online]. Available: An inspection of the initial processing of migrants arriving via small boats at Tug Haven and Western Jet Foil
[27] Surrey County Council, “Migrant Health: Rapid Needs Assessment,” May 2023. Migrant Health | Surrey-i
[28] Office for Health Improvement and Disparities, “Assessing new patients from overseas: migrant health guide.” Accessed: Dec. 10, 2024. [Online]. Available: Assessing new patients from overseas: migrant health guide – GOV.UK
[29] Office for Health Improvement and Disparities, “Migrant health guide: countries A to Z.” Accessed: Dec. 10, 2024. [Online]. Available: Migrant health guide: countries A to Z – GOV.UK
[30] BBC News, “Home Office to give refugees more time to find housing,” Dec. 05, 2024. Accessed: Dec. 16, 2024. [Online]. Available: Home Office doubles time given to refugees to find accommodation – BBC News
[31] Surrey County Council, “Annual Public Health Report 2024: The Health Needs of Vulnerable Migrants in Surrey,” 2024, Accessed: Jan. 13, 2025. [Online]. Available: The Health Needs of Vulnerable Migrants in Surrey: Annual Public Health Report 2024 | Surrey-i
[32] Home Office, “Public Funds: Migrant access to public funds, including social housing and homelessness assistance and social care,” Oct. 2023. Accessed: Dec. 16, 2024. [Online]. Available: Public funds
[33] No Recourse To Public Funds Network, “Assessing and supporting adults with no recourse to public funds: Practice guidance for local authorities in England,” Mar. 2023. Accessed: Dec. 16, 2024. [Online]. Available: Assessing and supporting adults with no recourse to public funds (NRPF)
[34] Public Health England, “Managing tuberculosis (TB) in prisons,” May 2013, Accessed: Jan. 13, 2025. [Online]. Available: Managing tuberculosis (TB) in prisons – GOV.UK
Key Contacts
Lead author: Dr. Tom Irving, Specialty Registrar in Public Health
Please direct any feedback or queries to: [email protected]