JSNA Multiple Disadvantage
Multiple Disadvantage Joint Strategic Needs Assessment
Publication date
This chapter was published in October 2024.
Contents
- Acknowledgements
- Foreword
- 1. Aims and methods
- 2. Level of need
- 3. Risk factors
- 4. National and local policies and best practice
- 5. Accessing support
- 6. Primary research and literature review findings
- 6.1. ‘Ways of working’: avoiding silos and fragmented care
- 6.2. ‘Feeling abandoned’: identifying gaps in service provision
- 6.3. ‘Misheard and misunderstood’: understanding multiple disadvantage and its link with trauma
- 6.4. ‘One size doesn’t fit all’: service design for people experiencing multiple disadvantage
- 6.5. ‘Overcoming hurdles’: barriers preventing people from accessing services
- 6.6. ‘Under pressure’: strategic challenges create disruption and discord
- 7. Conclusions and recommendations
- References
- Appendices
Acknowledgements
Lived Experience Recovery Organisation: Eleanor, Steve, Jaana, Tommy, Colin, Jack, Jennifer, Elaine, Lisa, and Keri.
Multiple Disadvantage JSNA Chapter Delivery Group:
- Lead Author: Ella Turner, Programme Manager – Health Determinants Research Collaborative, Public Health & Communities, Surrey County Council (SCC).
- Supervisor: Lisa Byrne, Changing Futures Programme Delivery Manager, Public Health & Communities, SCC.
- Lived Experience Lead: James Poole, Changing Futures Project Manager, Public Health & Communities, SCC.
- Project Manager: Rebecca Matthews, JSNA Programme Manager, Public Health & Communities, SCC.
- Data Analyst: Lynne Sawyer, Public Health Analyst, Public Health & Communities, SCC.
- Data Analyst: Tyla Bailey, Business Support Officer, Public Health & Communities, SCC.
Contributing authors:
- Prof. Raja Mukherjee MBE, Consultant Psychiatrist, Clinical Lead Adult Neurodevelopmental disorders (NDD) & Foetal Alcohol Spectrum Disorder (FASD), Chief Clinical Information Officer – People with Learning Disability (CCIO PLD), Foetal Alcohol Spectrum Disorder Service, Surrey and Borders Partnership NHS Foundation Trust (SaBP).
- Dr Jo Jennison, Consultant Clinical Psychologist Trauma-informed care (TIC) Lead Multiple Disadvantage, Surrey and Borders Partnership NHS Foundation Trust.
- Lisa Byrne, Changing Futures Programme Delivery Manager, Public Health & Communities, SCC.
- Rebecca Matthews, JSNA Programme Manager, Public Health & Communities, SCC.
- James Poole, Changing Futures Project Manager, Public Health & Communities, SCC.
With special thanks to our sponsor: Vicky Stobbart, Director of Long Term Planning Delivery, Surrey Heartlands Integrated Care System (ICS).
Foreword
The experience of multiple disadvantage is a reality for far too many people. It is estimated that approximately 336,000 adults in England are experiencing multiple disadvantage, with at least 3,000 of these individuals living in Surrey. For many of them, their current circumstances are shaped by long-term experiences of poverty, trauma, abuse, and neglect. Multiple disadvantage also puts them at an increased risk of chronic and premature mortality and morbidity, poorer physical and mental health, higher social care needs, and a poorer life expectancy.
Multiple disadvantage – where people face overlapping issues such as mental health needs, substance use, homelessness, domestic abuse, and contact with the criminal justice system – requires a progressive and integrated system response.
It is with a profound sense of responsibility and commitment that we present Surrey’s first Joint Strategic Needs Assessment (JSNA) chapter on multiple disadvantage. This JSNA represents a comprehensive effort to understand the breadth and depth of the challenges faced by those affected by multiple disadvantage in Surrey. It is the result of extensive stakeholder engagement, data analysis, and collaboration across sectors. By bringing together insights from health, social care, housing, criminal justice, and the voluntary and community sector, we aim to provide a detailed picture of the needs and gaps in service provision for this vulnerable population.
Our findings highlight the urgent need for coordinated and sustained action. The complexity of multiple disadvantage means that no single organisation can address these issues in isolation, instead, we must work effectively as a ‘whole system’. By working together, we can ensure that the needs of those experiencing multiple disadvantage are met with dignity, respect, and comprehensive support.
Effective intervention requires a partnership approach, one that is responsive to the interconnected nature of multiple disadvantage challenges and focuses on providing relational, and person-centred solutions. We must strive to break down silos in areas where they still exist, continue to foster collaboration, and ensure that our efforts carry on being driven by compassion, understanding, and a commitment to making a real difference to our residents.
As we move forward, we are committed to using the insights from this JSNA to inform our future strategic planning, decision-making, and resource allocation. We are ambitious that this document will serve as a lever for change as well as a foundational tool for shaping our strategies and interventions, ensuring that they continue to be evidence-based and targeted to where they are most needed.
Our deepest gratitude goes to our Lived Experience Recovery Organisation, whose members have put heart and soul into delivering this chapter. Without their invaluable expertise, insight, and commitment, producing this JSNA would not have been possible. We extend our gratitude to all the partners, stakeholders, and individuals who contributed to this JSNA. Your involvement demonstrates a system-wide dedication, and your expertise and knowledge have been instrumental.
This JSNA is not an endpoint but a beginning, a call to action for all of us. Let us seize this opportunity to work collaboratively towards a brighter, more equitable future for all, one where ‘no one is left behind’.
Vicky Stobbart
Chapter Sponsor
Director of Long Term Planning Delivery
Surrey Heartlands ICS
James Poole
Lived Experience Project Manager
Surrey County Council
1. Aims and methods
1.1. What is the JSNA?
A Joint Strategic Needs Assessment (JSNA) is a statutory document that measures and improves understanding of the current and future health and social care needs of a population group. It supports local leaders and commissioners to make informed decisions and to shape services in a way that best serves their communities.
This is the first time in Surrey that a JSNA chapter focusing on multiple disadvantage has been produced, and this is one of the few multiple disadvantage JSNA chapters in the country. This JSNA chapter will be published in two phases:
- Phase 1: Adults experiencing multiple disadvantage (this document).
- Phase 2: Children, Young People, and Families experiencing multiple disadvantage.
Multiple disadvantage has clear links to Surrey’s whole system Health and Wellbeing Strategy (HWBS) and applies across its priority populations, strategic priorities, and system capabilities. Elements of multiple disadvantage are identified under the HWBS narrative outcomes and specifically the outcome: ‘The needs of those experiencing multiple disadvantage are met’. [1]
1.2 Aims
The primary objective of this JSNA chapter is to serve as a tool to help key decision-makers and commissioners across Surrey to better understand the needs of people experiencing multiple disadvantage. This chapter provides an evidence-base for partners to make informed-decisions and take action to improve the lives of this population group.
The JSNA also sets out to achieve the following:
- To identify the current and future health, care, and wellbeing needs of people experiencing multiple disadvantage in Surrey.
- To highlight the current response to health needs across the system and identify gaps and unmet needs.
- To explore system and service-level challenges, as well as barriers to accessing support.
- To consider suggestions regarding potential improvements and changes that could take place to improve care, support, and health outcomes.
- To identify commissioning priorities and recommend priority actions specific to the needs of this cohort.
1.3 Co-production of the JSNA
It is important that the voices of people with lived experience are included in a JSNA. This JSNA chapter has therefore been co-produced with a group of experts by experience that make up Surrey’s Changing Futures Lived Experience Recovery Organisation (LERO). Some members of the Surrey LERO also form part of the National Expert Citizens Group (NECG), which is a group of people from across England that harnesses the power of lived experience to tackle multiple disadvantage. Co-producing the chapter with the LERO has helped to ensure that people with lived and living experience of multiple disadvantage have been involved at each stage of the chapter writing journey (from design to delivery), and that their voices have led the chapter structure and content.
The Surrey LERO was set up in early 2023, with the group meeting with the JSNA Chapter Delivery Group an average of 2-3 times per month through a combination of online and in-person meetings. The JSNA chapter’s governance process also includes the Multi-Agency Group: Tackling Multiple Disadvantage and the JSNA Oversight Group. For a summary of the JSNA Chapter Delivery Group including individual roles and responsibilities, please see Appendix 1.
Co-production means working on an equal basis with people who have relevant experience of the topic being researched (in this case, multiple disadvantage). Co-production applies to all stages of the JSNA chapter writing process, from designing the chapter scope, to conducting primary research, and analysing and disseminating findings. The co-production of this chapter with people who have lived experience of multiple disadvantage adheres to HWBS principles for working with communities. This includes delivering more collaborative and creative work together with the lived experience community. [1] Co-producing the JSNA also aligns with Surrey Heartlands Integrated Care Strategy which sets out priorities for working as a partnership and alongside local people and communities to enable positive health and care for residents of Surrey. [1]
At the start of the chapter delivery process, we delivered a research skills training session to experts by experience. This session covered the purpose of research, different methods for conducting research (e.g., qualitative and quantitative), interview types and techniques, how to prepare for an interview and interview role play. Experts by experience were then supported to lead some of the in-depth interviews with stakeholders. They were able to probe and challenge discussion points where necessary. To view the log of co-production work with experts by experience, including dates of sessions and topics of discussion, please see Appendix 2.
The chapter has benefitted greatly by experts by experience sharing their knowledge, and authentic and valid insights into the real-world impact of multiple disadvantage. Collectively, the LERO has demonstrated their passion towards improving understanding of multiple disadvantage and reducing health inequalities for this population. This passion and dedication are evidenced at a group level through the collaborative delivery of this JSNA chapter, and also on a personal level too, with some members of the Chapter Delivery Group carrying out Naloxone training, championing peer research, and participating in national discussions around multiple disadvantage and lived experience involvement. Some of the LERO members reflected on their participation:
“This is the best engagement that I’ve experienced because it follows a value system, it’s hopeful and encouraging, there is an underlying belief that if you give quality attention and time to people, that will pay off and have an overall benefit to the community. It’s worth doing and it’s worth doing it well. It’s so evident that this group here does that.” (Interview LERO, expert by experience)
“It restores that faith, hope and belief that I can break away from this life, this stigma, this box that I’ve been put in.” (Interview LERO, expert by experience)
Achieving ‘genuine’ co-production takes time and dedication from all involved and often requires working in new and creative ways that best suit the individual needs of people in the co-production group. It is hoped that this way of working will continue in Surrey.
1.4 Methodology
This assessment adopted a mixed-methods approach, using a combination of desk analysis, in-depth interviews, focus group discussions and qualitative and quantitative surveying. Combining both qualitative and quantitative research approaches allows for a deeper exploration of attitudes and experiences, and it provides richer insights into the context and complexity of multiple disadvantage. The data collection took place throughout May 2023 – March 2024.
Our approach consisted of:
- Literature review:
- A literature review of relevant national and local reports, policies, guidance and evaluations on multiple disadvantage and related factors.
- Secondary data analysis:
- Collation and interpretation of relevant quantitative data from service providers and organisations across Surrey.
- Primary research:
- A total of 86 in-depth interviews with key stakeholders either working to support people experiencing multiple disadvantage or working to address one of the multiple disadvantage core risk factors in Surrey.
- A series of seven focus group discussions with 36 frontline staff.
- An in-person qualitative survey with 29 service users with living experience of multiple disadvantage. Surveying was carried out at outreach provider settings such as peer support groups, SMART meetings, and recovery cafes.
- An online survey with 100 Surrey-based organisations whose services are accessed by people experiencing multiple disadvantage.
- A total of five in-depth interviews with members of the LERO.
The design, conduct, analysis, interpretation and dissemination of insights from each of the three research strands (literature review, secondary data analysis and primary research) were co-produced through regular sessions between the JSNA Chapter Delivery Group and the Changing Futures LERO. This included delivering a research skills training session for experts by experience to become peer researchers.
Results across all research strands were triangulated through iterative discussion within the JSNA Chapter Delivery Group and LERO to inform the chapter conclusions and recommendations. Sections 2, 3 and 4 of this report were informed by literature review and secondary-data analysis. Section 5 is informed by the literature review. Section 6 reports primary research findings and supported by a literature review. Results from all three research strands are triangulated to inform chapter conclusions and recommendations in Section 7. For the full summary of the methodology including what data sources were used as the supporting evidence base for each section of the report, please see Appendix 3.
Any direct quotes used through this chapter are presented anonymously using the following codes followed by their unique number:
| Code | Descriptor | Explanation |
|---|---|---|
| IP | Interview participant | Service providers or individuals at organisations working to support people experiencing multiple disadvantage or one of the multiple disadvantage core risk factors in Surrey. |
| FG | Focus group participant | Frontline providers or outreach workers working to support people experiencing multiple disadvantage or one of the multiple disadvantage core risk factors in Surrey. |
| QS | Qualitative survey participant | Individuals with lived and/or living experience of multiple disadvantage, which includes both service users and people who are not currently engaged with statutory services. |
| OS | Online survey participant | Service providers or individuals at organisations working to support people experiencing multiple disadvantage or one of the multiple disadvantage core risk factors in Surrey. |
| LERO | Member of the Lived Experience Recovery Organisation | Expert by Experience that is a member of the LERO |
Where the broader term ‘research participant’ is used, this refers to any individual that took part in any primary research activities carried out for the purpose of this JSNA chapter, this includes in-depth interviews, focus groups, in-person surveys and online surveys. The term ‘research participant’ includes service providers, frontline staff, outreach staff, practitioners, health and care partners, system leaders, stakeholders working to support people experiencing multiple disadvantage or one of the multiple disadvantage core risk factors in Surrey. ‘Research participant’ also includes individuals with lived and/or living experience of multiple disadvantage, which includes both service users, and people who are not engaged with statutory services.
2. Level of need
The 2015 Hard Edges report on mapping severe and multiple disadvantage estimates that in England there are at least 58,000 people annually who have contact with homelessness, substance use and criminal justice services. [2] More recently, Changing Futures national programme estimated that approximately 336,000 adults in England face at least three of homelessness, mental health, substance use, contact with the criminal justice system, or domestic abuse. Many of these individuals have repeated contact with statutory and voluntary services over a number of years. [3]
Each individual risk factor of multiple disadvantage, such as homelessness, substance use, mental health, contact with the criminal justice system, and domestic abuse, puts an individual at risk of experiencing health inequalities. This risk is even greater for individuals affected by multiple disadvantage; an individual experiencing a combination of these factors has a summative effect which means the impact on health and wider determinants is even greater. The combination of challenges is further worsened by most services being set up to provide support for one individual need rather than effectively collaborating to offer a holistic approach.
It is difficult to accurately quantify the number of people in Surrey as a whole who are experiencing multiple disadvantage as this is not routinely recorded in health, social care, and other information systems. By looking at some key population datasets though we can begin to make some estimates. This section explores the local picture of multiple disadvantage in Surrey, including how multiple disadvantage is both defined and understood, and the current level of need.
2.1. What does the term multiple disadvantage mean?
In Surrey, work has been underway to support people experiencing multiple disadvantage since 2015, with the introduction of a High Impact Complex Drinkers service, and the Surrey Adults Matter Making Every Adult Matter (MEAM) approach in 2019. Most recently, the Changing Futures programme has introduced a specialist, trauma informed, relational model of support for people experiencing multiple disadvantage in Surrey.
Primary research identified that multiple disadvantage is described in different ways in different parts of the system, with professionals in diverse support and care settings using a range of terms to refer to what their organisation considers multiple disadvantage. Examples include service users experiencing ‘multiple needs’, ‘multiple unmet needs’, ‘multiple and complex needs’, ‘multiple and compound needs’, ‘co-occurring conditions’, ‘co-morbidities’, ‘dual diagnosis’, ‘entrenched rough sleepers’, ‘prolific offenders’, or ‘high support needs’ and those in inclusion health groups.
The varying labels and definitions that are used in different spaces often overlap and can lead to duplication and inefficiency. It is important for a system to operate with a shared understanding of what the term ‘multiple disadvantage’ means, and the cohort it should be used to describe. Achieving this consistency in terminology helps to support adults facing the sharpest health and social inequalities in an integrated, unified way.
The most used definition of multiple disadvantage is that set out by the Department of Levelling Up, Communities & Housing (DLUCH) when the Changing Futures programme funding was first announced. The Changing Futures programme defines multiple disadvantage as:
Adults experiencing three or more of the following five: homelessness, substance misuse, mental health issues, domestic abuse, and contact with the criminal justice system.
Surrey is one of the 15 local areas across England that has received funding to develop its own Changing Futures delivery model. Bridge the Gap is an alliance of third sector providers that have joined together to deliver the Changing Futures programme in Surrey. Bridge the Gap defines multiple disadvantage as: [4]
Someone who is dealing with three or more of the following:
- Contact with the criminal justice system.
- Mental health issues.
- Substance use (alcohol or drugs).
- Homelessness or at risk of becoming homeless.
- Domestic violence/ abuse.
Bridge the Gap also considers individuals with a physical health need and neurodevelopmental conditions.
Making Every Adult Matter (MEAM) is a unique coalition of four national charities that supports local areas across the country to transform services and systems, and to directly improve the lives of people facing multiple disadvantage. Multiple disadvantage awareness began in Surrey in 2018 when the decision was made to become a MEAM area, adopting the MEAM approach for clients experiencing multiple needs. MEAM defines multiple disadvantage as: [5]
People facing multiple disadvantage experience a combination of problems. For many, their current circumstances are shaped by long-term experiences of poverty, deprivation, trauma, abuse, and neglect. Many also face racism, sexism, and homophobia.
These structural inequalities intersect in different ways, manifesting in a combination of experiences including homelessness, substance misuse, domestic violence, contact with the criminal justice system and mental ill health.
2.1.1. Co-designed definition of multiple disadvantage
There are interchangeable ways of talking about, defining, and understanding multiple disadvantage that are relevant to the individual affected by multiple disadvantage and the local context, as well as the support system and system partners.
It is recognised that the term ‘multiple disadvantage’ is stigmatising. The term ‘disadvantage’ itself carries a negative connotation, implying that the person lacks certain advantages or opportunities compared to others. This can contribute to the perception of individuals as inherently less capable or worthy, reinforcing stereotypes and societal biases.
To support this JSNA chapter, we have discussed both preferred and appropriate phrasing and language with the LERO and a wider group of stakeholders working to support people experiencing multiple disadvantage in Surrey. For the purpose of this JSNA chapter, we primarily adopt the national Changing Futures programme definition of multiple disadvantage:
“Adults experiencing three or more of the following five: homelessness, substance use, mental health issues, domestic abuse, and contact with the criminal justice system.”
However, the LERO identified that using only this definition is an oversimplification that excludes many other people facing multiple disadvantage and could result in:
- Perpetuation of exclusion and triggering of trauma.
- Perpetuation of cycles of disadvantage.
- Lack of adjustment towards complex trauma and trauma informed care.
- Underestimation of true levels of multiple disadvantage.
- Short term gains followed by longer term retrenching of problems.
The LERO would like to emphasise that experiences of multiple disadvantage are relative to an individual’s personal journey. Many individuals may experience overlapping disadvantages that are often persistent, interrelated and affect a person’s life course, impair quality of life and wellbeing, and incur social costs without necessarily crossing the threshold into the types of severity addressed by the Changing Futures programme.
This chapter therefore expands upon the Changing Futures programme definition, acknowledging that an individual who is experiencing multiple disadvantage may be more severely affected by a combination of three or more of the following:
- Mental health conditions
- Substance use (alcohol or drugs)
- Homelessness or at risk of becoming homeless
- Domestic abuse
- Contact with the criminal justice system or prison leavers
- Neurodevelopmental conditions, learning disabilities or learning difficulties
- Physical health disabilities including chronic long-term conditions and impaired social function
- Poverty
- Trauma
- Adverse Childhood Experiences (ACEs)
- People with experience of state care (care leavers)
- Other addictions (e.g., gambling, eating disorders)
- Bereavement (the experience of losing someone important to you i.e., a close friend or family member)
- Social exclusion, isolation, or loneliness
- Financial problems (e.g., experiences of debt or financial abuse)
- People experiencing stigma, prejudice or discrimination based on minority.
The above multiple disadvantage challenges are often rooted in childhood trauma and Adverse Childhood Experiences (ACEs). They may also be linked to underlying social and systemic factors (e.g., policies, structural inequalities), which are typically outside the control of the individual experiencing them. [26]
2.2. Evidence of multiple disadvantage: literature review and secondary data analysis
Research suggests that 85% of people in England facing multiple disadvantage as adults experienced trauma as children. [2] For many, their current circumstances are shaped by long-term experiences of poverty, trauma, abuse, and neglect. Many also face racism, sexism, and homophobia. Multiple disadvantage is a systemic, not an individual issue. People experiencing multiple disadvantage are among the most vulnerable in our communities, however they continue to face barriers and challenges when accessing support services and are often failed by a system that is geared up to focus on singular factors.
In the absence of appropriate and suitable support, the challenges faced by those experiencing multiple disadvantage continue, and often worsen, with many becoming more entrenched. This makes it harder for individuals to address their problems, lead fulfilling lives and contribute fully to their communities. [5] Recent national research estimates that in England 63% of people experiencing homelessness are experiencing a long-term health issue, disability, or infirmity and 82% had a mental health diagnosis with 45% of people reporting that they are self-medicating with drugs or alcohol to help them cope with their mental health. [6]
This JSNA chapter used secondary data analysis to estimate that there are at least 3,000 adults in Surrey who are experiencing multiple disadvantage. Whilst the definition of multiple disadvantage for the purpose of this JSNA chapter is any individual experiencing a combination of three or more multiple disadvantage risk factors, in some instances estimates of multiple disadvantage have been calculated based on two of more challenges due to pragmatism related to type of data available. Where data captures only two challenges, these have been clearly stated.
In 2022/23, housing returns show that 3,367 people in Surrey were owed a homeless relief duty or support duty. Applying the above estimates to this overall figure suggests that a minimum of 2,760 people who are homeless or at risk of homelessness in Surrey are also experiencing multiple disadvantage if this is defined as two or more challenges (in this instance homelessness and mental health). As there will also be 2,125 people experiencing homelessness alongside other long term health issues and disabilities, even allowing for significant overlap between the two sets of figures, this 2,760 is likely to be an underestimate. Additionally, people will also be experiencing other disadvantages e.g. contact with the criminal justice system.
Over two-thirds of people starting treatment for drug or alcohol dependence (70% if looking just at alcohol dependence) said that they had a self-reported mental health need. [11] 2020/21 data reports that 2,134 Surrey residents were receiving treatment at specialist drug use service and 1,352 at specialist alcohol use services – we can estimate that over 2,370 of this cohort of residents would be experiencing mental health issues in addition to substance use, so experiencing multiple disadvantage. [7]
The Hard Edges report on mapping severe and multiple disadvantage recognises poverty as an almost universal, common, and complicated factor affecting people experiencing multiple disadvantage. The report indicates that poverty is a factor in difficult family relationships, poor educational experiences, and is part of the early roots of severe multiple disadvantage. The report includes a mapping exercise that suggests an association between multiple disadvantage prevalence rates and areas of the country where poverty tends to be concentrated. [2] The Indices of Deprivation are a unique measure of relative deprivation at a small local area level (Lower-layer Super Output Areas (LSOAs)) across England. As of July 2024, the Indices of Deprivation 2019 (IoD2019) is the most recent release. In Surrey, there are 21 Health and Well-Being Key Neighbourhoods; these areas were selected on the basis of the overall deprivation score established in the English Indices of Deprivation 2019.
Integrated Care Systems (ICS):
ICSs are partnerships of NHS bodies and local authorities, working with other relevant local organisations, that come together to plan and deliver health and care services to improve the lives of people in their area. A further explanation of Integrated Care Systems and how they function and what they mean for different parts of the system is available from the Kingsfund.
Place-based partnerships operate on a smaller footprint within an ICS. They include multi-agency partnerships involving the NHS, local authorities, the voluntary and community sector (VCSE) and local communities themselves. There are four place-based partnerships within Surrey Heartlands ICS and five within Frimley Health and Care ICS. All four of the place-based partnerships in Surrey Heartlands ICS (Surrey Heartlands place-based partnerships) sit within Surrey county boundaries. Three of the five place-based partnerships in Frimley health and care ICS (Frimley Health and Care communities map) overlap with Surrey county boundaries: Part of Windsor and Maidenhead (which covers Windsor PCN, on the edge of Runnymede and used to cover East Berkshire CCG), all of Surrey Heath (which covers Surrey Heath PCN, Surrey Heath borough council and a part of the West of Guildford borough council) and part of North East Hampshire and Farnham (Farnham PCN on the West of Waverley borough council).
For more information on the Surrey context, please see People and Place JSNA chapter.
Data of patients registered from Frimley Health and Care Integrated Care System (ICS):
Looking at the population of Frimley Integrated Care System, of 14,567 people experiencing mental health diagnoses, 1,254 (8.6%) also had substance use or alcohol issues, 73 (0.5%) were flagged as being homeless and 11 (0.1%) were prison leavers. In total, 1,338 (9.2%) had two or more of mental health issues, substance use or alcohol dependence syndrome, homelessness or being a prison leaver. [8]
Demographics of those experiencing a combination of mental health and substance use issues are:
- 83% identified as White
- 50.3% identified as male
- 29.5% were in the 50-59 age group, 19.7% were aged 40-49.
This data is not for the whole of Surrey, and it would be difficult to estimate a Surrey wide figure from this dataset, but this does help to support the estimates above
Secondary Users Services (SUS) data from Surrey Heartlands Integrated Care Board (ICB):
Surrey Heartlands ICB was able to provide Secondary User Services (SUS) activity data from 2019 to 2023 relating to the number of admissions where the patient was identified as having two or more issues relating to mental health, alcohol and drug related issues and domestic abuse. This was summarised at both Place and Primary Care Network (PCN) level. Place-based partnerships operate on a smaller footprint within an ICS. They include multi-agency partnerships involving the NHS, local authorities, the voluntary, community and social enterprise sector (VCSE) and local communities themselves.
Primary Care Networks (PCNs) bring together general practice and other primary care services, such as community pharmacy, to work at scale and provide a wider range of services at neighbourhood level. There are currently 25 PCNs in Surrey Heartlands, and four PCNs in Frimley which have patients in Surrey, more information on PCNs here.
Table 1 (below) based on data from 2019-2023 shows the average annual admissions for patients with two or more issues relating to mental health, alcohol, drug related issues and domestic abuse, per 100,000 registered population by ICS Place. Data may include people who were admitted more than once over the year.
Table 1: Average annual admissions where the patient was identified as having multiple disadvantage per 100,000 population.
| Place | Average Annual Admissions, 2019-2023 | Lowest PCN Value | Highest PCN Value |
|---|---|---|---|
| North West Surrey | 810.17 | 592.14 | 962.56 |
| Guildford and Waverley | 1024.99 | 705.02 | 1307.41 |
| Surrey Downs | 644.42 | 583.95 | 751.29 |
| East Surrey | 898.60 | 820.17 | 983.86 |
Table 2 (below) shows the total admissions from 2019-2023 for these patients by Place and a breakdown by age. Although the greater part (52%) were in the 18-64 age bracket, a large proportion (46%) were in the 64+ age bracket.
Table 2: Total admissions for patients identified as experiencing multiple disadvantage from 2019/20-2022/23.
| Place | 0-17 age group | 18-64 age group | 64+ age group | Total |
|---|---|---|---|---|
| North West Surrey | 149 | 4741 | 4563 | 9453 |
| Guildford and Waverley | 201 | 4236 | 2689 | 7126 |
| Surrey Downs | 141 | 2832 | 3145 | 6118 |
| East Surrey | 113 | 2694 | 2428 | 5235 |
Surrey’s Changing Futures Programme data:
The current Changing Futures Surrey dashboard has data for 71 people being supported via the Changing Futures programme (Bridge the Gap), and contains data gathered from May 2022 up until August 2023. The demographics of those receiving support are summarised on the dashboard, although it should be noted that information was not submitted for all those receiving support and/or information was suppressed due to small numbers:
- Age: 26% were between 30-39, 30% between 40-49, 21% between 50-59. Surrey has a slightly older age profile than clients being supported nationally as shown in Figure 3.
- Gender: 66% were male, 32% female. This is similar to the national figures of 62% male and 37% female.
- Ethnicity: 89% were reported as being White, compared to 87% nationally.
- Neurodiversity: 26% reported having ADHD, 28% a learning disability. These are higher than the national percentages of 14% reporting having ADHD and 12% reported as having a learning disability.
The figures below show the types of disadvantage experienced by those supported by Changing Futures in Surrey compared to the national picture. Figure 4 demonstrates that the types of disadvantage experienced by those being supported by Changing Futures in Surrey is very similar to the national picture. Almost all experienced mental health issues, with high proportions experiencing substance use and homelessness.
Figure 1: Percentage of Changing Futures clients in each age bracket (Source: Changing Futures dashboard)
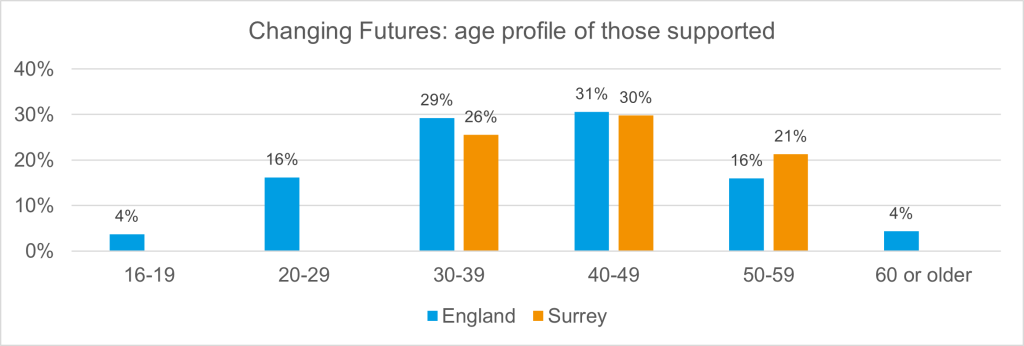
Figure 2: Percentage of Changing Futures clients experiencing each type of disadvantage (Source: Changing Futures dashboard)
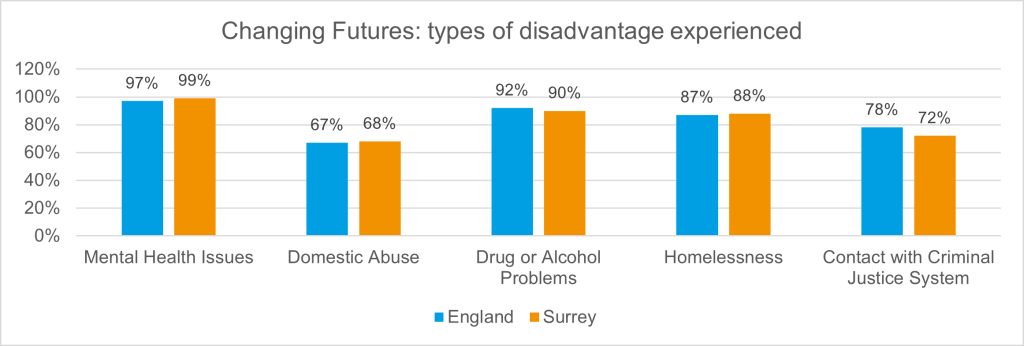
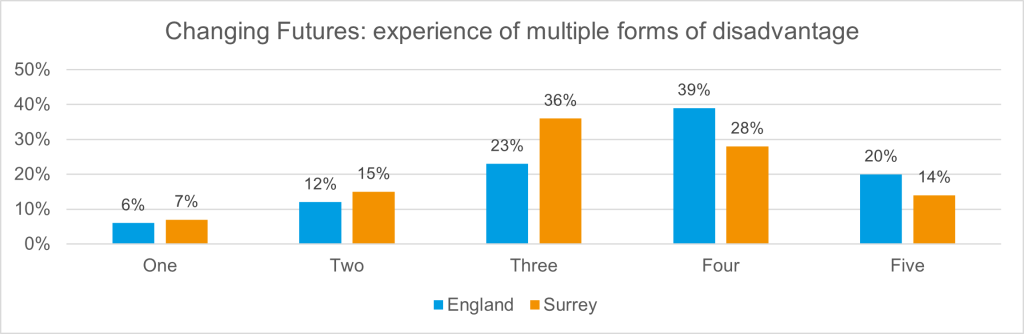
Figure 3 below shows a comparison of people being supported by the Changing Futures programme in Surrey and nationally who are experiencing four or five disadvantages. In Surrey, a lower percentage of individuals are experiencing multiple forms of disadvantage compared to national figures.
Figure 3: Percentage of Changing Futures clients experiencing multiple types of disadvantage (Source: Changing Futures dashboard)
Making Every Adult Matter (MEAM):
Cordis Bright, an external consultancy providing advice and research aimed at improving public services, were commissioned to carry out the national evaluation of the MEAM Approach. In October 2022, Cordis Bright produced a Local area Common Data Framework supplement focusing on Surrey. The supplement report includes analysis of information about people experiencing multiple disadvantage who have been supported by work developed using the MEAM approach in Surrey i.e., Surrey Adults Matter.
As of 31st March 2022, Surrey had supported 93 people with data being provided for 79 people. The average age was 42, but the age bracket with the most people was 31-35, with nearly a fifth of people falling into this age range at time of support starting. 61% of people identified as male, with the remaining 39% identifying as female. The greater majority, 99%, reported being heterosexual. 95% reported being British.
Surrey County Council’s Health Inequalities Task Group Report (Adults and Health Select Committee):
The Health Inequalities Task Group report (2023) was written to provide the Adults and Health Select Committee with a detailed report on the findings and recommendations of the Health Inequalities Task Group. This was set up to explore health inequalities/disadvantages amongst key priority population groups within Surrey.
This focused on three specific groups: firstly, individuals from minority ethnic backgrounds and Gypsy, Roma and Traveller (GRT) communities; secondly, individuals experiencing homelessness or drug and alcohol use; and thirdly, individuals experiencing domestic abuse. It was highlighted that these groups experienced more health inequalities relative to other groups. These groups were also included in the HWBS’s priority populations, and individuals in these groups were also likely to fall into several other priority population categories. This report highlighted a number of issues related to people experiencing multiple disadvantage:
- Those that are homeless often experience health needs that are highly complex with various physical health challenges and are also significantly more prone to developing mental health issues.
- Homeless people experiencing a mental health crisis often do not receive the required support and struggle to access services.
- Domestic abuse victims are likely to experience additional physical and mental health challenges and difficulties accessing healthcare.
3. Risk factors
This section presents the secondary data analysis and literature review of the five core risk factors relating to multiple disadvantage and nine additional locally identified risk factors.
3.1. Core risk factors
The ‘core risk factors’ are those identified in the Changing Futures programme definition of multiple disadvantage that have been adopted for the purpose of this JSNA chapter. This includes mental health, domestic abuse, substance use, homelessness, and contact with the criminal justice system.
3.1.1. Mental health
Mental health is both a cause and a consequence of multiple disadvantage. [9] In March 2023, Surrey County Council published a JSNA chapter on Emotional and Mental Wellbeing in Surrey Adults; this chapter includes detail on universal services, primary care, and secondary care for people with a mental health need. For more information, please see Emotional and Mental Wellbeing in Surrey Adults | Surrey-i (surreyi.gov.uk).
The most common entry point for mental health support is through primary care. Mind Matters Surrey is an NHS talking therapies service provided by Surrey and Borders Partnership NHS Foundation Trust. Talking therapies services are also known as Improving Access to Psychological Therapies (IAPT) services. In Surrey, 2021/22 there were 29,055 referrals to Improving Access to Psychological Therapies (IAPT) with 21,235 commencing treatment. In 2021/22, there were 34,977 referrals (either self-referrals or GP referrals) to IAPT, with 20,297 people completing treatment.
There are a range of patient/citizen facing digital services available to support mental wellbeing, which may be accessed in both a health and care setting, or in the home or another public place. This includes but is not limited to websites (such as Healthy Surrey), applications (including the national NHS app itself), online forums (such as those supporting children and young people), remote monitoring technologies (such as assisting those with dementia) and clinical services (such as an online IAPT offer).
Adult Social Care Mental Health Team:
Although not specifically related to people experiencing multiple disadvantage, an analysis of the characteristics of individuals supported by Adult Social Care (ASC) services in Surrey provides some insight into this group. As of October 2023, Adult Social Care have approximately 3,250 open cases where the individual has a Primary Client Category (PCC) of Adults Mental Health. The percentage of people with a PCC of Adults Mental Health with a primary or secondary support reason of ‘learning disability support’ and ‘physical and sensory support’ is 3%, and 11%, respectively. Additionally, approximately 5% of this cohort, people open to ASC with a PCC of Mental Health live in a LSOA with an Index of Multiple Deprivation (IMD 2019) ranking of 1-3, so could be categorised as living in the most deprived areas. [10]
The IMD has 10 deciles, 1 – 10, with 1 = 10% most deprived LSOAs in England. Surrey has no LSOAs with a decile of 1, four with a decile of 2, 15 with a decile of 3 and 41 with a decile of 4. Although Surrey has no LSOAs in decile 1, some people live out of county in a LSOA in decile 1. Table 3 (below) shows the breakdown of cases open to ASC who are aged 18 or over with a PCC of Mental Health by district and borough in Surrey. Some districts and boroughs have notably higher percentages in the lower deciles for deprivation, indicating a higher proportion experiencing multiple disadvantage, in particular Reigate and Banstead, Runnymede and Spelthorne.
Table 3: Cases Open ASC who are aged 18 or over with a PCC of Mental Health by D&B and IMD
| District and Borough | IMD 2019 decile 1 | IMD 2019 decile 2 | IMD 2019 decile 3 | IMD 2019 decile 4 | IMD 2019 decile 5 | IMD 2019 decile 6 | IMD 2019 decile 7 | IMD 2019 decile 8 | IMD 2019 decile 9 | IMD 2019 decile 10 | Not found |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Elmbridge | 0% | 0% | 2.0% | 9.1% | 1.7% | 9.5% | 6.1% | 13.2% | 19.6% | 38.9% | 0% |
| Epsom and Ewell | 0% | 0% | 5.0% | 12.6% | 0% | 9.9% | 14.3% | 14.3% | 18.7% | 25.3% | 0% |
| Guildford | 0% | 2.3% | 1.3% | 2.6% | 14.2% | 10.8% | 19.3% | 9.8% | 11.3% | 28.4% | 0% |
| Mole Valley | 0% | 0% | 3.1% | 4.9% | 5.8% | 10.2% | 13.7% | 19.9% | 22.6% | 19.9% | 0% |
| Reigate and Banstead | 0% | 3.6% | 5.2% | 11.0% | 9.0% | 13.5% | 16.0% | 11.0% | 13.0% | 17.8% | 0% |
| Runnymede | 0% | 0% | 7.1% | 10.7% | 19.9% | 12.8% | 17.9% | 14.3% | 12.8% | 4.6% | 0% |
| Spelthorne | 0% | 0% | 6.8% | 22.1% | 9.4% | 27.7% | 9.4% | 14.0% | 7.7% | 3.0% | 0% |
| Surrey Heath | 0% | 0% | 0% | 12.9% | 9.6% | 11.0% | 2.4% | 10.5% | 30.1% | 23.4% | 0% |
| Tandridge | 0% | 0% | 0% | 9.8% | 6.3% | 11.2% | 24.5% | 30.1% | 9.8% | 8.4% | 0% |
| Waverley | 0% | 0% | 3.6% | 2.3% | 1.7% | 7.9% | 11.2% | 19.1% | 26.4% | 27.7% | 0% |
| Woking | 0% | 1.5% | 3.6% | 10.5% | 19.0% | 0% | 14.8% | 9.9% | 25.3% | 15.4% | 0% |
| Out of county | 5.0% | 4.6% | 10.3% | 13.6% | 6.6% | 10.7% | 10.7% | 11.6% | 13.2% | 11.6% | 2.07% |
| Unknown | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 100% |
| Grand Total | 0.4% | 1.3% | 4.0% | 9.5% | 8.8% | 10.8% | 13.2% | 13.6% | 17.3% | 19.6% | 1.7% |
The information provided above indicates that of those people supported by ASC with an ASC PCC of Adults Mental Health, at least 11% or 357 people could be categorised as experiencing multiple disadvantage. Approximately 50% of people supported by ASC, with an ASC PCC of Adults Mental Health, who could be categorised as experiencing multiple disadvantage, were male, and 50% were female. Drilling down on Secondary Support Reasons shows:
- A slightly higher proportion of people with an ASC PCC of Mental Health, with a primary/secondary support reason of Learning Disability are male than female.
- A higher proportion of people with a secondary support reason of Physical and Sensory are female (approximately two thirds) than male (one third).
Looking at the ethnicity of this cohort, the approximate breakdown is 75% White, followed by 4% Asian / Asian British, with 15% not known. Other ethnic groups accounted for around 6% of this cohort. The percentage of people belonging to each ethnic group is lower in the cohort of people support by ASC with an ASC PCC of Adults Mental Health than in Surrey’s general population. These differences may be as a result of the higher proportion of people of ‘not known’ ethnicity in the ASC PCC Adults Mental Health cohort compared to the Surrey general population. The exception to this pattern is that a slightly proportion of people in the ASC PCC Adults mental Health cohort are of Black ethnicity (3%) compared to the Surrey general population (2%).
Surrey County Council’s Adult Social Care team shared information on people they have open to ASC who may be experiencing multiple disadvantage. Over 10% of people open to ASC and with a Primary Care Category (PCC) of mental health are also experiencing other disadvantages and challenges, with older people more likely to have physical disability issues and younger people in this cohort more likely to have learning disabilities.
An analysis of the age of people open to ASC with a PCC of Adults Mental Health shows that the peak age range is between 50 to 59 (20%). This is a similar pattern to the age range distribution for Surrey’s general population. Drilling down on ASC Primary/ Secondary Support Reasons shows:
- For ASC Physical and Sensory Support, the peak age range increases to 80-89 with 25%. A higher proportion of people are in the 80-89 age range in this cohort than the Surrey population.
- For ASC Learning Disability Support, the age range decreases to 20-29 also with 25%. A higher proportion of people are in the 20-29 age range in this cohort than the Surrey population.
For this cohort, an analysis of their religion is likely to be skewed with the high number of unknowns at over 50%. The religion with the highest percentage is Christian (approx. 25%), None (approx. 10%) and Other Religions (approx. 2%).
Local provider data – Example: Oakleaf:
Oakleaf, a charity based in Guildford that works with the local community to manage mental health needs, shared data for the purpose of this JSNA chapter as an example of the clients that voluntary and community sector organisations serve locally. Oakleaf is also one of the Voluntary Community & Social Enterprises (VCSEs) that makes up the Bridge the Gap Alliance of outreach providers.
A snapshot of their 552 clients as of September 2023 showed that:
- 92 (16.7%) of clients also had a physical disability.
- 86 (15.6%) of clients also had learning disabilities, learning disabilities or neurodivergence.
- 83 (15.0%) had substance use or alcohol use issues.
- 39 (7.1%) had had contact with the criminal justice system.
Demographic data for clients of Oakleaf was only available for the whole client group, rather than just for those clients experiencing multiple challenges, but shows that the majority of clients were aged between 30 and 60 (n=361). Females were the largest gender group attending the service with 286 (51.8%) being female. The majority of service users (n=388; 70.3%) were White British.
3.1.2. Domestic abuse
Surrey County Council’s Domestic Abuse Needs Assessment:
Between April 2021 and September 2022, 17% of those accessing domestic abuse outreach services disclosed a disability, of which mental health disability was the most common with 8.8% of those accessing these services reporting that they had a mental health disability. The proportion with a disability was higher than that seen in the population overall as the 2021 census reported that only 13.8% of residents in Surrey had a disability. For hospital Independent Domestic Violence Advisors (IDVAs) in Surrey the figure is higher still, with 46.4% of those accessing the service reporting a disability (28.3% for mental health disabilities).
Data for the hospital IDVAs also shows the overlap between those accessing domestic abuse services and with substance use needs, with 15% accessing the IDVAs between October 2021 and September 2022 disclosing an alcohol support need and 5% a drug support need.
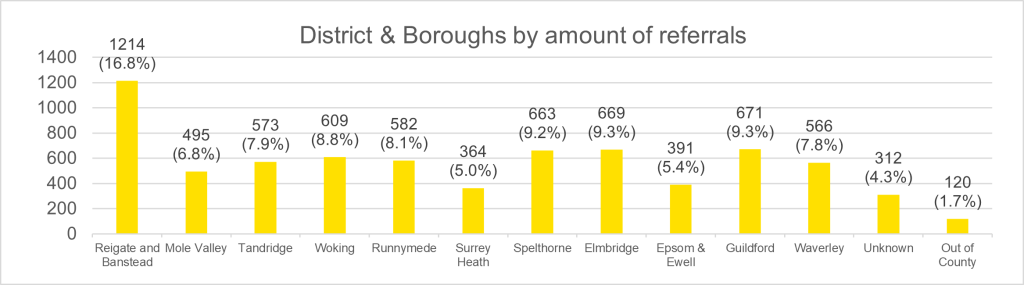
Referrals to domestic abuse services vary greatly across the eleven district and boroughs in Surrey (see Figure 4), with Reigate and Banstead receiving 17% of all referrals.
Figure 4: District & Boroughs by amount of referrals from 1st April 2021 to 30th September 2022
Multi-Agency Risk Assessment Conference (MARAC):
MARACs are meetings where information is shared on individuals who are at the highest risk of domestic abuse. The information below relates to the whole of Surrey. MARAC representatives include local police, health, child protection, adult social care, housing practitioners, IDVAs, probation and other specialists from the statutory and VCSE sectors.
Referral routes into MARAC for Surrey as a whole (Table 4) demonstrate the complexity of this population group and that many are using / in touch with other services and are probably therefore experiencing multiple disadvantage:
Table 4: Referral routes, 2018/2019 to 2022/2023 (Source: Marac, 2020/2021 – 2022/2023)
| Referral Routes | 2022/2023 | 2021/2022 | 2020/2021 | 2019/2020 | 2018/2019 |
|---|---|---|---|---|---|
| Police | 64.7% | 89.8% | 85.2% | 82.8% | 77.8% |
| Independent Domestic Violence Advisor (IDVA) | 10.4% | 3.0% | 2.4% | 3.8% | 4.0% |
| Probation | 7.9% | 2.3% | 4.6% | 4.7% | 5.5% |
| Adult Social Care Services | 3.0% | 0.9% | 2.7% | 1.7% | 0.7% |
| Children’s Social Care Services | 3.0% | 1.1% | 2.4% | 2.7% | 3.9% |
| Housing | 1.6% | 0.2% | 0.4% | 0.7% | 0.9% |
| Secondary Care/ Acute trust Services | 1.4% | 0.5% | 1.5% | 1.8% | 0.4% |
| Primary Care Services | 0.9% | 0.3% | 0.2% | 0.1% | 0.4% |
| Substance Use Services | 0.2% | 0.1% | 0.0% | 0.5% | 0.0% |
| Voluntary Sector | 0.2% | 0.7% | 0.2% | 0.2% | 1.0% |
| Mental Health Services | 0.0% | 0.3% | 0.4% | 0.3% | 0.6% |
| Other | 6.3% | 0.7% | 0.0% | 0.8% | 4.9% |
The number of cases discussed at MARAC have increased annually from 2018/2019 to 2022/2023. The police referral route made the most cases (64.7% in April 2022 to March 2023), and this is a decrease of 28.0% in the last 12 months compared to the previous 12 months, April 2021 to March 2022 (89.9%).
IDVAs have increased the number of referrals in the last 12 months by 246.6%: IDVAs referred 165 (10.4%) cases to MARAC in April 2022 to March 2023 compared to April 2021 to March 2022, where they referred 45 (3.0%).
The proportion of cases which involved victims with a recorded disability in April 2022 to March 2023 was less than 1%. The proportion of referrals where the victim is Black/Asian or racially minoritised shows a drop in the number of referrals recorded during 2019/2020 to 2021/2022. This is not an indication of no referrals of Black/Asian victims or racially minoritised cases referred to MARAC, but that these figures were not captured during this time period. The proportion of Black/Asian or racially minoritised cases from April 2022 to March 2023 was 19.5%, higher than the national population rate 17.9%.
Although there is no formal obligation for MARACs to exist in every area as they are not a statutory provision, it is estimated they do save money by supporting the most complex of domestic abuse cases.
East Surrey Domestic Abuse Services (ESDAS) outreach monitoring:
Outreach monitoring reports provided by East Surrey Domestic Abuse Services show that 5,205 clients in total were seen from 2023/24, of whom 1,522 (29%) had additional vulnerabilities so could be described as experiencing multiple disadvantage. Out of all referrals received during this period:
- 46% were police referrals.
- 18% were high risk cases heard at the Multi-Agency Risk Assessment Conference (MARAC).
The service reported an increasing trend in people experiencing multiple disadvantage. Looking at additional disadvantages as a proportion of total clients seen shows that:
- 891 (59%) also had a mental health support need.
- 226 (15%) also had a physical health support need.
- 168 (11%) also had an alcohol support need.
- 105 (7%) also had a drug support need.
- 38 (2%) also had an offending support need.
- 17 (1%) were also carers.
3.1.3. Substance use
In April 2024, Surrey County Council published a JSNA chapter on Substance Misuse, for more information, please see JSNA Substance Misuse | Surrey-i (surreyi.gov.uk).
The ASC data (quoted above in the mental health section) can also be used to provide insights into those people facing multiple disadvantage and experiencing substance use as at October 2023. ASC currently have approximately 170 open cases supported by the ASC Substance Use team. When drilling down on ASC Primary/ Secondary Support Reasons this shows ‘Mental Health Support’ at 11% and then Physical and Sensory Support at 5%. Approximately 8% of the people supported by the ASC Substance Use team live in a LSOA with an IMD ranking of 1-3.
The approximate breakdown of demographics in this ASC cohort are:
- Gender: males, 55%; females 45%.
- Ethnicity: Approximately 70% White, with 25% not known.
- Age: 92% are aged between 30 and 69 and the age range with the highest percentage is 40-49 at approximately 30%.
Local Alcohol Profiles for England:
The OHID Local Alcohol Profiles for England highlight that “alcohol misuse is the biggest risk factor for death, ill-health, and disability among 15–49-year-olds in the UK. It’s also the fifth biggest risk factor across all ages and is a causal factor in more than 60 medical conditions.”
The figures below illustrate the data by districts and boroughs within Surrey for alcohol specific mortality and potential years of life lost due to alcohol related condition for both males and females:
Figure 5: Alcohol specific mortality, 2020 Directly standardised rates, per 100,000
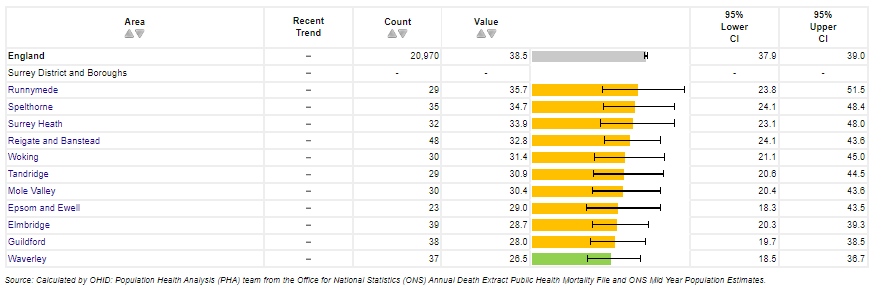
Figure 6: Potential Years of life lost due to alcohol related conditions (Male) DSR, per 100,000
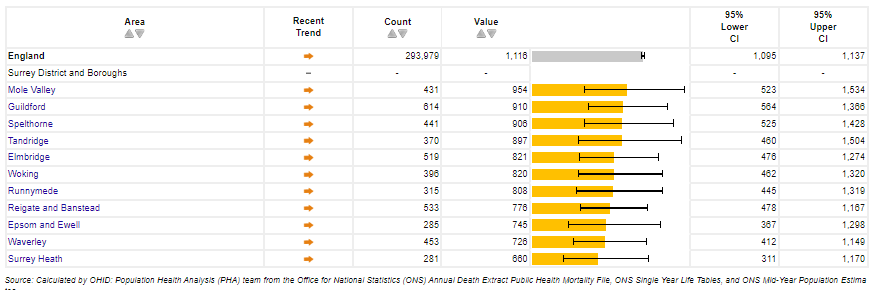
Figure 7: Potential Years of life lost due to alcohol related conditions (Female) DSR, per 100,000
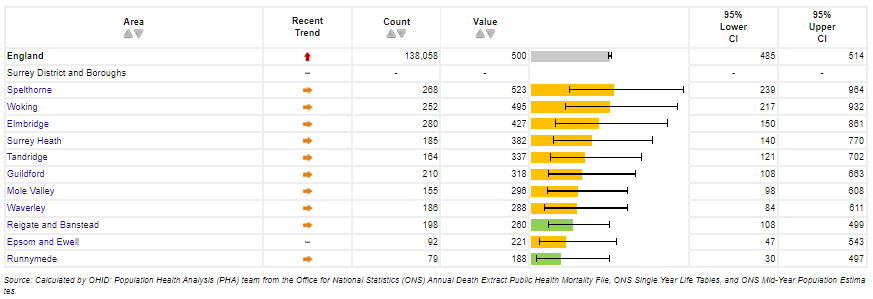
Potential years of life lost (PYLL) is a measure of the potential number of years lost when a person dies prematurely. Although not specifically about people experiencing multiple disadvantage, a proportion of this cohort will be experiencing multiple disadvantage.
National data from latest National Drug Treatment Monitoring System (NDTMS) report:
National data from latest National Drug Treatment Monitoring System (NDTMS) report (2022 to 2023), which looks at data for people in contact with drug and alcohol services between April 2022 and March 2023, highlights that:
- 20% of people starting treatment had no home of their own – this included people living with friends or family as a short-term guest (6%), in temporary supported accommodation (4%), sofa surfing (3%), living on the streets (2%).
- 9% said they were at risk of homelessness in the next eight weeks.
- 71% had a mental health treatment need.
Restricted data showing the local Surrey picture indicates an unmet need for those people experiencing multiple disadvantage with a number of people in contact with the criminal justice system and known to be opiate or crack cocaine users (OCU) but not recorded in the community treatment data. This proportion is higher than that for England.
Please note that not all individuals accessing services are reported on NDTMS data. For example, there may be people experiencing multiple disadvantage who are engaged with services providing support, but not receiving structured treatment and therefore not recorded in NDTMS data.
For more information, please refer to the Substance Misuse JSNA chapter.
Office for Health Improvement and Disparities (OHID) Inclusion Health Reports:
The Inclusion Health data packs produced by Office for Health Improvement and Disparities (OHID) highlight the “significant overlap of populations experiencing multiple disadvantage including alcohol and drug dependence, homelessness, offending behaviours and mental ill health.” Drug use is associated with numerous mental and physical health conditions. For more information, please refer to the Substance Misuse JSNA chapter.
Alcohol consumption is also identified as a risk factor in developing mental health conditions as well as a risk to physical health. It is reported that over two-thirds of people starting treatment for drug or alcohol dependence said that they had a mental health need; looking at the figures presented in the OHID Inclusion Health Reports and quoting from this national report for alcohol treatment only, this figure is 70%. Out of those people identified as having a mental health treatment need, 79% were receiving support from mental health treatment services.
Data from 2020/21 shows that 1,352 Surrey residents were reported to be in treatment at specialist alcohol use services; based on evidence quoted above, we could expect over 946 of these to also be experiencing a mental health need. [11]
From the OHID Public Health Profiles in 2020/21, 2,134 Surrey residents were in treatment at specialist drug use services; based on the evidence quoted above, we could expect over 1,400 of these to also be experiencing a mental health need.
High Intensity Users (HIUs):
There are five acute trusts in Surrey. As an example, the data from one hospital’s High Intensity Users are patients who regularly call an ambulance or attend Accident and Emergency (A&E) (i.e., the top 50 people who make most high intensity use of A&E identified utilising A&E data systems). A snapshot of high intensity users at one hospital also demonstrates the co-occurrence of substance health and mental health issues. Out of 79 attendances included within the snapshot for 2023, 37 (47%) had co-occurring mental health and substance use issues. A total of 53 (67%) attendances were for females. The most common age band was the 30-39 age bracket with 29 attendances.
Sexual health:
Data from Surrey’s sexual health service included details of service users that could be used to identify those people who were experiencing multiple disadvantage. The data included information on the following:
- Those service users with substance use, including alcohol use.
- Those with a mental health need.
- Those experiencing homelessness or in residential care.
- Those with a learning disability.
- Those who had experienced domestic abuse in the previous three months.
The challenge experienced by the most people was substance use, so this dataset has been included in this section.
Data from 3,629 service users was analysed covering the 6 years from 2017 to 2022. Of this total number, 100 were flagged as experiencing more than one challenge from the list above. From this cohort of 100: 75 had substance use issues, 68 had mental health issues, seven had learning disabilities, 47 reported being homeless, and 12 reported domestic abuse in the previous three months. As mentioned, substance use was the most commonly occurring disadvantage and 49 experienced co-occurring substance use and mental health issues.
Little demographic information is available for this cohort of people, but we do know that 69% of those highlighted as experiencing multiple disadvantage were female.
Surrey Drugs-Related Deaths Audit:
This is an audit of deaths identified as drug related or by suicide with a drug-related causes in Surrey between 2017-20. Key findings demonstrate the overlaps between substance use issues and other challenges, in particular mental health, physical disabilities and contact with the criminal justice system: [12]
- Out of 151 drug-related deaths in these four years, 27% had a Coroner’s verdict of death by suicide.
- 102 of these deaths were men, 49 women. The mean age of death for men was 42.6 years, lower than the mean age of death for women of 49.8 years. Nine of every ten deaths in men are of those under 60, compared to seven in ten deaths in women under 60.
- Individuals who died had many complex needs. Three in ten (31%) of those who died from a drug related death were recorded as having a disability; one in ten were homeless; three in ten were unemployed; and almost a quarter had a history of violence and abuse, as either perpetrators or victim.
- The most common contributing factors to individuals’ deaths was mental health needs and addiction (44%), followed by chronic pain or illness (22%), relationship problems (21%) and bereavement (19%).
- Although three quarters (77%) of individuals had a documented history of use of alcohol or drugs and the majority (83%) were currently using them, only a third (35%) had a record of ever being in contact with substance use services. Only one in ten (10%) were in contact with substance use services at the time of their death.
- Three in ten (31%) of those who died from a drug related death were recorded as having a disability, higher than the two in ten UK average.
- Three quarters (75%) of individuals had a diagnosed mental health condition, whilst half had a record of being in contact with mental health services. Of these, half were currently in contact with mental health services at the time of death.
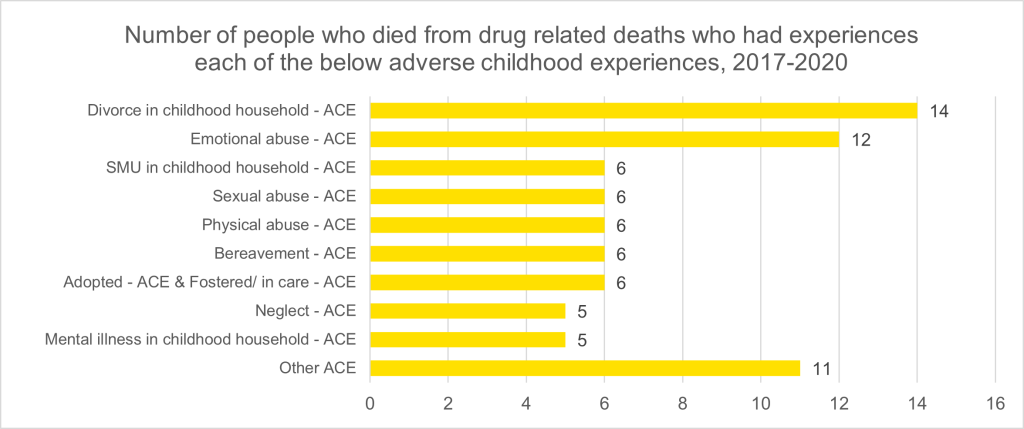
- 32% had a record of adverse childhood experiences (ACEs), see Figure 8 below.
Figure 8: Number of people in Surrey who died from drug related deaths who had experiences each of the below adverse childhood experiences, 2017-2020
Another key finding from the 2020 Drug Related Death Audit was the high proportion of individuals that had a history of substance use who had either never been in contact with substance use services or were not in contact with them at the time of their death. Treatment for substance use and contact with specialist substance use services are protective factors in reducing drug related deaths. Therefore, any action plan to reduce drug related deaths needs to consider how accessible services are to a diverse range of potential service users with multiple needs.
The audit was not able to identify the reason for this gap between need and service use, however the audit states that possibilities could include lack of service capacity, accessibility of services, insufficient identification of those in need, amongst other reasons.
The audit also found three quarters (75%) of individuals for whom information about mental health was available had a diagnosed mental health condition, whilst half of the individuals had a record of being in contact with mental health services, of whom almost half were currently in contact with mental health services. Whilst this unmet need is not on the same scale as the deficit in need for substance use services and compares relatively favourably with national data, the scale of unmet mental health need is still large.
A national enquiry into drug related deaths noted a range of risk factors for drug-related death: being white, single or divorced, unemployed, male, and living alone. The national enquiry is quoted in the Surrey-specific 2020 audit, and highlights that:
- Two-thirds of cases had a self-diagnosed mental health condition, but only 14% of these cases had a record of being in contact with mental health treatment services when they died.
- 77% of this cohort were categorised as ‘White’ with 14% ‘not stated’. 75% were categorised as heterosexual, with 23% not stated.
- 54% who died from drug related deaths were single, higher than the England figure of 35% who are single. 35% were living alone at the time of death, higher than the figure of 27% for Surrey as a whole (from the 2011 census).
In recognition that the factors responsible for increased drug-related deaths are multiple and complex, an attempt was made in this audit to identify the number of individuals who had died experiencing multiple disadvantage. The audit acknowledged that specific definitions of multiple disadvantage differ, and there is no Surrey-wide agreed definition. However, the concept applies to those individuals who have complex and persistent health and/or social care needs that affect their life and ability to function in society. More than one of the following factors will be present, including homelessness or being vulnerably housed, substance use, mental, psychological, or emotional health needs, physical health needs, experience of domestic abuse, and contact with the criminal justice system.
Deaths identified as suicide:
Based on records held by the Surrey Coroner’s Office of suicides that occurred during 2017-2020 (inclusive), the audit identified 409 suicide deaths over the four-year period. Men accounted for approximately three quarters of all suicides. 34.6% of all people who died from suicide were aged 45-59. [36] The Coroner’s Office closed for parts of 2020 and 2021 due to the COVID-19 pandemic which resulted in fewer inquests over these time periods. The lower number of suicides in 2020 should be interpreted as not a reduction in the number of suicides but as a lower number of inquests occurring during the time period 2020-2021.
- Mental health need: Mental health was a common factor, with 50.6% known to mental health services before their death. 24.7% had contact with a mental health service prior to their death and a further 5.1% had had contact within the last three months leading up to their death. 68.9% were known to have at least one mental health diagnosis (Table 5). Around a third of people who died by suicide were known to have made a previous suicide attempt and over a third of deaths identified by suicide were known to have self-harmed. Public Health profiles (Fingertips) data published by the Office Health Improvement & Disparities (OHID) indicate that between the more recent time period of 2020-22, the average number of deaths identified as suicides per year in Surrey was 100. [34]
Table 5: Suicide deaths with one or more mental health diagnosis, between 2017 to 2020 (Source: Surrey Coroner’s Office, 2017-2020)
| Mental Health Disorder |
2017 (n) | 2018 (n) | 2019 (n) | 2020 (n) | Total (n) | 2017 (%) | 2018 (%) | 2019 (%) | 2020 (%) |
|---|---|---|---|---|---|---|---|---|---|
| 0 | 33 | 26 | 32 | 26 | 117 | 27.7% | 25.5% | 31.4% | 30.2% |
| 1 | 32 | 33 | 31 | 22 | 118 | 26.9% | 32.4% | 30.4% | 25.6% |
| 2 | 27 | 21 | 26 | 17 | 91 | 22.7% | 20.6% | 25.5% | 19.8% |
| 3 or more | 22 | 21 | 12 | 17 | 72 | 18.5% | 20.6% | 11.8% | 19.8% |
| Not stated | * | * | * | * | 11 | 4.2% | 1.0% | 1.0% | 4.7% |
An (*) indicates a suppressed value due to low numbers.
- Substance use: On average, in the four years between 2017-2020, 64.1% of deaths by suicide had either an alcohol or substance use recorded before their death. This covers individuals who had a combination of long-established alcohol use and/or drug use. National evidence reveals that only a minority of individuals who die by suicide were in contact with specialist substance use services despite alcohol and drug use being a common antecedent of suicide across the UK. If an individual is successfully engaging in treatment, treatment is a protective factor. This resonates with the Surrey situation whereby only 3% of the individuals who died by suicide were in contact with specialist substance use service prior to death, 1% in the previous three months, 3% in the last 12 months and 3% over 24 months.
- Contact with the criminal justice system: Over a fifth (n=41; 20.2%) of people who died by suicide were known to have been involved with the criminal justice system (this includes a history of prison, remand, arrest, or chargeable offences). 9.9% (n=20) of suicides were in contact with the criminal justice system at the time of their death.
- Neurodevelopmental conditions: When individuals with a neurodevelopmental conditions are not picked up by support services appropriately or their condition is not recognised, it has been demonstrated that the risk of suicide is far greater. [72] The lack of access to appropriate timely therapeutic interventions can exacerbate mental health conditions and/or increase the likelihood of involvement with the criminal justice system. It has also been demonstrated that better recognition and earlier intervention can lead to a change in the individual’s presentation and long-term outcomes.
- Analysis of coroner reports show that some cases who sadly died of suicide had recently been engaged with mental health services. More analysis is needed to understand the timing of the death. This can be done via the suicide audits. Of suicides that occurred 2017-2020 inclusive 4% visited their GP in the preceding 24 hours to death and one in five individuals had a GP visit up to two weeks before death. The highest proportion of individuals, equating to just over a quarter (28%) visited over three months prior to death. The reasons for the visit varied between a mental health issue, a physical issue, both issues or just a routine appointment. One research participant reflected on the impact of people being told they are not eligible for a service: “People have killed themselves the day after their appointment, so when they were told they weren’t eligible for a service.” (Interview IP43, person supporting people with lived experience of multiple disadvantage)
3.1.4. Homelessness or at risk of becoming homeless
In February 2024, Surrey published a JSNA chapter on Housing and Related Support, for more information, please see Housing and Related Support JSNA.
Underlying causes of homelessness include structural, societal, and economic factors, and inequalities, such as poverty, unaffordable housing, unemployment, exclusion, and discrimination. People experiencing homelessness often experience multiple disadvantage and unmet health and social care needs that may be contributing factors for becoming homeless as well as consequences of homelessness. Experience of psychological trauma and adverse childhood events are common in people experiencing homelessness, and the prevalence of people who are neuro-atypical or have a brain injury is higher than in the general population. [13]
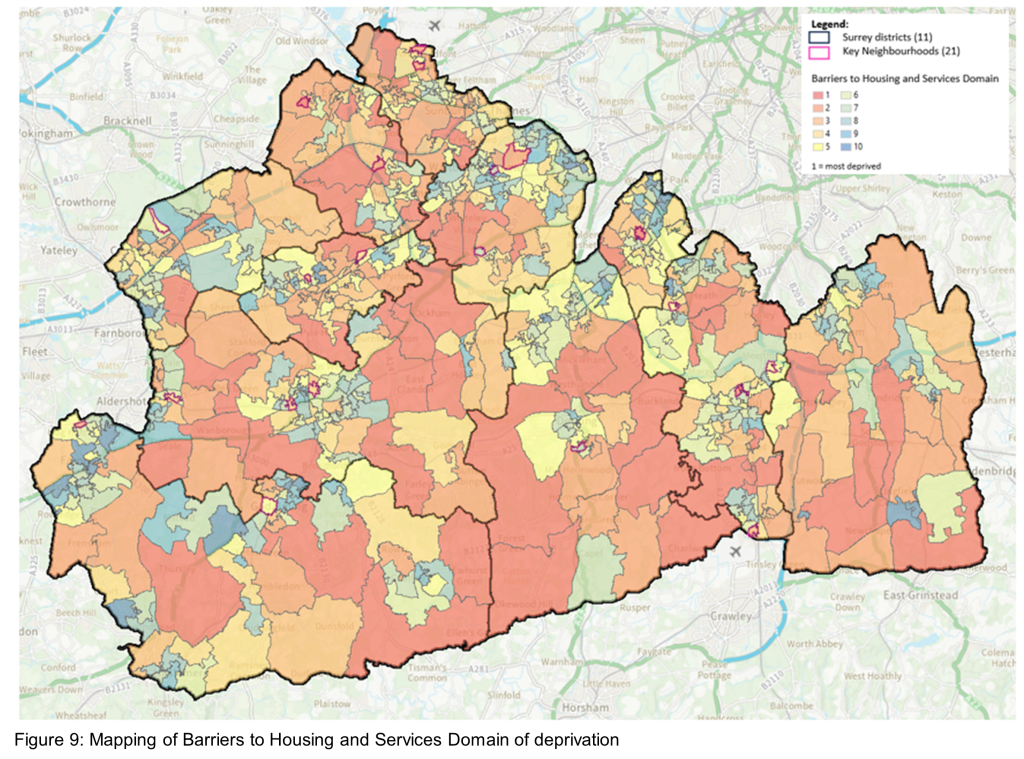
The Index of Multiple Deprivation (IMD) is an overall relative measure of deprivation constructed by combining seven domains of deprivation according to their respective weights. The map below (Figure 9) shows the 11 Surrey Districts and Boroughs and 21 Key Neighbourhoods alongside the Barriers to Housing and Services Domain of deprivation. The Barriers to Housing and Services Domain measures the physical and financial accessibility of housing and local services. The indicators fall into two sub-domains: geographical barriers, which relate to the physical proximity of local services, and wider barriers which includes issues relating to access to housing such as affordability.
Figure 9: Mapping of Barriers to Housing and Services Domain of deprivation
Owed a duty and support needs:
Information on people at risk of homelessness includes information on new prevention and relief duties owed. Prevention duties include any activities aimed at preventing a household threatened with homelessness within 56 days from becoming homeless. Relief duties are owed to households that are already homeless and require help to secure settled accommodation.
The main duty describes actions a local authority must take for an applicant who is unintentionally homeless, eligible for assistance and has priority need. This definition has not been changed by the 2017 Homelessness Reduction Act (HRA). However, these households are now only owed a main duty if they did not secure accommodation in the prevention or relief stage. The Department for Levelling Up, Housing and Communities (DLUHC) Homelessness Case Level Collection (H-CLIC) Homelessness returns include information on support needs for those households, which provide an indication of those at risk of homelessness and also experiencing multiple disadvantage.
Surrey has a similar percentage of homeless household support needs to that of the Southeast, slightly higher than the England average across the number of support needs groups of one need, two support needs or three or more needs. (1, 2, 3+) (see Figure 15).
Reigate & Banstead has the highest number of households with three or more support needs, (43.4%), this is a slight decrease from the previous 12 months, April 2021 to March 2022. This is significantly higher than both the England (30.4%) and the South East (28.1%) averages.
Mole Valley (32.1%) and Spelthorne (32.1%) have the highest proportion of households which have two support needs, this is higher than the National average (24.1%), South East (25.0%) and Surrey (26.1%). 9 of the 11 district and boroughs show that applicant needs of two or more are above the England average (24.1%). A third of households who are owed a duty of support have at least one support need in Surrey.
Table 6: Households with the number of support needs in 2022/23 and the percentage of those households experiencing 1, 2, or 3 or more support needs.
| Area | Total Number of Support Needs 2022/2023 | Number of Support Needs 1 |
Number of Support Needs 2 |
Number of Support Needs 3+ |
% of Support Needs 1 |
% of Support Needs 2 |
% of Support Needs 3+ |
|---|---|---|---|---|---|---|---|
| England | 157,470 | 71,520 | 38,020 | 47,930 | 45.4 | 24.1 | 30.4 |
| South East | 21,440 | 10,070 | 5,350 | 6,020 | 47.0 | 25.0 | 28.1 |
| Surrey | 1,841 | 854 | 480 | 507 | 46.4 | 26.1 | 27.5 |
| Elmbridge | 120 | 60 | 33 | 27 | 50.0 | 27.5 | 22.5 |
| Epsom & Ewell | 134 | 83 | 35 | 16 | 61.9 | 26.1 | 11.9 |
| Guildford | 250 | 123 | 62 | 65 | 49.2 | 24.8 | 26.0 |
| Mole Valley | 221 | 90 | 71 | 60 | 40.7 | 32.1 | 27.1 |
| Reigate & Banstead | 385 | 127 | 91 | 167 | 33.0 | 23.6 | 43.4 |
| Runnymede | 122 | 59 | 26 | 37 | 48.4 | 21.3 | 30.3 |
| Spelthorne | 165 | 74 | 53 | 38 | 44.8 | 32.1 | 23.0 |
| Surrey Heath | 98 | 39 | 30 | 29 | 39.8 | 30.6 | 29.6 |
| Tandridge | 83 | 62 | 11 | 10 | 74.7 | 13.3 | 12.0 |
| Waverley | 139 | 58 | 40 | 41 | 41.7 | 28.8 | 29.5 |
| Woking | 124 | 79 | 28 | 17 | 63.7 | 22.6 | 13.7 |
In the 12 months from April 2022 to March 2023 there were 3,831 households in Surrey reported as “owed a homelessness duty by support need”. This is similar to the previous 12 months of 3,599 households. Approximately a quarter of households have a history of mental health problems (n=873; 22.8%), this is similar to the previous 12 months April 2021 to March 2022.
Physical ill health and disability (16.5%), at risk or experiencing domestic abuse (10.2%), offending history (6.8%) and a history of repeat homelessness (5.3%) are in the top five categories of support needs. This is similar to the previous 12 months, April 2021 to March 2022.
Multiple support needs can be reported per household, but each support need is reported only once. Support needs are not the same as ‘priority need’ and it is possible that a household with support needs does not have a priority need.
In summary, headline figures from this data indicate:
- The highest proportion of Surrey applicants assessed as owed a housing relief or duty are in the age group range of 25 to 34 years (25.5%), below the national average (30.0%). Reigate and Banstead borough (32.0%) is slightly above the national average.
- All age groups between 45-75+ are above the national average, which reflects Surrey’s aging population, with the 65 and over age cohort estimated to increase over the next three years.
- Reigate & Banstead (67.0%) has the largest proportion of households who are owed a homelessness duty with two or more support needs. This is a decrease in the previous 12 months April 2021 to March 2022, (71.5%). Tandridge (25.3%) has the lowest number of households with two or more support needs.
- Top three support needs in Surrey were history of mental health problems (22.8%), physical ill health and disability (16.5%) and those at risk of domestic abuse (10.2%).
- Runnymede (83.3%) had the highest percentage of referrals under the duty to refer, followed by Surrey Heath (76.9%) and Epsom and Ewell (74.1%).
- The National Probation Office (34.3%) made the highest proportion of referrals, followed by Children’s Social Services (17.3%), and Hospital A&E, Urgent Treatment Centres and/or in-patient care (16.3%).
- Approximately 22.6% of applicants at the time of applying for support were living with family, followed by those with no fixed abode (15.4%), and private rental sector (14.6%). 10% were rough sleeping.
Co-morbidity, frailty and premature death:
Many people experiencing homelessness will also be experiencing multiple disadvantage. Increasingly frailty and premature ageing is being seen in the homelessness population, with one research study of people experiencing homelessness with an average age of 56 years finding levels of frailty comparable to 89 year olds in the general population and that participants had an average of 7 long term conditions. [14] Although the proportion of households experiencing homelessness that also suffer from mental health problems within Surrey are below the England figure of 11.5% and the Southeast figure of 13.25%, there are some areas that have significantly higher proportion of households experiencing homelessness and suffering from mental health problems, in particular Mole Valley (27%) and Guildford (25%). [14]
Many people experiencing homelessness will also have substance use issues – in England and Wales in 2021, 35% of deaths of those people recorded as being homeless had a main cause of drug poisoning and 9.6% of deaths had a cause of death that was alcohol specific. 87.3% of all deaths were amongst men. Compared to all regions in England in 2021, the Southeast region had the third highest number of estimated deaths of homeless people. [14]
People experiencing homelessness have far worse health and social care outcomes than the general population. The average age of death for the homeless population is around 30 years lower than for the general population. [13] These premature deaths could be prevented with better access to healthcare. [37]
MEAM produced national policy guidance to encourage national and local government to take clear steps to ensure there is greater learning from the premature deaths of people facing multiple disadvantage. Local areas can significantly improve the response to and subsequent learning from the deaths of vulnerable individuals, in particular those experiencing multiple disadvantage.
Housing Related Support:
Housing Related Support services include help with obtaining benefits and managing money; support to improve safety, health and wellbeing; help to avoid social isolation; and support to access mainstream services, manage everyday tasks, to develop new skills and move into employment. Housing Related Support services do not provide personal care. There are two streams to which funds flow: 1) older people and people with disabilities and 2) socially excluded people.
In Surrey, a total of 1,619 people went through the Housing Related Support accommodation-based services in Q1-Q3 of 2023/24 (end of quarter). For people who have used the Housing Related Support floating support services in Q1-Q3 of 2023/24, there were a total of 750 one to one visits.
Local provider data – Example: Rentstart:
Rentstart, a charity based in Elmbridge that helps local people who are homeless or vulnerably housed, shared data for the purpose of this JSNA chapter as an example of the clients that VCSEs serve locally. In 2022/23 the charity helped 121 clients, of these:
- 36 people (30%) had substance use issues.
- 48 people (40%) were experiencing a mental health need.
- 11 people (9%) reported contact with the criminal justice system, although this is expected to be under-reported.
- 10 people (8%) reported that they had a learning difficulty.
Demographic data is only available for the client group as a whole rather than specific to those clients experiencing multiple disadvantage but demonstrates that:
- The majority of clients were male (79%).
- The majority (76%) were White British or European, with 17% being Mixed Race British or European.
- The majority were aged 25-35 (37%) with 30% aged 36-55.
3.1.5. Prison leavers or people in contact with the criminal justice system
Individuals experiencing multiple disadvantage may be at an increased risk of involvement with the criminal justice system. This can have long-term consequences for mental health, employment prospects, and overall wellbeing.
The Crime Domain of the IMD 2019 measures the risk of personal and material victimisation at local level and is made up of several indicators based on the recorded numbers of violent crimes.
Figure 10: Surrey map of the Crime Domain of IMD (2019)
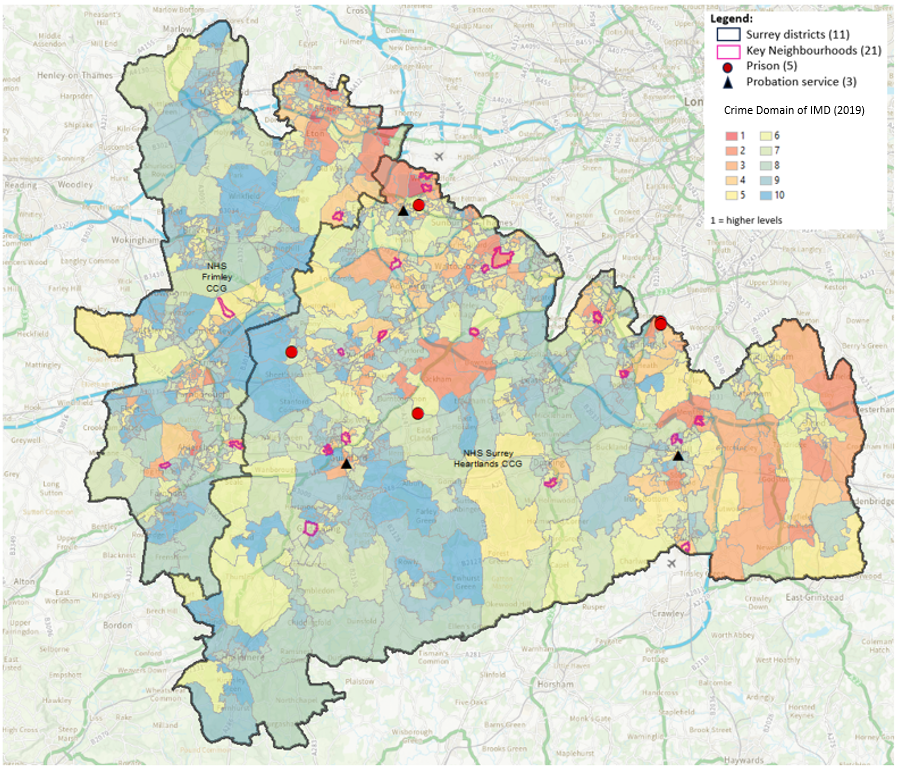
Data collated by the Ministry of Justice from their Offender Assessment System (OASys), an operational database used to assess the risks and needs of eligible offenders in prison and probation trusts across England and Wales, although mostly only available at a national or regional level, helps to describe people in contact with the criminal justice system who are experiencing multiple disadvantage. [15]
Table 7 below shows accommodation, drug and alcohol needs of offenders in England and Wales by gender and age (June 2021):
Female
| Age Band | Accommodation Need (%) | Drug Misuse Need (%) | Alcohol Misuse Need (%) |
|---|---|---|---|
| 18-25 | 67 | 46 | 27 |
| 26-29 | 73 | 62 | 30 |
| 30-39 | 73 | 62 | 32 |
| 40-49 | 73 | 56 | 31 |
| 50-59 | 64 | 29 | 24 |
| 60+ | 70 | 3 | 10 |
| All | 71 | 53 | 29 |
Male
| Age Band | Accommodation Need (%) | Drug Misuse Need (%) | Alcohol Misuse Need (%) |
|---|---|---|---|
| 18-25 | 59 | 61 | 16 |
| 26-29 | 59 | 56 | 21 |
| 30-39 | 62 | 54 | 25 |
| 40-49 | 64 | 50 | 21 |
| 50-59 | 64 | 31 | 18 |
| 60+ | 58 | 8 | 8 |
| All | 62 | 49 | 20 |
All
| Age Band | Accommodation Need (%) | Drug Misuse Need (%) | Alcohol Misuse Need (%) |
|---|---|---|---|
| 18-25 | 59 | 61 | 17 |
| 26-29 | 60 | 56 | 22 |
| 30-39 | 63 | 54 | 26 |
| 40-49 | 64 | 50 | 21 |
| 50-59 | 64 | 31 | 18 |
| 60+ | 59 | 8 | 8 |
| All | 62 | 49 | 21 |
Data is aggregated so individuals may have more than one need and it should also be noted that not all prisoners will have a Full Layer 3 assessment. A Layer 3 assessment contains all sections of OASys including the predictors, criminogenic needs sections, risk sections, risk management plan and sentence plan. In this publication, 78% of the custody population had a complete layer 3 assessment. Regional data (for Kent, Surrey, and Sussex) is available here for male prisoners. The regional proportion of offenders with accommodation and alcohol needs are far lower than the national figures, although higher for drug needs.
Learning difficulties, mental health and maturity needs are also described in the OASys data. Table 8 (below) shows data (proportion of offenders with these needs) for England and Wales for these, although from 2018. [16]
Table 8: Learning Difficulty, Mental Health and Low Maturity Needs by Sentence Length in England and Wales on June 2018
| Sentence Length | Learning Difficulty (%) | Mental Health (%) | Low Maturity (%) |
|---|---|---|---|
| Up to & including 6 months | 49 | 18 | 10 |
| Over 6 months to up to and including 12 months | 52 | 17 | 13 |
| Over 12 months to under 4 years | 39 | 12 | 13 |
| Exactly 4 years | 35 | 9 | 13 |
| Over 4 years to up to and including 10 years | 31 | 8 | 12 |
| Over 10 years to less than Life | 27 | 6 | 6 |
| Life | 30 | 14 | 5 |
| Extended Determinate | 42 | 19 | 13 |
| Imprisonment for Public Protection | 45 | 23 | 2 |
| Recall | 45 | 19 | 15 |
| Total | 36 | 12 | 10 |
Additional Surrey data on those people in secure settings with mental health needs identifies that around a third of those starting treatment for alcohol or drug issues also had a mental health need. [17]
OHID Official Statistics identify that there were 45,096 adults in alcohol and drug treatment in prisons and secure settings in England between April 2021 and March 2022. Numbers in treatment saw an increase of 3% in the last twelve months from April 2021 to March 2022. The proportion of adults released from prison and successfully starting community treatment within three weeks of release was 37.4% in 2021 to 2022. This is a slight decrease from the proportion reported in 2020 to 2021 (38.1%) but is still 7.1% higher than when these data were first reported in 2015 to 2016 (30.3%).
Empowering Communities with Integrated Network Systems (ECINS) platform:
The ECINS platform is a multi-agency system providing “a secure, General Data Protection Regulation (GDPR) and data protection compliant platform for timely and efficient information sharing on joint interest cases for the reduction of crime, disorder and anti-social behaviour under the Crime & Disorder Act 1998 and complementary legislation such as the Anti-Social Behaviour Police and Crime Act 2014. It can also be used to identify and support vulnerable victims and people with complex multiple needs who need targeted support and intervention by a variety of different agencies at any one time, such as victims of cuckooing or criminal exploitation.” [18] Data from this platform is categorised into different ‘galleries’ which helps to identify those people experiencing multiple disadvantage. Data relates to all areas of ECINS and is not restricted to a specific service area.
Table 9: Total number of people in the top 10 ECINS galleries by district and borough
| District & Borough | ACES | Complex Needs | Domestic Abuse Victims | Drug Intervention | Early Intervention | Housing | Mental Health | Schools | Vulnerable Persons |
|---|---|---|---|---|---|---|---|---|---|
| Area unrecorded | <5 | 7 | <5 | <5 | 0 | <5 | 14 | 5 | <5 |
| Elmbridge | 16 | 12 | 10 | 6 | 11 | 8 | 13 | <5 | <5 |
| Epsom and Ewell | 5 | 14 | 13 | 8 | <5 | 5 | 23 | <5 | 8 |
| Guildford | 0 | 26 | 9 | 15 | 0 | 16 | 29 | 0 | <5 |
| Mole Valley | 0 | 13 | 10 | 2 | 0 | <5 | 16 | 0 | <5 |
| Reigate & Banstead | 0 | 17 | 16 | 6 | 0 | 8 | 26 | <5 | 5 |
| Runnymede | 0 | 7 | 18 | <5 | <5 | 7 | 12 | <5 | <5 |
| Spelthorne | <5 | 10 | 22 | <5 | 0 | 12 | 16 | <5 | 5 |
| Surrey Heath | 10 | 14 | 25 | 6 | 7 | 8 | 20 | <5 | <5 |
| Tandridge | 0 | <5 | <5 | <5 | 0 | 5 | 5 | 0 | <5 |
| Waverley | <5 | 16 | 26 | <5 | 0 | 8 | 19 | 0 | 8 |
| Woking | 7 | 11 | 71 | 7 | <5 | 12 | 34 | 7 | <5 |
| Total | 42 | 151 | 227 | 64 | 26 | 92 | 227 | 27 | 45 |
Probation data:
Probation data provided to us by Kent, Surrey and Sussex (KSS) Probation Service includes information on those people on probation who also experienced other disadvantages namely mental health, domestic abuse, substance use and homelessness. The data tells us that across KSS, 91.6% of people on probation are male, of those 38.4% have two recorded multiple disadvantage conditions, 53.1% have three or more conditions. 8.4% of people on probation are female, of those 23.8% have two identified multiple disadvantage conditions, and 76.2% have three or more recorded. Some key headlines are given below. Note that these are for Surrey as a whole:
- 7.7% of people on probation had at least one recorded mental health need. Of those 57.2% had a drug and alcohol issue and 3.7% were identified as homeless.
- A fifth of those on probation have a drug or alcohol need.
- 29.7% of those on probation were identified as having been a victim or a perpetrator of domestic abuse. Of those, two thirds had a record of drug and alcohol use, 30.2% were known to have at least one mental health diagnosis, and 5.2% were recorded as homeless.
- Less than 3% of those on probation are considered to be homelessness, with approximately one fifth (18.9%) of those with a drug or alcohol need.
OHID Inclusion Health reports:
The OHID Inclusion Health Reports highlight that, on a national level, many of those in contact with the criminal justice system are experiencing multiple disadvantage: a third of that population have a learning disability or difficulty, a third have neurodivergent needs, and 71% of women and 47% of men have mental health problems.
Within Surrey Heartlands Integrated Care System (ICS), as of September 2023 the total adult prison population was 2,649 with 1,642 (62%) being male. There are no prisons within Frimley Integrated Care System (ICS).
Cuckooing:
Cuckooing refers to a vulnerable person’s home being taken over by drug dealers or organised crime gangs and used as a place from which to run their drugs business or other crime activity. It is important to consider this population group when looking at those experiencing multiple disadvantage as victims of cuckooing are often part of this cohort. In Surrey, cuckooing support is co-commissioned by Surrey County Council’s Public Health Substance Misuse team and the Office of the Police and Crime Commissioner (OPCC). Catalyst Support’s Specialist Outreach Cuckooing Service works in partnership with Surrey Police and local authority housing to ensure a partial closure order is put in place when there is evidence of cuckooing – this order will enable the tenant to stay in their homes and the people that are exploiting the individual are prevented from being there, and if they fail to comply it is a criminal offence. The service helps individual’s build their resilience and ensure services and support are in place to prevent the re-occurrence. The service also offers prevention visits and advice to anyone in Surrey.
Data from an infographic produced by Catalyst Support details the breakdown of indicators presented by cuckoo clients in Surrey in 2022:
- 76% were engaged in substance use.
- 66% had reports from neighbours (anti-social behaviour or concerns).
- 52% had a mental health diagnosis.
- 51% had a history of homelessness.
Data from June 2023 showing referrals to date for Catalyst Support’s cuckooing services shows that:
- 148 females and 245 males have been referred to date, so 38% females and 62% males.
- The majority of referrals (over 90%) were White British
- Over 83% had current or past substance use issues.
3.2. Other risk factors (locally identified)
The following risk factors have been acknowledged by the LERO as additional factors that an individual who is facing multiple disadvantage may experience.
3.2.1. Neurodevelopmental conditions
Neurodiversity is another risk factor of multiple disadvantage, as people can be disadvantaged because of the lack of recognition and support around neurodivergence. Substance use can also typically ‘mask’ neurodivergent behaviours and is often misinterpreted. [68]
The Emotional and Mental Wellbeing in Surrey Adults JSNA chapter includes information on neurodivergence. Neurodivergence is an umbrella term for people with Autism Spectrum Disorder (ASD) 1.5-2%, Attention Deficit Hyperactivity Disorder (ADHD) 3-6%, Foetal Alcohol Spectrum Disorder (FASD) 4-6%, Tourette’s 2-3%, Development Coordination Disorder (DCD) 2-6%, Dyslexia and Sensory integration disorders. It is now widely evidenced that people with one form of neurodivergence are more likely to have other commonly co-occurring forms, in addition to both an increased risk and occurrence of mental health issues across their life course.
People with a learning disability and/or autism who have a mental health condition may result in them displaying behaviour that challenges, for example aggression and violence. This can result in people having contact with the criminal justice system instead of mental health services.
Many autistic people, for example, experience feeling:
- very worried a lot of the time (anxiety).
- unhappy, irritable, or hopeless (depression).
- a need to keep doing certain actions – obsessive compulsive disorder (OCD).
It should be noted, though, that ADHD is now recognised as a neurodevelopmental condition and not a mental health issue in itself. Though as with autism, the prevalence of mental health issues alongside ADHD is higher than in the general population. [79]
Surrey County Council’s All Age Autism Strategy 2021 to 2026 highlights the local picture of autism across Surrey. In 2021, the strategy estimated that Surrey’s population was 1.23 million. Therefore, based on national data the strategy shares a best approximation of Surrey’s autistic population, estimating that the autistic population is 12,300 people, made up of:
- 3,200 children aged 17 and under.
- 900 young people aged 18-24.
- 8,200 people aged 25 and over.
Currently autism is thought to be three times more common in males than females. This ratio may change as understanding of the way autism presents in women and girls improves. Research has suggested that autism may be under-diagnosed in females, gender-fluid and non-binary people. [19]
Of the 9,100 autistic people aged 18 and over in Surrey in 2021, 20% (n=1,834 people) are in receipt of a service from Adult Social Care (ASC), and a fifth (20%; n=1,834) of these are women. [19]
National Institute for Health and Care Excellence (NICE) guidance estimates that around 70% of autistic people have an additional condition, which is “often unrecognised”. The main conditions that co-occur more frequently in autistic people compared with the general population include:
- Mental health conditions: Research from Autistica suggests that 70% of autistic people have a mental health condition, and that 40% have two or more. Autistic people are up to four times more likely to have an anxiety disorder, and twice as likely to have depression, compared to non-autistic people.
- Additional neurodevelopmental conditions: Autism is one such condition, and people with 1 diagnosis may also have traits of other neurodevelopmental conditions. [73] Research shows that these include general learning disabilities (affecting between 15% and 30% of autistic people), specific learning difficulties (such as dyslexia and attention-deficit hyperactivity disorder), and other conditions such as epilepsy. Delays in language development are common in autism, and research from the Health Policy Partnership indicates that up to 30% of autistic people are non-speaking (completely, temporarily, or in certain contexts).
- Foetal Alcohol Spectrum Disorder (FASD): People with FASD previously were thought to require specific facial features to meet diagnosis, but now it is understood that this presents in around 2 to 5% of individuals affected. [20] This means by far the majority of people with FASD do not present as typically understood and therefore often go undetected and missed by services. Even when diagnoses are sought for people experiencing these challenges, often people present subthreshold for the FASD diagnostic profile. Despite this they may still have neurological deficits. These can include difficulties with working memory, executive function, language, visuospatial skills, emotional regulation as well as other areas of sensory integration which may not be severe enough on their own to meet a diagnostic threshold, yet when combined, lead to significant deficits for the individual. These are all neurological deficits in information processing that put individual’s experiencing them at a disadvantage and vulnerable to other experiences. [74]
Research is increasingly demonstrating that individuals who have these levels of difficulty, especially when they are missed, are vulnerable to subsequent adverse experiences and traumatic presentations. People with neurodevelopmental conditions are far more likely to experience environmental trauma, experience abuse or be exploited by others.
Where the vulnerability is not identified early on, it is far more likely that subsequent mental health conditions will develop. Suicide is a leading cause of early mortality amongst autistic people. A systemic review of suicide in autism carried out by Hedley and Uljarević in 2018 found that prevalence rates for suicidal ideation were 11 to 66% and suicidal attempts were 1 to 35%. Research has suggested that 14% of autistic children experience suicidal thoughts, compared with 0.5% of non-autistic children (Please see Emotional and Mental Wellbeing in Surrey Adults for more information). Some studies have identified that almost 60% of people presenting to a mental health pathway may well have an underlying neurodevelopmental presentation, which is often missed. [21] Having a neurodevelopmental condition also increases the likelihood of not being able to access appropriate support or help and being vulnerable to exploitation by others; this means the likelihood of them presenting either as homeless or within the criminal justice system is far greater. [22]
Due to individuals with neurodevelopmental conditions not always presenting in a way that is easy to identify, it is sensible to consider whether or not there is a neurodevelopmental condition potentially in all individuals who have a complex presentation. This does not mean that there will be an issue, but it prevents individuals being missed. Undertaking this screening and consideration in all such cases will allow better recognition, earlier intervention and appropriate signposting to treatments that will be beneficial, rather than using standardised approaches which may have no therapeutic ongoing benefit. This approach could enable efficient signposting to the most appropriate treatment route (psychological, pharmacological and/or social), which would be valuable in a context of limited health resources.
Based on the evidence presented in this chapter, it is clear that understanding the complex interplay between life experiences trauma and vulnerability is vital to understanding the nature, triggers and management of complex presentations. These factors need to be considered to help understand the person and guide their ongoing care. Not doing so risks exacerbating the presentation and perpetuating the vulnerability of these individuals.
3.2.2. Physical health and long-term health conditions
People experiencing multiple disadvantage may experience long-term difficulties, including health conditions and comorbidities of mental and physical health problems, which limit their ability to live independently. Threats to physical health include diseases such as liver disease, blood borne viruses (BBV), cardiovascular diseases (CVD), and chronic obstructive pulmonary disease (COPD). The Homeless and Inclusion Health Barometer (2024) includes evidence from Homeless Health Needs Audit (HHNA) that indicates why some people in inclusion health groups attend A&E. Physical health problems/conditions are one of the most common reasons for people experiencing homelessness in England to attend A&E, accounting for 32% of attendances. Similarly, HHNA data shows physical health problems or conditions (37.3%) are the most common reason for emergency inpatient admissions amongst people experiencing homelessness. The Barometer also presents evidence suggesting that living in temporary accommodation can actively contribute to poor mental and physical health. Survey research from Shelter found that 66% of people living in temporary accommodation in England reported it as having a negative impact on their mental or physical health
OHID Liver Disease profiles indicate that:
- During the financial year ending 2021, the England rate of hospital admissions due to liver disease in persons was 124.3 (123.4 to 125.3) per 100,000 population.
- During 2020 the average rate of mortality from liver disease in persons was 13.8 per 100,000 population aged under 75 in NHS Surrey Heartlands ICB.
The ASC dataset provides information about those people with physical disabilities and sensory impairments experiencing multiple disadvantage in Surrey. As of October 2023, ASC have approximately 3,500 open cases aged 18 or over where the individual has a PCC of Adult with a Physical Disability Matching it against other Primary / Secondary Support Reason shows the support reasons of ‘Learning Disability support’ and ‘Mental Health support’ occur for 6% with PCC of Adult with Physical Disability. Approximately 5% of the people open to ASC with a PCC of Adult with a Physical Disability live in a LSOA with an IMD deciles (2019) 1-3. When looking at the breakdown by district and borough in Surrey, some districts and boroughs have notably higher percentages of Adults with a Physical Disability in the lower deciles of IMD (2019), such as Spelthorne, Guildford, Epsom and Ewell and Reigate and Banstead compared to other areas of greater affluence.
For Adults with Physical / Sensory Disabilities the approximate breakdown by sex is two thirds female and one third male. Drilling down on Primary / Secondary Support reasons shows:
- For Mental Health support the approximate breakdown by sex is two thirds female, one third male.
- For Learning Disability support the inverse pattern is seen, with one third females and two thirds male.
Surrey’s 18+ population as a whole is a fairly even split between males and females.
For PCC of Adults with Physical Disability, the approximate breakdown of ethnicity is 80% White, followed by Asian / Asian British at approximately 5%, with approximately 10% ‘not known’. Drilling down on Primary / Secondary Support Reasons shows that for ‘Mental Health Support’ and ‘Learning Disability Support’ there is not much difference in the ethnicity proportions.
For PCC of Adults with Physical Disability the peak age range is between 50 to 69, representing approximately 50% of the whole cohort. Drilling down on Primary / Secondary Support Reasons shows:
- For mental health support there is not much difference with the peak age still between 50 to 69, but the relative proportion is higher (approximately 60%) than for the whole ASC PCC Adults with Physical Disability cohort.
- For learning disability support the peak is at an earlier age with approximately 40% of the population between 20 to 29.
For ‘Adults Physical Disabilities’ the highest percentage in terms of religion is Christian (approx. 40%), none (approx. 15%) and Muslims (approx. 2%). Drilling down on Primary / Secondary Support Reasons shows:
- For mental health support there is not much difference, although percentages are relatively higher compared to the whole PCC Physical Disability cohort, probably as a result of the proportion of ‘not knowns’ reducing.
- For learning disability support the percentage of those reported as Christian increases to around 60%, likely to be as a result of ‘not knowns’ reducing. Approximately 30% of the population is unknown / declined to answer and this high percentage is likely to skew the results.
Surrey Coalition of Disabled People Cost of Living Report:
A report from the Surrey Coalition of Disabled People examining the cost of living crisis from the perspective of disabled people highlights the number of people in Surrey who are physically disabled who are also likely to be experiencing multiple disadvantage:
- 33% of adults in the lowest 10% for household income are disabled compared to 9% in the highest 10%.
- Disabled people had 44% less disposable income than the non-disabled population.
3.2.3. Learning disabilities
ASC currently have approximately 4,000 open cases aged 18+ where the individual has a Primary Client Category (PCC) of Adults Learning Disability. Matching it against other Primary / Secondary Support Reason shows the support reasons of Mental Health support is 4% and Physical and Sensory support is 3%. Approximately 6% of the people open to ASC with a PCC of Adult with Learning Disabilities live in a LSOA with an IMD decile (2019) 1-3.
For Adults with Learning Disabilities the approximate breakdown is two thirds male and one third female. Drilling down on Primary / Secondary Support Reasons shows
- For mental health support there is a relatively lower proportion of males (approximately 55%) and a higher proportion of females (approximately 45%).
- For physical and sensory support shows a more even split between males and females, with females making up a slightly higher percentage.
For ethnicity, the approximate breakdown is 85% White, followed by Asian / Asian British at approx. 5%, with 5% not known. Drilling down on Primary / Secondary Support Reasons shows
- For mental health support there is not much difference.
- For Physical and Sensory support, the White proportion is lower in this group (approximately 80%) while ‘other than white’ is higher (approximately 15% from 10%).
For Adult with Learning Disabilities the peak age range is between 20 to 29 (approximately 30% in this age bracket). Drilling down on Primary / Secondary Support Reasons shows:
- For mental health support there is still a peak at between the ages of 20 to 29 (approximately 20%) but there is also a similar peak at 50-59.
- For physical and sensory support, the peak is at a slightly later age range of 30-39 with approximately 25% of the population.
The religion with the largest number of ‘Adults with a Learning Disability’ is Christian (approx. 60%), none (approx. 15%) and Muslims (approx. 2%).
3.2.4. Adverse Childhood Experiences (ACEs)
Adverse Childhood Experiences (ACEs) are specific traumatic events which occur in childhood (0-17 years). Examples of ACEs include experiencing violence, abuse, or neglect, witnessing violence, or having a family member attempt or die by suicide. ACEs may also include parts of a child’s environment that can undermine their sense of safety and stability e.g., growing up in a household with mental health or substance use problems, parental separation, or an incarcerated relative. A child’s health and wellbeing can also be impacted by traumatic experiences such as homelessness or housing instability, food poverty, or experiencing discrimination. [23]
The impact of Adverse Childhood Experiences:
Experiencing ACEs can have an impact on our future physical and mental health, and often ACEs can be barriers to healthy attachment relationships forming for children. ACEs are also linked to chronic health problems, mental health challenges, and substance use in adolescence and adulthood. ACEs can also negatively impact education, job opportunities, and earning potential. [24]
The national household survey of adverse childhood experiences and their relationship with resilience to health-harming behaviours in England shows that the adversity we experience as children can affect us into adulthood. The Blackburn with Darwen Borough Council study on childhood trauma highlights that ACEs are prevalent across the population and states that:
- Nearly half of people in England experience at least one ACE, with around 9% experiencing four or more ACEs (Blackburn & Darwen Study).
- Six ACEs can reduce your life expectancy by 20 years.
Some of the effects of ACEs on our physical and mental health are: [25]
- An increased risk of certain health problems in adulthood, such as cancer and heart disease, as well as increasing the risk of mental health difficulties, violence and becoming a victim of violence.
- An increase in the risk of mental health problems, such as anxiety, depression, and post-traumatic stress. One in three diagnosed mental health conditions in adulthood directly relate to ACEs.
- The longer an individual experiences an ACE and the more ACEs someone experiences, the bigger the impact it will have on their development and their health.
Some of the other factors exposure to ACEs can impact are:
- The ability to recognise and manage different emotions.
- The capacity to make and keep healthy friendships and other relationships.
- The ability to manage behaviour in school settings.
- Difficulties coping with emotions safely without causing harm to self or others.
To have multiple ACEs is a major risk factor for many health conditions. The outcomes most strongly associated with multiple ACEs represent ACE risks for the next generation (e.g., violence, mental health, and substance use). [26]
A study conducted by Hughes and colleagues (2017) explored the health outcomes and financial burden of ACEs in England and Wales, concluding that cumulative relationships were found between ACEs and risks of all outcomes. [25] For health risks, population attributable fractions for ACEs were highest for drug use (Wales 58.8%, England 52.6%), although ACE-attributable smoking had the highest estimated costs (England and Wales, £7.8 billion). For causes of ill health, population attributable fractions for ACEs were highest for violence (Wales 48.9%, England 43.4%) and mental health (ranging from 29.1% for anxiety in England to 49.7% for other mental health needs in Wales). The greatest ACE-attributable costs were for mental health (anxiety, depression and other mental health; England and Wales, £11.2 billion) and cancer (£7.9 billion). Across all outcomes, the total annual ACE-attributable cost was estimated at £42.8 billion. The majority of costs related to exposures to multiple rather than a single ACE (ranging from 71.9% for high body mass index to 98.3% for cancer). This study concludes that ACEs impose a substantial societal burden in England and Wales. Policies and practices that prevent ACEs, build resilience and develop trauma informed services are needed to reduce burden of disease and avoidable service use and financial costs across health and other sectors. Local areas can invest in approaches that tackle the traumatic effects of ACEs head on, by enabling people to access support in a way that is acceptable to them. This can help improve mental health and wellbeing for those who have experienced trauma in childhood. [27]
3.2.5. Socioeconomic factors
Multiple disadvantage often leads to lower socioeconomic position, which, in turn, affects access to resources such as education, employment opportunities, and adequate housing.
Lower socioeconomic position is a known determinant of health, influencing overall living conditions and wellbeing. Economic hardship is highly correlated with poor health. Economic hardship is a threat to wellbeing, especially for the unemployed and those experiencing wage and benefit cuts. [75]
The Indices of Deprivation 2019 provides an overall set of relative measures of deprivation for small areas (LSOAs) across England, based on seven domains of deprivation (Income, Employment, Education, Health, Crime, Barriers to Housing and Services, Living Environment). LSOAs are small areas designed to be of a similar population size, with an average of approximately 1,500 residents or 650 households. There are 32,844 LSOAs in England, with over 700 in Surrey. They were produced by the Office for National Statistics (ONS) for the reporting of small area statistics. There are 21 Health and Wellbeing Key Neighbourhoods in Surrey, which are the wards with the most deprived “pockets” (LSOAs) within the county according to IMD score
The Cost-of-Living Crisis in Surrey:
The UK is facing its biggest cost of living crisis in decades. In February 2024, SCC reported on how the Cost of Living Crisis may affect Surrey by bringing together a variety of publicly available local and national statistics, as well as locally produced information on local Warm Welcome sites and from Citizens Advice. The report highlights the following:
- Employment: Unemployment activity is still low, though showing signs of increasing. In Surrey, 1.5% of the working age population is unemployed compared to 3.9% for England (Annual Pop. Survey, Oct 2022- Sept 2023).
- Crime: Crime up 5% overall, shoplifting up 49%, and harassment up 55% compared to the same quarter one year previously. Latest public data on crime by detailed offence runs to the end of December 2023.
- Homelessness: Homelessness activity still low, though showing signs of increasing. Statutory homelessness data for the period from April 2022 to March 2023 recorded that 892 households received initial assessments of homelessness. Of the households assessed during this period, 97% (871) were owed a duty: 520 were owed a prevention duty, and 351 were owed a relief duty. For every 1,000 households in Surrey, 1.08 households are assessed as threatened with homelessness and 0.73 are assessed as already homeless. There has also been a sharp increase in landlord repossessions.
The report provides maps of neighbourhoods with greatest proportion of households affected by multiple disadvantage (deprived in at least three of the dimensions of deprivation in the 2021 Census (employment, education, health and disability, and housing overcrowding) versus access to Food Bank delivery points, health and disability deprivation, fuel poverty.
In 2022, SCC and Surrey Heartlands ICS commissioned research into the impact of Cost of Living. This research provides an in-depth view at the current health and wellbeing experiences of residents in 5 of the most deprived wards across Surrey (Chertsey St. Anne’s, Goldsworth Park, Old Dean, Stoke and Court Ward). These wards were chosen based on how they scored on Index of Multiple Deprivation 2019 and District and Borough willingness to participate. Amongst participating residents, 67% feel the Cost of Living Crisis has made them significantly more stressed, 54% feel that the crisis has negatively impacted their mental health, and 45% feel that the crisis has negatively impacted their physical health. [28]
The research also identified that the resilience to the Cost of Living depends on a range of factors, primarily whether or not they have a strong neighbours’ network and have consistently accessed a community organisation and the mesh of care it provides. People tend to access community support at points of crisis. Once through the door they gain easier access to many more sources of support. This boosts their coping mechanisms and their ability to access information and practical support. However, there are many residents that do not access any support, yet the impact of the Cost of Living on them is acute. They need particular attention and help getting an initial positive interaction with community support. [28]
There are multiple interventions across Surrey helping to mitigate the effects of the cost of living and preventing poverty. However, work to further integrate these interventions into a more of a whole system approach to poverty would be valuable.
3.2.6. Adults with experience of care
Care leavers (i.e., individuals who have been in the care of child welfare services and aged out of the system) are often at risk of experiencing multiple disadvantage. At 22 March 2024, there are a total of 959 care leavers in Surrey (aged between 21-25).
The Care Leavers’ Association identified that research and policy on adults who have been in care as children typically focuses on 16–25-year-olds and related challenges such as homelessness, unemployment, and lack of educational qualifications. However, some issues affecting care leavers can apply across the life course. [29] According to the Department for Education, in 2021/22 there were 45,940 care leavers in England aged 17 to 21. Phase 2 of this Multiple Disadvantage JSNA chapter will include data on care leavers and looked after children in Surrey.
3.2.7. Cross-addictions
Cross-addiction can occur when a person replaces one addictive behaviour for another. This can include eating disorders, interconnecting with substance use or other psychological addictive behaviours such as sex, shopping, or gambling. People often assume that if someone stops using their substance of choice, they are cured. Recovery is not straightforward and as Dame Carol Black reports, addiction is a “chronic relapsing condition”. As one addictive behaviour is overcome, it is not uncommon for people to develop new ones. Various risk factors can make people more vulnerable, including a history of substance use, trauma and underlying mental health conditions. A variety of studies have focussed upon a combination of risk factors including genetic predisposition, environmental influences and socioeconomic factors being attributed to creating a propensity for some individuals being more prone to developing addictions than others.
Gambling:
The GamCare helpline and treatment data for 2021/22 and 2022/23 demonstrates the impact of gambling and the links into people experiencing multiple disadvantage. Service users were asked if gambling has had an impact on them in any other aspect of their lives.
- 74% reported anxiety/stress.
- 63% reported depression or low mood.
- 22% reported that they had had suicidal thoughts.
- 15% had been diagnosed with mental health conditions
- 9% had housing problems.
- 2% had substance use issues.
Research on the association between gambling and financial, social and health outcomes in big financial data (2021) examines the link between gambling as a proportion of monthly income and 31 financial, social and health outcomes using anonymous data provided by a UK retail bank, aggregated for up to 6.5 million individuals over up to 7 years. Findings highlighted the impact of gambling on individuals’ health and quality of life. There was a statistically significant correlation between gambling and declining health, opportunity, and quality of life outcomes, with harm rapidly escalating at higher levels of gambling spend. Gambling is associated with higher financial distress and lower financial inclusion and planning, and with negative lifestyle, health, wellbeing, and leisure outcomes. Gambling is also associated with higher rates of future unemployment and physical disability and, at the highest levels, with substantially increased mortality. [30]
GambleAware provide information on levels of harmful gambling. The Problem Gambling Severity Index (PGSI) measures levels of gambling behaviour which may cause harm to an individual, ranging from low risk gambling (score of 1-2), moderate risk gambling (3-7), and problem gambling (8+).
Table 10: percentage of people by local authority experiencing harmful gambling behaviours. Data is from the 2022 GB Treatment and Support Survey.
| Local Authority | PGSI score 1+ | PGSI score 3+ | PGSI score 8+ |
|---|---|---|---|
| Elmbridge | 12.1% | 5.2% | 2.2% |
| Epsom and Ewell | 13.1% | 5.8% | 2.7% |
| Guildford | 12.5% | 5.4% | 2.6% |
| Mole Valley | 11.2% | 4.4% | 1.9% |
| Reigate and Banstead | 12.6% | 5.2% | 2.3% |
| Runnymede | 13.2% | 5.7% | 2.7% |
| Spelthorne | 14.0% | 6.2% | 3.0% |
| Surrey Heath | 13.1% | 5.9% | 2.9% |
| Tandridge | 11.9% | 4.8% | 2.1% |
| Waverley | 11.0% | 4.4% | 1.8% |
| Woking | 12.9% | 5.7% | 2.5% |
| Great Britain | 13.4% | 5.9% | 2.9% |
The percentage of people with a PGSI score of 1 or more in Surrey ranges from 11% in Waverley to 14% in Spelthorne. All districts and boroughs are below the Great Britain figure of 13.4%, with the exception of Spelthorne. A similar pattern is seen for the higher PGSI scores
Eating disorders:
The Health Survey for England 2019 Eating Disorders report found that adults who screened positive for a potential eating disorder were more likely than others to have consulted their GP for a mental health, nervous or emotional problem (24%, compared with 10%). They were also more likely to have received counselling or therapy (16%, compared with 7%). It is estimated that 10-25% of those with an eating disorder are men, eating disorders can affect people of all ages but most develop between late teen and mid-twenties. Eating disorders are linked to physical health conditions and commonly occur alongside mental health conditions and substance use issues.
3.2.8. Gypsy, Roma and Travellers
Data are included within the OHID Inclusion Health data packs around the experiences of the Gypsy, Roma and Travellers (GRT) communities. The GRT communities are considered a health inclusion group alongside those experiencing multiple disadvantage and complexities can be concurrent. As a minority population they have a high prevalence of substance use and domestic abuse. Challenges and inequalities faced by this population include: [31]
- Life expectancies are 10-25 years shorter than the general population.
- Communities are often not recognised in health data meaning healthcare services are unaware of the specific challenges of this group.
- Due to discrimination and stigma faced, GRT communities often have poor health outcomes because of low access to services and care, including challenges when registering for GP services. This group can experience early onset of conditions such as frailty, falls and dementia.
- 42% of Gypsies and Travellers are affected by a long term condition, compared to 18% of the general population.
From 2021 census figures, Gypsy or Irish Travellers made up 0.21% of the population in Surrey Heartlands ICB and 0.19% of the population in Frimley ICB. This compares to 0.18% in the South East and 0.11% nationally. From 2021 census figures, Roma Travellers made up 0.14% of the population in Surrey Heartlands ICB and 0.13% of the population in Frimley ICB. This compares to 0.14% in the South East and 0.19% nationally.
3.2.9. Vulnerable migrants and refugees
Immigrants have been supported in Surrey for many years, arriving either through formal resettlement or visa schemes (with full legal or refugee status and with full access to work, benefits and services) or via irregular routes (those who make a claim for asylum on arrival and are at risk of destitution).
Surrey’s Migrant Health Rapid Needs Assessment highlights how the changes over time in those seeking asylum are largely driven by geopolitical events, since most arrive from countries affected by political and military conflict. In recent years there has been a significant build up in the asylum accommodation system, resulting in large numbers of people being housed in Home Office provided hotel accommodation and in dispersal accommodation in the community.
The Migration Observatory notes that migrants tend to be younger and healthier than many of the general UK population. However, some who arrive have been travelling for many months or longer, are vulnerable and have significant complex unmet health needs that require support. These may be: pre-existing or related to conditions in their country of origin; related to their journey to the UK; or related to conditions they face when they arrive in the UK. The key determinants of health for migrants lie not just with the individual, their country of origin and the circumstances of the journey, but also the circumstances they find themselves in once they arrive in the UK.
Vulnerable migrant populations such as asylum seekers and refugees are considered a health inclusion group and typically experience multiple disadvantage.
Migrants may have experienced: violence or persecution; torture; human trafficking and modern slavery; sexual or gender-based violence, in their country of origin or during their journey. Once in the UK they may be at further risk of exploitation due to their vulnerable circumstances. [76]
Common health challenges for refugees and asylum seekers include: [32]
- Poorly controlled chronic conditions.
- Mental health and specialist support.
- Maternity care.
- Untreated communicable diseases.
Gender, culture and language and translation needs increase the impact of these challenges on both the migrants and the services supporting them.
The response to meet the needs of these population groups has been complex and challenging and continues to evolve to meet need. For more information on the current health needs of the population, the support services in place, and any gaps in the system, please see Surrey’s Migrant Health Rapid Needs Assessment. The report focuses on 6 key health topic areas, identified as a priority for the system including mental health, primary care, women and child health, housing, education, and community integration.
4. National and local policies and best practice
This section considers the policies, best practice, and strategies that exist at both a local and national level relating to multiple disadvantage. Specific recommendations and guidelines that should continue to be implemented in Surrey are highlighted in this section.
4.1. Local policies and guidance
At a local level, policies, strategies, and resources have been developed to help local authorities, commissioners, service providers, and practitioners to improve integrated health and care, and achieve better health outcomes for people affected by multiple disadvantage. The principal local best practice and guidance relating to multiple disadvantage are explored below.
4.1.1. Surrey Health and Wellbeing Strategy
In 2019, the Surrey Health and Wellbeing Board published a 10-year Health and Wellbeing Strategy. It was based on evidence from the Surrey Joint Strategic Needs Assessment and the views of Surrey residents.
The Board refreshed the Health and Wellbeing Strategy in early 2022 in response to COVID-19, to ensure it had a greater focus on reducing health inequalities so no-one is left behind. In the refreshed Strategy there is also a commitment to the outcome: ‘the needs of those with multiple disadvantage are met’ and the following Principles for Working with Communities and an acknowledgement that applying these will be crucial to our success:
- Community capacity building: building trust and relationships.
- Co-designing: deciding together.
- Co-producing: delivering together.
- Community led action: communities leading, with support when they need it.
Delivering the Strategy continues to play a crucial role in achieving the ‘Community Vision for Surrey in 2030’ and quarterly highlight reports of progress across the Surrey system are published here.
4.1.2. Surrey’s Joint Strategic Needs Assessments (JSNAs)
The Joint Strategic Needs Assessment (JSNA) is an assessment of the current and future health and social care needs of the population of Surrey. It supports local leaders and commissioners to make informed decisions and to shape services in a way that best serves their communities. The JSNA informs the Health and Wellbeing Strategy (HWBS) which outlines the collective health priorities for all partners across Surrey.
JSNA chapters that have been used to inform the multiple disadvantage chapter include:
- Housing and related support
- Substance Misuse JSNA
- Emotional and mental wellbeing in Surrey Adults
- Migrant Health Rapid Needs Assessment
4.1.3. Surrey Heartlands Integrated Care System (ICS) Strategy
Integrated Care Systems (ICSs) are partnerships of organisations that come together to plan and deliver joined up health and care services to improve the lives of people in their area. Each ICS has two statutory elements, an Integrated Care Partnership (sometimes known as an ICP) and an NHS Integrated Care Board (sometimes referred to an ICB) – in Surrey Heartlands our ICB is known as NHS Surrey Heartlands.
Surrey Heartlands Integrated Care Strategy sets out priorities for working as a partnership and alongside local people and communities to enable positive health and care for residents of Surrey.
4.1.4. Frimley Health and Care Integrated Care System (ICS) Joint Forward Plan
The Frimley Health and Care system brings together Local Authorities, NHS organisations and the VCSE sector with a clear shared ambition to work in partnership with local people, communities and staff to improve the health and wellbeing of individuals, and to use their collective resources more effectively.
The Joint Forward Plan, signed off with NHS partners in June 2023, is set in the context of their system ambitions and has three objectives to: (1) improve the health and wellbeing of Frimley communities; (2) provide high-quality care to all patients; and (3) ensure healthcare services are sustainable.
4.1.5. Equality, diversity and inclusion (EDI) action plan
The Surrey action plan (2023-2024) sets out five themes: employee experience, leadership, knowing and engaging our communities, communication and engagement, and delivering inclusive services.
Under the theme ‘Knowing our community’, the action plan includes prioritising working with communities to address their needs and maximise local participation. This involves seeking regular updates from VCSEs on community participation work, any key feedback they are gathering, and opportunities for liaison.
The theme ‘Delivering inclusive services’ is pivotal to supporting health inclusion. This action plan emphasises embedding equality, diversity and inclusion (EDI) in commissioning, delivering domestic abuse shelters for underrepresented groups and developing a Community of Practice.
4.1.6. Surrey Homes and Accommodation Summit
The Surrey Homes and Accommodation Summit provides a broad contextual analysis of the commonalities, and shared challenges and opportunities that confront decision-makers and service providers in respect of housing, accommodation and homes across Surrey. During summer 2022, data were gathered from the ONS, from the Department of Levelling Up, Housing & Communities, and from statistical returns prepared by the Districts and Boroughs in Surrey. These data present a snapshot of the situation at that time and upon which, following further engagement and consultation, a Housing, Homes & Accommodation Strategy for Surrey is being prepared. Some of the priority themes that emerged across Surrey were:
- Partnership Working: there is both a desire for greater partnership working across Surrey, and frustration at the unrealised potential in the face of high demand and need.
- Support for Vulnerable Residents: it was felt that “housing is picking up the slack” from a lack of funding or provision for high-needs families or individuals and that problems were being passed around, rather than being resolved in partnership.
Affordability, public sector land, delivery capacity, climate response, and under-occupation and ageing population were also highlighted as priority areas in the NICE guidance on coexisting severe mental illness and substance misuse: community health and social care services indicates that. [59]
4.1.7. Kent, Surrey, and Sussex Reducing Reoffending Plan 2022-25
Reducing reoffending cannot be achieved by working in isolation. Kent, Surrey, and Sussex (KSS) will continue strengthening their relationships with their partners, including police and crime commissioners, the judiciary, and the wide range of skilled and experienced partners who KSS work collaboratively with as members of the local Criminal Justice Boards. Some of the three-year objectives includes having a comprehensive suite of physical and emotional wellbeing resources, expanding the workforce, and increasing psychological consultancy with multi-disciplinary colleagues.
4.2 National policies and guidance
There is a suite of national policies, guidance, resources, and best practice that provides advice for local authorities, commissioners and service providers, healthcare practitioners in primary, secondary and tertiary care, social care practitioners, and for people experiencing multiple disadvantage, including their families, advocates, and the public.
Below are some of the key framework and guidelines relevant to multiple disadvantage.
4.2.1. A national framework for NHS – action on inclusion:
Inclusion Health is a field which seeks to prevent and address the health and social inequalities experienced by groups of people at risk of or living with extremely poor health as a result of poverty, marginalisation, multi-morbidity, and social exclusion. [57]
A national framework for NHS – action on inclusion health states that inclusion health is an umbrella term used to define individuals who are socially excluded, typically experience multiple overlapping risk factors for poor health such as stigma, discrimination, poverty, violence, and complex trauma, and are not consistently accounted for in electronic records (such as healthcare databases). These experiences frequently lead to barriers in access to healthcare and extremely poor health outcomes.
People in inclusion health groups tend to have poor experiences of healthcare services which can lead to individuals avoiding future contact with NHS services and being least likely to receive healthcare despite having high needs. [48]
People belonging to inclusion health groups also tend to suffer from multiple health issues, which can include mental and physical ill health and substance dependence issues. This leads to extremely poor health outcomes, often much worse than the general population, lower average age of death, and it contributes considerably to increasing health inequalities. Inclusion health includes any population group that is socially excluded.
The framework sets out principles for practical action and high impact changes that can be made now to improve access and outcomes for inclusion health groups, recognising that long-term cross sector changes to policy and services are needed to tackle the extreme burden of disease and poor quality of life experienced by people in inclusion health groups.
Principles for action on inclusion include:
- Commit to action on inclusion health.
- Understand the characteristics and needs of people in inclusion health groups.
- Develop the workforce for inclusion health.
- Deliver integrated and accessible services for inclusion health.
- Demonstrate impact and improvement through action on inclusion health.
As part of the framework, NHS England has developed the Inclusion Health Self-Assessment Tool for Primary Care Networks. This online tool helps Primary Care Networks to assess their engagement with inclusion health groups. These are the groups identified as experiencing the worst health inequalities in the UK.
4.2.2. Core20PLUS5 approach (adults) – an approach to reducing healthcare inequalities:
Core20PLUS5 is a national NHS England approach to inform action to reduce healthcare inequalities at both national and system level. The approach defines a target population – the ‘Core20PLUS’ – and identifies ‘5’ focus clinical areas requiring accelerated improvement.
- ‘Core20’ refers to the most deprived 20% of the national population as identified by the national Index of Multiple Deprivation (IMD).
- ‘PLUS’ population groups are identified at a local level. Populations expected to be identified are ethnic minority communities; people with a learning disability and autistic people; people with multiple long-term health conditions; other groups that share protected characteristics as defined by the Equality Act 2010; and groups experiencing social exclusion.
- ‘5’ refers to the five clinical areas of focus which require accelerated improvement: maternity, a severe mental health need, chronic respiratory disease, early cancer diagnosis, and hypertension case-finding and optimal management and lipid optimal management.
- In Surrey Heartlands ICS, their Core20PLUS5 approach mirrors the Priority Populations (including the Key Neighbourhoods) in the Surrey Health and Wellbeing Strategy.
4.2.3. NICE and health inequalities
Health inequalities are differences in health across the population, and between different groups in society, that are systematic, unfair, and avoidable. They are caused by the conditions in which we are born, live, work, and grow. These conditions influence our opportunities for good mental and physical health. [58]
NICE have mapped relevant guidance to various factors that impact on our health. Through a system map of the causes of health inequalities (an adapted Labonte model on place-based approach for reducing health inequalities), NICE highlights where factors that impact health come from and how they interact with each other. It also shows how interventions must focus on treating place, and not just people. NICE’s guidance supports strategies that improve population health as a whole, while offering particular benefit to the most disadvantaged.
4.2.4. Public Health Outcomes Framework
The Public Health Outcomes Framework sets out a vision for public health that is to improve and protect the nation’s health and improve the health of the poorest fastest. The framework focuses on two overarching outcomes OHID want to achieve across the system: (1) increase healthy life expectancy, and (2) reduce differences in life expectancy and healthy life expectancy between communities.
4.2.5. Health Equity in England: The Marmot Review 10 Years On
The Marmot Review 10 Years On highlights how since 2010 life expectancy in England has stalled; this has not happened since at least 1900. The review (2020) highlights how the national government has not prioritised health inequalities, despite the concerning trends and there has been no national health inequalities strategy since 2010.
Reducing health inequalities requires action on six policy objectives:
- Give every child the best start in life.
- Enable all children, young people, and adults to maximise their capabilities and have control over their lives.
- Create fair employment and good work for all.
- Ensure a healthy standard of living for all.
- Create and develop healthy and sustainable places and communities.
4.2.6. Priorities and operational planning guidance (NHS)
The annual NHS priorities and operational planning guidance (2024/25) focuses on the recovery of core services through continuous improvement in access, quality, and productivity, whilst transforming the way care is delivered.
The priorities align with support for inclusion health groups, including people affected by multiple disadvantage. The guidance sets out plans to reduce inequalities in line with the Core20PLUS5 approach and improve access to mental health services so that more people of all ages receive the treatment they need.
4.2.7. Integrated health and social care for people experiencing homelessness, NICE guidance
This NICE guideline covers integrated health and social care for people experiencing homelessness. It provides a set of recommendations on ways to improve access to and engagement with health and social care, and ensure care is coordinated across different services. It also gives advice on how commissioners, planners, providers and practitioners across disciplines and agencies can work together to support and improve outcomes for people experiencing homelessness.
The guideline recognises that more effort and targeted approaches are often needed to ensure that health and social care for people experiencing homelessness is available, accessible, and provided to the same standards and quality as for the general population. It also highlights the value of co-designing and co-delivering services with people with lived experience of homelessness, to improve the quality of health and social care.
This guideline also recommends implementing assertive outreach to better support this population: “assertive outreach is used in some areas in current practice, particularly when engaging with people with complex mental health needs. It takes more practitioner time and may be more expensive, but persevering with people and improving engagement among people who would benefit from support is likely to substantially improve the health and wellbeing of people who have been marginalised, and reduce morbidity and mortality, and associated public sector homelessness costs.”
4.2.8. Discharging people at risk of or experiencing homelessness, GOV.UK
In January 2023, gov.uk, published guidance for staff involved in planning to discharge patients at risk of or experiencing homelessness, or who have no recourse to public funds.
Homelessness is not just about housing. People at risk of or experiencing homelessness often have physical and mental health needs including high levels of frailty, brain injury and disability. These long-term conditions interact with each other (so called ‘multimorbidity’) and are often exacerbated by poverty, psychological trauma, drug and alcohol use, and self-neglect.
The guidance highlights that admission to hospital should be seen as a ‘window of opportunity’ to address these complex needs including obtaining consent for the duty to refer, with a referral form where required and to support a move out of homelessness. Ensuring people get the right support to be safely discharged in a timely manner is important both for them and for the health and care system. It can help individuals rebuild their lives and reduce pressures on health and care services caused by repeat attendance, readmission, and delayed transfers of care. In addition, patients at risk of or experiencing homelessness typically have much longer stays in hospital after they become medically fit than other cohorts. Continuous improvement of the processes around discharge of people at risk of or experiencing homelessness therefore has significant benefits for both the individuals and the wider health and care system.
The guideline recommends that local authority partners should also ensure that people with complex needs receive appropriate care in community settings. This should allow time for health, housing, social care and VCSE services to undertake a comprehensive multidisciplinary assessment of patients’ longer-term needs. [60]
4.2.9. Dame Carol Black Review
In 2019, Professor Dame Carol Black led a two-part independent review of drugs: prevention, treatment, and recovery which was commissioned by the UK Government. Part one was a broad assessment of the evidence on illegal drug supply into the UK and how criminals meet the demand of users, and part two made specific recommendations for improving prevention, treatment and recovery. Dame Carol Black’s review details the extent of the drug crisis in the UK and sets out an evidence-based way forward on drug treatment and recovery.
The review provides recommendations for improvements to all areas of the system and states that a whole-system approach is needed. To move forward, multiple departments (including Home Office (HO), Department of Health and Social Care (DHSC), Department for Work and Pensions (DWP), Department of Levelling Up Housing and Communities (DLUHC) and the Ministry of Justice (MoJ)) must work together to invest in and improve treatment, employment, housing support and the way that people with addictions are treated in the criminal justice system.
4.2.10. From harm to hope: A 10-year drugs plan to cut crime and save lives, GOV.UK
This government policy paper sets out the collective ambition to achieve a generational shift in the country’s relationship with drugs and to reduce overall drug use towards a historic 30-year low. It also plans to reduce the harms that drug addiction and supply cause to individuals and neighbourhoods.
The chronic and entrenched nature of drug use in this country and around the world means that system partners need to take a long-term approach. This 10-year plan is an evidence-based and modern approach to addressing the demand for, and supply of, drugs. This is essential to prevent problems from resurfacing or worsening. The three strategic priorities are: breaking drug supply chains, delivering world class treatment and recovery systems, and achieving a shift in the demand for recreational drugs.
The 10-year plan, in the immediate term, will focus on efforts to combat the supply of heroin and crack cocaine, and on getting those suffering from addiction the treatment and support they need. At the same time, the plan retains a sharp focus on pursuing the illegal supply of all drugs and on delivering high-quality treatment for addiction to other drugs. Investing in the education and resilience of children and young people will also help to level up the whole country, particularly for those families at higher risk of drug use or harm.
Successful delivery of the government’s drugs strategy relies on co-ordinated action across a range of local partners including in enforcement, treatment, recovery, and prevention. The plan highlights that when agreeing the membership of the partnership, organisations should ensure there is appropriate representation of a range of perspectives. As the partnership is to be accountable for delivery of the outcomes in the locality, the Senior Reporting Officer (SRO) should be confident that the membership provides representation from key stakeholders, with appropriate individuals involved who are able to make decisions and hold each other to account.
The following are the minimum key organisations and individuals that should be represented in a Combating Drugs Partnership in England: elected members, local authority officials, NHS, Jobcentre Plus, substance misuse treatment providers, police and police and crime commissioners, National Probation Service, people affected by drug-related harm and the secure estate, such as prisons, young offender institutions (YOIs).
4.2.11. UK clinical guidelines for alcohol treatment
These clinical guidelines were developed with individuals with lived experience of alcohol treatment and recovery and in active recovery organisations. They are relevant to practitioners in any health, social care, or community service working with a person with an alcohol problem.
The guidelines identify priorities for providing high quality alcohol treatment and principles of care that should underpin all support for people experiencing problems with alcohol. These include:
- Alcohol treatment should take place in the context of a recovery-oriented system of care where clinicians, support staff, peers and people engaged in treatment all have roles to play.
- People should be able to access personalised care from any part of the treatment and recovery system.
- A non-judgemental, empathic approach and staff working together with people in treatment is essential.
- Peers and recovery communities can play a central role in supporting recovery at all stages of the treatment and recovery journey.
- Individual treatment and recovery plans should include flexible recovery goals from the start, and the focus on recovery-oriented activities will increase during treatment and after they leave.
4.2.12. UK clinical guidelines for drug treatment
Often called the Orange Book, this guidance (2017) is for clinicians treating people with drug problems. This guidance offers new guidelines on prison-based treatment, new psychoactive substances and club drugs, mental health co-morbidity, misuse of prescribed and over-the-counter medicines, stopping smoking, and preventing drug-related deaths, including naloxone provision.
The guidelines also have a stronger emphasis on recovery and a holistic approach to the interventions that can support recovery.
4.2.13. Coexisting severe mental illness and substance misuse, NICE guidance
NICE guidance on people with co-occurring conditions recommends that people should not be excluded from secondary care mental health services and that a person-centred approach should be adopted to reduce stigma and address inequity in access. [59]
4.2.14. Domestic Abuse Act 2021 Statutory Guidance, Home Office
This statutory guidance is intended to increase awareness and inform the response to domestic abuse. It also conveys standards and promotes best practice.
This statutory guidance is aimed at organisations working with victims, perpetrators and commissioning services, including the police, local authorities, and the NHS. It is also of relevance to organisations dealing with consequences of domestic abuse such as employers and financial institutions.
This guidance highlights the role of individual agencies in identifying and responding to domestic abuse, including assessing risk. It also identifies the responsibility for agencies to work together and share information.
4.2.15. Recovery support services and lived experience initiatives, GOV.UK
Government Guidance on recovery support services and lived experience initiatives is divided into three parts. Part 3: how to develop systems of care that support recovery sets out guidance for local partnership support for recovery support services and lived experience initiatives.
The guidance highlights the roles of local alcohol and drug partnerships in supporting the growth of recovery support services and lived experience initiatives. Stigma, risk aversion and competition can inhibit their development.
This guidance also supports the growth of lived experience initiatives into fully-fledged lived experience recovery organisations (LEROs) that employ staff, manage grants, and deliver services for local authorities.
4.2.16. Working in partnership with people and communities: Statutory guidance (NHS)
The legal duties on public involvement require organisations to make arrangements to secure that people are appropriately ‘involved’ in planning, proposals and decisions regarding NHS services. While involving people and communities is a legal requirement, working with them also supports the wider objectives of integration including population health management, personalisation of care and support, addressing health inequalities and improving quality.
The guidance recommends that ICBs, NHS trusts and foundation trusts:
- Ensure people and communities have an active role in decision-making and governance.
- Involve people and communities at every stage and feed back to them about how it has influenced activities and decisions.
- Understand their community’s needs, experiences, ideas and aspirations for health and care, using engagement to find out if change is working.
- Build relationships based on trust, especially with marginalised groups and those affected by inequalities.
- Work with Healthwatch and the VCSE sector as key partners.
- Use community-centred approaches that empower people and communities, making connections to what works already.
- Have a range of ways for people and communities to take part in health and care services.
- Tackle system priorities and service reconfiguration in partnership with people and communities.
- Services need to work together so people with alcohol problems who also have mental health conditions do not get turned away. People should be able to get help for both conditions in a shared approach.
- Services need to engage and support people from diverse communities. They should co-produce service plans with diverse communities and work flexibly in a culturally sensitive way to do this.
- Learn from what works and build on the assets of all health and care partners – networks, relationships, and activity in local places.
4.2.17. Beyond pockets of excellence
This report shares lessons learned from a collaboration programme that encouraged seven ICSs to explore how they could improve health and care outcomes for people in inclusion health groups. Individuals who are part of inclusion health groups experience extremely poor health outcomes including higher morbidity, comorbidity, mortality rates and low average ages of death compared to the general population.
This programme identifies actions that ICSs could undertake to improve system integration and address health inequalities. [61]
4.2.18. Making Every Adult Matter (MEAM)
Figure 11: Seven principles of the MEAM approach
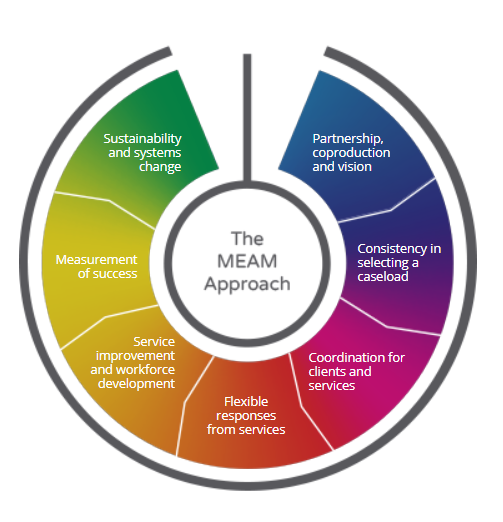
The MEAM Approach helps local areas design and deliver better coordinated services for people experiencing multiple disadvantage. It’s currently being used by partnerships of statutory and voluntary agencies in 42 local areas across England. The MEAM Approach areas consider seven principles (Figure 11), which they adapt to local needs and circumstances. The work starts with partnership, coproduction, and vision – getting the right providers from different sectors, commissioners, and people with lived experience around the table to agree a shared understanding of the problem and a vision for the whole area. They work to create systems change so that services work better for people facing multiple disadvantage in the future.
4.2.19. Making Every Contact Count (MECC)
Make Every Contact Count (MECC) enables the delivery of consistent and concise health and wellbeing information and encourages individuals to engage in conversations about their health at scale across organisations and populations. MECC is an approach to behaviour change that supports the opportunistic delivery of consistent and concise healthy lifestyle information and enables individuals to engage in conversations about their health at scale across organisations and populations.
The fundamental idea underpinning the MECC approach is that it recognises that staff across health and care, local authority and voluntary sectors have thousands of contacts every day with individuals and are ideally placed to support health and wellbeing. The MECC approach encourages health and social care staff to use the opportunities arising during their routine interactions with patients to have conversations about how they might make positive improvements to their health or wellbeing.
MECC have developed an e-learning programme and a toolkit with a wealth of resources that can be used to support the development, implementation, and evaluation of MECC programmes across local communities.
4.2.20. Local Authority Implementation of the Socio-Economic Duty in England
The purpose of this guidance is to support local authorities and combined authorities to voluntarily adopt and implement the socio-economic duty, in partnership with people with lived experience.
Section 1 of the Equality Act 2010 introduces a socio-economic duty on public bodies that requires them: “when making decisions of a strategic nature about how to exercise its functions” to “have due regard to the desirability of exercising them in a way that is designed to reduce the inequalities of outcome which result from socio-economic disadvantage”. Section 1 asks public bodies to consider how their decisions and policies could increase or decrease inequality that results from socio-economic disadvantage. Despite the Equality Act being passed by the UK Parliament in 2010, successive UK Governments have not implemented Section 1 in England. While in April 2018, Scotland brought Section 1 into force as the Fairer Scotland Duty, and in March 2021, Wales brought it into force. [62]
The guide provides a series of practical steps to consider when adopting the duty, drawing on its implementation across England, Wales, and Scotland. In adopting the socio-economic duty local authorities should:
- Formally incorporate poverty and socio-economic disadvantage as a protected characteristic in equality impact assessments, equality plans, and the broader decision-making process and strategies.
- Use a range of relevant data to inform the implementation of the socio-economic duty.
- Ensure strong and visible commitment from senior leaders.
- Recognise the value of engaging with people with lived experience and commit to finding new and sustainable ways to incorporate diverse expertise in policymaking.
- Collaborate with residents, civil society, and voluntary and community sector organisations to build awareness and understanding of the socio-economic duty and people’s lived experience of socio-economic disadvantage.
- Identify what works through monitoring and evaluation, skill-sharing, and innovation.
- Actively consider what more can be done to reduce the inequalities of outcome caused by socio-economic disadvantage.
5. Accessing support
This section explores the services that are currently in place to support Surrey residents facing multiple disadvantage. It looks at national examples of programmes and approaches that provide specialised support relating to multiple disadvantage, as well as a light-touch mapping local services and organisations that directly or indirectly support this cohort.
5.1. Local service provision
For the purpose of this JSNA, services supporting people affected by multiple disadvantage are placed within the following categories:
Type A: services with a specific remit to work with people experiencing multiple disadvantage, for example, Surrey’s Changing Futures Bridge the Gap and Surrey Adults Matter.
Type B: services without a specific multiple disadvantage remit but that tend to work mainly with people experiencing at least one multiple disadvantage challenge, for example, district and borough housing authorities, Mind Matters Surrey (previously Improving Access to Psychological Therapies – IAPT) and the i-access Drug & Alcohol service.
Type C: services that work with people experiencing multiple disadvantage, but this does not make up the majority of their work, for example, DWP, Police, GPs and primary care services, food banks and Citizens Advice.
The below examples provide a snapshot of the key services available to people experiencing multiple disadvantage. This is a nonexhaustive list.
5.1.1. Type A: services with a specific remit to work with people experiencing multiple disadvantage
Surrey Adults Matter (SAM)
Surrey Adults Matter is an initiative set up and run by SCC. SAM was initiated in 2020 to adopt the MEAM approach to work to improve the lives of adults facing multiple disadvantage. Surrey became a MEAM partner area in 2018 and MEAM is commissioned as a support partner for Changing Futures areas. The MEAM approach supports Surrey to build services and systems that can engage with people in a personalised, trauma informed, and strength-based way. It encourages models whereby support workers can sit outside organisational boundaries, build long term trusting relationships with people and provide support that follows people on their journeys with highly skilled outreach staff, small caseloads, and flexible budgets.
SAM uses a ‘Team Around the Person’ (TAP) process which facilitates, liaises, and supports joint working between partner services across the system such as housing services, police, health and social care, probation and the voluntary sector. The approach invites a group of professionals to form a multi-agency forum that can meet at regular interval (via TAP meeting) to share information and assess what support would be beneficial to the person experiencing multiple disadvantage, and priorities keeping the client at the centre where possible. This includes discussing what is going well, what is not going so well, what needs to change or improve and to form an action plan together.
Alongside the focus on facilitating joint working that results from referrals and TAP meetings, SAM provide advice to agencies or service providers to request assessments. In doing so, SAM ensures consent and appropriate records of the TAP meetings for partner reference and use in wider learning (e.g. Subject Access Requests). Clients are an integral part of the TAP and so wherever possible the person being discussed is invited to the meetings and/or an advocate is invited who could be a family member or a trusted support worker. By working with partners, SAM enables flexibility in systems and services and demonstrates a commitment to improve the outcomes for both individuals and services in Surrey.
Changing Futures – Bridge the Gap (BTG)
Changing Futures is a government initiative to achieve better outcomes for people with multiple disadvantage at system, service, and individual levels. The programme is jointly funded through £46 million from the government’s Shared Outcomes Fund with almost £18 million in aligned funding from The National Lottery Community Fund, the largest funder of community activity in the UK. [3] It aims to deliver improvements at the individual, service, and system level:
- To stabilise and then improve the life situation of adults who face multiple disadvantage.
- To transform local services to provide a person-centred approach and to reduce crisis demand.
- To test a different approach to funding, accountability and engagement between local commissioners and services, and between central government and local areas.
Bridge the Gap pilot has been funded by the Changing Futures grant and is one of 15 areas providing a proof of concept initiative to provide innovative ways of working to support individuals with multiple disadvantage.
BTG is a relational model of long-term specialist community outreach, offering up to eight hours of bespoke support to people experiencing multiple disadvantage in Surrey. BTG is provided by trauma informed specialist workers employed through an alliance of Surrey’s VCSE organisations.
There are 12 local charities that form part of the Bridge the Gap VCSE Alliance supporting people experiencing multiple disadvantage these include:
- Catalyst
- Guildford Action
- The Hope Hub
- Oakleaf
- Richmond Fellowship
- Rentstart
- St Peters
- Your Sanctuary
- North Surrey Domestic Abuse Service
- South West Surrey Domestic Abuse Outreach Service
- East Surrey Domestic Abuse Services
- Surrey Domestic Abuse Partnership (SDAP), made up of Your Sanctuary, North Surrey Domestic Abuse Services, South West Surrey Domestic Abuse Services and East Surrey Domestic Abuse Services
Figure 12: Bridge the Gap VCSE Alliance Partner Logos

BTG considers the underlying trauma that someone has experienced in the past and the support provided nurture’s a person’s ability to shape and change their own lives.
BTG focuses upon a person’s strengths rather than their issues and complexities. Taking a trauma informed, strength-based approach, the service sees beyond a client’s presentation and supports them towards their own personal goals. The majority of BTG clients with substance use issues are also living with mental health challenges and chronic long term health conditions. Clients do not have to be abstinent from substances to receive support and the BTG outreach worker can act as an advocate for their client.
Workers are trained to continually assess dynamic risks, offering a service which is risk aware, whilst providing a co-occurring conditions support pathway to facilitate timely and appropriate access to mainstream health services such as primary care, substance use and mental health treatment services at the clients’ pace and request. BTG outreach workers are skilled to offer harm reduction advice, while providing relational support and motivate individuals to engage and benefit from, wider social care support, healthcare, benefits, housing, and other services as well as connecting people with their communities.
Workers take a personalised approach and spend time building relationships before any traditional ‘outcomes’ are achieved. Workers keep small caseloads and shape relationships built on trust and understanding that complex multiple disadvantage takes time to address. BTG continues to support people over time to make positive life changes whilst providing advocacy for their clients and challenging operational and strategic obstacles that present when seeking pertinent support for their clients. When the client is ready the BTG workers will help to ‘pull in’ specialist services at the request and pace of their client. If appropriate and with the client’s consent and wishes, the BTG worker will work with Surrey Adults Matter to assist in seeking support from specialist services for their client. A specialist BTG worker in collaboration with their client, will create a ‘psychological formulation’ with clinical support to create a plan that will help other services understand the client’s story, strengths and hopes. This psychological formulation is used as a tool to ensure that specialist services make ‘reasonable adjustments’ required to be more flexible in meeting the requirements of the client experiencing multiple needs.
High Impact Complex Drinkers (VIA)
This service is for adults with long-term alcohol dependency or individuals that present significant challenges on public services. This contract is delivered by VIA, a London based charity, formerly Westminster Drug Project.
5.1.2. Type B: services without a specific multiple disadvantage remit but that tend to work mainly with people experiencing at least one multiple disadvantage challenge
Surrey and Borders Partnership NHS Foundation Trust (SaBP):
- Mental health: SaBP is the only NHS mental health trust in Surrey. SaBP provides support to improve the mental health of local residents. Some examples of what the SaBP mental health offer includes are: forensic outreach, liaison and diversion service, adult inpatient services, community services, the Surrey Mental Health Crisis Helpline, therapies, Mind Matters, and Safe Havens. Safe Havens provide out-of-hours help and support to people who are experiencing a mental health crisis or emotional distress and their carers. The Safe Havens are open evenings, weekends and bank holidays and also offer an out-of-hours virtual service. The Safe Havens are designed to provide adults with a safe alternative to A&E when in crisis. There are five Safe Havens in Surrey, they are in Aldershot, Epsom, Guildford, Redhill and Woking.
- Substance use: The Substance Misuse JSNA chapter gives an overview of prevention, treatment and recovery services in Surrey. SaBP provide the main drug and alcohol treatment service for adults through i-access Drug & Alcohol Service. The service offers both pharmacological and psycho-social treatment, including individual support, group work and recovery support, screening, triage assessment, outreach, alcohol and/or drug-related information and advice. i-access work in partnership with Via whose focus includes peer mentoring and recovery support. Recognising the need for additional specialist interventions for individuals reaching the age of 18 and requiring ongoing support, the Young People’s Substance Misuse Treatment Service, provided by ’Catch 22 was extended up to 25 years (2019).This is to ensure that the needs of those aged between 18-25, considered to be within the ‘transitional period’ between children and adult services, can be met where they are best suited; i.e. either with an adult service or within the young people’s service.
Adult Social Care (ASC), Surrey County Council: In Surrey, the Substance Misuse Social Care team is co-located and works in partnership with i-access, the substance use treatment provider. The Substance Misuse Social Care team is county wide and comes under the umbrella of Specialist Mental Health Services. ASC Substance Misuse team and i-access have separate responsibilities but are collocated and work collaboratively. This service receives referrals through ASC and work with service users who may not be engaged with treatment services. This is a high activity dedicated team that ensures statutory responsibilities are met within the Care Act and Mental Capacity Act. The responsibilities include social care assessments, meeting eligible social care needs, carers assessments, undertaking reviews, professional working, managing the rehabilitation pathways and managing safeguarding whilst ensuring Care Act compliance. This service is one of the gateway to residential rehabilitation pathways as part of RAP process (Rehabilitation Assurance Process).
Voluntary, Community, and Social Enterprise (VCSE) organisations: Surrey has over 5,700 voluntary, community and social enterprise (VCSE) organisations. The VCSE network in Surrey supports people experiencing multiple disadvantage by providing essential care services such as mental health support, housing and homelessness support, food and material aid. They advocate for individuals’ rights and also foster social inclusion through peer support groups, recreational activities, and person-centred, holistic support.
Hepatitis C Operational Delivery Network: Surrey is one of 20 Operational Delivery Networks in England. The aim of specialised Hepatitis C Operational Delivery Networks for adults is to maximise appropriate uptake and completion of Hepatitis C Virus treatment and to cure more people of infection. Clinics are located throughout Surrey and innovative outreach is provided in the community through a converted ambulance ‘Wilma’.
Harm Reduction Services: Harm reduction services that support residents experiencing multiple disadvantage include: needle and syringe provision, Naloxone provision, and supervised consumption. As at November 2023, there are 75 pharmacies in Surrey providing supervised consumption, 26 provide Needle and Syringe provision, and 16 providing Naloxone. See below:
- Community pharmacies: A number of pharmacies closed in the Surrey Heartlands and Frimley Integrated Care Board areas in 2023 and 2024, including some on the fringes to Surrey which will be utilised by Surrey residents. It is reported by i-access and Luminus that pharmacy closures are likely to negatively impact on service users as individuals may have to travel further and at more expense to access opiate substitute treatment and there is a significant paucity in access to injecting equipment and increasing risk of overdose and Hepatitis C re-infection. A full assessment of the pharmaceutical needs of Surrey residents is in development and is due publication in 2025.
- Needle and Syringe and Naloxone Programmes: Surrey’s Public Health Substance Use Team commission the provision of injecting equipment and Naloxone via Community Pharmacy. Some pharmacies have also signed up to provide Naloxone in injectable and nasal inhalation form. However, there are very few community Needle and Syringe Provision (NIP) services. The Woking Exchange is run by i-access as part of the treatment offer. Guildford Action also provide NIP and were one of the first homelessness day services to provide Naloxone in England with clinical oversight from Dapdune GP Surgery. Guildford Action continues to provide a comprehensive package of Overdose Awareness Training to partners and professionals across Surrey and have provided the highest number of Naloxone kits in Surrey to individuals who inject drugs and support their families and carers as well frontline staff at risk of witnessing an overdose. Naloxone is the emergency antidote for overdoses caused by heroin and other opiates or opioids (such as methadone, morphine, and fentanyl). The main life-threatening effect of heroin and other opiates is to slow down and stop breathing. Naloxone blocks this effect and reverses the breathing difficulties. Local data on historic Naloxone administration by ambulance services in the Chertsey and Guildford areas indicates that 264 patients were given Naloxone doses in 2017 and 2018 calendar years with the majority (93.5%) resulting in an A&E attendance. Although this data only covers a part of Surrey this helps to show the resources needed to treat opiate overdoses. There is currently a trial with Guildford Action to provide inhalation kits to reduce the risk of Blood Borne Virus transmission between people who share crack pipes and if successful this will be rolled out to community pharmacies in Surrey.
- Supervised consumption: SCC Substance Misuse team commission community pharmacies to provide a supervised consumption service for Opiate Substitution Therapy (OST) in the community to more complex and high-risk opiate users. This is prescribed by i-access. Clients who are currently in treatment with i-access can safely be supervised by a pharmacist to take their prescribed oral methadone or buprenorphine and helps to reduce incidents of overdose and prevents controlled drugs from entering the local illegal markets.
Rehabilitation: The ASC Substance Misuse team manage the gateway to residential rehabilitation via two pathways.
- Pathway 1: is the established route for those people who have substance misuse needs and clear eligible social care needs.
- Pathway 2: Rehabilitation Assurance Panel (RAP) is the wellbeing and prevention pathway that was launched to support the drugs strategy agenda. The focus is on wellbeing and prevention to access rehabilitation including community and Surrey residents leaving prisons and returning to Surrey. This RAP model will continue to utilise the assessment skills and expertise within the specialist ASC team but will open the access criteria beyond those eligible under an adult social care assessment for those with low to no social care needs.
GP Provision of Care of the Homeless: All practices are expected to provide those essential and additional services they are contracted to provide to all their patients. This additional level of support in GP practices is commissioned by Public Health and enables more specialised care to be offered above that normally provided through essential and additional services than General Medical Services are contracted to provide. This service aims to:
- Ensure there is enhanced support for homeless people engaging with practices in areas of the county with the highest homelessness and particularly where service provision (e.g. hostels and temporary accommodation) means the need for appropriate primary care for this group is greater.
- Ensure GPs are provided with the knowledge and resources about local service provision and networks to enable them to deal effectively with homeless people’s health needs.
- Ensure GP services are empowered to tackle the health needs of homeless people holistically by working with relevant services (e.g., housing and social services) to integrate homeless people into local communities.
- Encourage provision of outreach sessions in partnership with local service provision and networks to help meet the immediate health needs of homeless persons and encourage them to access mainstream provision.
It is generally recognised that all practices would support a homeless person should they come to their practice, however such occasional support does not automatically entitle a practice to sign up. As of May 2024, 31 GP surgeries out of approximately 122 are signed up to this Public Health Agreement and receive payment.
The service includes the following support provision:
- The development and production of an up-to-date register.
- Liaison with local statutory services and homelessness agencies.
- Awareness of local homeless services and support and signpost patients whenever appropriate.
- Promotion of health services.
- Flexible registration procedures.
- Flexible appointment system.
- Ensure relevant guidelines on the prescription of drugs are followed.
- Ensure all practice staff have a good understanding of and sensitivity towards the particular problems faced by homeless people.
- Appropriate referrals to counselling and psychiatric services where available.
- Assessment of the physical and mental health of homeless people when registering and provision for appropriate and regular screening assessments.
- All practices involved in the scheme should response to the annual review of provision.
The Cabins – Emergency accommodation before and after the pandemic: The pandemic facilitated many new collaborations with partners which included close working relationships being formed between Surrey Public Health’s Multiple Disadvantage Team, District and Borough Housing teams, VCSE Organisations and, ASC Mental Health Team. All partners collaborated to accommodate the needs of the homeless population – the majority of whom have more than one disadvantage. i.e., mental health, behavioural difficulties, drug and/or alcohol problems, victim of domestic abuse and/or contact with the criminal justice system.
One practical provision throughout the pandemic and beyond was a Surrey wide license agreement between Public Health Surrey County Council and the Districts and Boroughs which provided an additional option to local housing teams when someone experiencing homelessness was identified as needing to self-isolate. The agreed license meant whichever borough placed someone in the accommodation would be responsible for moving them on afterwards.
Over the period of this provision (December 2020 – May 2022) three temporary cabin sites, each containing 12 self-contained cabins, were established in Reigate and Banstead, Elmbridge, and Surrey Heath. In Elmbridge and Surrey Heath, the projects were led and managed by Public Health Multiple Disadvantage team in partnership with the Districts and Boroughs. In Reigate and Banstead, the project was led and managed by the housing team and Public Health purchased the use of six cabins. Whilst supported housing and other specialist provision exists within the wider provision, the referrals to the Cabins from December 2020 – May 2022 highlighted that mainstream provision is not always able to meet the needs of people experiencing more complex situations.
The Cabins highlighted a range of benefits and improved soft and hard outcomes for 184 people with multiple disadvantage over an eighteen month period. Soft outcomes are qualitative or subjective changes that may be challenging to measure precisely and often involve personal or behavioural changes, such as improved self-esteem, greater sense of wellbeing and increased confidence. Hard outcomes are quantifiable, objective, and measurable changes that can be directly attributed to a programme or intervention. This or a similar model can provide good results with a range of support and security where needed. This meant the Cabins were increasingly utilised as a more flexible option to ensure people could be supported. As a result of this, there is a plethora of work to look at meeting the actions of the Housing and Related Support JSNA Chapter, including finding appropriate accommodation solutions for people experiencing multiple disadvantage.
Housing First Units: Housing First (Housing First | Homeless Link) is an approach to ending homelessness through housing and support provision. The model is built upon the principle that housing is a human right and prioritises helping people to quickly access stable and permanent housing. Housing First is designed to support people with histories of repeat homelessness, very complex needs, experiences of multiple disadvantage and for whom other services have not been successful in ending their homelessness. The model also provides tailored, open-ended, wraparound support that places emphasis on choice and control by giving rights and responsibilities back to people who may have previously experienced repeated exclusion from services.
Permanent housing is provided without the requirement of being ‘housing ready’ and the support is free from conditions (e.g., sobriety or abstinence is not a requirement), except from the willingness to sustain a tenancy. Furthermore, maintaining the tenancy is not dependent on the tenant using support services.
The Housing First model has 7 principles:
- People have a right to a home,
- Flexible support is provided for as long as it is needed,
- Housing and support are separated: a person’s housing is not conditional on engaging with support,
- Individuals have choice and control,
- An active engagement approach is used.
- The service is based on people’s strengths, goals and aspirations
- A harm reduction approach is used.
Crisis, the national charity for people experiencing homelessness, reported on the University of York’s 2015 evaluation of nine Housing First services. National data collected from 60 Housing First participants showed that:
- 43% reported ‘very bad or bad’ physical health a year before using Housing First, falling to 28% when asked about current health.
- 52% reported ‘bad or very bad’ mental health a year before using Housing First, falling to 18% when asked about current mental health.
- 71% reported they would ‘drink until they felt drunk’ a year before using Housing First, falling to 56% when asked about current use.
- 66% reported drug use a year before using Housing First, falling to 53% when asked about current use.
Since 2010 in England, a growing number of local areas have established Housing First services to meet an identified need. Areas covered in Surrey include Elmbridge, Epsom & Ewell, Mole Valley, Reigate & Banstead, Runnymede, Surrey Heath and Tandridge. National and local Housing First models to date largely demonstrate positive outcomes for people experiencing multiple disadvantage. However, since 2020, Surrey’s delivery of four housing first style units for homeless applicants with complex needs does not meet the demand.
Rough Sleeping Initiative (RSI): The Government published a Rough Sleeping Strategy in August 2018 that lays out their commitment to halve rough sleeping by 2022 and end it by 2027. Work to deliver these aims is built around three core pillars:
- Prevention (understanding the issues that lead to rough sleeping and providing timely support for those at risk).
- Intervention (helping those already sleeping rough with swift support tailored to their individual circumstances).
- Recovery (supporting people in finding a new home and rebuilding their lives).
The Strategy acknowledges that ending rough sleeping will require central and local government, as well as businesses, communities, faith and voluntary groups and the general public to work together to tackle the problem. The strategy identifies six key objectives which emphasise the importance of early intervention and prevention, as well as the development of new affordable housing in helping to meet the need of homeless people:
- The early identification, intervention & prevention of homelessness
- Reduce Rough Sleeping
- Increase accommodation options including social rented, private rented, supported and move on accommodation and in-borough temporary accommodation
- Improve the Health & Wellbeing of homeless people
- Ensuring sufficient support is available for homeless people
- Partnership working
The funding allocated to certain organisations as part of the strategy helps to provide longer term support with housing and accommodation. In Surrey, considerable investment is going into ‘Rough Sleeper Initiatives’. This includes Housing First properties designed to provided accommodation with no preconditions as an anchor from which to address other support needs – such as mental health issues, drug and alcohol dependency and poor overall health.
Domestic Abuse Outreach Services: The Surrey Domestic Abuse Partnership (SDAP) is a group of independent charities who work together across the whole of Surrey to ensure that survivors of domestic abuse, aged 16 and over, are safe and to build a future where domestic abuse is not tolerated. SDAP outreach services offer an independent, confidential, listening service to anyone affected by domestic abuse. They are free impartial services giving practical help and emotional support, as well as providing information on a wide range of issues including housing, benefits, safety planning and the needs of children affected by domestic abuse. They can assist with accessing refuge accommodation if you need to leave your home to keep yourself safe. SDAP’s outreach services provide support to any victim of domestic abuse regardless of age, gender, sexuality or race.
Surrey Steps to Change Hub: The Surrey Steps to Change Hub is a safe space where individuals can benefit from localised, specialist support to increase survivor safety and reduce harm from perpetrators of domestic abuse and stalking.
Sanctuary Scheme: Sanctuary schemes allow survivors of domestic abuse to stay safe in their own homes through making physical changes such as new locks or reinforcing doorways, as well as providing specialist domestic abuse support to help survivors stay safe and understand risk in their wider day to day lives. Sanctuary can take away the onus on survivors that they must move out of their home and instead put the focus on the perpetrator. Sanctuary schemes can also prevent survivors from becoming homeless and offer an alternative accommodation type for survivors for whom a refuge might not be suitable.
For more information on domestic abuse services in Surrey, please visit: Surrey Against Domestic Abuse | Healthy Surrey
5.1.3. Type C: services that work with people experiencing multiple disadvantage, but this does not make up the majority of their work
- Primary care services (NHS England): primary care services refer to the day-to-day healthcare available in every local area and are the first place people go when they need health advice or treatment. It is the first stop for symptoms that are new or for concerns about physical or mental health. Primary care includes GPs (general practitioners), chemists (community pharmacy), community and practice nurses, community midwives and health visitors, family planning or sexual health clinics, out of hours GP services, dental, and optometry (eye health) services and hearing care providers.
- General Practice Integrated Mental Health Service (GPiMHS) is an emotional and wellbeing service for adult patients over 18 years of age who are registered with a GP in any of the Primary Care Network (PCN) areas supported. In Surrey, GPiMHS currently covers a total of 72 GP surgeries out of 91. GPiMHS provides support for difficulties patients may be experiencing such as depression, anxiety, stress, social isolation, problems in relationships, and physical health difficulties. Patients are offered extended consultation times, quick and easy access to practical advice and tailored support for their mental health needs from Mental Health Practitioners or Community Link Workers. The service seeks to ensure that people’s wellbeing and independence is maximised by involving their family, friends and anybody who supports a person in keeping them well. For more information GPiMHS, see this video created by Surrey Heartlands: Transforming community mental health services in Surrey Heartlands – YouTube.
- Citizens Advice Bureau (CAB): Citizens Advice offers free, confidential, independent, and impartial advice to anybody who wishes to use the service. CAB can advise on a range of issues including benefits, work, debt, consumer rights, relationship, and housing matters. i-access has two part time CAB workers offering advice, information, support with benefits and finances.
- Department for Work and Pensions (DWP): The DWP is responsible for welfare, pensions, and child maintenance policy. As the UK’s biggest public service department it administers the State Pension and a range of working age, disability, and ill health benefits to around 20 million claimants and customers.
- Surrey Police: Surrey Police is the territorial police force responsible for policing the county of Surrey in Southeast England. They also support with suicide prevention, harm reduction and county lines.
- Surrey Fire and Rescue Service (SFRS): Surrey Fire and Rescue Service provide fire and rescue services to over a million Surrey residents in addition to the county’s many visitors.
- Local Area Coordinators: A Local Area Coordinator is a skilled and connected worker based in the local community for the local community. Their job is to build relationships and make connections with local people, families, and groups before offering practical help to anyone who may need it for any reason. There are no assessment criteria, thresholds, or time limits. Local Area Coordinators are based in eight key neighbourhoods in Surrey: Woking, Spelthorne, Mole Valley, Tandridge, Reigate & Banstead, Surrey Heath, and Guildford.
- Community Link Officers: Community Link Officers (CLOs) run and join up local engagement learning and problem solving in Surrey. CLOs join in with local events and understand community strengths and how Surrey County Council can provide better support through its services and offers. CLOs are based in each of the 11 District and Boroughs in Surrey.
- Food banks: As at June 2024, this map shows the spread of food banks, community fridges and food clubs in Surrey. There are 57 food banks, a total of 27 community fridges and cupboards and 10 food clubs and community lunches.
6. Primary research and literature review findings
This section describes the results of the thematic analysis of insights from participants across all primary research streams (interviews, surveys and focus groups). These insights have been triangulated with additional, contextual insight provided by our experts by experience (LERO members), and relevant findings from the literature review, to generate six key themes exploring: ways of working, gaps and unmet needs in service provision, service design, barriers to access, strategic challenges, and commissioning models. These findings, along with insights from the literature review and secondary data reviews reported in Sections 2 to 5, inform the recommendations in Section 7 of this JSNA chapter. Full research methods are reported in Appendix 3.
A total of 156 research participants took part in either in-depth interviews, in-person surveys and focus group discussions for the purpose of this JSNA chapter. In addition, 100 responses were received by to an online survey, some of the survey respondents also took part in the above-mentioned primary research activities. Research participants include service providers, frontline staff, outreach staff, practitioners, health and care partners, system leaders, service users with living experience of multiple disadvantage, members of the LERO, and all stakeholders working to support people experiencing multiple disadvantage or one of the multiple disadvantage core risk factors in Surrey.
Qualitative research provides a rich source of information, with a focus on uncovering the deep, human insights that are fundamental to understanding the challenges faced by people experiencing multiple disadvantage. Some of the findings are hard-hitting and may challenge partners, but they reflect the feedback from participants. The aim of reporting these findings is to help key decision-makers across Surrey to better understand the needs of people experiencing multiple disadvantage and take action to improve the lives of this population group.
A note on reflexivity and positionality:
The primary research was led by the JSNA Lead Author with the support of the LERO. Four experts by experience from the LERO conducted interviews, either 1:1 or with the support of the JSNA Lead Author or Lived Experience Project Manager as requested. Some of the primary research activities, predominantly the in-depth interviews and focus group discussions, were also supported by the JSNA Project Manager and 5 members of the SCC Public Health team. The LERO and the JSNA Chapter Delivery group supported with the thematic analysis and triangulation of findings. The above individuals make up the research team for this chapter.
The research team took a reflexive approach to thematic analysis of qualitative data. [77]. This means the themes presented are understood to represent the research team’s interpretation of patterns within the data. This interpretation is inherently and unavoidably influenced by the context within which data collection, analysis and write up was undertaken.
For the purpose of this JSNA chapter, the primary research was undertaken with the aim of understanding the needs of adults in Surrey experiencing multiple disadvantage, with a specific focus on making evidence informed recommendations for cross-system improvement. All members of the research team are passionate about building on the foundations of the hard work of system partners to support sustained improvement of the outcomes and experiences of people experiencing multiple disadvantage in Surrey.
With this shared goal in mind, the JSNA Chapter Delivery Group and members LERO were driven throughout the research process to generate clear, actionable and evidence-based insights from the data to help guide service development. The questions asked to participants, and themes presented, therefore reflect this laser focus on identifying areas where improvements can be made, whilst centring the voices of those with lived or living experience of multiple disadvantage.
This does not negate nor undermine the areas of best practice which system partners continue to deliver. Rather, it provides one part of the evidence-base needed to inform meaningful quality improvement. The JSNA Chapter Delivery Group and LERO also reflect that the primary research themes presented are based on a cross-sectional snapshot of a sample of people in Surrey experiencing multiple disadvantage, and those involved in supporting them (directly or indirectly). As such, the final recommendations presented in section 7 are based not just on these primary qualitative insights, but also on the crucial insights from the literature and secondary data analysis, which combined, paint a richer, more holistic picture of the needs of people experiencing multiple disadvantage in Surrey.
6.1. ‘Ways of working’: avoiding silos and fragmented care
This section explores ways of working in Surrey, including pockets of siloed working, organisational relationships, and system collaboration. The research findings reflect the importance of a ‘whole system approach’ to multiple disadvantage to help improve outcomes for this population. The primary research suggests that some statutory services are geared up to ‘assess’ and ’treat’ an individual’s assumed primary need and do not always recognise the interconnected nature of multiple disadvantage. This section also presents evidence exploring the suggestion from some primary research participants that Surrey’s voluntary and community organisations and local community assets can sometimes feel that they are left holding the most vulnerable and high-risk clients, with some also noting the need for further efforts to ensure the sector is valued as an equal system partner.
6.1.1. Siloed working as a risk factor for poor quality and fragmented care
Background and insights from the literature:
Literature on systems change for people experiencing multiple disadvantage reflects how “siloed working and poor information sharing mean that relevant information is often not passed between services”. [66] This is further supported by some research participants who reported that people facing multiple disadvantage often experience fragmented care as a result of pockets of siloed working and navigating care from multiple services across the system. Fragmentation can lead to a limited coordination between services across all levels – from frontline, to commissioning, and strategic planning. Participants reflected that these pockets of siloed working can result in people experiencing multiple disadvantage falling through the gaps between services or presenting in crisis, and make it difficult for individuals to access the comprehensive support they need. Considerations including informed consent, data protection and governance policies are important when sharing information appropriately between services.
Surrey-specific primary research insights:
In Surrey, statutory support services are typically organised into silos, whereby each provider specialises in meeting one primary need e.g., a substance use, mental health, or housing need, which can create barriers to integrated care. Participants explained this can be challenging for individuals facing multiple disadvantage:
“The big challenge we have is that is that our services are so siloed and for people with multiple disadvantage, that’s the sharp end, that’s what makes it so difficult for them.” (Interview IP58, person supporting people with lived experience of multiple disadvantage)
“Despite an array of extra services over the years, it often feels like agencies work in silos more than ever. There has been a drive to meet targets rather than individual need.” (Interview IP06, person supporting people with lived experience of multiple disadvantage)
Literature suggests that working in silos can have a range of impacts on service delivery and how services can effectively and holistically address an individual’s needs. Potential impacts of siloed working in Surrey identified by interview and focus groups participants, include:
Ineffective joint working: Siloed working can act as a barrier to effective joint working by hindering the delivery of integrated care and shared ownership of the multiple disadvantage agenda. Primary research findings suggest that joint working and communication could be improved in Surrey, as one participant highlighted:
“Joint working, just like communication between services is so important and yet it just doesn’t happen” (Interview IP54, person supporting people with lived experience of multiple disadvantage)
Another participant referred to the joint working approach as:
“us and ours, not you and yours” (Interview IP57, person supporting people with lived experience of multiple disadvantage)
highlighting the importance of an integrated and unified system that holds shared ownership of multiple disadvantage and associated barriers, challenges, and solutions.
Duplication of efforts: One participant shared an example from their line of work which they believe demonstrates duplication of efforts, explaining that SCC currently provides a Tenancy Support Programme which duplicates the support offered by the Districts and Boroughs. The participant reflected that this duplication may not be an efficient use of resource and capacity, has the potential to hinder a smooth and streamlined process, and is not consistently trauma informed as individuals frequently must re-tell their story to various services. (Focus group FG03, person supporting people with lived experience of multiple disadvantage)
Resistance to change: Silos can become entrenched over time, leading to resistance when attempts are made to break down barriers and encourage collaboration. When commenting on factors that may have the potential to prevent or hinder change at system or service level, one participant reflected that:
“what could hinder it is a resistance to change things […] historically this is the way we’ve always done things so I think there will be a huge culture shift in thinking and that could hinder things, but it may be positive thing too. Organisational beliefs as well, they’re all different across the system. And reducing the bureaucracy and allowing more of a free flow of working together.” (Interview IP15, person supporting people with lived experience of multiple disadvantage)
Organisational competitiveness: Limited funding and resources for organisations supporting multiple disadvantage can lead to intense competition for grants, donations, and government funding. [33] Some participants identified this competitiveness mostly within the VCSE sector, with many organisations feeling the need to “fight to survive” due to limited financial support and competition. They reflected that this competition may result in some organisations securing more resources than others, while others struggle to meet their goals:
“it is difficult to steer away from siloed working due to the fear of losing funding. There is a competitiveness between some organisations, with the sense that they need to compete for funding” (Interview IP49, person supporting people with lived experience of multiple disadvantage)
Commissioners adhere to procurement legislation. Legislation ensures public money is spent properly and that services are safe and accountable. Statutory and non-statutory providers compete with each other and bid for funding. Providers should be able to evidence factors such as financial viability, appropriate governance structures and data collection infrastructure.
Perceived hierarchy: Primary research findings also indicate that some system partners feel there is currently a culture where an assumed hierarchy exists, with some participants from the third sector expressing a perceived authority of other partners over VCSEs. One participant explained:
“The third sector do not have many of the restrictions our statutory partners do but there is still a lack of understanding about what we can and cannot provide. I would love to see the sector given the same value as statutory services as it still feels very there is a hierarchy with us at the bottom.” (Interview IP06, person supporting people with lived experience of multiple disadvantage)
Navigating the system: Some service users reported having negative experiences of health and care support as a result of siloed systems, often moving between different services, experiencing long waiting times, or being excluded from services as they interact with various parts of the system that operate in distinct ways. This is illustrated by the reflection of one expert by experience who reflected on their referral to a Community Mental Health Recovery Service (CMHRS) when they became unwell with their Bipolar Disorder:
“due to the waiting time I usually am able to get better independently before I am seen by the CMHRS. By the time I see the CMHRS I present as fine and I am discharged back to my GP. This has happened on a number of occasions. I am fortunate that I have insight and awareness knowing what makes me better but I feel if others face the similar experience of waiting so long that they actually get better or so long that they actually get worse then this could be detrimental.” (Interview LERO, expert by experience)
Another expert by experience shared their experience of supporting family members experiencing multiple disadvantage with referrals, stating:
“In my own experience, having referred my partner using crisis referral she saw 6 different services before reaching the right one.” (Interview LERO, expert by experience)
Interpretation and implications:
A ‘Whole Systems Approach’: Considering the risks associated with siloed working reported in this section, a whole-systems approach should be considered for Surrey. This approach requires strategic leadership at each area level, including place leadership, local authority leaders, health commissioners, statutory agencies, voluntary sector organisations, and individuals with lived and living experience.
Taking a ‘Whole Systems Approach’ to addressing multiple disadvantage encourages decision-makers, services providers, and service users to work together to improve access to support for people affected by multiple disadvantage. This includes considerations of how decisions and changes made in one part of the system may affect outcomes of another. Services should work together, learn together, and treat people as individuals with accountability and ownership of support shared across the system. Encouraging people to work together, have open, honest conversations and hold each other respectfully to account will facilitate the delivery of effective support for people affected by multiple disadvantage. [34]
6.1.2. Organisational relationships, collaboration and delivery of integrated care
Background and insights from the literature:
In Surrey, many statutory services that support people experiencing core multiple disadvantage risk factors have evolved to ‘assess’ and ‘treat’ only one primary need instead of delivering an integrated approach. As a result, individuals experiencing co-occurring mental conditions and multiple disadvantage sometimes face challenges in receiving integrated care.
A common example of a co-occurring condition is an individual experiencing a mental health need at the same time as substance use. Co-occurring conditions are also commonly referred to as co-morbidity(ies) or dual diagnosis. Dual diagnosis is defined as a severe mental health need combined with use of substances whereas comorbidity generally refers to when a person has more than one disease or condition at the same time. These challenges are often interconnected and cyclical in nature, for example, an individual may turn to substances as a way to cope with mental health symptoms, but substance use can exacerbate mental health symptoms, leading to an ongoing cycle. The Baseline Evaluation of the National Changing Futures Programme identifies that there is a high degree of overlap between mental health and drug and alcohol problems – almost seven out of ten participants have experience of both.
Failure to identify a person affected by co-occurring conditions and/or multiple disadvantage early on has the potential for increased crisis presentations and healthcare costs due to frequent hospitalisations, A&E attendances, and long periods of time bouncing between various treatment services. [62] For some services, systems are in place to identify individuals experiencing co-occurring conditions or multiple disadvantage, where collaborative assessments are carried out. Supporting a person affected by a co-occurring condition often requires progressive, bespoke and integrated healthcare approaches. Guidance from Public Health England on commissioning services for people with co-occurring conditions is based on the principles that mental health and substance use services have a joint responsibility to meet the needs of individuals, and providers should have an open door policy. [35] This guidance is outlined in SaBP’s Dual Diagnosis Policy. Drug and alcohol use should not be automatic exclusion criteria for accessing mental health services, in fact it is pivotal that drug, alcohol and mental health services work seamlessly together to ensure access to more specialist services.
Surrey-specific primary research insights:
One research participant suggested there may be misunderstandings around the provision of an integrated for people affected by multiple disadvantage and co-occurring mental health and substance use conditions:
“i-access are claiming ‘we’re integrated with them, and we all work together’ and then they’re saying, ‘oh hang on a second, no, we’re different’. So, there’s a lot of mistrust and misunderstanding across the system which is part of the multiple disadvantage challenge…. I think they [organisations] are finding it really hard to admit and say what and where there are issues” (Interview IP03, person supporting people with lived experience of multiple disadvantage)
Insights from the primary research suggested that stakeholders working within mental health and substance use services may hold differing views due to various factors, including:
- Differing treatment offers: for example, mental health services may focus on psychotherapy, diagnostics, and prescribing, while substance use services often include behavioural interventions and support groups.
- Service thresholds and criteria: individuals experiencing multiple disadvantage may face exclusion from service as a result of their co-occurring needs. Services must work together to take responsibility for supporting clients experiencing a combination of challenges.
- Systemic issues: mental health and substance use services are commissioned through different funding streams, however, primary research identifies that there remains examples of disconnect regardless of both services being commissioned to the same provider (Surrey and Borders Partnership – SaBP).
These disparate views are evidenced by quotes from research participants, who shared several examples of limited collaboration in statutory services, often in relation to tensions between mental health and substance use services:
“There seems to be a sort of lack of flexibility about working together, so mental health will say ‘you need to sort out substance misuse’. Substance misuse say, ‘they’re not engaging, so we can’t help them, they need to go back to mental health’ and it’s kind of hard. We need to kind of pull together those substance misuse and mental health to support people better.” (Interview IP64, person supporting people with lived experience of multiple disadvantage)
“I’m embarrassed to say that all mental health services often say, ‘Well, have you got autism?’ or ‘We can’t really progress with your mental health need if you got alcohol abuse or drug dependency, we can’t really support you’. And then the drug and alcohol services say, ‘Well, we can’t support you if you’ve got autism or a mental health need’. … How often do you think it is that someone with a mental illness doesn’t then have a or an autism or a drug and alcohol comorbidity? It is actually quite rare.” (Interview IP62, person supporting people with lived experience of multiple disadvantage)
“Our clients just don’t ever seem to meet any criteria, they’re the last to be supported. They’re told ‘you’ve got to deal with your substance use before your mental health’, but the reality is for a lot of people that their mental health is the reason that they’re using. You know, there’s an addiction in there that’s come from some sort of trauma.” (Interview IP49, person supporting people with lived experience of multiple disadvantage)
Interpretation and implications:
Examples of poor communication, as demonstrated by the above experiences, result in gaps in the delivery of integrated care. The research indicates that these often repeated experiences of services excluding individuals and discharging people when still in need of support, are potentially retraumatising for individuals and are likely to increase an individual’s feelings of hopelessness and mistrust in services. The Homeless and Inclusion Health Barometer (2024) supports similarly identifies services’ inability to meet complex needs as a significant barrier to care, a study respondent interviewed as part of the Barometer said: “Anyone with complex needs homelessness, substance misuse, mental health, physical health really struggles to access services. They are told by social services that their support needs are too high, by mental health that they need to be in recovery, and they usually wait to seek treatment for physical health until it is a severe need. Equally when these clients access hospitals- staff are dismissive, don’t understand substance misuse adequately and just add to a lifetime of experience of services working against them.”
6.1.3. Multi-agency approaches in Surrey:
Background and insights from the literature:
Multi-agency working involves different organisations or professionals from various sectors working together to collaborate and achieve common goals. Multi-agency working enhances communication, prevents duplication of services, and enables the sharing of resources, skills, knowledge, and information which can lead to more efficient and effective service delivery.
It is important that services supporting people experiencing multiple disadvantage involve the individual and remain person-centred. Team Around the Person (TAP) meetings and Community Harm and Risk Management Meetings (CHaRMMs) are two examples of multi-agency working taking place in Surrey. Their approaches are discussed below:
Team Around the Person (TAP) meetings: TAP meetings have been an integral part of the Surrey Adults Matter (SAM) model since April 2020. TAP meetings allow a space for services involved in supporting the client to meet collectively to decide on support pathways and next steps. The person being discussed is invited to take part and is sometimes accompanied by an advocate or family member. Partnership Leads will invite the referrer, the client, any family member, or advocate the client would like to be present to a TAP meeting, in addition to all professionals who are working with the client or whose expertise is required. This is done with the consent of the client. A typical TAP meeting might include a Social Housing representative, Probation Officer, Drug and alcohol support, Adult Social Care, Police, Healthcare providers, the client, and the client’s advocate / family member or support worker.
Following discussion and consent, whilst always invited, clients may not always attend a first meeting but in subsequent meetings can choose to attend all or part of a meeting and be on or off screen for virtual meetings as they wish. Some clients choose to attend all or some of the meetings, others are happy for their keyworker or advocate / family member to attend on their behalf. There is no pressure on them to join if they give consent for the meetings to take place and know they have an opportunity to make comment and receive the minutes / feedback. TAP meetings will be held according to the needs of the client and so frequency varies significantly with meetings ranging from weekly to being several months apart. The TAP approach is used to support where clients may require robust risk management plans, specialist professional input, or more frequent weekly meetings. Other clients may be supported with less frequent 6-weekly meetings. An underlying principle of TAP is being as flexible as possible to meet the needs of the clients and service professionals involved. Professionals that are engaged in TAP are supported and encouraged to try and adopt strengths-based and trauma informed approaches.
As part of the TAP meetings, minutes are recorded which can contribute to Subject Access Request (SAR) reviews and be used in different capacities to inform decision-making in respect of a client for example, housing decisions, Domestic Homicide Reviews (DHRs) and Police enforcement action to safeguard vulnerable clients.
Feedback received from social care and mental health teams highlights “how valuable it is to have space where we can all come together as different agencies and discuss people.” (Interview IP64, person supporting people with lived experience of multiple disadvantage) TAP meetings can be very successful in bringing services together, however, managing a balance of power in these spaces can be challenging.
Community Harm and Risk Management Meetings (CHaRMMs): CHaRMMs are local delivery groups led by Community Safety, that bring together professionals from key local agencies (both statutory and voluntary) to work together, in partnership, to tackle crime and disorder in their localities and deal with individuals of concern. CHaRMMs will discuss and agree action to reduce the negative impact that individuals and families have on Surrey’s communities through their anti-social behaviour (ASB). Using the expertise that exists on this multi-agency group, members will share information on referrals, and incidents, and put in place appropriate risk management and disruption plans to address the behaviour of the perpetrator and reduce the negative impact on victims.
One research participant mentioned that CHaRMMs allow partners “to work in a multi-agency approach to be able to identify issues and to solve them without having to wait until it has to be reactive.” (Interview IP14, person supporting people with lived experience of multiple disadvantage)
Multi Agency Risk Assessment Conference (MARAC): A Multi Agency Risk Assessment Conference (MARAC) is a regular local meeting to discuss how to help domestic abuse survivors, aged 16 or over, at high risk of murder or serious harm. Each agency signed up to MARAC has a representative who attends meetings and is responsible for the actions of their agency. MARAC runs alongside other multi-agency assessment processes. Domestic abuse specialists, police, children’s and adults social care, health and other relevant agencies all attend. They talk about the survivor, the family and perpetrator, and share information. The meeting is confidential. There are six MARAC meetings regularly held in Surrey. Between them, they cover the geographical area of Surrey: Surrey Heath and Woking, Guildford and Waverley, Tandridge, Mole Valley and Epsom, Spelthorne, and Reigate and Banstead and Ewell.
Surrey-specific primary research insights:
Through the primary research conducted for this JSNA chapter, some services report positive experiences of multi-agency meetings as providing spaces to wrap support around those experiencing multiple disadvantage, especially if they are particularly vulnerable and safeguarding risks are high. However, some participants suggested that some multi-agency style models still feel very “done to” to the client rather than “done with” or “done by” the client:
“You’ve got someone that’s chairing the meeting that’s trying to get you to all go down their way of thinking rather than the clients. It’s not trauma informed. You have you’re say and then you’re beaten down. It’s appeasing the services rather than the clients.” (Focus group FG03, person supporting people with lived experience of multiple disadvantage)
6.1.4. Voluntary and community organisations are an equal system partner in supporting people facing multiple disadvantage
Background and insights from the literature:
Voluntary, community and social enterprises (VCSEs) and local community assets play an important part in supporting service users who fall through the gaps in provision. VCSEs hold a wealth of experience and expertise in supporting people affected by multiple disadvantage and many have built trusted and long-term relationships with individuals, are embedded in the community, and have flexibility to find creative and innovative solutions. As such, statutory bodies should ensure that VCSEs are consistently involved as an active part of workstreams, with mechanisms built to enable this. [38]
Surrey-specific primary research insights:
Some research participants highlighted the need for individuals with lived experience of multiple disadvantage, as well as local communities and VCSEs, to drive the way commissioning is structured and funded. This would include involvement in the identification of commissioning models for this population, in addition to the co-production of funding structures, service design and service specifications. Commissioners go through a robust process of needs assessments, stakeholder engagement as part of the commissioning process. However, one research participant commented that commissioners could be better informed about areas of needs and gaps prior to decision-making:
“Commissioners don’t always have the knowledge or don’t have the experience to be able to commission some of the service work.” (Interview IP16, person supporting people with lived experience of multiple disadvantage)
This sentiment was echoed by members of the LERO who emphasise the importance of relevant training for commissioners working in commissioning for multiple disadvantage.
Some research participants commented on the perceived blocks around statutory support, stating:
“We’re just finding that statutory services aren’t responsive in the way that we need them to be because presumably they are understaffed and oversubscribed.” (Interview IP55, person supporting people with lived experience of multiple disadvantage)
“It’s about going to where people are rather than them having to come and find where you are.” (Focus group FG06, person supporting people with lived experience of multiple disadvantage)
Some participants observed that the responsibility to provide continuity of support after individuals are discharged from statutory services is thus being pushed on to the VCSE sector. As one participant commented:
“We often hear from statutory agencies that ‘they’re [the service user] too extreme’. So, what happens? We end up still holding them, cause we’re not going to let them go. So, we’re the people who aren’t the experts, but we’re holding them cause the actual experts are saying ‘they’re too tough for me’. I mean, that’s really wrong.” (Interview IP17, person supporting people with lived experience of multiple disadvantage)
Many research participants (including both service delivery stakeholders and service users) felt VCSE staff have a good understanding of multiple disadvantage and how best to support and work alongside an individual. Some research participants said that the provision of assertive outreach – whereby the provider meets the service user where they are at, works at the pace and time the individual decides, and fosters positive relationship building and trust – is more common with VCSEs than in statutory services, which were felt to typically expect service users to come to them to access support:
“I think the only services that meet the needs of these individuals are the voluntary services…they are holding the most complicated, risky kind of individuals … I think the only people really who go out and do assertive outreach are the voluntary sector. I suppose their governance structure is less, should we say less claustrophobic? They’re able to be flexible, they’re able to meet the demand, they’re able to support drop-ins, they’re able to have that time to create those relationships, which is so important to the work that we do. I just think they are just more tooled up to meet individuals needs and coordinate that for them.” (Interview IP01, person supporting people with lived experience of multiple disadvantage)
However, some participants felt strongly that VCSEs should not be supporting the most vulnerable service users. Although they recognised that VCSEs have a good understanding of multiple disadvantage, some participants suggested that many professionals working in these voluntary organisations may lack the specialist skills needed to support the unique challenges facing clients experiencing multiple disadvantage (i.e., they are not mental health or substance use specialists, for example). One participant shared their perception of VCSEs supporting multiple disadvantage:
“The voluntary and community sector is seen as cuddly and fluffy, doesn’t really deal with the issues, doesn’t have the skills and the letters after names that we have in the statutory sector so it’s not as good.” (Interview IP03, person supporting people with lived experience of multiple disadvantage)
Regardless, the approach and support of VCSEs was highlighted by participants as indispensable, who noted it should be valued, particularly in relation to their ability to engage with and open up the option of support to people who need help, with VCSE staff afforded equal access to upskilling and training opportunities. The participant continued:
“Absolutely some of the workers that we have are not mental health social workers, they’re not clinicians, they’re not experts in substance misuse but they are experts in engaging with people, getting alongside them and enabling them to be open to the support that they need and I think that the system is not valuing that.” (Interview IP03, person supporting people with lived experience of multiple disadvantage)
Figure 13: Word cloud of key words describing ‘What makes a good service?’ Source: Primary research with member of the LERO
The adjacent word cloud illustrates the key qualities and values identified by members of the LERO in response to the question: ‘What makes a good service?’
Primary research suggests that across Surrey, VCSEs supporting people experiencing multiple disadvantage have a strong understanding of what it means to be affected by multiple challenges simultaneously. Many outreach workers have their own lived experience, which helps with their understanding of both multiple disadvantage and the roots of trauma.
Some research participants felt this understanding was lacking in some statutory services that support people experiencing core multiple disadvantage risk factors and at a system-wide level due to a range of factors such as the culture, training, and structural challenges:
“I would say there is a far, far better understanding from voluntary services than there is from statutory services… statutory services are obviously huge institutions and there is a culture set from the top. Often that culture trickles down and it almost takes years to unpick. Whereas in the voluntary sector, our teams are much smaller, the culture really comes from the individuals who are delivering the work. So, it’s much more of a shared approach rather than a ‘Top-Down’ approach.” (Interview IP06, person supporting people with lived experience of multiple disadvantage)
“In terms of a system-wide level, I don’t think there’s breadth or depth in that level of understanding and I think that’s therefore why people with multiple disadvantage face the barriers that they do. Some of it is structural and some of it is about levels of training and awareness, and some of it I think can be tackled at an individual, personal level in terms of the workforce, but some of it is I think also is kind of inherent in the system.” (Interview IP07, person supporting people with lived experience of multiple disadvantage)
6.2. ‘Feeling abandoned’: identifying gaps in service provision
This section explores evidence of gaps in the availability of effective and suitable support services for people facing multiple disadvantage in Surrey. The primary research and supporting literature suggest this is a significant challenge that often compounds difficulties and barriers experienced by these individuals, leads to worsened health outcomes, and contributes to the persistence of health disparities and cycles of poverty and inequality.
Mental health plays a key role in overall wellbeing and quality of life; however, our research indicates that the limited availability, accessibility, and flexibility of mental health support in Surrey for people experiencing multiple disadvantage often intensifies mental health challenges for these individuals.
This section also discusses evidence showing housing and accommodation support in Surrey is not able to meet current need, with gaps in provision for people experiencing multiple disadvantage. Housing should be considered as a priority and primary need for people experiencing multiple disadvantage prior to engaging in treatment services. However, the evidence reported here shows that the current lack of housing both nationally and locally means many individuals are homeless or living in inappropriate and unsuitable accommodation.
We know from the literature that many people facing multiple disadvantage will have experienced early life trauma and adverse childhood experiences; as such, early intervention and prevention are vital long-term solutions to responding to trauma and identifying risk and support earlier. Our primary research aligns with evidence from the wider literature that improving intervention and prevention approaches at all stages of the life course is crucial to reducing the incidence and impact of multiple disadvantage in Surrey.
Surrey-specific primary research insights:
We surveyed 100 service providers supporting people experiencing multiple disadvantage in Surrey; organisations shared information on the types of services they offer, the population groups they support, and the extent to which they agree or disagree that current provision sufficiently meets the present need. Around three in five respondents agreed that current service provision sufficiently meets the needs of people experiencing multiple disadvantage, with 28% of respondents disagreeing with this statement.
Figure 14: Stakeholder Survey – Extent to which service provision meets the needs of people experiencing multiple disadvantage (Base Size:100)
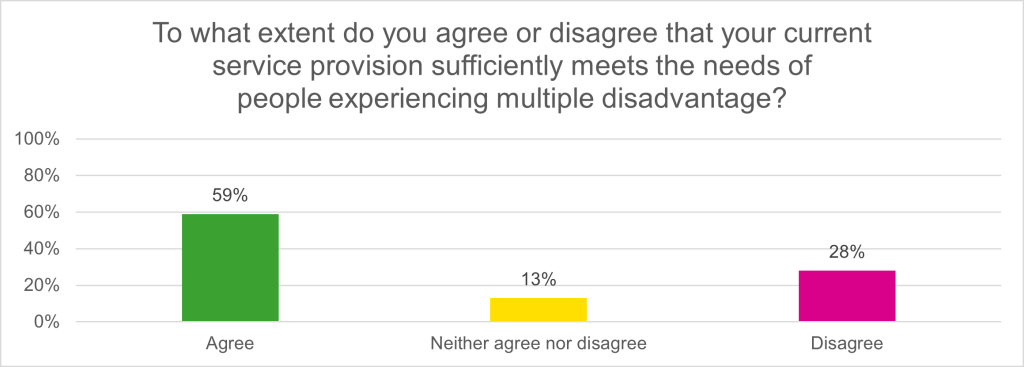
However, insights from the qualitative surveys with service users and insight from the LERO experts by experience however, suggest there is a mismatch between service user and service provider perception of the extent to which services meet needs.
6.2.1. Limited access to mental health services intensifies mental health challenges for people experiencing multiple disadvantage
Background and insights from the literature:
People experiencing multiple disadvantage often have a high need for mental health support, with mental health playing a key role in overall wellbeing and quality of life. [9]
Surrey-specific primary research insights:
Mental health services in Surrey were identified by research participants as a major sticking point, with limited access to support often leading to an exacerbation of mental health challenges. Many research participants reported believing the mental health support system in Surrey is broken:
“The one thing that would improve Surrey immeasurably is sorting out the mental health… There’s not enough staff. There’s not enough infrastructure. It doesn’t work. The whole thing’s broken.” (Interview IP17, person supporting people with lived experience of multiple disadvantage)
Some of the key challenges to mental health support service delivery in Surrey identified by research participants include:
Availability of support: Participants highlighted a need for increased availability of mental health service options with less stringent thresholds for people experiencing multiple disadvantage and mental health needs. For example, some participants reported there are limited “low-level” support options for people experiencing multiple disadvantage and mental health conditions such as depression and anxiety, eating disorders, and personality disorders, and often people experiencing this type of mental health need do not typically meet thresholds for support. Likewise, some participants felt drug and alcohol use should not be automatic exclusion criteria for accessing mental health services. As one participant identified:
“Where do personality disorders go? Where does your anxiety go? Where does depression go? Because you know, whilst they’re not classed as ‘severe and enduring’, sometimes those mental health conditions can be absolutely debilitating, and people need help and I’m still struggling to try and find a service that actually fits them.” (Interview IP52, person supporting people with lived experience of multiple disadvantage)
Ease of access: Frontline providers and outreach workers reported challenges in primary health care registration, including their clients being refused in some locations (e.g., GP registration). GPs are often the first point of contact for people in need of a referral to secondary mental health care such as psychological wellbeing services, Community Mental Health Recovery Services (CMHRSs) or Crisis Resolution and Home Treatment Teams (CRHTs). One member of the LERO stated:
“If I’d got accepted onto the mental health years ago, I would have been in such a much better place” (Interview LERO, expert by experience)
For many people with a mental health need, delayed intervention may result in the progression and exacerbation of mental health symptoms.
Suitability of assessments: A mental health assessment is when a professional, such as a psychiatrist or psychologist, meets an individual for a consultation to explore whether there is a mental health need and what type of treatment is required. Feedback from primary research participants indicated that assessments for mental health services are often unsuitable for people experiencing multiple disadvantage, with assumption-based questions or questions that oversimplify complex issues which can result in exclusion from services. One service provider shared:
“I’ve been to mental health assessments with clients, and they’ve gone out so depressed because they’re not listened to. There isn’t the time or perhaps even the will sometimes, or the expertise. It’s a bit of a conveyor belt.” (Interview IP55, person supporting people with lived experience of multiple disadvantage).
Links with community mental health services: Some frontline providers expressed that they do not think there are sufficient links to Community Mental Health Teams, with others identifying a lack of flexibility and person-centred approach in community mental health. VCSE staff in particular reported feeling that they are holding clients in their service, for example, in a refuge or supported accommodation, or sending clients to A&E due to challenges they have as service providers in accessing CMHRS support. One research participant stated:
“There’s just a lack of support available from the Mental Health Trust in terms of the Community Mental Health Recovery Service, I think they just haven’t got enough staff.” (Interview IP59, person supporting people with lived experience of multiple disadvantage).
Frontline staff expressed that they would like a direct connection to CMHRS in order to discuss cases and put appropriate support in place in a timely manner.
Presentations of individuals with neurodevelopmental conditions: One research participant who is a subject matter expert shared how currently mental health services in secondary care are built around serious mental health needs such as schizophrenia, bipolar or severe personality disorders. The participant comments that many practitioners are not familiar with how the neurodevelopmental condition impacts the mental health presentation Many however, either fall within primary care level mental health services where the complexity is too great or fall between service gaps. (Interview IP12, written contribution from subject matter expert).
Interpretation and implications:
Links with the Community Mental Health Recovery Service (CMHRS) could be improved across Surrey to prevent service users experiencing multiple disadvantage from being held in primary services for longer than necessary. For example, direct communication channels could be set up between CMHRS and frontline staff of any services supporting people facing multiple disadvantage to support continuity of care.
The majority of individuals with a neurodevelopmental condition will not present with a serious mental health need. More commonly they present with anxiety, arousal, and conditions such as depression. Where these are not treated or managed, they may well develop into acute and transient psychotic presentations and in some cases, more serious illnesses such as schizophrenia and bipolar. Should the individual meet the threshold to be included within a secondary care mental health service, they may get their needs met. (Interview IP12, written contribution from subject matter expert)
6.2.2. Designing a housing and accommodation support system for people affected by multiple disadvantage
Background and insights from the literature:
Improved housing conditions and greater access to green spaces should have a positive impact on health, however, the outlook is uncertain for individuals facing multiple disadvantage.
The shortage of housing and accommodation available in Surrey was identified through primary research as a significant gap in current service provision affecting people experiencing multiple disadvantage. However, it should be noted that this is a national issue that is not exclusive to Surrey. The JSNA chapter on Housing and Related Support identifies that there is a specific shortage of lower-level supported living, or for people waiting to go on the housing register, or housing for people on the register and bidding.
People who leave prison with strong foundations in place to make a success of their lives are less likely to re-offend. These foundations include a stable home. 65% of those without settled accommodation after release from prison between February 2019 and February 2020 had re-offended within 12 months. This figure is significantly lower in those who did have settled housing at 44% (HMI Probation, 2020). Data from The Forward Trusts clients being released from Surrey prisons nationally in the year 2022/23, suggested that 64.15% of individuals had no stable housing upon release. [39]
Surrey-specific primary research insights:
Research participants suggested that the shortage of housing has a knock-on effect on an individual’s interaction with other services; when there is not enough appropriate housing for people’s needs, they stay in services for longer periods of time. Participants stated this also presents challenges with benefits, as benefits cannot be claimed without a fixed address, which then has an impact on wider determinants of health.
“When we’re talking about people’s fundamental basic needs without a roof over your head, you can’t really address anything else. So that’s seems to me a really big gap.” (Focus group FG03, person supporting people with lived experience of multiple disadvantage)
There is a lack of suitable accommodation in Surrey and this impacts upon a large number of issues. For example, research participants reflected that people with high levels of need who are experiencing homelessness commonly go through general need hostels and do not receive the support they need. The rigid criteria for hostels were also highlighted, which sometimes result in people being placed in accommodation that is in a different district or borough to where they lived previously – away from their network, community, or support system:
“Because you’re moving out of area then all the health services, the mental health services, adult social care services, go because you’re out of their area. I know they try really hard to then link up with the team’s over there, but they’re so stretched, they’ll put you on a wait list for ages. So, when you move somebody because there’s nowhere else for them to live, you’re actually taking all those services away from them.” (Focus group FG03, person supporting people with lived experience of multiple disadvantage)
People experiencing multiple disadvantage require specialist housing support and accommodation that addresses their unique needs. One service user shared their challenges in living in unsuitable accommodation:
“I do wish I had an actual plan with i-access to actually help me with my drug addiction. The problem is I am in a hostel which is full of drugs and how can I get clean there.” (Qualitative survey QS04, service user with lived experience of multiple disadvantage)
Specialist housing can create spaces that are conducive to healing and recovery, fostering a sense of security and stability. Appropriate housing ensures that individuals have a safe and secure place to live – inadequate or substandard housing can contribute to health issues such as respiratory problems, stress, and mental health disorders. Many frontline providers supporting individuals experiencing multiple disadvantages express the difficulties they face in finding appropriate, specialist support for service users:
“We have a young lady with autism at the moment, plus a whole raft of other conditions. It’s hard to find the right housing for her, so she’s staying in an environment that doesn’t suit her, that actually she feels is making her ill. But there is nowhere better for her to go.” (Interview IP55, person supporting people with lived experience of multiple disadvantage)
Research participants suggested that the system for applying for housing, benefits and managing a tenancy is not designed for people experiencing multiple disadvantage. Inadequate coordination between mental health, substance use, criminal justice and housing services can perpetuate housing instability, making it difficult for individuals to maintain stable living conditions.
“Housing’s got to be one of the most important things for people because how can you progress and move on and deal with those other issues if you haven’t got a roof over your head that’s suitable.” (Interview IP25, person supporting people with lived experience of multiple disadvantage)
There is a need for more dedicated housing support for women, in particular for survivors of domestic abuse and prison leavers. When leaving a women’s refuge, it is often difficult to secure suitable accommodation and many women are temporarily placed in suboptimal bed and breakfast accommodation. In some cases, women have returned to unsuitable circumstances / relationships due to the lack of safe and suitable housing options. One frontline provider working to support domestic abuse survivors reflected:
“I remember the days when if somebody was in refuge, they would automatically get social housing when they came out of a refuge. Those days are long, long gone.” (Focus group FG03, person supporting people with lived experience of multiple disadvantage)
Individuals facing multiple disadvantage, in particular substance use challenges, may face discrimination from housing services. The challenge in finding providers to support this population is described as a “travesty” by one frontline provider, for example, research participants reflected on instances when their clients have been living on a hospital ward for four years because providers do not have the capacity to support with housing and accommodation. Others highlighted the reluctance of housing providers to support people experiencing multiple disadvantage:
“Providers are quite reluctant to take people with the forensic background or if they’ve got comorbidities… it’s quite difficult to find providers who are skilled enough to take that group of people.” (Interview IP59, person supporting people with lived experience of multiple disadvantage)
“The housing associations who provide long term settled accommodation, they’re very risk averse to taking anybody who could be a problem.” (Interview IP14, person supporting people with lived experience of multiple disadvantage)
Interpretation and implications:
Primary research participants noted a reluctance from landlords and property managers to let to individuals experiencing multiple disadvantage, often relating to concerns around late payments and property damage. However, due to barriers to securing social housing for this population, private letting often remains their only option. One service user shared their experience with private renting, and highlighted how the Rent Choice scheme offered by the council is not widely accepted by landlords. The Rent Choice scheme is to help those who are homeless or at risk of being homeless secure private rented accommodation by providing financial support for the first month’s rent in advance, and/or a deposit bond. When Rent Choice assistance is agreed, the Council may issue a deposit bond to help a tenant secure the property. A landlord can make a claim against the deposit bond at the end of the tenancy to cover any rent arrears or damage to the property. Evidence of the costs being claimed must be provided. All claims against the deposit bond must be made within four weeks from the date of the tenancy ending.
The local authority could offer better incentives to landlords to support them in letting to people affected by multiple disadvantage. For example, the local authority could offer to pay landlords six months rent in advance, take responsibility for furnishings or maintain heating systems. Surrey can learn from similar work taking place both locally through voluntary and community organisations, and nationally in areas such as Liverpool and Manchester.
Further insights from the primary research:
Temporary accommodation permitting the consumption of alcohol in a controlled environment. i-access provides advice, information, and signposting to other relevant services for accommodation and supported housing. However, through the eyes of some service providers, this remains an unmet need and ‘wet housing’ is identified as a gap in provision. It should be noted that the term ‘wet’ or ‘damp’ housing can be construed as stigmatising and other terms should be developed to replace them.
Service user case study*
Graham, 65 years old, Addlestone
Graham has been living in Addlestone for 3 and half years now. He is living in an outhouse in the back of a house. The landlady has said it’s got a bed in there and it’s got a fridge. It’s really not habitable but served a bit of a purpose for 3 and a half years. He’s now clean, he’s doing well. He’s going to [a local VCSE organisation] doing an upholstery course. He’s ready to move on.
So, we couldn’t get him on Runnymede Borough Council Housing list until he’s lived in the borough three years. So, at the three-year mark back in December, we put in an application. We didn’t hear from them [Runnymede Borough Council] for two months. We’ve chased and chased it. We then went back two months ago, and they said he has to provide proof of addresses for the last five years.
Now, we can prove the last 3 and half years cause he’s had a tenancy in this place, he’s registered with i-access, with the GP, we’ve got bills, we can do that. What we can’t do is find any proof of his accommodation before. He was basically in a bedsit in Camberley and that was at the time where he was heavily entrenched in using drugs, he was being exploited. There were all kinds of stuff going on and this place that he was renting was bills included so he had no bills in his name. He never changed his bank details over cause he was an injecting drug user and that wasn’t a priority.
I had another conversation with the Council yesterday and I said: “we can’t prove it”, and they said: “well, then he’ll have to wait until he’s been in his current accommodation five years.” He’s 65 now, he’s been through so much trauma. I asked: “even if we produced a piece of paper today with proof of tenancy for 5 years, what are you going to do with that?” They said: “nothing, we just have it on the file” and I said: “well, it’s pointless. This is just a barrier to housing”.
We waited long enough; we waited the three years like they said we had to, and he’s lived in these dire conditions for long enough.
*Excerpt from stakeholder research interview (RP03). Please note names have been changed and some information has been redacted to protect the identity of the service user.
Additional gaps in support:
Research participants identified other areas of unmet need, including:
Trauma therapy: Access to trauma therapy was considered pivotal to recovery for many service users. Trauma therapy is a form of therapy specifically focused on helping someone cope with the emotional response caused by a traumatic event. As one service user commented:
“there should be more green social prescribing and better promotion of what services are available in the local area.” (Qualitative survey QS01, service user with lived experience of multiple disadvantage)
Social prescribing: Social prescribing is a healthcare approach that involves prescribing or recommending non-medical interventions to individuals to address social, emotional, and practical needs. Instead of, or in addition to traditional medical treatments, healthcare providers may suggest activities, services, or support networks that can contribute to the overall wellbeing of an individual or link them in with community resources. Social prescribing recognises the impact of social determinants on health and aims to address the broader factors that influence an individual’s health and quality of life. Service providers and service users would like to have more informal support groups, including peer support networks, coffee mornings, yoga, walking groups and/or exercise classes. One research participant explained how:
“the medical model is outdated as far as I’m concerned. What people need is relationships and contact and connection”. (Interview IP06, person supporting people with lived experience of multiple disadvantage)
Additional primary care services: There is an unmet need for primary care services such as dental care and optometry. One participants shared their personal opinion on dental services, stating:
“I get so fed up with it when I go and see a person with a life-long enduring mental health condition and their teeth are rotting or, you know, that general physical neglect is there. Where are the agencies stepping up to support these people who can’t or won’t register with a dentist? You know, community dental health care, the people that are supposed to go round and see you in your home.” (Interview IP51, person supporting people with lived experience of multiple disadvantage)
Probation: there is a need for continued support for individuals on probation and experiencing multiple disadvantage. There are often hidden support needs within this population, including mental health needs and disability support. Support needs to be provided when people enter into the community, and training could be improved in the probation service to improve understanding of multiple disadvantage, trauma, and how the related risk factors can impact people and the way services should work with them. One service user shared how they would like to be:
“able to access support whilst I’m in prison and having services ready to work with me as soon as I am out of prison.” (Qualitative survey QS21, service user with lived experience of multiple disadvantage)
Residential Rehabilitation: In Surrey, rehabilitation pathways are assessed and managed within the ASC Substance Misuse team, which is co-located with i-access. This team can refer individuals to Social Services for assessment of suitability for rehabilitation and also refer via the Rehabilitation Assurance Process (RAP) pathway which is an open referral pathway. However, the criteria for accessing residential rehabilitation remains challenging for individuals experiencing multiple disadvantage. Residential rehabilitation is outsourced and spot purchasing of beds out of county are sourced for the few individuals that are successfully assessed for this opportunity. One service user shared that from their perspective:
“rehab is costly and not nearby so would have to be away from family.” (Qualitative survey QS21, service user with lived experience of multiple disadvantage)
The NHS does not provide residential rehab programmes; however, they may provide funding for the most serious of cases.
6.2.3. Early intervention and prevention are crucial long-term solutions for responding to multiple disadvantage
Background and insights from the literature:
Many people facing multiple disadvantage will have experienced early life trauma and adverse childhood experiences; as such, early intervention and prevention are crucial long-term solutions to responding to trauma and identifying risk and support earlier. By turning the dial towards prevention, services will be able to reach more people who are heading into crisis, work with them sooner, and prevent multiple disadvantage from taking root in the first place. Early intervention means identifying and providing effective early support to people who are at risk of poor outcomes, and typically refers to support for children, young people, and families.
Early intervention can lead to better health outcomes, for example, timely medical treatments, screenings, and preventive measures can prevent the development of diseases, improve recovery rates, and enhance overall wellbeing. Early intervention in mental health is crucial for preventing the development of more severe mental health conditions. Identifying and addressing mental health concerns early can improve emotional wellbeing and prevent long-term suffering. Ensuring early intervention can also prevent situations from reaching crisis levels, whether in mental health, family dynamics, or community issues.
Early intervention is often more cost-effective in the long run as preventing or mitigating problems early can reduce the need for extensive and expensive interventions later on, including medical treatments, rehabilitation and social support. Meeting the needs of people in multiple disadvantaged groups costs society an estimated £10.1 billion per year. [2]
Surrey-specific primary research insights:
Early intervention aims to address any challenges at their initial stages before they escalate which serves to prevent the progression of health, social, or behavioural issues into more severe and challenging conditions. One participant noted that the lack of early intervention can therefore have a causal effect on multiple disadvantage:
“It’s that lack of early intervention that then brings on these multiple disadvantages, cause once you’ve lost one part of the jigsaw then the other part goes and […] it’s that whole thing of how quickly and scarily someone can fall down the ladder and be gone through all the gaps.” (Interview IP17, person supporting people with lived experience of multiple disadvantage)
Effective early intervention was considered by some research participants to support the occurrence of problems in the first instance, or to help tackle them head-on before problems worsen or individuals become more entrenched:
“If we don’t get the prevention right, we’re in all sorts of a mess in five years’ time.” (Interview IP76, person supporting people with lived experience of multiple disadvantage)
Some research participants consider early intervention as crucial in situations such as mental health crises, domestic violence, or financial difficulties, helping individuals navigate and overcome difficulties before they worsen:
“If you can meet people earlier on and support them early on and understand them early on, you save a great amount of pain for them, but you also save an awful lot of money because you’re not having to provide massively expensive interventions when things have gone completely pear shaped.” (Interview IP05, person supporting people with lived experience of multiple disadvantage)
Not all people experiencing multiple disadvantage are frequent users of emergency services or are involved with the criminal justice system – but some are, and this kind of avoidable use of public services can be costly. One research participant highlighted the benefits of early intervention, stating:
“By investing a little bit and doing it in the right way, what you will do is prevent some of that serious stuff and actually save money down the line… to do that you need to be thinking five years ahead and not about the here and now. And do you invest a budget where we have a five-year plan when the government’s only giving you money for a next year? How do you plan long term where you can’t do that?” (Interview IP12, person supporting people with lived experience of multiple disadvantage)
Interpretation and implications:
The finite funding and eligibility criteria for services at present, both locally and nationally, often means that only the most vulnerable and high need individuals are able to be supported within this remit. People affected by multiple disadvantage do not always meet the threshold for support as they are deemed ‘not bad enough’ or not ‘in crisis’. Focusing on early intervention and prevention means that services should be supporting people in a ‘milder state’ so that the challenges they face not become entrenched.
6.3. ‘Misheard and misunderstood’: understanding multiple disadvantage and its links with trauma
This section discusses the primary research finding that support systems and services often fail to recognise and address the multifaceted nature of multiple disadvantage and its roots in trauma. Without proper recognition from services, these individuals may be misdiagnosed or receive inadequate or no treatment.
Primary research identified that people affected by multiple disadvantage commonly experience stigma and judgment and the limited understanding and implementation of trauma and psychologically informed approaches further contributes to this systemic discrimination and implicit bias. Embedding a Trauma Informed Approach (TIA) cannot be done piecemeal, it is a system-wide cultural change that requires the system to work collectively and take small steps towards equipping services to recognise and respond to people’s trauma and embodying trauma and psychologically informed principles in a meaningful way.
The secondary data analysis exercise highlighted a noticeable scarcity of data and intelligence around multiple disadvantage and associated risk factors in Surrey due to data governance, data infrastructure and data quality. The invisibility of multiple disadvantage within datasets further hinders a comprehensive understanding of this population’s specific needs and infers that the systems designed to serve them are unintentionally set up to fail from the outset.
6.3.1. People affected by multiple disadvantage experience stigma and judgment
Surrey-specific primary research insights:
Primary research findings indicate that systemic discrimination, stigma, and implicit bias about people experiencing multiple disadvantage continue to exist in Surrey. These judgmental and victim-blaming attitudes act as a barrier to accessing services, as one participant described:
“If you’re using drugs, a lot of services won’t provide you with support. You’ll find it really difficult to get a job. You’ll find it really difficult to hold a tenancy. Well, now you’ve got no source of income, no job, no house. You’ve got low self-esteem. You probably haven’t got meaningful relationships. Is it any surprise then that life then starts to get into a negative spiral of it just getting worse and worse and worse.” (Interview IP62, person supporting people with lived experience of multiple disadvantage)
Primary research findings considered how the limited understanding around multiple disadvantage from society and the system can often leads to stigma and judgment. One participant noted how there is also a tendency from some services to blame individuals for their circumstances, assuming that their disadvantages are a result of personal failings rather than systemic issues, for example, “what did you do to bring this on yourself?” (Interview IP21, person supporting people with lived experience of multiple disadvantage) One participant shared their account of witnessing judgement and stigma towards clients experiencing multiple disadvantage:
“It’s not nice to be judged and saying, “Well, it’s your fault you’re in this thing”, you know people quite well aware, they don’t wake up and say, “Yeah, I wanna be a drug addict or an alcoholic.” You know, usually it’s been some sort of trauma that has affected their life.” (Interview IP02, person supporting people with lived experience of multiple disadvantage)
This outlook can marginalise those who need assistance the most and lead to feelings of shame, low self-esteem, and a reluctance to seek help. (Interviews with the LERO, experts by experience). One service user shared how they do not like “being referred to as “not another drug addict”” by services with which they have engaged (Qualitative survey QS20, service user with lived experience of multiple disadvantage). This stigma can also lead to social exclusion, isolation, and a sense of being unwelcome. In September 2024, Surrey published a separate JSNA chapter on Loneliness and Social Isolation which provides significant insight into different population groups’ experiences of loneliness, isolation, and exclusion.
Stigma and judgment are experienced in many healthcare settings, particularly in Accident & Emergency services. Service users report receiving suboptimal care or facing discrimination with such negative experiences often leading to a reluctance to seek support in the future and exacerbating health disparities:
“If you go in there [hospital] and maybe you’re intoxicated, are you treated the same way as somebody who isn’t? […] All our domestic abuse survivors haven’t had very good experiences around that”. (Focus group FG03, person supporting people with lived experience of multiple disadvantage)
It is also noted that some pharmacies show a reluctance to provide supervised consumption or needle exchange services, with one factor being stigma around the type of people using this service. One participant explained the impact of stigma on pharmacies:
“Pharmacies don’t want people coming in who are at high risk of shoplifting… not everybody shoplifts to feed their habit, but they only have to have one bad experience and then that just that paints everyone with a in a poor light.” (Interview IP18, person supporting people with lived experience of multiple disadvantage)
Stigma also impacts access to housing, with service users who are unemployed or in receipt of benefits finding it challenging to secure a rented property. One service user shared their experience with housing services, stating that the service was:
“Very harsh about addiction, like you’ve caused your own situation and you’re lucky that you’ve got six weeks in the homeless house.” (Interview LERO, expert by experience)
Background and insights from the literature:
The language used when speaking about or referring to people affected by multiple disadvantage can have a significant impact on how individuals view themselves, and how others view them. Trauma informed and trauma sensitive language uses the person’s own language and descriptions and language that heals rather than harms, for example, describing someone with experience of domestic abuse as a ‘survivor’ rather than a ‘victim’ as it conveys a sense of empowerment. It is important that stigmatising labels or descriptions of behaviour which infer or uphold negative stereotypes (e.g., manipulative, attention seeking), punitive attitudes, and individual blame, are avoided.
This JSNA chapter refers to its subject as an individual ‘experiencing multiple disadvantage’ or ‘affected by multiple disadvantage’ rather than an individual ‘with multiple disadvantage’. This change in language shows that a person “has” the problem, rather than “is” the problem. A further example of preferred language in this JSNA chapter is the term ‘substance use’ rather than ‘substance abuse’ or ‘substance misuse’. The latter terms are presumptive with a high association with negative judgements and punishment. [40]
Surrey-specific primary research insights:
Research participants reflected on how words can be alienating, particularly when defining people solely by the challenges they are facing or labelling them as ‘others’, inferior or morally flawed. One participant highlighted how stigma and judgement is accepted as the norm for multiple disadvantage:
“If somebody’s racist, somebody would go: ‘You’re being racist’. If somebody’s being homophobic or sexist, somebody would say: ‘You’re being homophobic, you’re being sexist’. But you can say whatever you like about substance users, about ‘alkies’, ‘druggies’, ‘bagheads’, ‘donkeys’, and nobody would bat an eyelid. It’s almost like an outlet for people to vent all their kind of petty hatreds and petty prejudices. You can say whatever you like.” (Interview IP23, person supporting people with lived experience of multiple disadvantage)
Appropriate use of language was also highlighted as being pivotal for professionals supporting multiple disadvantage, as the labels and stigmatising language used to discuss an individual can impact their access to services and the ways other services view that individual. One research participant explained the importance of professionals avoiding stigmatised language and labels when discussing a service user or writing up case notes:
“If I put a referral in and I start it along the lines of… ‘This person is really complex, and they never engage, and they’re really hard to speak to and they’re a drug user and this, that, and the other…’, that person is stereotyping already about what this person looks like, what they’re going to be like, thinking they’re going to be a complete nightmare. Actually, if we set out that narrative in a different way, it just changes everything.” (Interview IP11, person supporting people with lived experience of multiple disadvantage)
6.3.2. Understanding of trauma and psychologically informed approaches
Background and insights from the literature:
The majority of people experiencing multiple disadvantage as adults have also experienced trauma as children, however, services are not always equipped to recognise and respond to people’s trauma and its continuing impact. In a post from Fulfilling Lives (Lambeth, Southwark, and Lewisham) on understanding the link between trauma and multiple disadvantage, it was noted that: “recent research revealed a high prevalence of trauma amongst people experiencing multiple disadvantage, and how, for many, interactions with the system can re-traumatise…. We found that services did not always understand how trauma manifested in people’s behaviour and that women who have experienced trauma are in danger of being labelled as hysterical or manipulative.” [41]
Trauma refers to events or circumstances that are experienced as harmful or life threatening and that have lasting impacts on mental, physical, emotional and or social wellbeing. A significant singular traumatic event can lead to Post Traumatic Stress Disorder (PTSD) – for example car crashes, natural disasters, serious illness, loss of a loved one. However, much trauma is relational, that is it can often occur at the hands of other people, often those we hope would care for us and the effect can be insidious. It is well evidenced that such relational trauma often begins in childhood (but can occur or continue into adulthood resulting in compound trauma effect, or a diagnosis of Complex Post Traumatic Stress Disorder). When these traumatic experiences are at the hands of people, services or systems holding power, and/or caregivers of some kind the impact on lifelong psychological/emotional wellbeing, behaviours and interpersonal functioning is significant. [42]
As knowledge about trauma and the lifelong impact it can have has increased, the concept of a Trauma Informed Approach (TIA) has evolved. This assumes people have a trauma history and aims to make services accessible and appropriate for people who have experienced trauma and for those employed within them.
Taking a Trauma Informed Approach means acknowledging the widespread impact of trauma on thoughts, feelings, and behaviour, taking a holistic approach to each individual and recognising the signs of trauma and responding accordingly. Furthermore, a TIA aims to prevent further re-traumatisation by realising that services and systems can create further traumatisation and then working to prevent this from happening.
Within a TIA, ensuring people’s safety is paramount. People strive for a sense of internal and external safety by any means necessary often leading to behaviours which in of themselves can inadvertently increase traumatic experiences. Importantly, a TIA also adopts a strengths-based approach coupled with collaboration and importance given to the person’s voice, choice, and views. Thereby promoting a sense of control and empowerment.
Building trust and transparency between staff, managers, services, and people accessing services is a key to embedding a TIA. One important way this can be established is by listening and taking heed of the views and advice given by a lived experience community. Another key point embedded within a TIA is consideration of divergence in all forms and intersectionality, cultural, historical and gender contexts.
The 6 overarching principles of a Trauma Informed Approach:
| Safety | clients and staff experience physical and psychological safety |
| Trust and transparency | decisions are made with transparency, cultivating an ethos of trust |
| Peer support | stories and experiences are shared to facilitate recovery |
| Collaboration and mutuality | power differences are levelled, and decisions are shared between all involved |
| Empowerment, voice and choice | positive attributes are built upon, choice is offered, and self-advocacy promoted |
| Respect for diversity | stereotypes and stigmatising language are avoided and addressed, and individual need is recognised |
A Psychologically Informed Approach is focused on the development of effective communication between clinicians and patients rather than on an “assess and educate” model in which the main focus is on the didactic provision of information rather than the development of patient-centredness. [43]
Figure 15: Psychologically Informed Environments
The adjacent iceberg diagram demonstrates how on the surface it can appear that a Trauma Informed Approach is everything, but under the surface it is evident that broader psychological understanding, attachments, and brain functioning underpins and provides the foundations for a Trauma Informed Approach.
A Psychologically Informed Approach is essential in providing a holistic understanding and facilitating conversations between practitioners around what is needed for someone and why.
Psychologically Informed Approach are services that are designed and delivered in a way that considers the emotional and psychological needs of the individuals using them. Any service supporting multiple disadvantage can become a Psychologically Informed Approach. [44]
Surrey-specific primary research insights:
In a survey with 100 stakeholders supporting multiple disadvantage across Surrey, around four in five stakeholders (79%) agreed or strongly agreed that their service works with people in a way that is trauma informed. However, interviews identified a mismatch in organisations believing they are trauma informed and organisations evidencing trauma informed ways of working in practice:
“I think a lot of services will say their trauma informed… but in practice when dealing with this cohort, it’s a different matter.” (Interview IP01, person supporting people with lived experience of multiple disadvantage)
“People get labelled and diagnosed and boxed and categorised and their trauma experiences aren’t considered. They’re not listened to.” (Interview IP55, person supporting people with lived experience of multiple disadvantage)
Service users identify compassion, empathy and respect as some of values that make a service provider ‘good’; these values can be attributed to trauma informed care. Research participants working in the VCSE sector demonstrated their understanding of what it means to be trauma informed and shared clear examples of trauma informed care in practice:
“We work with them. We don’t do stuff to them; we walk alongside them. We create a safe space for them. In other words, we work in a trauma informed way before we even put a label on it.” (Interview IP05, person supporting people with lived experience of multiple disadvantage)
“We walk with them; we don’t pull them along.” (Focus group FG03, person supporting people with lived experience of multiple disadvantage)
Other participants identified additional key qualities that go hand in hand with being trauma informed, such as listening to the individual being supporting, empowering individuals with voice and choice, and upholding honesty and transparency.
Should trauma informed training be mandatory?
Background and insights from the literature:
Surrey can learn from national examples such as Plymouth, which has recently become a Trauma Informed City and work towards developing a network of professionals with insight of how trauma can affect people and to start to look at a system wide approach to tackling the effects of trauma.
Professionals should be trained to understand what implementing a Trauma Informed Approach means, and why it is relevant to their work. For TIA to be effective and valuable, practitioners must want to work in this way because they believe it has value, not simply because policy obliges them to do so. Embedding TIA can be monitored and evaluated through use of an appropriate tool or framework such as the Embedding TIA. It can be monitored and evaluated through use of an appropriate tool such as Surrey and NE Hants’ Trauma Informed Approach Framework and Toolkit. This Toolkit can help organisations to identify areas for trauma informed quality improvement and empower organisations to prioritise an action plan for practical trauma informed change.
Key highlights in the Surrey and Northeast Hampshire Trauma Informed Care Training Attendance Overview Year 1 (2023) include:
- The first year of Trauma Informed Training workshops began in Q3 2022 and ran to the end of Q1 2023. A total of 180 workshops ran across 14 different modules. A total of 1242 individuals attended training workshops.
- Participants represented a wide-ranging workforce from seven sectors, employed by 61 organisations across 24 service remits, including Mental Health, Drug and Alcohol, Learning Disabilities and Community Services, Social Care Services (examples). The largest numbers of individuals who attended workshops were from the NHS, Charity or Local Authority sectors.
- The job role category with the largest number of individuals attending training was registered clinicians such as psychologists, therapists, nurses, doctors, counsellors, midwives, occupational therapists, mental health practitioners and social workers as well as those in training.
Surrey-specific primary research insights:
Some primary research participants identified the need for trauma informed training to be included as mandatory training for all professionals in Surrey, both statutory and non-statutory services.
“I feel it should be embedded as part of a core training offered. So as people do statutory health and safety, then I think we should do a statutory training course and follow up modules on trauma so that the identify when people perhaps represent them social care, children, or adults, that there could be an absolute trigger in terms of trauma from people.” (Interview IP22, person supporting people with lived experience of multiple disadvantage)
Embedding Trauma and Psychologically Informed Approaches requires a combination of training and culture change and may take years to fully embed into a system and practice. It is often reliant on the individual service provider and their way of thinking and experiences, but as reflected by these quotes from our research participants, it is also pivotal to have understanding and commitment from senior leadership:
“To have a trauma informed approach, it’s got to be a cultural change through the organisation. It’s not something that you kind of learn and do. It’s got to be a real belief. You’ve got to have that real passion and value for people and people being equal, and I don’t think statutory services are set up to treat people like it.” (Interview IP06, person supporting people with lived experience of multiple disadvantage)
“I don’t think there’s the commitment higher up as well. I think people like to talk about it [Trauma Informed Approaches] cause it’s the buzz phrase, but I actually don’t know whether senior staff in organisations really grasp what that means.” (Interview IP20, person supporting people with lived experience of multiple disadvantage)
Interpretation and implications:
As a minimum, all professionals working with people experiencing multiple disadvantage should undertake the foundation Trauma Informed Approach modules: ‘Understanding trauma informed care’. Not only does this include specialist multiple disadvantage services, but also all services interacting or supporting people facing multiple disadvantage such as housing and accommodation services, substance use services, mental health services, domestic abuse services, probation services, in addition to the wider workforce including non-clinical staff and organisations. This includes staff at all at levels of these organisations, including junior, senior and executive.
Staff training and support enables workers to move away from crisis management and work in a more therapeutic and planned way. The challenge is that many professionals have limited time and capacity to complete training, further there is a lack of understanding around the importance of embedding TIA. Embedding a TIA does not require every individual to have the experience of a clinical psychologist, however, a foundational knowledge and understanding is important. Some service providers have been offered it but have not taken it for fear of taking someone else’s place, such as a practitioner who is frontline working directly. The messaging needs to change.
6.3.3. People facing multiple disadvantage are often invisible in data sets and data recording
Background and insights from the literature:
People’s experiences of multiple disadvantage are not always recorded in health datasets or are inconsistently recorded, rendering them and their needs almost invisible. Similarly, a lack of data sharing between services means that people experiencing multiple disadvantage must frequently retell their story to each of the individual services they are in contact with, often resulting in re-traumatisation and further harm.
Two primary examples of gaps in data resulting in people being failed by the system are sex workers and people experiencing homelessness.
- Sex workers rarely appear in health datasets due to the private nature of the sex industry and the transience of the activities required in their work. More importantly, however, in the UK there is currently “no source of data [that] allows for the production of representative population estimates for [sex workers].” [45]
- People experiencing homelessness likewise fall within gaps in datasets as their lack of fixed addressed prevents them from accessing the majority of public services, for example, registering with a General Practitioner (GP). There is also no national figure for the number of people experiencing homelessness in the UK, this is because homelessness is recorded differently in each nation, and because many people experiencing homelessness do not show up in official statistics. [46]
Data has the potential to have a significant impact on decision-making and strategic commissioning, and as such, gaps in data can lead to poor decisions, wasted resources, missed opportunities, and increased risk and harm to individuals affected by multiple disadvantage. These missing populations are thereby not adequately represented in health data, and as such, systems are not only struggling to address their specific needs but run the risk of putting these groups in further harm. Mental health data for example fails to reflect demography, consolidating disparity for people with certain characteristics.
Surrey-specific primary research insights:
In order to address concerns about data invisibility, an expert by experience commented on the need for sharing information and collaborating on treatment plans as being essential for effective outcomes:
“If I had to make a single recommendation it would be for systems to support and encourage practitioners to make sure that the details they enter on systems include sufficient cultural and demographic information to be able to provide fuller social context. This would improve the system’s visibility of people with characteristics that might need adjustments and encourage systems to adapt approaches towards more person-centred and trauma informed care, which of course should involve empowering practitioners to work collaboratively with other agencies including development through reflective practice and engagement of lived experience.” (Interview IP04, person supporting people with lived experience of multiple disadvantage)
Interpretation and implications:
As incomplete information regarding the needs of certain populations has the potential to result in inadequate resource allocation and poor service provision, some participants identified the need for a Community of Practice (CoP). A CoP is a place where data leads and those working with data for multiple disadvantage could come together to talk about the progress of their services and reporting on a regular basis. A CoP would offer a dedicated space to discuss any issues and connect with peers for support and shared learning.
6.4. ‘One size doesn’t fit all’: service design for people experiencing multiple disadvantage
Literature shows people in inclusion health groups such as those experiencing multiple disadvantage struggle to access health and social care and often have poor experiences when they do. The primary research presented in this chapter reflect how ‘one size doesn’t fit all’ when it comes to support for people experiencing multiple disadvantage. The findings show individuals experiencing multiple disadvantage require access to a diverse, integrated, accessible, and flexible market of service providers that offer a range of treatment and pre-treatment options to foster flexibility, choice, and innovation.
Primary research and findings from a wider literature base indicate that progressive, person-centred support models that focuses on relational support, provides assertive outreach, and is delivered in a trauma informed way would better support people facing multiple disadvantage. Individuals experiencing multiple disadvantage do not always require a web of services placed around them and often this can in fact cause further complexity due to multiple referrals, multiple assessments, multiple retelling of stories, and multiple barriers relating to service criteria. Progressive support models can ‘pull’ in traditional support and treatment services as and when desired and/or directed by the person at their own pace once their priority needs have been met. There is therefore a place for non-medical models which can work in tandem with both relational support services and larger specialist services to support this population.
People with lived and living experience of multiple disadvantage are vital to decision-making processes and their involvement is pivotal in the design, delivery, co-production, and evaluation of services through genuine co-production.
6.4.1. Person-centred services in Surrey
Background and insights from the literature:
Person-centred care is recognised as a core, guiding approach to delivering holistic support for people experiencing multiple disadvantage. [51]
- Person-centred care considers the unique needs, preferences, and values of the individual receiving the care, treating them with respect, compassion, and empathy, and recognising that they are the experts on their own lives. It encourages collaboration between the service provider(s) and service user when making decisions about care.
- Person-led care empowers the individual receiving the care to be the expert on their own needs and preferences, putting them in the driver’s seat and encouraging active participation in decisions about their care. Person-led care recognises that individuals have the right to make informed choices about their care and that they are the most important voice in the decision-making process.
Surrey-specific primary research insights:
Primary research indicates that there are limited services in Surrey that provide person-led and person-centred support for people experiencing multiple disadvantage. People affected by multiple disadvantage have said they require bespoke support that both understands and recognises the interconnected nature of multiple disadvantage as well as the impact of their trauma. For example, one service user reflected on their involvement with services:
“There have been certain support workers who I have not connected well with. They have seemed controlling in telling me what I have to do. I feel much better supported when I am gently encouraged to do things and supported with them.” (Qualitative survey QS13, service user with lived experience of multiple disadvantage)
Another shared:
“If support staff are more encouraging rather than telling me what do to. When I’m told what to do I feel like I’m under pressure more.” (Qualitative survey QS20, service user with lived experience of multiple disadvantage)
It is these experiences which remind the system and service providers of the need to apply continued efforts to ensure the individual experiencing multiple disadvantage is at the heart of how support is designed and delivered.
“It’s not good enough to just expect people to just about survive. That’s no way to live, is it? There needs to be stuff out there that’s going to actually support people to really be independent and resilient and have a good life.” (Focus group FG06, person supporting people with lived experience of multiple disadvantage)
Many research participants also emphasised the importance of flexibility when responding to the different priorities and concerns of each individual experiencing multiple disadvantage. Some service users may feel confident in attending appointments independently, others may experience anxiety, some may have childcare issues, and many will have worries that fluctuate and change week-by-week.
Interpretation and implications:
It is important that services strengthen their delivery design by taking a more person-centred care approach. For example, outcome-based support is an approach to providing services that focuses on achieving specific, measurable results or outcomes for individuals. This method emphasises the effectiveness and impact of support, rather than simply the activities or services provided. Introducing more of an outcome-based approach alongside meeting the output-based Key Performance Indicators (KPIs) required by statutory service models will help to encourage providers to ‘work with’ service users rather than ‘do to’. This means that services will continue to work with the client to achieve the individual’s goals, as opposed to making assumptions about the care the individuals would like to receive and taking actions based on what the provider thinks is best.
6.4.2. Flexible service design helps to support the non-linear journey of relapse and recovery
Surrey-specific primary research insights:
Some participants reported that some services are not flexible with an expectation of a linear progression to recovery. However, this does not always reflect the reality of relapse and recovery and the complex nature of the needs of people experiencing multiple disadvantage. Person-led and person-centred services are a better match, as some participants commented:
“I’ve worked with so many great workers from i-access, but they have quite rigid pathway. So, if you can get beyond that and get one-to-one sessions and get a worker then you’re doing quite well. But if you go down the normal pathway that can be two misses and you’re out.” (Focus group FG03, person supporting people with lived experience of multiple disadvantage)
“My clients, they don’t fit a package. There’s no box that you are going to stick them in, there has to be some flexibility.” (Interview IP08, person supporting people with lived experience of multiple disadvantage)
Substance use care pathways for people experiencing multiple disadvantage could therefore be reviewed, as substance use services in Surrey are designed to offer person-centred care planning with a selection of options available to meet service user needs and be inclusive for all, including people experiencing multiple disadvantage. Service users refer to experiencing a ‘take it or leave it’ attitude from service providers when it comes to accepting treatment, with service users having limited to no alternative support options. Research participants reflected on the ‘all or nothing’ approach of the service offer in Surrey, stating:
“This is what we can offer you and that’s it. And if you don’t like that offer, there’s nowhere else in Surrey that you can go to get this offer. So, you know, you’re stuck with us.” (Interview IP01, person supporting people with lived experience of multiple disadvantage)
“With i-access, you’ve got a very complex person that’s got an addiction and they’re asking for help. First of all, they’re told they don’t meet the threshold. Well, so what now? They should go and use more heroin? They should go and drink another 2-litre bottle of cider just to meet that threshold? What if you don’t want to just reduce down? So, i-access is very black and white, you give up or nothing…. We all know from working in the substance misuse field for somebody that is in the real throes of addiction that needs that service that is one of the scariest things you can say to somebody, it’s overwhelming, they don’t think they can do it. You need to take baby steps, so you don’t just jump them from A-Z.” (Interview IP52, person supporting people with lived experience of multiple disadvantage)
Short-term interventions:
Background and insights from the literature:
For someone experiencing ‘low level’ challenges, current short-term interventions may work well, however, over 80% of people facing multiple disadvantage as adults experienced trauma as children. [2] For many, their current circumstances are shaped by long-term experiences of poverty, deprivation, trauma, abuse, and neglect. As such, short-term interventions are highly ineffective and can even do more harm than good.
Surrey-specific primary research insights:
Primary research participants identify that some of the current interventions offered by mental health and substance use services may provide immediate relief or support for individuals affected by multiple disadvantage, but are not always able to address the root causes and often fail to recognise long term social value. One service user shared:
“I would like to see longer-term ongoing support, I don’t want set courses or support with an end date.” (Qualitative survey QS08, service user with lived experience of multiple disadvantage)
This is partly because some of these interventions tend to be designed based on a defined recovery period in-line with the current evidence base. For example, a 6-week CBT course has shown to be effective to alleviate mental health symptoms.
Many research participants felt that episodic interactions (e.g., 6 appointments over 6 weeks or fortnightly appointments with a time limit) make it difficult to build genuine connections and foster trust and respect. One participant stated that in order to make every contact count, partners must prioritise “human interaction, not just a process-based interaction” (Interview IP10, person supporting people with lived experience of multiple disadvantage)
Long-term solutions are generally more effective in fostering sustainable improvements and breaking the cycle of disadvantage. [66] Some research participants agreed that opting for a ‘quick fix’ as an easy remedy or solution, especially a temporary one, fails to address underlying problems and root causes, and does not serve to improve future health outcomes for this cohort.
6.4.3. The voices of people with lived experience are vital to informing service design and commissioning
Background and insights from the literature:
People affected by multiple disadvantage have a wealth of expertise, experience, skills, and assets to offer. [47] Services are often experts in processes and setting up infrastructure, yet they can struggle to understand or address challenges, like how to help people access services, without the input of those who use the service. The voluntary and community sector in Surrey is well placed to understand the local context and its assets (people, places, and things). VCSEs hold a wealth of information and experience about the multiple disadvantage population.
The national framework on action on inclusion health provides examples of good practice and practical actions for organisations relating to the involvement of lived experience. [48] The framework suggests using participative research approaches to support people with lived experience contribute to research and evidence and listening to the voices of people with lived experience. NHS guidance on working in partnership with people and community emphasises how involving people and communities support the wider objectives of integration.
What is co-production?
Co-production involves institutions like local government or treatment services working in equal partnership with local communities to make decisions, design and deliver public services or programmes of support. Co-production means that the partners will have mutual respect and use an inclusive approach that values difference.
The Think Local Act Personal ladder of co-production was developed by the National Co-production Advisory Group. It describes a series of steps towards full co-production in health and social care and supports greater understanding of the various steps such as access, inclusion, and consultation.
At the top of the ladder, and what organisations should be working towards when commissioning services, is co-production. Co-production is an equal relationship between the people who use services and the people responsible for services. They work together, from design to delivery, sharing strategic decision-making about policies as well as decisions about the best way to deliver services. In the middle of the ladder is consultation. Common examples of consultation are inviting service users to complete a survey or attend a meeting. Consultation is often considered tokenistic if the people who use services do not have the power to influence or affect change. It is not enough to only consult and engage people who access treatment and recovery services. The experiences of people who are not currently accessing services and those who have never accessed services, and their families or carers, are equally valuable when developing services and projects. Their input is especially helpful when partnerships want to ensure equity of access, reach into specific communities, and develop early intervention, harm reduction and recovery support services. [49]
At the bottom rung of the ladder is coercion. Coercion does not take into account the views of people who access services and often considers them as passive recipients and is a clear example of what needs to be avoid in strategic commissioning and service design.
The value of genuine co-production:
Having to put ‘genuine’ in front of co-production reflects the misinterpretation, within Surrey and more widely, about what true co-production is and how it is practised. It can often be mistaken for feedback and tokenism. Genuine co-production is a way of working that places the input from people using services on an equal powerbase with those who work in the system and design the services. When co-production works best, people who use services are valued by commissioners as equal partners, can share power, and have influence over decisions made.
In May 2022, Luminus (formally Healthwatch Surrey) produced an engagement report focusing on understanding co-production and ‘Who holds the power?’. The report identifies that “genuine co-production would mean a culture shift in services; if people with lived experience are to be equal partners and peer employees working together in the commissioning, design, and evaluation of services, they would also, in some form, need to share in the responsibility and accountability for those services.” [50]
In Surrey, there are two coordinated multiple disadvantage LEROs (i.e., groups of people with lived and living experience) in which members share experiences of services and discuss options on how to make things better for the service users. The lived experience group is starting to get some real traction and engagement, with the groups sharing experiences and providing rich discussions on how we move forward. The general mood of both groups is of hope that individuals do not have some the experiences that they have had, and they are contributing to the future design and delivery of services moving forward. That being said, the LERO have expressed that they have experienced challenges and resistance within certain parts of the system with unconscious bias and stigma. For this to be addressed current culture at a higher level (management and above) need to understand the value and principles of doing “with and not doing too” and relinquish some of the historical power dynamics so equality can be achieved. The ambition of co-producing this JSNA chapter as taking part in other co-produced projects is to distribute the power base on an equal footing and have lived / living experience at the governance – overseeing with scrutiny at how public services are designed, developed, and held to account, having positive conversations with achievable outcomes with the individual at the centre of their care.
An example is Changing Futures, programme funding has allowed Surrey’s Bridge the Gap service to value the contribution from our lived experience partners and renumerate them accordingly for their expertise. Most people would not work for free or except being paid in vouchers, therefore we offer a financial payment at an agreed hourly rate for someone’s time and expertise when engaging in co-production.
Surrey-specific primary research insights:
Involving individuals with lived and living experience in service design can create a more responsive and effective support system and ensure a depth of understanding and insight. It also humanises experiences and challenges associated with multiple disadvantage, thus reducing stigma. Involvement in the design process also provides people with lived experience ownership and empowerment in decision making as they are actively included in shaping the services that directly impact their lives, fostering a sense of agency and dignity. Some members share their personal experiences of being involved in the lived experience group:
“It’s the first time I’ve got to a place where I want to be involved and contribute.” (Interview LERO, expert by experience)
“It has helped me develop my research skills and after one year I now have got some part-time work as a researcher. I was encouraged to do interviews with stakeholders and learnt about so many projects and initiatives through the Chapter. Having fortnightly meetings and a monthly face to face meeting gave me new purpose. I was destroyed by my mental health and addiction and needed hope and a project with which i could get involved. I also needed contact with people who could understand and encourage me as felt so much shame over my past.” (Interview LERO, expert by experience)
“It has been refreshing not to be judged and just be given a chance to advocate.” (Interview LERO, expert by experience)
6.4.4. A relational approach is needed to best respond to multiple disadvantage
Background and insights from the literature:
National literature highlights that when designing and delivering services, relational models rather than medical models can be more beneficial for people affected by severe and multiple disadvantage. An evaluation of Fulfilling Lives (The National Lottery Community Fund investment to support people experiencing multiple disadvantage) highlights that traditional models of delivery exclude people experiencing multiple disadvantage. The report states that: “the traditional ‘appointment’ model of healthcare does not work for people facing multiple disadvantage. People are required to remember appointment, attend at times that do not take into account their needs and often have to wait long a period between assessment and treatment. Communication methods, including mailing out appointments and telephone calls are unsuitable for many. Appointments take place in institutional and clinical settings that are unwelcoming and feel daunting to beneficiaries; there appears to be a lack of community-based or outreach services that might be more appropriate.”
As echoed in the Fulfilling Lives Re-thinking Outcomes report, proof of concept models such as the Fulfilling Lives and Changing Futures programme demonstrate the benefits of designed services aimed specifically at people experiencing multiple disadvantage. A relational model provides a platform for building trusted relationships between people and organisations, improving connections with services, and supporting individuals power, choice, and autonomy.
Surrey-specific primary research insights:
Primary research identifies how the majority of service provision for people experiencing multiple disadvantage is currently geared up to support people based on what it considers to be their primary need, be that housing provision, substance use treatment, or mental health support. However, leading with a relational approach works well for people experiencing multiple disadvantage and can help prepare individuals for timely medical/clinical interventions.
Research participants shared how a holistic offer of support for people experiencing multiple disadvantage can help to better address an individual’s needs in a comprehensive and integrated manner, recognising the interconnected nature of various aspects of a person’s life. It is important for services to ensure they are ‘doing with’ people affected by multiple disadvantage, rather than ‘doing to’, and making assumptions around their care. For example, service users involved in primary research share how in their interactions with drug and alcohol treatment, it is often assumed that being in recovery means abstinence from substances, yet for the individual experiencing multiple disadvantage the journey of relapse and recovery is far from linear and abstinence may not align with their personal goals.
Treating the person, not the condition:
Surrey-specific primary research insights:
System structure was highlighted as a key challenge to the delivery of effective support. Research participants report that some services in Surrey tend to focus is on treating a condition rather than treating a person holistically and typically support people on what it assumes to be their primary need. As one research participant advised:
“Put the person in the centre of everything you do…don’t treat the condition, treat the person” (Interview IP12, person supporting people with lived experience of multiple disadvantage)
When people affected by multiple disadvantage are referred to support services, participants reflected it is often the condition they are experiencing that guides the conversation and treatment plan, with little consideration of the individual’s specific needs and background. A service provider highlighted:
“I’m met with their diagnosis before ever get to know who they are and it’s almost like it’s led by what they’ve got wrong with them rather than what we can do to help in that situation.” (Interview IP49, person supporting people with lived experience of multiple disadvantage)
Providing support for only one condition, by consequence, creates further issues with the other challenges an individual may have happening in their life. One participant explained that organisations not taking a holistic approach may create challenges in effectively supporting a person on their journey:
“It’s like having a jigsaw with three pieces missing. You’re not going to finish it and it will never be quite right.” (Interview IP12, person supporting people with lived experience of multiple disadvantage)
Interpretation and implications:
Providing an individual with housing support without putting in place support for mental health and/or substance use at the same time, may make it difficult for an individual to sustain their housing. Likewise, an individual experiencing multiple disadvantage should not be expected to have improved mental health or successfully participate in substance use treatment while being homeless. It is important for the system and providers to understand that multiple disadvantage must be considered as multiple disadvantage, rather than a series of individual needs to be treated distinctly. In Surrey, the service offer from i-access demonstrates examples of collaboration, with wider teams including Adult Social Care, housing, Surrey Adults Matter, Citizens Advice, and prisons and probation.
Progressive support:
Insights from the literature:
Progressive support models address an individual’s needs in a comprehensive and integrated manner, recognising the interconnected nature of various aspects of a person’s life, allowing for a more thorough understanding of the challenges an individual may be facing, and addressing underlying issues and root causes rather than merely treating symptoms.
Surrey-specific insights from the primary research:
Primary research findings highlighted that many service providers and service users are in support of adopting more holistic and progressive support models, whereby support offered considers the full array of needs a person may have, from mental health to physical health needs and emotional and social wellbeing. One service provider suggests “you need to look at the bigger picture” when supporting an individual experiencing multiple challenges at any one time (Interview IP52, person supporting people with lived experience of multiple disadvantage). Another commented:
“I’d like to see it be the case that an individual that enters a service for whatever need is then holistically assessed and that there is a workforce that is then upskilled to deal with any number of those issues or to at least recognise and identify those issues and then support that individual to go on to access that service provision.” (Interview IP50, person supporting people with lived experience of multiple disadvantage)
This progressive, ‘whole person’ approach allows for the delivery of more personalised care that is bespoke to an individual ‘as a whole’, rather than catering to ‘one part’ of an individual (i.e., supporting only one of the challenges they are experiencing). Often, this personalised care has the potential to be more effective as people are “nurtured through the service” and supported in their full recovery journey; past, present, and future (Interview IP27, person supporting people with lived experience of multiple disadvantage)
Interpretation and implications:
Progressive support models aim for sustainable change by considering long-term goals and incorporating strategies that promote lasting wellbeing. Successful proof of concept models such as Changing Futures (and similar national and local models and pilots) demonstrate pockets of excellence which could be sustained as long-term multiple disadvantage initiatives in Surrey to reach a wider cohort. These approaches contrast with short-term, isolated interventions that may not lead to enduring positive outcomes by instead promoting accountability and empowerment by involving individuals in decision-making processes and fostering a sense of agency over their lives. Progressive models also foster collaboration among different service providers and sectors, ensuring that interventions are coordinated and aligned to meet the diverse needs of individuals. Changing Futures works in collaboration with partners across the system, including Adult Social Care.
Relational models of working:
Background and insights from the literature:
Relational models seek to ‘get to know’ the individuals they are supporting and build a rapport that provides a platform for build more trust between people and organisations, better connection with services, and support individuals with power, choice, and autonomy. [51]
Relational approaches take the time to ensure that a positive relationship is built first, upon which other support work and positive changes can take place. [52] Relationships are there considered ‘a transformational tool’, providing a basis for support workers to identify and address other issues facing the person they support.
“It restores that faith, hope and belief that I can break away from this life, this stigma, this box that I’ve been put in.” (Interview IP05, person supporting people with lived experience of multiple disadvantage)
With relational models, people with lived experience are supported throughout the support process and are engaged when they are ready to do so, only pulling in support specialisms at the right time and the right place. Changing Futures Northumbria’s ‘The Liberated Method’ provides a strong example of delivering public services in alignment with a relational model works well for the multiple disadvantage cohort. They described the effectiveness of this model, explaining that: “Designing public services around relationships is far more effective. People who have bounced around various public services for years start to positively change how they see themselves, the community, and the world when they’re contributing to a relationship and are understood.”
Surrey-specific primary research insights:
There is also professional stigma with regards to medical models of care and relational models of care, with the former sometimes being seen as superior. Working with people experiencing multiple disadvantage requires balancing and recognising the value of both models of care. There is also a need to continue to ensure people are seen as people and treated with respect and dignity. As one research participant highlighted:
“I just think it needs to move from a more of a clinical model to a more of a psychological understanding model. That’s a simple thing really. But it’s a huge move with some of these organisations…Are we really dealing with the problem or are we sticking plasters over it?” (Interview IP01, person supporting people with lived experience of multiple disadvantage)
Research participants considered ensuring consistency in interactions and working with people over a longer period in order to build relationships as integral when supporting people experiencing multiple disadvantage:
“To be seen, to be heard, to be validated and not to be judged, to be respected. You know when you’re homeless and you’re filthy and you’re on the streets, to have somebody treat you with some respect and to value what you have to say is very meaningful, it’s very impactful. It’s the start of building that relationship up to receive support.” (Interview IP05, person supporting people with lived experience of multiple disadvantage)
Assertive outreach:
Background and insights from the literature:
Assertive outreach is characterised by working with service users in their own environment. The flexibility of approach allows services to be provided to service users who may not otherwise receive them where they feel most comfortable.
Surrey-specific primary research insights:
In Surrey, the Bridge the Gap service includes around 22 outreach workers who work in this way. Professionals in these roles are described as “the glue” between statutory services that support people experiencing core multiple disadvantage risk factors and the service user:
“I look at the role as being the glue that keeps the services together…they get a relationship with that particular worker, and honestly that can fly. So, I feel like that is a major contribution that Bridge the Gap workers will have made to get those services together.” (Focus group FG04, person supporting people with lived experience of multiple disadvantage)
One example of outreach workers offering invaluable support is with missed appointments. If a service user is unable to attend an appointment, the service provider may presume that the client is ‘disengaged’, as one service user explained:
“i-access could be more sympathetic, just asking why an appointment was missed would be nice instead of receiving a text. It would have been nice for someone to call.” (Qualitative survey QS23, service user with lived experience of multiple disadvantage)
However, BTG outreach workers act as advocates for the individual and can better understand the various factors that may prevent someone from attending an appointment i.e., the service user may feel overwhelmed, it may not be the right time for the service user to access support, they may not have access to a phone, or they may have missed the letter with the appointment date.
“We just try to get to know them and find out from them what it is that they wanna change about their lives. So, we’re not assuming that they that they want to tackle anything in particular cause they might not want to.” (Focus group FG04, person supporting people with lived experience of multiple disadvantage)
In some Changing Futures programme delivery areas, outreach workers may be referred to as ‘navigators’. The aim of this role is for the service use to have a trusted person who is their single point of contact and overcome the challenge experienced by service users in navigating the system and various services as the outreach worker takes on this role on behalf of the beneficiary. It is important for outreach workers or navigators to have smaller caseloads to enable relationship building, time and capacity to develop trust and a relationship with the client and enable them to provide a holistic and personalised service.
“When you look at Bridge the Gap, individuals can access those services and actually it’s a joined-up approach to how somebody will work with that individual. But it would be great to have someone to hold that person, being a lead, speaking for that person, rather than five different agencies all kind of trying to pull a multi-agency meeting together that no one’s got time to attend”. (Interview IP50, person supporting people with lived experience of multiple disadvantage)
“It’s almost like as soon as you get into a service or soon as you ask for help from the service, you’ll contacted by an advocate who’s there to almost facilitate for you, build that relationship up so that you can go through the system with that individual”. (Interview IP01, person supporting people with lived experience of multiple disadvantage)
One service provider shared a clear description of how services should approach multiple disadvantage, placing emphasis on empowering the individual and ensuring care is both person-centred and trauma informed.
Service provider’s account of delivering person-centred care:
I know there is this drive to get everybody in services, like it’s a good thing. Well, you know, I’m not sure what’s good about being in services, I think services keep people stuck.
So, somebody presents to a service, they’re in the middle of absolute chaos, injecting drug use or drinking. They go to i-access, usually because somebody has told them to, or told them a hostel will take them if they engage in treatment services, or probation will tick that box if they engage in treatment services.
I’m working with loads of people who come under i-access and what happens is they go once every two weeks to pick up their script for their methadone or Subutex if they’re on opiates, and they go through the same old stuff: “How much do you drink?”, “Are you still using?”
That’s it, the starting point. But it shouldn’t be the starting point.
The starting point should be the kind of the questions like: “Tell me about when this started”, “When do you think it became out of control?”, “What are the benefits for you at the moment for using?”
Let’s have a look at the root causes without asking people to disclose and divulge all kinds of trauma.
Strength-based practice:
Background and insights from the literature:
Strength-based practice is a collaborative process between the person supported by services and those supporting them, allowing them to work together to determine an outcome that draws on the person’s strengths and assets.
The phrases ‘strength-based approach‘ and ‘asset-based approach‘ are often used interchangeably. The term ‘strength‘ refers to different elements that help or enable the individual to deal with challenges in life in general and in meeting their needs and achieving their desired outcomes in particular. These elements include:
- their personal resources, abilities, skills, knowledge, potential, etc.
- their social network and its resources, abilities, skills, etc.
- community resources, also known as ‘social capital’ and/or ‘universal resources’. [53]
Peer support:
Background and insights from the literature:
Peer support is a supported self-management intervention whereby people use their own experiences to help each other and happens when people with similar long-term conditions, or health experiences, come together to support each other. Some examples of peer support groups in Surrey include:
- Recovery Cafés are social hubs for people who are in recovery from drug or alcohol addiction. They provide a safe place to support engagement, to socialise, and meet with staff and other people who are in recovery.
- SMART Recovery (Self-Management and Recovery Training) is a programme to help people manage their recovery from any type of addictive behaviour. This includes addictive behaviour with substances such as alcohol, nicotine or drugs, or compulsive behaviours such as gambling, sex, eating, shopping, and self-harming. SMART teaches self-empowerment and self-reliance in meetings that are educational, supportive, and focused on open discussion. The 4-point programme includes building and maintaining momentum, coping with urges, managing thoughts, feelings, and behaviours, and living a balanced life.
- Peer mentor programme support those who have completed a treatment pathway and are currently stable in their recovery journey. Peer Mentors use their lived experience as a tool to help motivate and generate momentum in other service users who may be finding it hard to engage fully into treatment.
- Fellowship meetings such as Alcoholics Anonymous (AA) and Narcotics Anonymous (NA) promoted and supported. Fellowship meetings provide support to those in recovery in the form of group therapy. Being part of a fellowship helps to build long lasting friendships with like-minded people, encourage one another to live a life of sobriety, act as a talking therapy to help those overcome deep-rooted trauma, and fight boredom or loneliness.
Peer support groups can take place either on a one-to-one or group basis, as well as in-person or virtually and is enabled through relationships that build mutual acceptance and understanding. The power of peer support lies in connecting people with shared experience to create an encouraging, inspiring, and safe space. This personalised, holistic support focuses on wellbeing and understanding the value of lived experience, rather than focusing on medical interventions. [54]
Surrey-specific primary research insights:
Research participants highlighted that there are limited peer support groups for wider challenges relating to multiple disadvantage and core risk factors within Surrey. One participant reflected:
“I think we tend to look at peer support from the view of substance misuse and mental health, all great, all needed, all valuable. But actually, there’s something to be said for peer support with an individual experiencing extreme poverty and, you know, and linking people in that have that real understanding. […] I think peer support has real value in many, many areas and maybe peer support around multiple disadvantage would be of value. I mean when you look at Bridge in Gap, obviously you know, individuals can access those services and actually it’s a joined up approach to how somebody will work with that individual. But it would be great to see maybe some peer support around that and better hand holding in services.” (Interview IP50, person supporting people with lived experience of multiple disadvantage)
Practical support:
Surrey-specific primary research insights:
Research participants highlighted that practical support such as offering cups of tea and coffee, having washing machines available to use, and providing hot showers and food, are also important for service users experiencing multiple disadvantage. A handful of service providers feel that some services are “pushing people towards treatment” when instead services should be “meeting the person where they are at” (Interview IP18, person supporting people with lived experience of multiple disadvantage). For example, participants suggested that undertaking a task that a person may find difficult, offering the support an individual needs in that specific moment, which could be anything from seeing friendly face, going for a walk with someone, helping to read a letter, or buying bus tickets. Voluntary and community organisations were reported as valuable providers of practical support in the primary research.
Having a specialist service for multiple disadvantage:
Surrey-specific primary research insights:
Some research participants identify a need for a specialist service for multiple disadvantage:
“A team that has access to housing has access to mental health, access to substance use has access to criminal justice. It’s almost that whole kind of team that specializes in those in that kind of multiple disadvantage.” (Interview IP62, person supporting people with lived experience of multiple disadvantage)
“If I had the money, I would take that Bridge the Gap concept and really see how we can spread it across the whole system.” (Interview IP05, person supporting people with lived experience of multiple disadvantage)
“It’s unfair on the individual to say, ‘Right, you’ve got to go there for your mental health, you’ve got to go there for your substance use, you’ve got to go there for your housing, you’ve got to go there for your benefits…’ when you could have a specific team that could probably deal with all of that multiple disadvantage.” (Interview IP60, person supporting people with lived experience of multiple disadvantage)
Interpretation and implications:
Having a Surrey-wide specialist multiple disadvantage service would ensure that people facing by multiple disadvantage receive targeted and bespoke care designed to meet their specific needs. This could be a new service or build on existing approaches in Surrey including Bridge the Gap specialist outreach service.
The NHS operational planning guidance 2024/25 prioritises the need to continue to deliver against the 5 strategic priorities for tackling health inequalities and to be including within the planning “meeting the needs of inclusion health groups through implementation of the inclusion health framework”. This includes delivering integrated and accessible service for inclusion health groups including those experiencing multiple disadvantage. The planning guidance highlights that funding can be provided through core Integrated Care Board (ICB) allocations to support the delivery of system plans developed with public health, local authority, VCSE and other partners. Alternative funding options such as the Better Care Fund are also highlighted for proven areas of preventative impact where the avoided costs are also supported by the health and wider public services in Surrey.
By investing in what is working well for Surrey, a specialist multiple disadvantage service could help to coordinate access to services for people at the time and in the way they choose. Interview participants identified key factors that may support the effective delivery of support to meet the needs of people experiencing multiple disadvantage, these include:
- Providing person-centred care over the period of time required based on individual need, thus avoiding short-term and rigid structures, and instead encouraging flexibility.
- Engaging with appropriate specialist support services (i.e., substance use, mental health) when the individual facing multiple disadvantage is ready. They should continue to be support by the specialist multiple disadvantage team throughout the process.
- Aiming to be outcomes-driven rather than focusing on outputs and performance indicators.
- Being founded on the principles of trauma and psychologically informed approaches.
- Being dedicated to meeting individuals where they are at, this can be achieved through relational and assertive outreach models of working. The voluntary and community sector are well-placed to deliver this approach.
- Involve people with lived experience are involved in the development of any specialist multiple disadvantage service and/or team to ensure it is designed to best meet the needs of this population.
Surrey can also learn from national work taking place to support multiple disadvantage. For example, Nottingham City Council has set up a Practice Development Unit. The unit aims to promote and facilitate collaborative learning among those who work with people experiencing multiple disadvantage.
6.5. ‘Overcoming hurdles’: barriers preventing people from accessing services
This section discusses the evidence suggesting that service thresholds, eligibility criteria and referral pathways can be barriers to service access that can place people experiencing multiple disadvantage at risk of exclusion from services.
Routes to ensuring services are accessible to everyone who needs them are discussed, as well as tailored solutions to addressing the specific intersectional challenges faced by each individual. Everyone should have access to tools and skills to participate fully in the economy and society, this includes consideration of factors such as equity of experience, the provision gender-specific services, services for people with a neurodevelopmental condition, as well as support for people facing digital exclusion, language and translation barriers, and cultural differences.
Place-based service delivery is also an important consideration due to Surrey’s large geographical area and services should offer improved flexibility and continue to adapt to the specific needs of a place so that people everywhere can expect the same quality of service.
This section considers the evidence suggesting support services tend to follow standardised approaches and models that are not always sensitive to the diverse needs of individuals experiencing multiple disadvantage. Logistical barriers that impede the smooth delivery and receipt of services are explored, including transport, form filling, inflexibility and waiting times.
6.5.1. Service thresholds and eligibility criteria risk excluding people from accessing support
Surrey-specific primary research insights:
Service providers and service users alike found eligibility criteria and service thresholds to be one of the biggest barriers to accessing support for people experiencing multiple disadvantage, putting those individuals at risk of exclusion from services. One participant stated that:
“Even though it is called referral criteria, it is actually exclusion criteria…the system is incentivised to make its walls as tall as possible to limit the amount of people that meet its criteria so that it can in some way balance the amount of people it’s got employed against the number of people who would like support.” (Interview IP62, person supporting people with lived experience of multiple disadvantage)
Another participant noted the paradox within service thresholds, whereby the restrictive thresholds enable the most vulnerable individuals to be supported, but at the same time they can be seen to prevent people accessing support early on when their symptoms are presenting as mild:
“Thresholds are an interesting one because actually, the money that we’ve got means we can only deal with the most complex and the most difficult, but actually, by supporting some of the people who are milder, you prevent that. […] Whereas actually the reality is what we are doing is by having a resource restrictive environment that is setting thresholds which are too high for some people until they become ill enough to get in.” (Interview IP12, person supporting people with lived experience of multiple disadvantage)
One research participant reflected that excluding people from services on the basis of risk simply displaces the cost and moves them further away from the service that they need and towards the risk of harm:
“For somebody to be told: ‘You’re not bad enough’, it’s like: ‘How bad do I have to get before I get a service that I need?’ … It reaffirms their core beliefs around: ‘Oh, obviously I’m not good enough… I have to get really, really bad to get into that service’. It’s not the right narrative to be giving.” (Interview IP01, person supporting people with lived experience of multiple disadvantage)
Another participant shares the impact of exclusion on the service users they support:
“‘Nobody cares about me, nobody’s going to support me’. You know, a sense of helplessness. I mean, for lots of people, the shame of having to come forward and say I need help is bad enough to be then told ‘it ain’t bad enough quite yet’.” (Interview IP05, person supporting people with lived experience of multiple disadvantage)
Services can be also difficult to access and navigate, with many individuals affected by multiple disadvantage presenting to multiple services across the system. From both a service provider and service user perspective there is a lack of awareness of what support is available for people affected by multiple disadvantage. This includes information on the type of service, to whom they are available, opening times and how to make contact:
“Not only do individuals not know where to go, but sometimes organisations don’t know where to signpost to either.” (Focus group FG06, person supporting people with lived experience of multiple disadvantage)
Referrals approaching release from prison:
Background and insights from the literature:
When an individual is approaching release from prison, referrals to support services such as healthcare and housing can be made up to 12 weeks prior to release and within 28 days post release. Referrals can be made by prison staff, reconnect services, probation, liaison and diversion services, self, or family.
RECONNECT is the care after custody service that seeks to improve the continuity of care of people leaving prison or an immigration removal centre (IRC) with an identified health need. This involves working with them before release to support their transition to community-based services. RECONNECT services aim to improve the wellbeing of people leaving prison, reduce inequalities and address health-related drivers of offending behaviours. Whilst not a clinical service, RECONNECT offers liaison, advocacy, signposting, and support to facilitate engagement with community-based health and support services.
Surrey-specific primary research insights:
Reflections from research participants suggest that individuals experiencing multiple disadvantage are at high risk of harm if referrals are not made, received, and responded to in a timely manner. A research participant working in probation commented on the lack of flexibility and forward planning imposed by the 12 weeks prior to release referral rule:
“When we’ve got somebody leaving prison, you know, we can’t make referrals too far in advance. So, I’ve got somebody that’s been in prison for 10 years. You think that actually, if I know that they’re being released a year down the line, why can’t I start making the referrals then? Why can’t I let people know that actually, somebody’s going to be coming out in six months and they’re going to need appropriate housing. Why do we have to do it 12 weeks prior to release or, even worse, wait for assessment to be done once they’re released?” (Interview IP54, person supporting people with lived experience of multiple disadvantage)
6.5.2. Services should recognise the diverse forms multiple disadvantage takes and ensure they are accessible to everyone who needs them
Support services tend to follow standardised approaches and models that are not always sensitive to the diverse needs of individuals experiencing multiple disadvantage. [78] Primary research findings suggest that consideration is needed around how areas of unmet needs and logistical and operational barriers experienced by people facing multiple disadvantage can be further supported in Surrey to ensure equity in access to resources and opportunities, and that individuals have positive service interactions that align with their specific needs
Diversity and neurodiversity:
Background and insights from the literature:
Services need to be accessible and work for everyone, regardless of race, sexuality, gender, religion, disability status and age, including those who are neurodivergent. Whilst the medical diagnostic model is important as it guides the individual to both the types of support, treatment and prognostic factors related to that condition, in reality it is more of a holistic approach using a biopsychosocial model that is necessary for this group. This model considers biological, psychological, and social factors and their complex interactions. Instead of inappropriate use of resources, appropriate targeted interventions can be offered which have greater cost benefit and also greater impact. For example, offering psychodynamic psychotherapy to an individual with poor emotional understanding will have lesser impact than offering them community support to help them access services and improve their broader social functioning. [70]
The Emotional and Mental Wellbeing in Surrey Adults JSNA chapter reports that nationally access to psychology, speech and language, and occupational therapy services after diagnosis is to be similar or better than in 2016. Generally, access was reported to be better for people with learning disabilities than for those diagnosed with autism who do not have learning disabilities. But access to psychology and occupational therapy assessments was reported to have improved in a substantial number of places for those without learning disabilities. There is no data at county level for comparison currently.
Surrey-specific primary research insights:
Research participants felt that often the system is not designed for the needs of individuals with neurodevelopmental conditions and accessing support is often extremely difficult. One specific area of unmet needs includes support for people awaiting diagnosis or with a diagnosis of neurodevelopmental conditions and gender-sensitive services. One service user shared:
“I waited two years for diagnosis regarding autism, and my partner is told to expect a four year wait for ADHD diagnosis confirmation.” (Interview LERO, expert by experience)
Some participants reflected that the expectation is that the person themselves should be able to self-manage, yet this is often not the case for these groups.
“Neurodivergent individuals I think have traditionally always had a very difficult experience of accessing services and getting the right support at the right time. We also know we have our sort of global majority population groups who perhaps again we don’t have the right spaces available, the right communication.” (Interview IP63, person supporting people with lived experience of multiple disadvantage)
One research participant highlighted the limited availability of current services for ongoing care, case management, therapeutic intervention, or support for individuals with complex presentation related to their mental health needs in Surrey. They report that there are very few, if any, such services around the country. Where they do exist, they reflected that these tend to be only in highly specialist services with limited access and limited resource for ongoing care and rarely, if any, specific case management.
Logistical and operational barriers:
Logistical barriers may include financial constraints, transportation issues and a lack of services in underserved areas, exacerbating difficulties in seeking help. These barriers are mostly practical and operational challenges that impede the smooth delivery and receipt of services. The infographic below integrates findings from the literature review and primary research to summarise eight key logistical and operational barriers likely to be faced by people experiencing multiple disadvantage in Surrey.
Travel, transport and geographies:
Lack of reliable and affordable transportation can be a significant barrier to accessing services, especially in rural or underserved areas. Individuals may struggle to access healthcare, education, employment services, and other essential resources. Services users would like to see:
“More support for public transport […] more bus services, travelling is hard.” (Qualitative survey QS20, service user with lived experience of multiple disadvantage)
Research participants reported that some service providers may assume every person in Surrey has access to a car, which is not the case for the vast majority of individuals affected by multiple disadvantage. Many therefore rely on public transport to access services, however, service users shared how when using public transport to attend appointments and to access services, they often find public transport options to be infrequent, indirect (i.e., multiple connections to reach a destination), unaffordable and/or unreliable, these factors pose significant barriers to access. [71] Efforts are being made across the system to mitigate this.
Limited operating hours:
Services with restricted operating hours are often inaccessible for this population as their experiences of multiple disadvantage are not restricted to occurring during standard business hours. Limited service opening-hours can make it difficult for people to schedule appointments or access support. This is a particular challenge with mental health services, as one research participant explained:
“If you look at the normal NHS SaBP provision for mental health services, it’s 9am-5pm. The app service in Surrey is 9am-5pm. However, three quarters of Section 136 detentions[] for people that are in crisis take place out of hours, so whether that’s the weekend or after 5pm. There are very few services outside of the emergency services that provide any support. Safe Havens are one, and are doing a fantastic job, but their time is still limited, it’s not 24/7. [*] There is a 24/7 Crisis Line and I know that is well used, but what is it actually that the service delivers? There’s such a disparity and I think that’s failing people.” (Interview IP26, person supporting people with lived experience of multiple disadvantage)
[*] Section 136 allows the police to take you to (or keep you at) a place of safety. [**] Safe Havens open daily from 06:00-23:00
Long wait times for appointments and referrals:
There is a delay in accessing services, particularly support for urgent needs. These long waiting times can be particularly challenging for people experiencing multiple disadvantage, and often exacerbate existing challenges and hinder timely support. People waiting for a referral for an assessment for neurodevelopmental conditions such as ASD and ADHD reported long waiting times.
“We’re seeing a lot of people who are wanting to know if they have ADHD or ASD, and the lengthy wait times on the NHS, I think it’s about four or five years…I understand that they’ve paused referrals due to demand… so it leaves people with this sort of uncertainty.” (Focus group FG05, person supporting people with lived experience of multiple disadvantage)
“I think you need a service that fills in the gap, while you can’t get support, I think there needs to be like…. there is like a massive waiting list and people like addicts and homeless, you need instant help. You can’t wait six months or nine months. It’s not a thing. You need an interim.” (Interview IP03, person supporting people with lived experience of multiple disadvantage)
Lack of service flexibility:
Primary research findings indicate that there is a lack of flexibility from services in terms of scheduling options, ability to change the appointment method, operation times, eligibility criteria, and options around the way support is received. This inflexibility can result in people experiencing multiple disadvantage having a negative and damaging experience with support services, and in many cases, not receiving support at all. One service provider reflected:
“It’s a barrier to entering into services where an individual is feels they’re going to be punished because maybe they didn’t pick up seven times because of the place they were in, so I think it’s how we can be more open.” (Interview IP50, person supporting people with lived experience of multiple disadvantage)
Participants identified that although services do not operate a ‘three strikes and you’re out’ policy, some services users continue to report experiences of this exclusion from services, particularly after missing appointments or being ‘disengaged’. This is more pertinent in substance use and mental health services. One participant felt services should be more flexible and understanding, commenting that:
“If somebody’s cancelling appointments at the last minute, instead of just writing them a letter and saying, “you’re discharged”, try to work out why that is, what’s happening?” (Interview IP54, person supporting people with lived experience of multiple disadvantage)
One participant noted the impact of reduction in pharmacy provision of support such as needle and syringe provision and substitute prescription drugs (such as methadone or buprenorphine). They state:
“Pharmacy provision is so important in terms of delivering the medications that we wanna be able to prescribe […] pharmacies used to provide more and more and I think that’s dwindling, that’s a barrier to treatment for people that have got banned from multiple pharmacies and they’re really, really struggling to get hold of a pharmacy or maybe they haven’t been banned from any but there’s just none in their vicinity and they haven’t got transport to be able to get to the pharmacy that is the only one that will take their prescription. So you know, that’s one of the barriers to getting into treatment.” (Interview IP46, person supporting people with lived experience of multiple disadvantage)
To mitigate this, there could be an extension of shared care opportunities for people in recovery from drug use to provide a more diverse choice in how they acquire substitute prescription drugs, for example, individuals could receive a prescription from their GP or from the drug and alcohol treatment service depending on their preference. Having additional shared care options in neighbourhoods and communities could continue to remove barriers for individuals who are unable to travel to a service and allow service users a choice depending on with whom they have a good rapport.
Form filling:
Complex registration or application processes can deter individuals from seeking assistance: Often services have lengthy paperwork and administrative requirements which can act as a barrier to access, particularly for those with low literacy levels. Digital accessibility is also a factor here as many services now need to be accessed online. Individuals without internet access or digital literacy skills may struggle to navigate online registration, appointment scheduling, or virtual service delivery.
“There’s lots of waiting, lots of filling in forms, lots of not knowing what’s going on.” (Focus group FG04, person supporting people with lived experience of multiple disadvantage)
Environment:
Physical location and environment of some services were also considered a barrier to access, with participants describing some locations as “unwelcoming” and “harsh” (LERO). One service provider shared:
“I was thinking about our neurodivergent communities, and it was funny, we were in a meeting the other day and all of our buildings; the lights are so bright…. if you’re sitting in a room and your senses are really overloaded, you’re not going to be able to communicate what you’re what you’re trying to communicate very effectively. So, environment is sometimes an obstacle as well.” (Interview IP63, person supporting people with lived experience of multiple disadvantage)
6.6. ‘Under pressure’: strategic challenges create disruption and discord
This section reports evidence on the vital role commissioning models play in addressing multiple disadvantage, since they determine what type of services are delivered in Surrey and the way they are delivered. Current strategic commissioning could offer improved flexibility, choice, and innovative solutions for people facing multiple disadvantage. There is enthusiasm from parts of the system supporting people experiencing multiple disadvantage to adopt progressive commissioning models, embrace innovation, and commit to sustainable system change.
The primary research, in particular the feedback from people with lived and living experience of multiple disadvantage, identifies that some statutory services supporting people experiencing multiple disadvantage often offer a ‘one size fits all’ support approach. This approach does not always best meet the needs of this population who do not typically fit neatly into standard service criteria and thresholds. This section explores how current commissioning models in Surrey could be adapted to support improved outcomes for individuals facing multiple disadvantage.
This section also considers how fragment funding, such as short-term or individual grants or contracts offered to try and manage demand pressures, can present challenges in long-term, strategic planning. Organisational capacity also puts pressures on services to deliver, with factors including staff recruitment and retention, resource and capacity challenges, ownership of multiple disadvantage, reflective practice, and training opportunities having the potential to either help or hinder system change.
6.6.1. Current commissioning models
Background and insights from the literature:
Commissioning is the process by which health and care services are planned, purchased, and monitored. Activities including assessing needs, setting priority actions, service planning, service procurement and monitoring quality. Commissioning arrangements and responsibilities can be complex and should regularly shift to meet the need. [55] In Surrey the NHS Integrated Care Boards and Surrey County Council are the bodies responsible for leading commissioning and transformation of services to meet residents’ needs. They have to follow statutory rules and regulations to ensure that commissioning is undertaken in a fair and transparent way.
Surrey-specific primary research insights:
Primary research findings identify the need for a priority review of current commissioning models for services supporting people facing multiple disadvantage to assess their coherence, effectiveness, efficiency, impact, and sustainability, as well as evaluate the long-term soft and hard outcomes for individuals experiencing multiple disadvantage receiving support.
One research participant suggested conducting a full review of current strategic commissioning prior to making further decisions around care and support for people experiencing multiple disadvantage:
“Before we do any strategic commissioning I would like to review the whole system and turn it on its head and you know, make it fit for purpose and then fund the right things at the right time. I think we often end up firefighting and literally funding the tip of the iceberg just to keep us from head above water just which is very short term view.” (Interview IP76, person supporting people with lived experience of multiple disadvantage)
One research participant shared that having one provider responsible for a significant proportion of the service provision can limit the service user choice and access to a diverse and flexible market of providers to meet their needs in a bespoke and person-centred way. The participant commented that:
“I think where you have all your commissioning money focused in some big areas of provision, I think there’s a risk there. You don’t have a diverse and flexible market of providers that you can tweak and adapt and change as you’re developing that sort of outcomes and lived experience-informed response. You’ve just got these big monolithic blocks of statutory service which are, even with the best will and intentions, are really hard to turn around. So, if you do have a more diverse and dispersed service response then I think you’ve got a better chance of doing that.” (Interview IP03, person supporting people with lived experience of multiple disadvantage)
Some participants highlighted the need for individuals with lived experience of multiple disadvantage, as well as local communities and VCSEs, to drive the way commissioning is structured and funded. This would include involvement in the identification of commissioning models for this population, in addition to the co-production of funding structures, service design and service specifications. Commissioners go through a robust process of needs assessments, stakeholder engagement as part of the commissioning process. However, one research participant commented that commissioners should be better informed about areas of needs and gaps prior to decision-making:
“Commissioners don’t always have the knowledge or don’t have the experience to be able to commission some of the service work.” (Interview IP16, person supporting people with lived experience of multiple disadvantage)
This sentiment was echoed by members of the LERO who emphasised the importance of relevant training for commissioners working in commissioning for multiple disadvantage.
Interpretation and implications:
Adopting progressive commissioning models for services supporting people experiencing multiple disadvantage could offer diverse solutions and ensure that services are able to adapt more readily to presenting and evolving needs. This is supported by the NICE guideline on delivering integrated health and social care and the national framework for action on inclusion health which highlights that targeted approaches that are person-centred, empathetic, non-judgemental, inclusive, and pay attention to the diverse experiences of people using the service are needed to support this vulnerable population. [66] [67] Likewise, OHID guidance on commissioning alcohol and drug treatment and recovery (August 2022) highlights that the approach to designing and contracting treatment and recovery support services should be well-thought-out, inclusive, and in line with the interests of its affected populations. This includes following a collaborative commissioning process, integrating with other services that provide support for people affected by problem alcohol and drug use, and developing commissioning plans that are appropriately financed to provide accessible, good quality services. Commissioners should also proactively seek engagement from partners in commissioning decisions and processes and consider opportunities for joint or integrated commissioning. The current commissioning process incorporates these key guidelines and principles. However, the process can be further strengthened by incorporating user voice in the development of future service specifications to support people experiencing multiple disadvantage. This approach is also being supported by Surrey Substance Use Partnership (see section below on joint commissioning).
Joint commissioning:
Background and insights from the literature:
Joint commissioning refers to arrangements in which public bodies look to undertake the planning and implementation cycle collaboratively – this could be for a whole population or in relation to people with particular needs (such as those with a complex disability) or facing common challenges (such as being homeless). There are services overseen by Public Health in Surrey County Council which benefit from the opportunity of being jointly commissioned with other partners such as the High Impact Complex Drinkers service (HICD) and the Cuckooing service which are jointly commissioned with the Office of the Police and Crime Commissioner (OPCC). Joint commissioning of services can involve the organisations ‘pooling’ their related budgets so that the funding available to meet these needs is shared, or aligning budgets so that the funding is more transparent but is still held by the individual organisation. [56]
Surrey-specific primary research insights:
One research participant commented on substance use services in Surrey, explaining that they felt the current commissioning process contributes to less integrated ways of working. The participant understood that Public Health hold the statutory responsibility to commission substance use treatment services, however, reflected that funding allocation could help support a more holistic response to the need of people with multiple disadvantage:
“Substance misuse needs to be taken out of its silo. I think it is in a silo partly because it’s Public Health commissioned, partly because there’s a lot of discrimination against people who have a substance dependency and I think both of those things then create quite an exclusionary process, it’s really unhelpful…, I do feel there’s like, well, you know, ‘if you’re using drugs there’s nothing more we can do for you’.” (Interview IP62, person supporting people with lived experience of multiple disadvantage)
Interpretation and implications:
To see more information on adult substance use commissioning, please refer to the Substance Misuse JSNA chapter. In 2017, Surrey began a programme of change in the provision of adult structured substance use treatment in order to create a more integrated service. A service model was developed with SaBP, community providers, and peer mentors which brought together harm reduction, treatment for less complex need and treatment for more severe and complex dependencies under one service know as i-access, provided in partnership by SaBP and a community provider. The remodelled i-access service begun to operate in 2018, and in 2020 a co-operation agreement was made between commissioners, Surrey County Council and SaBP and their community partner (now Via). The service has been overseen by a Substance Misuse Programme Board since 2018 and includes a shared oversight and responsibility for delivery of treatment, performance outcomes, partnerships and budget management. In 2025/26 a whole systems substance use treatment and recovery assessment will be undertaken, and the voice of people with lived and living experience and wider stakeholders will be central this.
Surrey Substance Use Partnership brings together strategic leads to take a whole systems approach to preventing and reducing the harm caused by substance use, focusing on addressing the root causes of substance and alcohol use, rather than treating the symptoms in isolation, in line with the national strategy ‘From Harm to Hope’. Partners work together to address four priorities: breaking drug supply chains, delivering a world class treatment and recovery system, a generational shift I demand for drugs, reducing alcohol and tobacco related harm. This provides a forum for joint working and collaboration across organisational boundaries.
6.6.2. Redistribution and restructuring of funding structures to support service stability and long-term planning
Background and insights from the literature:
There is insufficient long-term national funding to help services supporting people affected by multiple disadvantage to provide continual support, in turn, this has significant impact on the sustainability and quality of local service delivery and retention of a competent workforce. The short-term and sometimes ring-fenced nature of some grants also presents councils with a challenge when it comes to long-term, strategic planning.
The Local Government Association (LGA) reported that in recent years, councils in England have seen a rise in the number of short-term, ring-fenced, small grants they receive annually from government departments and agencies. The LGA calls for an end to fragmented funding of council services and meeting demand pressures through individual grants.
Surrey-specific primary research insights:
Research participants working in the voluntary and community sector highlighted how the availability of funding on a short-term basis presents a challenge to their organisation. For example, it can create instability for many service providers, who are often not able to offer staff long-term contracts or offer people accessing services a guarantee that the service will still be there in the future.
Services also find themselves spending a lot of time and resources applying for funding or contracts instead of delivering services.
“Currently all our funding is piecemeal, we are grateful for it, but it makes it hard to focus on the work as we are continually thinking about sustainability and ‘earning’ the next pot of money to move a project forward.” (Interview IP34, person supporting people with lived experience of multiple disadvantage)
For many service providers, and VCSE organisations in particular, delivering consistent, high-quality work cannot continue without the reassurance of long-term funding. In a survey conducted as part of the primary research for this JSNA chapter, 84 out of 100 local stakeholders agreed that funding might prevent or hamper changes to their organisation
“You will start something up and then the contract ends after a year or two years, so there’s no continuity, staff leave because they’re worried about how we’re going to continue the service.” (Interview IP05, person supporting people with lived experience of multiple disadvantage)
“Funding is only available year on year, and that then creates a challenge to provide a security and a level of consistency for the services, and I often tend to think that there’s a lack of awareness around if a service has been running and then it’s pulled that that then leaves that gap.” (Interview IP15, person supporting people with lived experience of multiple disadvantage)
A further concern raised by service providers is complexity of funding applications, with some commissioned services reporting that applications to Surrey County Council are too complicated. Smaller organisations often lack the manpower and capacity to scope and complete extensive applications within limited timeframes which then places extra stress on an already overstretched system.
“You have to justify what you spend, when you spend every penny, and that’s fine but then you have to demonstrate how does it match what was put in the funding application.” (Interview IP24, person supporting people with lived experience of multiple disadvantage)
Interpretation and implications:
Short-term funding and grants represent poor value for money. As an alternative, providing long-term and flexible funding can provide much better value for the same amount of funding. For example, staff can be offered long-term contracts, allowing time for training, and improving staff retention. It also allows service providers time and resource to identify and implement innovative solutions which prevent crises from happening.
6.6.3. Improving organisational capacity can help the system to effectively respond to multiple disadvantage
Background and insights from the literature:
Organisational capacity refers to the system’s ability and readiness to meet its goals effectively and efficiently. There are many drivers of organisational capacity, including leadership, strategy, governance, skills, human capital, and accountability. In Surrey, some of these drivers have created barriers to organisational change, as described below based on the primary research insights:
Surrey-specific primary research insights:
Leadership and accountability: Strong and effective strategic leadership is essential for improving multiple disadvantage and tackling system priorities. Some research participants highlighted poor leadership and management as a hindering factor to fostering change:
“There’s never any change at the top. You kind of feel like it gets filtered out as it as it goes to the top…you never see the changes that need to be implemented.” (Interview IP49, person supporting people with lived experience of multiple disadvantage)
Tackling multiple disadvantage requires ownership, system-wide engagement, and accountability:
“It is the hierarchy in Surrey… they move so slow too and I think it’s hampered by too much management.” (Interview IP41, person supporting people with lived experience of multiple disadvantage)
Human capital (staff recruitment and retention): Research participants indicated that frequent staff changes are a concern and may lead to a loss of organisational memory and understanding. Just under three in five stakeholders who responded to the stakeholder survey agreed that staff recruitment might prevent or hamper change such as systems change, service improvement or innovation, in their organisation. A further 53% agreed that staff capacity could prevent change, and 38% identified staff retention as a factor with the potential to hinder progress.
One local challenge for staff recruitment is Surrey’s proximity to London. Due to the wider range of jobs and London Weighting Allowance, staff commonly choose to work within the London boundary.
“What we really need to do is retain staff in posts for, you know, sort of 10 years so they can build up their breadth of experience in terms of working with clients and what resources and services are out there. Otherwise, the churn of staff is, you know, someone comes in for two or three years, they experience burnout and they leave the service. In that way the service is just kind of naturally held back from increasing its knowledge and experience of working with people.” (Interview IP68, person supporting people with lived experience of multiple disadvantage)
In response to the online survey, respondents suggested the following factors could help recruit, retain, and motivate staff in their organisation to better meet the needs of those experiencing multiple disadvantage:
- Improving job security by offering more long-term and/or full-time job contracts
- Increasing pay and awarding competitive salaries
- Improving access to long-term funding for their organisation
- Providing opportunities for career progression
- Increasing training opportunities
- Ensuring staff feel valued and their wellbeing is supported
- Improving communication and collaboration between VCSEs and statutory services
Capacity and resources constraints: Limited resources and capacity, both financial and human, can make it challenging for services to develop and deliver tailored support to meet the demand. Research participants reflected that limited resource and capacity can result in a lack of access to crucial services such as healthcare, education, housing, and social support which exacerbates existing disadvantages and creates barriers to improving overall health outcomes:
“I don’t believe the services are able to cope with the current demand” (Interview IP26, person supporting people with lived experience of multiple disadvantage)
Secondary care services such as hospitals are a prime example of capacity and resource limitations, with many research participants citing examples when these services appear overwhelmed. Similarly, one participant reflected on similar capacity and resource challenges across the system:
“I know so many agencies where they don’t have that support and the staff are literally having breakdowns.” (Interview IP17, person supporting people with lived experience of multiple disadvantage)
A further example is hospitals with patients being discharged without immediate housing and follow-on care arrangements. One participant shared examples of women from their refuge being discharged from hospital:
“We’ve had instances where women are discharged from hospital back to our refuge, at midnight or three o’clock in the morning with no money. We’re scrabbling about trying to get them, and thankfully they are in our refuge and thankfully, there’s an on-call service who’s trying to help them. I don’t know what happens to anybody else who’s just thrown out literally onto the streets in the middle of the night.” (Focus group FG03, person supporting people with lived experience of multiple disadvantage)
A service user shares a similar experience:
“When I had a breakdown when I was homeless, you know, I was just discharged in my pyjamas in winter like, you know, at three o’clock in the morning, I was discharged in pyjamas. Freezing cold, no coat, nothing. And they didn’t care.” (Interview LERO, expert by experience)
Reflective practice:
Background and insights from the literature:
Since informed approaches require practitioners to engage with people’s traumatic experiences, it may cause them distress as well. It is therefore important that staff wellbeing is protected and that organisations promote a culture that supports staff wellbeing. This includes psychological supervision and debriefing, ensuring no-one’s workload is overwhelming, and a leadership which fosters a culture of learning, trust, and reflection, so that practitioners can say when they are struggling to cope.
Surrey-specific primary research insights:
Some service providers shared their perspectives on the importance of reflective practice and support of staff:
“If you don’t treat your staff with trauma informed care, you can’t expect them to deal with other human beings in that way.” (Interview IP21, person supporting people with lived experience of multiple disadvantage)
“Having support and having supervision and that opportunity for reflective practice is absolutely essential.” (Interview IP36, person supporting people with lived experience of multiple disadvantage)
Research participants shared examples through interviews and/or the online survey of reflective practice opportunities that are currently taking place across Surrey include:
- Management supervisions: these typically take place monthly or 6-weekly. It is a chance for individuals to meet with their manager discuss any issues or challenges.
- Clinical supervisions: these supervisions help to support and develop the knowledge, skills and values of an individual group or team.
- Case discussions: also referred to as case recordings, whereby providers and practitioners discuss individual cases and clients they are working with.
- Team meetings: group meetings with members of the same team coming together to talk about workload, concerns, and any topics of interest to the team.
- Wellbeing days: days allocated for staff to support their occupational mental health and wellbeing. This is particularly important for frontline staff at risk of experiencing vicarious trauma.
- Practice Reviews: these reviews identify learning for future practice, for example, practitioners carry out an informal audit of an area and self-assess their practice. This includes reflections on what is going well and where there is room for improvement.
- Protected Learning Time: this is an opportunity for practice staff to address their own learning and professional development needs.
Skills and training:
Background and insights from the literature:
Training provides individuals with new skills or helps to improve existing knowledge and abilities and it also helps staff stay updated on industry trends and evolving best practices. Ongoing training ensures that providers stay updated on the latest treatment options, and evidence-based practices; knowledge which contributes to delivering high-quality care and improving service user outcomes. Providing professional developmental and growth opportunities also supports staff retention and helps to foster collaborative working.
Surrey-specific primary research insights:
In a survey with 100 stakeholders across Surrey, participants shared the training offered by their organisation. They also provided examples of gaps in training and areas where they would like to see increased training delivered. Just under four in five organisations (79%) provide Equality, Diversity, Inclusion and Discrimination training, a total of 64% provide Trauma Informed Approaches training, and 60% provide mental health training. Many stakeholders identified that some of these trainings should be mandatory. Additional trainings stakeholders would like to access include:
- Trauma Informed Care
- Inclusion health
- Accessing information and support
- Addiction and substance use
- Naloxone access and use
- Lone worker/lone working
- Domestic abuse
- Financial abuse
- Intersectionality
- Working with statutory services
- Mental Health First Aid
- Making Every Contact Count (MECC)
- Supporting people with sensory needs
- Working with people from minority groups
- Nutrition training
- Supporting people with neurodevelopmental conditions
- Supporting people learning disabilities
- Immigration and legal aid
- Carrying out assessment
7. Conclusions and recommendations
7.1. Conclusions
In comparison to the general population, people affected by multiple disadvantage often experience poorer physical and mental health, higher social care needs, and a poorer life expectancy. Multiple disadvantage also puts people at an increased risk of chronic and premature mortality and morbidity. [63] The risks of multiple disadvantage often build up over a person’s life span and more action is needed locally to prevent people experiencing multiple disadvantage in the first instance. Fundamental change is vital at individual, service, and system levels to help people experiencing multiple disadvantage to feel safer, healthier, and thriving to thrive, ensuring that ‘no one is left behind’.
The primary research conducted for this JSNA chapter identifies that Surrey can take a number of key actions to improve both the type of the support available, and the way support is delivered, to our residents experiencing multiple disadvantage.
This JSNA chapter primarily explores challenges associated with ways of working in Surrey, including examples of the impact of siloed working and some organisational relationships on the delivery of integrated care for individuals experiencing multiple disadvantage. The research findings reflect that many statutory services that support people experiencing core multiple disadvantage risk factors are felt to predominantly ‘assess’ and ’treat’ an individual’s assumed primary need as opposed to recognising the interconnected nature of multiple disadvantage. Multiple disadvantage therefore requires stakeholders to work together to achieve shared goals and overcome siloed service constraints. This cultural shift and systems transformation takes time to achieve and requires collaboration and partnership working across the whole system.
The chapter also places a spotlight on barriers to service access, noting that often service thresholds and eligibility criteria risk can exclude people from support. Such barriers to service access can often intensify the challenges experienced by people facing multiple disadvantage.
As a final point, the findings also consider current commissioning structures and identify the need to adopt progressive commissioning models and extend effective joint commissioning to foster flexibility, choice, and innovation. With a refresh of current commissioning structures of services supporting people experiencing multiple disadvantage, Surrey will have an opportunity to approach the work with a wider systems lens, flexing the boundaries and ultimately, achieving better outcomes for people experiencing multiple disadvantage.
People affected by multiple disadvantage can be better supported by services that continue to embody reliability, integrity, and empowerment alongside using a relational, person-centred, and trauma informed model of care. There is an assumption that people experiencing multiple disadvantage always require a web of services placed around them. However, this chapter identifies that there is a place for both relational and medical support models to effectively work in tandem to ensure equitable access, experiences, and outcomes for all.
7.2. Recommendations
“It is no use for us to have power in a system that fails to adapt in response to needs and fails to learn from our experiences!” (Expert by Experience)
The following recommendations have been developed based on triangulated findings from the primary research, secondary data analysis and background literature review described in this report in relation to the health and wellbeing needs experienced by individuals facing multiple disadvantage in Surrey.
This set of recommendations emphasises the overarching need for greater integration and collaboration across local services, enabling an accessible, relational, and person-centred approach to multiple disadvantage in Surrey. The system should prioritise the delivery of integrated services and demonstrate a commitment to strong partnership working and coordination across the whole system. The recommendations also place emphasis on the importance of co-production with people with lived experience of multiple disadvantage, and working collaboratively alongside Surrey’s statutory providers, voluntary organisations, and communities to redesign the way services are delivered for this population.
Working in partnership is essential if the Surrey system is to effectively deliver the recommendations outlined in this JSNA chapter. Therefore, as a priority, there must be a refresh of current governance arrangements for multiple disadvantage in Surrey that will develop a clearly defined and robust partnership structure. This may include stating the ambition to develop a Charter with people with lived experience to identify what a service user experiencing multiple disadvantage should expect when accessing services. These recommendations will form the basis of a 5-year strategy for multiple disadvantage and should be used to leverage support for driving lasting systems change that can be sustained to continually improve the life outcomes for this population.
The LERO will look to Surrey’s Health and Well-Being Board (HWBB) to support these recommendations to build stronger cross-sector partnerships at a strategic and operational level to create flexibility in how local services respond to the people who use them, taking a system-wide view with shared accountability and improved engagement between local commissioners and services.
The HWBB holds the statutory duty to improve the health and wellbeing of their local population and reduce health inequalities. The prevention of multiple disadvantage in Surrey must therefore be a whole system responsibility, with an expectation for all areas of the system to take accountability for improving the life outcomes of this vulnerable population.
| Recommendation | Description |
|---|---|
| Recommendation 1 | Strengthen governance structures by establishing a Multiple Disadvantage Partnership Board |
| Recommendation 2 | Develop a 5-year strategy for multiple disadvantage |
| Recommendation 3 | Improve system-wide data collection and sharing protocols |
| Recommendation 4 | Ensure people experiencing multiple disadvantage are placed at the centre of strategic decision-making processes and involved in the design, commissioning, co-production, and evaluation of services |
| Recommendation 5 | Invest in early intervention and prevention solutions to reduce the prevalence, duration, and impact of multiple disadvantage |
| Recommendation 6 | Prioritise embedding a cross-cutting Trauma Informed Approach at individual, service, and system levels |
| Recommendation 7 | Ensure that key health and care services are commissioned in a way that promotes partnership and integration through the adoption of commissioning best practices for people experiencing multiple disadvantage |
| Recommendation 8 | Redistribute existing funding to provide a range of integrated, accessible, relational, and person-centred services for people facing multiple disadvantage |
| Recommendation 9 | Ensure people affected by multiple disadvantage have access to high quality, effective, and person-centred alcohol, drug and recovery services by conducting a comprehensive review of commissioned substance use services in Surrey |
| Recommendation 10 | Ensure that people experiencing multiple disadvantage are offered a diverse range of mental health services with improved ease of access, flexibility and better outcomes |
| Recommendation 11 | Improve ease of access to housing and accommodation support and ensure sufficient housing options for people experiencing multiple disadvantage |
More detail for each of the recommendations is given below.
Recommendation 1: Strengthen governance structures by establishing a Multiple Disadvantage Partnership Board
A new Multiple Disadvantage Partnership Board should be established that is responsible for overseeing systems change and governance for multiple disadvantage in Surrey. This Partnership Board will take responsibility and accountability for the development and delivery of a 5-year strategy for multiple disadvantage, which includes progressing the priority actions and recommendations identified by this JSNA chapter. The Partnership Board will also take responsibility for agreeing a system-wide definition of multiple disadvantage.
The Multiple Disadvantage Partnership Board should have consistent and full representation from all local partners, including strategic leads across the system such as primary, secondary health care colleagues, local authority, voluntary and community organisations, housing, mental health, substance use and community safety, criminal justice, social care, safeguarding, and other pertinent and passionate stakeholders. Local partners and organisations should demonstrate commitment to this Board and allocate time for attendance and levering support. This Partnership will also work in parity alongside people with lived experience of multiple disadvantage in co-producing joint solutions to strategic issues. System leaders and local partners could continue to recognise that collective actions have a wider impact than the sum of individual actions. In line with this, the Partnership Board will work to achieve ambitions jointly with other pertinent Boards and aligned strategies such as the Mental Health System Committee, Integrated Care Boards, Surrey Substance Use Partnership, Health Inequalities and Core20PLUS Board, Adult & Children’s Safeguarding Board and Surrey Health and Well-Being Board and Strategy.
Strong leadership is pivotal to strengthening governance and driving systems change. Assigned to the Partnership will be a Senior Responsible Officer (SRO) to represent the Partnership, its values, principles, and its priorities. In addition, the Board should identify multiple disadvantage leadership at all levels of the system. An inclusive ‘bottom-up’ leadership approach gives all teams a voice in decision-making and recognises that frontline staff can also provide significant insights that inform and improve decision-making by the Board.
The Partnership Board will also support the creation of platforms for sharing local and national best practices, successful collaboration models, and research and data relating to multiple disadvantage (e.g., develop a Practice Development Unit). This platform could inspire and support ongoing efforts and provide opportunities for knowledge exchange and best practice sharing across the Surrey system.
Developing a robust Multiple Disadvantage Partnership Board will help to establish a unified whole systems approach and foster collaboration, shared accountability, and wiser ownership of the multiple disadvantage agenda.
Recommendation 2: Develop a 5-year strategy for multiple disadvantage
The research has identified the need for a long term and iterative view to system change with a proactive approach to delivering improvements to achieve sustained change at system, service, and individual levels. Partnership working and collaboration can support this.
The Multiple Disadvantage Partnership Board will oversee the development and delivery of a 5-year strategy for multiple disadvantage and utilise the recommendations from this JSNA chapter to inform development. The Partnership Board should ensure that the strategy is fully co-produced with people with lived and living experience of multiple disadvantage.
The 5-year strategy should be flexible, innovative, and iterative. It is important that the strategy is reviewed and updated regularly to ensure alignment with changing needs and other relevant strategies such as the Housing, Homes and Accommodation Strategy or the Health and Well-Being Strategy. These reviews can be co-designed with people with lived and living experience of multiple disadvantage. Partner agencies and system leaders who may be responsible for fulfilling parts of the strategy should be held to account through a robust scrutiny process such as scrutiny committee or external evaluation.
In recognition of collaborative working, the Partnership Board should also leverage support from Surrey’s Integrated Care Boards (ICBs) and work in partnership to clearly set out how the recommendations from this JSNA chapter align with the statutory ambitions, such as those set out in the NHS Long Term Plan, Core20PLUS priorities, and the NHS yearly planning guidance. This strategy should consider how the needs of health inclusion groups, such as those experiencing multiple disadvantage, will be included in future commissioning functions, plans, and strategies.
Recommendation 3: Improve system-wide data collection and sharing protocols
Identifying numbers of people experiencing multiple disadvantage or associated risk factors is a challenge in Surrey due to data governance, data infrastructure and data quality. There is a noticeable scarcity of data and intelligence available regarding multiple disadvantage to inform future commissioning and decision-making processes.
To address gaps in data availability, it is recommended that a population health management approach be adopted to bring together health and social determinants data to identify people who are at risk of multiple disadvantage for priority action and prevention planning. Current IT systems and infrastructure could be reviewed to ensure they are sufficient to enable routine data collection, for example, the option to consistently code information. A lack of coding means there is a lack of data to help understand the true numbers of people experiencing multiple disadvantage and their needs, which in turn impacts effective planning and commissioning.
Surrey should also work to improve the system-wide collection of data on multiple disadvantage and look to align systems and metrics. A ‘whole system view’ of people’s diverse and intersecting needs and strengths will help to drive earlier intervention, influence policy, and deliver improved person-centred support. Establishing a Community of Practice for multiple disadvantage would also provide a dedicated space for troubleshooting issues and making connections with peers for support and shared learning. Likewise, identifying Data Leads in each service area working with data around multiple disadvantage can support collaboration and provide a point of contact to discuss data reporting and recording, and address challenges while identifying trends
Practitioners should also be supported to collect sufficient cultural and demographic information to provide a fuller social context. This would enhance the system’s visibility of people with characteristics that might require adjustments and encourage the adaptation of approaches towards more person-centred and trauma informed care. The creation of secure data-sharing agreements would also allow public services and community agencies to share information effectively while respecting client privacy. This facilitates a holistic understanding of client needs. Supporting systems to improve data sharing where consent is given can prevent the constant retelling of stories and enable more efficient multi-working, speeding up the delivery of services. The inclusion of ‘facts about me’ (a form to record hopes and aspirations) will also contribute to tackling stigma and focusing on strengths.
We should also recognise that qualitative data is an underused but valid source of insight, which can be pivotal in supporting this under-researched cohort. Qualitative insights provide essential context and perspective crucial for interpretation and ensuring insights translate into meaningful action.
Importantly, we should start to foster a culture led by people, not by numbers, and develop an improved human learning system that reflects upon local qualitative and quantitative data from multiple sources and actively seeks to address local gaps in data and knowledge to develop iterative, adaptive local systems, which inform local strategies (like Joint Strategic Needs Assessments), and wider evidence to influence policy and commissioning practice.
Recommendation 4: Ensure people experiencing multiple disadvantage are placed at the centre of strategic decision-making processes and involved in the design, commissioning, co-production, and evaluation of services
The voices and full involvement of people who have experience of multiple disadvantage or been impacted by it must be integral to the Multiple Disadvantage Partnership Board and all decision-making around the design, commissioning, co-production and evaluation of services to support this population. Research conducted by Luminus further identifies that “genuine co-production would mean a culture shift in service” to ensure people with lived experience are valued as equal partners and peers. [64] It is therefore crucial we see a shift in power so that the local system is transformed into a service user-led system, whereby people with lived and living experience are valued as an equal partners in decision-making and strategic planning.
Systems change could include sustainable lived experience engagement and foster clear development pathways, such as voluntary or professional peer support roles, peer leadership, propagation of skills, training to enable their participation in service evaluation, and progression opportunities in professional development as system leaders. OHID guidance supports the implementation of lived experience initiatives and recovery support services to help people start and sustain recovery.
System partners could be more open to learning from national guidance and best practice around engaging with people experiencing multiple disadvantage. For example, the Surrey Substance Use Partnership could involve people experiencing multiple disadvantage and substance use disorders and foster a culture of genuine co-production. As a long-term aim, Surrey should establish a lived experience workforce, with the goal of employing staff members with lived experience of multiple disadvantage to contribute significantly to changing the organisational culture and improving services.
Finally, it is recommended that continue working to develop a human learning system with people with experience of multiple disadvantage. It is imperative that we address the power balance and adopt a culture of genuine co-production where people with lived and living experience of multiple disadvantage are genuinely involved in the design, commissioning, delivery, evaluation, and governance of all services supporting this population. Placing people with lived and living experience at the heart of decision-making processes ultimately offers individuals choice, control and empowerment over their health and wellbeing and care pathways.
Recommendation 5: Invest in early intervention and prevention solutions to reduce the prevalence, duration, and impact of multiple disadvantage
Many people facing multiple disadvantage will have experienced early life trauma and adverse childhood experiences, as such, early intervention and prevention are crucial long-term solutions to responding to trauma, identifying risk and support earlier, and reducing the incidence and impact of multiple disadvantage. By turning the dial towards ‘prevention’, services will be able to reach more people who are heading into crisis, work with them sooner, and prevent multiple disadvantage from taking root in the first place. A key example is improving early identification of multiple disadvantage risk factors, such as individuals experiencing a mental health need, using drug and alcohol, or affected by co-occurring conditions.
Failure to identify a person affected by co-occurring conditions and/or multiple disadvantage early-on has the potential to result in increased crisis presentations and healthcare costs due to frequent hospitalisations, A&E attendances, and long periods of time ‘bouncing’ between various treatment services. [64] Early identification and prevention have the potential to result in cost avoidance and encourage smoother navigation between various treatment services for the service user. A core priority of the NHS Long Term Plan is to reduce pressure on urgent and emergency care services.
Surrey’s Integrated Care Partnerships and Health and Well-Being Board could continue to use learnings from relational and trauma informed models such as the national ‘Fulfilling Lives’ and ‘Changing Futures’ programmes to inform future creation and commissioning of preventative interventions and solutions. These models can be developed in Surrey to reach the wider population of health inclusion groups (including people facing multiple disadvantage) earlier in their life course to prevent them reaching crisis point and to ensure equitable access to health and social care to reduce the health and social inequalities experienced currently.
Utilising local assets and valuing VCSEs as equal system partners and placing peers within the workforce is an important step towards implementing effective intervention and prevention solutions. Thus, there is a clear need for investment in community-based interventions to support early identification of challenges and addressing them in a timely manner. A clear example is the reduction in pharmacy provision both nationally and locally which has highlighted the existing deficit of prevention and harm reduction provision. These services, such as needle and syringe provision and access to Naloxone, could be enhanced through community-based interventions and local assets. This would also provide people experiencing multiple disadvantage with more flexibility and choice of local alternatives. Further work could be undertaken to identify the level of resource needed to support these individuals within a community setting and prevent them from being found later in other pathways such as the criminal justice system or homelessness.
By identifying and addressing issues at their early stages, preventative solutions and early interventions contribute to improved individual and population wellbeing, reduced social disparities, and more efficient use of resources.
Recommendation 6: Prioritise embedding a cross-cutting Trauma Informed Approach at individual, service, and system levels
Embedding a Trauma Informed Approach (TIA) cannot be done piecemeal, it is a system-wide cultural change that requires the system to work collectively and take small steps towards embodying trauma and psychologically informed principles in a meaningful way.
The goal in Surrey is for all services working with people facing multiple disadvantage to improve understanding of the centrality of trauma and mental health symptoms in multiple disadvantage presentations. Not only does this include specialist multiple disadvantage services, but also all services interacting or supporting people facing multiple disadvantage such as housing and accommodation services, substance use services, mental health services, domestic abuse services, probation services, in addition to the wider workforce including non-clinical staff (e.g., commissioners) and organisations. Not everyone needs to become a specialist, but everyone should have a foundational understanding of the basic models of implementing a Trauma Informed Approach. Surrey can also learn from national examples such as Plymouth, which has recently become a Trauma Informed City.
This requires upskilling staff to improve awareness and recognition of trauma informed practice and ensuring the workforce carry out mandatory training modules. It is recommended that as a minimum this training would include two foundation modules: ‘Understanding Trauma’ and ‘Trauma Informed Approach’. All organisations should allocate time for all staff at all levels of the organisation to carry out training. To support embedding of TIA, this JSNA chapter recommends allocating Trauma Informed Leads or Ambassadors in each service area to help champion trauma informed practice, ensure access and uptake of training, facilitate discussions, and connect TIA across system partners.
Reflective practice through supervisions and team meetings are also important for embedding trauma and psychologically informed approaches as they allow a space for practitioners to reflect on practice. Frontline staff are at risk of experiencing vicarious trauma and the provision of occupational mental health and wellbeing support, including opportunities for reflective practice, is a critical resource. It is important to continue creating an organisational culture that provides psychological safety for both service providers and service users.
Recommendation 7: Ensure that key health and care services are commissioned in a way that promotes partnership and integration through the adoption of commissioning best practices for people experiencing multiple disadvantage
Commissioning models are vital to tackling multiple disadvantage as they determine what type of services are delivered in Surrey and the way they are delivered. There is an enthusiasm from parts of the system to adopt progressive commissioning models, embrace innovation, and commit to sustainable system change. Surrey could start to look more outwardly and work at pace, learning from other areas to progress and embed innovative best practice commissioning in order to see significant and meaningful improvements to the health, wellbeing and mortality of its residents experiencing multiple disadvantage to ensure that ‘no-one is left behind’.
As a priority, current commissioning models for services supporting people experiencing multiple disadvantage could be comprehensively reviewed collectively by the Integrated Care Boards, Surrey’s Health and Wellbeing Board, system leaders and commissioners, VCSE organisation representatives and people with lived experience of multiple disadvantage. This review could evaluate the effectiveness, efficiency, impact, and sustainability of the current commissioned services to ensure they best meet the needs of people experiencing multiple disadvantage individuals. Multiple disadvantage commissioners could also develop a stronger understanding of the suitability and accessibility of specialist and targeted services for different groups at different times, ensuring the availability of a range of treatment options. This includes making space for community-based alternatives to make the system response to multiple disadvantage more accessible and resilient by recognising the diversity, expertise, and value of our VCSEs.
The primary research identifies that large statutory services supporting people experiencing multiple disadvantage often offer a ‘one size fits all’ which does not consistently meet the needs of these individuals. However, primary research supports the view that some of these services often do not effectively meet the needs of these individuals who do not typically fit neatly into service criteria and thresholds. This JSNA chapter identifies challenges with current commissioning in Surrey, including siloed ways of working, dominance of larger service providers, and short-term funding cycles. Many of these challenges are driven by the structures of the system and strategic commissioning. Consideration is therefore needed around how services can best be commissioned and funding allocated to improve quality, access, and experience for service users.
This JSNA recommends an extension of effective joint commissioning which can be supported by conducting a spending review to help to end the fragmented funding of services and better meet demand pressures. For example, moving away from short-term funding cycles and instead, providing long-term funding to a range of services, allowing organisations to adapt their approaches based on the evolving needs of the individuals they serve, providing stability and enabling long-term planning. Effective joint commissioning can also improve transparency around resources and allows for resources to be pooled into areas that benefit the whole system. For example, pooling of budgets and grants from larger service providers to fund collaborative work for this population. It is important to ensure representation for multiple disadvantage on all local Joint Commissioning Boards to support transparency.
As a final point, this JSNA chapter recommends that Surrey starts to take a more courageous approach to adopting progressive models of commissioning. This chapter identifies the need to move away from competitive commissioning and take a system-wide approach that offers transparency of funding streams and availability across all partner agencies. In a climate of austerity and threat of further reductions to public funding, we see a culture where a lack of funding transparency creates core barriers and prevents the delivery of high quality, effective and accessible person-centred services.
Recommendation 8: Redistribute existing funding to provide a range of integrated, accessible, relational, and person-centred services for people facing multiple disadvantage
People in inclusion health groups such as those experiencing multiple disadvantage struggle to access health and social care and often have poor experiences when they do. There are barriers to accessing care for people experiencing multiple disadvantage in all areas of the system including mental health, substance use treatment, housing and accommodation support, as well as intermediate care upon discharge from hospital or secure estates. Together, these produce systemic neglect, resulting in the widening gap between their outcomes and those of the general population.
Primary research identifies pockets of excellence in Surrey, however, many services were identified as operating in silos and are geared up to ‘assess’ and ‘treat’ only one primary need instead of delivering an integrated approach. Siloed working can have a detrimental impact on the delivery of integrated care and often results in a disjointed approach that fails to address the interconnected needs of individuals affected by multiple disadvantage.
Research findings highlight that individuals experiencing multiple disadvantage require access to a diverse, integrated, accessible, and flexible market of service providers that offer a range of treatment services to foster flexibility, choice, and innovation. Surrey should ensure the provision of progressive support models for this population that prioritise the individual, focus on relational support, provide assertive outreach, and are delivered in a trauma informed way. A progressive approach may better understand deep-rooted trauma and the multifaceted nature of multiple disadvantage. The system should recognise that individuals experiencing multiple disadvantage do not always require a web of services placed around them. Often this can in fact cause further complexity due to multiple referrals, multiple assessments, multiple retelling of stories, and multiple barriers relating to service criteria. Progressive support models can ‘pull’ in traditional support and treatment services as and when desired and/or directed by the person at their own pace once their priority needs have been met. There is therefore a place for non-medical models which can work in tandem with larger specialist services. This JSNA chapter identifies successful proof of concept models in Surrey such as Bridge the Gap. Similar national models and pilots demonstrate pockets of excellence which should be sustained as long-term multiple disadvantage initiatives in Surrey to reach a wider cohort.
Services should be accessible to everyone who needs them and offer tailored solutions to address the specific intersectional challenges faced by each individual. Everyone should have access to tools and skills to participate fully in the economy and society, this includes consideration of factors such as equity of experience, the provision of gender-specific services, services for people with a neurodevelopmental condition, support for people facing digital exclusion, language and translation barriers, and cultural differences. Place-based service delivery is also an important consideration due to Surrey’s large geographical area. Services should offer flexibility, improve consistency and transparency of service delivery, and adapt to the specific needs of a place so that people everywhere can expect the same quality of service.
The action on inclusion health framework for NHS recommends using evidence from best practice to commission sufficient specialist services for inclusion health groups, which includes people affected by multiple disadvantage. The framework also indicates that partners including local Integrated Care Systems, local authorities, Primary Care Networks, and VCSEs can work together to develop personalised integrated support for people in inclusion health groups. The quality of all support provision and integrated care should be raised to ensure equitable access, experience, and outcomes for all.
In light of the above recommendations which emphasise the need to continue to work towards integration and collaboration across the system, the following three recommendations (recommendations 9, 10 and 11) are more specific to different parts of service delivery. These recommendations can be considered as complimentary to the previous recommendations around the delivery integrated care and best meeting the needs of people experiencing multiple disadvantage.
The following recommendations also place emphasis on the need for co-production of services and service specifications with a diverse group of individuals with lived and living experiencing multiple disadvantage. This includes both current service users as well as those individuals who have experienced challenges in accessing support.
These recommendations can be read in conjunction with other JSNA chapters, including the Substance Misuse chapter, Emotional and Mental Wellbeing in Surrey Adults chapter, and the Housing and Related Support chapter.
Recommendation 9: Ensure people affected by multiple disadvantage have access to high quality, effective, and person-centred alcohol, drug and recovery services by conducting a comprehensive review of commissioned substance use services in Surrey
This JSNA recommends that a diverse group of people with lived and living experience of multiple disadvantage are involved in the co-production of the specification and the outcomes for future substance use service delivery. In addition, a comprehensive review of substance use services for this population could be conducted to help ensure that people facing multiple and co-occurring challenges are able to access services that are suitable for their needs. While the planned review of these services in 2025/26 could provide a good opportunity for this, a comprehensive review is required as a priority. The review may also help to ensure a system-wide view of funding availability and identify ways to redistribute and restructure relevant funding streams to maximise outcomes for people experiencing multiple disadvantage.
Partnership working is also vital in levelling up outcomes for people experiencing multiple disadvantage and as a system. The Surrey Substance Use Partnership could assist with levelling up outcomes by bringing together strategic partners and collaborating with people with lived experience of multiple disadvantage. We should continue to look to substance use commissioners to strengthen collaboration with partners and providers supporting people affected by multiple disadvantage and a substance use disorder.
As in other areas, substance use services could also consider developing suitable outcome-based measures to sit alongside output-based KPIs associated with drug and alcohol treatment outcomes. This could help to ensure that services supporting people experiencing multiple disadvantage continue to focus on what good outcomes mean to those supported.
In line with the national drug strategy From Harm to Hope, which emphasises the need for improved transparency of local alcohol and drug treatment and partnership approaches to effective commissioning, this JSNA chapter identifies the need for an extension of effective joint commissioning arrangements with a view to better supporting individuals experiencing co-occurring mental health conditions and drug and alcohol use. For example, commissioning and ensuring the availability of a range of treatment options, including pre-treatment, that focus on relational alongside medical models.
The commissioning of substance use services for people experiencing multiple disadvantage could continue to learn from evidence from national and local examples (e.g., the Changing Futures programme) to support progressive models that focus on the development of relational, strength-based and trauma informed approaches within service offers and the wider system. Market stewardship is also an important commissioning function which could support and enable the participation of community based voluntary sector organisations, recognising the diversity and expertise of Surrey voluntary and community partners, which can make the system response to multiple disadvantage more accessible and resilient. Redistribution of funding would be a result of this process.
Recommendation 10: Ensure that people experiencing multiple disadvantage are offered a diverse range of mental health services with improved ease of access, flexibility and better outcomes
Mental health plays a key role in overall wellbeing and quality of life; however, the research found that limited availability, accessibility, and flexibility of mental health support for people experiencing multiple disadvantage in Surrey often intensifies their mental health challenges.
Mental health services could offer an increased range of services for all levels of mental health needs, improved ease of access, and enhanced service flexibility to enable them to better meet the needs of individuals facing multiple disadvantage. There is a need for increased availability of mental health service options with less stringent thresholds for people experiencing multiple disadvantage and mental health needs. For example, there are limited ‘low-level’ support options for people experiencing multiple disadvantage and mental health conditions such as depression and anxiety, eating disorders, and personality disorders, and often people experiencing this type of mental health need do not typically meet thresholds for support. Likewise, drug and alcohol use should not be automatic exclusion criteria for accessing mental health services; in fact, it is pivotal that drug and alcohol and mental health services work together to ensure access to more targeted support. In alignment with the Substance Misuse JSNA Chapter, it is recommended that pathways between mental health and substance use services are continually strengthened to ensure that people are able to access the right care where there is a dual diagnosis or co-occurring condition.
Mental health services should offer flexibility in support type, location, and duration to meet varying mental health needs. Services should make reasonable adjustments to not place an individual at further disadvantage, in particular for individuals with neurodevelopmental conditions. Appropriate reasonable adjustments might include making changes to the way things are organised or done, making changes to the built environment or physical features, taking services to the person, and providing aids such as clear written information or an advocate.
It is also recommended that a review of assessments for mental health services is conducted to ensure they do not cause an oversimplification of multiple and complex challenges, do not only assess and treat one condition, and do not result in exclusion from services. Mental health services should look beyond immediate diagnostic thresholds and recognise deep-rooted trauma in multiple disadvantage presentations and the significant cross-over between risk factors. Furthermore, addiction should be considered more holistically rather than solely a substance use or mental health need.
Recommendation 11: Improve ease of access to housing and accommodation support and ensure sufficient housing options for people experiencing multiple disadvantage
In Surrey, housing and accommodation support is not able to meet to current need and there are gaps in provision for people experiencing multiple disadvantage. Housing should be considered as a priority and primary need for people experiencing multiple disadvantage prior to engaging in treatment services. However, the current lack of housing both nationally and locally means many individuals experiencing multiple disadvantage are homeless or living in inappropriate and unsuitable accommodation. The below recommendations align to those set out in the recent Housing and Related Support JSNA chapter.
This JSNA recommends that a review is conducted of the current housing support offer to ensure sufficient housing options for people experiencing multiple disadvantage. Individuals should be able to choose from a mix of regulated housing options, access ongoing support, and be part of the community. Housing options could include specialist housing, shared housing, independent/single occupancy housing and assured shorthold tenancies.
There is a need for increased availability and accessibility of new and appropriate specialist housing options for people with physical health needs, people with learning disabilities, learning difficulties and/or neurodevelopmental conditions, people with mental health needs, people with drug and alcohol dependencies, domestic abuse, prison leavers, and older people with care and support needs across Surrey. It is also recommended that the provision of ‘wet housing’ and similar accommodation options are available in Surrey. Likewise, individuals using substances or with a mental health need should have access to housing which accepts them regardless of whether they are ready for structured treatment and continue to use substances.
NICE guidance on integrated health and social care for people experiencing homelessness recognises that more effort and targeted approaches are often needed to ensure that health and social care for people experiencing homelessness is available. For example, Housing First units have had a demonstrable positive impact in reducing homelessness for people who have significant substance use and/or mental health needs by providing an opportunity to be supported whilst seeking treatment options. [65] The number of Housing First units should be increased in Surrey to better meet the need.
Early planning for winter provision is also pivotal to supporting people facing multiple disadvantage and homelessness. Commissioners and decision-makers should strongly consider investing in initiatives that support winter provision, create short-term solutions to reduce rough sleeping all year round, and develop pathways to sustained accommodation and access to healthcare.
There is also a need for clarity around housing support pathways for individuals facing multiple disadvantage. This includes identifying pathways to prevent failed housing placement and pathways for individuals placed in emergency accommodation out of county and leaving residential rehabilitation to facilitate their continued access to support and treatment.
Improved harm reduction training should be available to staff in supported housing so that they are competent and confident to support people who are still using substances without it jeopardising the individual’s accommodation offer.
Housing provides a fundamental human need for shelter and protection from the elements and people experiencing multiple disadvantage and homelessness or risk of homelessness should be supported to secure suitable and stable housing prior to entering traditional treatment services.
References
[1] Healthy Surrey. (2022) Surrey Health and Well-Being Strategy – update 2022. Available at: Surrey Health and Well-Being Strategy – update 2022 | Healthy Surrey (Accessed: 17 January 2024).
[2] Bramley, G., Fitzpatrick, S., Edwards, J., Ford, D., Johnsen, S., Sosenko, F., Watkins, D. (2015) ‘Hard Edges: Mapping severe and multiple disadvantage’, Lankelly Chase. Available at: Hard-Edges-Mapping-SMD-2015.pdf (exactdn.com) (Accessed: 11 October 2023).
[3] Gov.uk. (2021) Changing Futures: prospectus. Available at: Changing Futures: prospectus – GOV.UK (www.gov.uk) (Accessed: 16 June 2023).
[4] Healthy Surrey. Changing Futures – Bridge the Gap. Available at: Changing Futures – Bridge the Gap | Healthy Surrey (Accessed: 15 May 2023).
[5] Making Every Adult Matter. Working together to tackle multiple disadvantage. Available at: Home – MEAM (Accessed: 15 May 2023).
[6] Homeless Link. (2022) Unhealthy State of Homelessness 2022: Findings from the Homeless Health Needs Audi. Available at: Unhealthy State of Homelessness 2022: Findings from the Homeless Health Needs Audit | Homeless Link (Accessed 23 January 2024). The findings from 31 Homeless Health Needs Audits, representing 2,776 individuals.
[7] Office for Health Improvement & Disparities (2023). Inclusion Health Groups in Surrey Heartlands ICS: An overview of available data and published evidence. Office for Health Improvement & Disparities (2023). Available internally.
[8] Data from Frimley ICS provided via their Connected Care population health management platform.
[9] National Lottery Community Fund. (2020). Improving access to mental health support for people experiencing multiple disadvantage. Evaluation of Fulfilling Lives: Supporting people with multiple needs. CFE Research and The University of Sheffield, with the Systems Change Action Network. Available at: Full-Report-Improving-access-to-mental-health-support-for-people-experiencing-multiple-disadvantage-2020.pdf (tnlcommunityfund.org.uk) (Accessed 6 September 2023).
[10] Data shared via Surrey County Council’s Adult Social Care team.
[11] Office for Health Improvement & Disparities (2023). Adult Substance misuse treatment statistics 2021-22. Available at: Adult substance misuse treatment statistics 2021 to 2022: report – GOV.UK (www.gov.uk). (Accessed 5 October 2023).
[12] Making Every Adult Matter (2021). Reviewing the deaths of people facing multiple disadvantage. Available at: Revieiwng-the-deaths-of-people-facing-multiple-disadvantage.pdf (meam.org.uk). (Accessed 2 June 2023).
[13] National institute for Health and Care Excellence (2022). Integrated health and social care for people experiencing homelessness. NICE guideline [NG214]. Available at: Context | Integrated health and social care for people experiencing homelessness | Guidance | NICE Accessed (24 July 2023).
[14] Inclusion Health Groups SE datapack quoting Research by Pathway, the Marie Curie Palliative Care Research Department and Institute of Epidemiology & Health Care at UCL Premature frailty, geriatric conditions and multimorbidity among people experiencing homelessness: a cross-sectional observational study in a London hostel – Pathway.
[15] Gov.uk (2021). Identified needs of offenders in custody and the community from the Offender Assessment System, 30 June 2021. Available at: Identified needs of offenders in custody and the community from the Offender Assessment System, 30 June 2021 – GOV.UK (www.gov.uk). (Accessed 20 December 2023).
[16] Gov.uk (2019). Identified needs of offenders in custody and the community from OASys. Available at: Identified needs of offenders in custody and the community from OASys – GOV.UK (www.gov.uk) (Accessed 20 December 2023).
[17] Alcohol and drug treatment in secure settings 2021 to 2022.
[18] Healthy Surrey. ECINS multi-agency information sharing and case management system. Available at: ECINS multi-agency information sharing and case management system | Healthy Surrey (Accessed: 10 January 2024).
[19] UK Parliament POST, Postnote, Number 612 January 2020. Available at: POST-PN-0612.pdf (parliament.uk) Accessed: 24 April 2024.
[20] McQuire, C., Mukherjee, R., Hurt, L., Higgins, A., Greene, G., Farewell, D., Kemp, A., Paranjothy, S. ‘Screening prevalence of fetal alcohol spectrum disorders in a region of the United Kingdom: A population-based birth-cohort study’. Prev Med. 2019. Available at: 10.1016/j.ypmed.2018.10.013. (Accessed 19 March 2024).
[21] Antolini, G., Colizzi, M., Where Do Neurodevelopmental Disorders Go? Casting the Eye Away from Childhood towards Adulthood, (National Library of Medicine, April 2023). Available at: Healthcare | Free Full-Text | Where Do Neurodevelopmental Disorders Go? Casting the Eye Away from Childhood towards Adulthood (mdpi.com)
[22] Stone, B., Dowling, S., Cameron, A., Cognitive impairment and homelessness: A scoping review, (November 2018). Available at: Cognitive impairment and homelessness: A scoping review – PubMed (nih.gov)
[23] Surrey-i (March 2023). Emotional and Mental Wellbeing in Surrey Adults. Available at: Emotional and Mental Wellbeing in Surrey Adults | Surrey-i (surreyi.gov.uk) (Accessed 18 March 2024).
[24] Centers for Disease Control and Prevention. What are adverse childhood experiences? Available at: Fast Facts: Preventing Adverse Childhood Experiences |Violence Prevention|Injury Center|CDC (Accessed 14 December 2023).
[25] NHS Manchester University. Adverse Childhood Experiences (ACEs) and Attachment. Available at: Adverse Childhood Experiences (ACEs) and Attachment – Royal Manchester Children’s Hospital (mft.nhs.uk). (Accessed 8 January 2024).
[26] Hughes, K., Bellis, M., Hardcastle, K., Sethi, D., Butchart, A., Mikton, C., et al. (2017). ‘The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis’ The Lancet Public Health. Available at: The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis – The Lancet Public Health. (Accessed 8 January 2024).
[27] Hughes, K., Ford, K., Kadel, R., Sharp, C., Bellis, M. (2020). ‘Health and financial burden of adverse childhood experiences in England and Wales: a combined primary data study of five surveys’ BMJ Open. Available at: https://bmjopen.bmj.com/content/bmjopen/10/6/e036374.full.pdf . (Accessed 9 January 2024).
[28] Neighbourly Lab (2023). Research commissioned by Surrey County Council. ‘Impact of Cost of Living on Surrey Residents in 5 locations’.
[29] The Care Leavers’ Association. The Needs of Adult Care Leavers. Available at: The Needs of Adult Care Leavers – The Care Leavers Association. (Accessed 21 February 2024).
[30] Muggleton, N., Parpart, P., Newall, P. et al. ‘The association between gambling and financial, social and health outcomes in big financial data’. Nature Human Behaviour (2021). Available at: https://doi.org/10.1038/s41562-020-01045-w. (Accessed 19 January 2024).
[31] UK Parliament (2019). Tackling inequalities faced by Gypsy, Roma and Traveller communities. Available at: Tackling inequalities faced by Gypsy, Roma and Traveller communities – Women and Equalities Committee (parliament.uk).(Accessed 20 March 2024).
[32] British Medical Association, Refugee and asylum seeker patient health toolkit: Unique health challenges for refugees and asylum seekers, (September 2023). Available at: Unique health challenges for refugees and asylum seekers – Refugee and asylum seeker patient health toolkit – BMA
[33] The Guardian (2024). The Guardian view on the voluntary sector and the state: this crucial relationship needs resetting. Available at: The Guardian view on the voluntary sector and the state: this crucial relationship needs resetting | Editorial | The Guardian. (Accessed 15 January 2024).
[34] Social Care Institute for Excellence (SCIE). The participation of adult service users, including older people, in developing social care (June 2007). Available at: The participation of adult service users, including older people, in developing social care – Whole systems approach (scie.org.uk). (Accessed 29 November 2023).
[35] Public Health England (2017). Better care for people with co-occurring mental health and alcohol/ drug use conditions: A guide for commissioners and service providers. Available at: Better care for people with co-occurring mental health, and alcohol and drug use conditions (publishing.service.gov.uk). (Accessed 22 November 2023).
[36] Office for Health Improvement & Disparities. Fingertips, Public Health Data. Available at: Suicide Prevention Profile – OHID (phe.org.uk) (Accessed 4 October 2023).
[37] Gov.uk Guidance (2024). Discharging people at risk of or experiencing homelessness. Available at: Discharging people at risk of or experiencing homelessness – GOV.UK (www.gov.uk)
[38] Gilburt, H. Working with the VCSE as system partners. The King’s Fund (2023). Available at: Working with the VCSE as system partners – from warm words to actions | The King’s Fund (kingsfund.org.uk) (Accessed 4 February 2024).
[39] Surrey-i. JSNA Housing and Related Support (2024). Available at: JSNA Housing and Related Support | Surrey-i (surreyi.gov.uk).
[40] Kelly, F., Westerhoff, C. ‘Does it matter how we refer to individuals with substance-related conditions? A randomized study of two commonly used terms’. International Journal of Drug Policy (2010). Available at: 10.1016/j.drugpo.2009.10.010. (Accessed: 2 December 2023).
[41] Ruth Atkinson, R. (July 2021). Understanding the link between trauma and multiple disadvantage. (Accessed: 13 December 2023).
[42] Public Health England, The effectiveness of trauma informed approaches to prevent adverse outcomes in mental health and wellbeing: a rapid review (2021). Available at: The effectiveness of trauma informed approaches to prevent adverse outcomes in mental health and wellbeing a rapid review (publishing.service.gov.uk) (Accessed: 14 May 2024).
[43] Main, C., Ballengee, L., George, S., Beneciuk, J., Greco, C., Simon, C. Psychologically Informed Practice: The Importance of Communication in Clinical Implementation. Physical Therapy (2023). Available at: https://doi.org/10.1093/ptj/pzad047. (Accessed 29 November 2023).
[44] Homeless Link (2017). An introduction to Psychologically Informed Environments and Trauma Informed Care Briefing for homelessness services. Available at: Microsoft Word – TIC PIE briefing Mach 2017 (lawworks.org.uk). (Accessed 22 November 2023).
[45] University of Bristol (2019). The nature and prevalence of prostitution and sex work in England and Wales today. Centre for Gender and Violence Research. Available at: Prostitution_and_Sex_Work_Report.pdf (publishing.service.gov.uk).
[46] Crisis. ‘How many people are homeless?’. Available at: Homelessness: Causes, Types and Facts | Crisis UK.
[47] Moreton, R., Welford, J., Howe, P. (Update March 2021). Evaluation of Fulfilling Lives: Supporting people experiencing multiple disadvantage, Why we need to invest in multiple disadvantage. The National Lottery Community Fund. Available at: Why-we-need-to-invest-in-multiple-disadvantage-2021.pdf (tnlcommunityfund.org.uk).
[48] NHS England (2023). A national framework for NHS – action on inclusion health. Available at: NHS England » A national framework for NHS – action on inclusion health.
[49] Gov.uk (2023). Guidance: Part 3: how to develop systems of care that support recovery. Available at: Part 3: how to develop systems of care that support recovery – GOV.UK (www.gov.uk).
[50] Healthwatch Surrey, Who Holds The Power?: Understanding: Co-Production at Surrey And Borders Partnership NHS Foundation Trust, (May 2022). Available at: Microsoft Word – Who holds the power Final 17 May 22.docx (luminus-cic.uk)
[51] Department for Levelling Up, Housing & Communities (April 2023). Frontline support models for people experiencing multiple disadvantage A Rapid Evidence Assessment. Available at: Frontline support models for people experiencing multiple disadvantage (publishing.service.gov.uk).
[52] Young, L., Horvath, T. Promising Practice from the Frontline: Exploring gendered approaches to supporting women experiencing homelessness and multiple disadvantage. (2018). Available at: Promising_Practice_from_the_frontline.pdf (amazonaws.com). (Accessed 20 March 2024).
[53] Social Care Institute for Excellence (SCIE). Care Act guidance on Strengths-based approaches. (March 2015). Available at: Strengths-based approaches – Care Act guidance | SCIE.
[54] NHS England (2023). Supported self-management: peer support guide. Available at: NHS England » Supported self-management: peer support guide.
[55] Lillie Wenzel, L., Robertson, R., Wickens, C. What is commissioning and how is it changing?. The King’s Fund (July 2023). Available at: What Is Commissioning And How Is It Changing? | The King’s Fund (kingsfund.org.uk).
[56] Social Care Institute for Excellence (SCIE). Joint-commissioning for integrated care. Available at: Joint-commissioning for integrated care – SCIE.
[57] NHS. Want to improve your engagement with Inclusion Health groups? Available at: What is Inclusion Health? – Friends, Families & Travellers (inclusion-health.org).
[58] National institute for Health and Care Excellence. NICE and Health Inequalities. Available at: NICE and health inequalities | What we do | About | NICE.
[59] National institute for Health and Care Excellence (2016). NICE guideline [NG58] Coexisting severe mental illness and substance misuse: community health and social care services. Available at: Overview | Coexisting severe mental illness and substance misuse: community health and social care services | Guidance | NICE.
[60] Department for Levelling Up, Housing & Communities (January 2024). Discharging people at risk of or experiencing homelessness. Available at: Discharging people at risk of or experiencing homelessness – GOV.UK (www.gov.uk).
[61] O’Connell, D., Brennan, R., Lewis, T., Beyond Pockets of Excellence: Integrated Care Systems for Inclusion Health. The King’s Fund and Groundswell (August 2023). Available at: Pockets-of-Excellence.pdf (groundswell.org.uk).
[62] A Practical Guide for Local Authority Implementation of the Socio-Economic Duty in England. (June 2021). Available at: A Practical Guide for Local Authority Implementation of the Socio-Economic Duty in England (justfair.org.uk).
[63] Making Every Adult Matter, Reviewing the deaths of people facing multiple disadvantage (2021). Available at: Revieiwng-the-deaths-of-people-facing-multiple-disadvantage.pdf (meam.org.uk)
[64] National Institute for Health and Care Research (NIHR), Multiple long-term conditions (multimorbidity) and inequality- addressing the challenge: insights from research, (September 2023). Available at: Multiple conditions and health inequalities: addressing the challenge with research (nihr.ac.uk)
[65] Bretherton, J., Please, N., Housing First in England: An Evaluation of Nine Services. Centre for Housing Policy (February 2015). Available at: University of York’s 2015 evaluation of nine Housing First services
[66] Fulfilling Lives LSL Research and Learning Partnership, Systems change for people experiencing multiple disadvantage: What have we learned about the system and how it can change? (NPS, Groundswell, and CRESR, March 2022). Available at: FLLSL-Research-Partnership-synthesis-report.pdf (groundswell.org.uk)
[67] Local Government Association, Integrated commissioning and provision. Available at: Integrated commissioning and provision | Local Government Association
[68] The Big Issue, Missed, misunderstood and misdiagnosed (November 2023). Available at: The big issue: Missed, misunderstood and misdiagnosed (bacp.co.uk)
[69] Gilber, H., Ross, S., Addressing barriers to working with the VCSE sector in integrated care systems (The Kings Fund, April 2023) Available at: Actions to support partnership: Addressing barriers to working with the VCSE sector in integrated care systems (kingsfund.org.uk)
[70] Mandy, W., Six ideas about how to address the autism mental health crisis. (Autism, February 2022). Available at: Six ideas about how to address the autism mental health crisis – PubMed (nih.gov)
[71] Surrey County Council, Surrey Transport Plan: Surrey Health Local Transport Strategy, (January 2015). Available at: Surrey Transport Plan: Surrey Heath Local Transport Strategy (surreycc.gov.uk)
[72] Understanding neurodiversity and the risk of suicide. Available at: Understanding neurodiversity and the risk of suicide | Papyrus (papyrus-uk.org)
[73] Characteristics of autism. Available at: Autism | NHS inform
[74] Bernes, G., O’Brien, J., Mattson, S., Neurobehavioural Profiles of Individuals with Fetal Alcohol Spectrum Disorders (Encyclopedia on Early Childhood Development, January 2020). Available at: Fetal alcohol spectrum disorders: Neurobehavioral profiles | Encyclopedia on Early Childhood Development (child-encyclopedia.com)
[75] Bradley, S., Economic Hardship and the Emotional Health of Family Caregivers (University of Pittsburgh, 2008). Available at: SBradley_ETD2008.pdf (pitt.edu)
[76] Amnesty International, Refugees, Asylum Seekers and Migrants. Available at: Refugees, Asylum Seekers and Migrants – Amnesty International
[77] Clarke, V., & Braun, V. (2017). Thematic analysis. The Journal of Positive Psychology, 12(3), 297–298. Available at: https://doi.org/10.1080/17439760.2016.1262613
[78] Fulfilling Lives (Lambeth, Southwark, Lewisham), McCarthy, L., Parr, S., Green, S. Reeve, K., Understanding Models of Support for People Facing Multiple Disadvantage: A Literature Review, (Centre for Regional Economic and Social Research, Sheffield Hallam University, September 2020). Available at: FLLSL-Lit-Review_FINAL-September-2020.pdf (groundswell.org.uk)
[79] Ogrodnik, M., Karsan, S., Heisz, JJ. Mental Health in Adults With ADHD: Examining the Relationship With Cardiorespiratory Fitness. (National Library of Medicine, May 2023). Available at: https://doi.org/10.1177%2F10870547231158383
Appendices
Appendix 1: JSNA Chapter Delivery Group
| Role | Responsibility | Colleagues |
|---|---|---|
| Project Supervisor | A subject matter expert whose roles is to oversee, facilitate and support the work including arranging final sign off of the chapter structure/ outline, and the final draft. | Lisa Byrne, Changing Futures Programme Manager |
| Project Manager | Usually a senior Public Health Data Analyst whose role is to arrange initial meetings, liaise between analysts and authors and assist with project management. | Rebecca Matthews, JSNA Programme Manager |
| Lead Author | Usually a Public Health lead or appropriate expert whose role is to help direct section authors and have editorial responsibility for the final chapter. | Ella Turner, Programme Manager – Health Determinants Research Collaborative |
| Lived Experience Project Manager | The governance for the Multiple Disadvantage JSNA Chapter lies with the Lived Experience Recovery Organisation. The LERO’s Project Manager will be responsible for coordinating the group and supporting with the co-production of the chapter. | James Poole, Lived Experience Project Manager |
| Contributing Authors | Appropriate experts who write nominated sections. | • Dr Jo Jennison, Consultant Clinical Psychologist • Dr Raja Mukherjee MBE, Consultant Psychiatrist • Julie Shaw, Senior Partnership & Programme Manager, Surrey Adults Matter • Lisa Byrne, Changing Futures Programme Delivery Manager, Public Health & Communities, SCC.Programme Surrey, SCC. • Rebecca Matthews, JSNA Programme Manager • James Poole, Changing Futures Project Manager, Public Health & Communities, SCC. |
| Data Analysts | A member of the Public Health Intelligence and Insight Team unless other analytical teams are involved. Their role will be to understand and organise the data needs of the chapter. | • Lynne Sawyer, Public Health Analyst • Tyla Bailey, Business Support Officer |
| Sponsor | Leadership – a strategic lead to champion and support the project at strategic level | Vicky Stobbart, ICS Director of Long-Term Planning Delivery |
In addition to sign off from the LERO, the governance for the Multiple Disadvantage JSNA Chapter also lies with the Multi-Agency Group and JSNA Oversight Group.
Appendix 2: Co-production session log
Below shows the sessions that have been carried out with the Lived Experience Recovery Organisation (LERO) when working in partnership to produce this JSNA.
| Where? | When? | What? |
|---|---|---|
| In-person | 31st May 2023 | In this section we started with introductions from the SCC team and experts by experience and general discussion about the JSNA. Short presentation explaining the purpose of a JSNA, co-production, ways to get involved with the chapter, renumeration was delivered, with time at the end for Q&A. Topics of discussion: • Chapter scoping and defining multiple disadvantage. • We shared some definitions of Multiple Disadvantage with the group (SAM, MEAM, Changing Futures) and opened the table for group discussion. Using post-it notes and large sheets of paper, we created a mind map of our collective responses to the following questions: – How do we want to define multiple disadvantage for the JSNA Chapter? – What are the different definitions we can consider? – How can we avoid oversimplification or exclusion of a large proportion of people experiencing multiple disadvantage? |
| Online | 9th June 2023 | Next steps for co-production including what type of co-production activities work well for the group, frequency of meetings, learning styles etc. |
| Online | Planning involvement in the JSNA stakeholder workshop. This is an introductory workshop, some of the experts by experience presented to the group about a topic of their choice. | |
| Online | 15th June 2023 | Initial wider stakeholder JSNA working group Two experts by experience attended the workshop and presented on: • Overview of Lived Experience with Changing Futures • The importance of whole person approach • Meaningful conversations |
| In-person | 5th July 2023 | Focus group discussion |
| Online | 13th July 2023 | Stakeholder workshop 2: chapter scoping |
| Online | 14th July 2023 | Research Skills Training Session and 1hr co-design session 2 of service user voice interview questions |
| In-person | 21st July 2023 | Co-design of methodology tools. Provided an update on progress of the JSNA. (session one discussing methodology and types of questions, audiences etc.) Decision was made to not go forward with a survey for people with lived experience (disrespectful, unsympathetic). |
| Online | 2nd August 2023 | This session focussed on the service provider survey, we went through the individual survey questions to make amendments and add/remove as desired. The LERO were keen for questions to be included on reflective practice and training, this was a new point that had not been raised at previous discussions on the stakeholder survey. We created two questions to help up gather information on this topic. Towards the end of the meeting we spoke about how we would like to disseminate findings. The LERO raised the point of showing findings in a creative way and would like to have the opportunity to create videos. |
| Online | 11th August 2023 | It was originally decided that we would not survey service users however, the group decided a qualitative ‘speed dating’ style survey would be appropriate. We began to talk about possible questions, length of survey and what we would like to gather/aims. We came up with provisional questions which ET went away and set up on Surrey Says, this draft will be shared with the group at the next meeting for final edits and sign off. We spoke about possible ways of surveying service users and decided on going along to groups that already take place such as smart meetings, recovery cafes, peer support networks. We decided that we would speak to relevant contacts to gauge interest in the idea and decided on £10.50 incentives and a ‘thank you letter’. |
| In-person | 30th August 2023 | Provided an update on progress of the JSNA. Shared the final draft of the co-designed survey for service users and beneficiaries. Made some edits to the question wording and order of questions (e.g., starting with asking about type of services used, negative questions first and then end on what’s working well). Final sign off from the group on the survey. Amreet Battu (PH at SCC) shared topline findings from the substance use chapter and opened the table to discussion on findings and an opportunity to share experiences to help shape the chapter. |
| Online | 8th September 2023 | Updates and findings from in-person qualitative interviewing at service provider outreach settings. |
| Online | 22nd September 2023 | Co-designing the coding framework for qualitative analysis (session 1). |
| Online | 3rd October 2023 | Co-designing the coding framework for qualitative analysis (session 2). |
| In-person | 4th October 2023 | Sharing the coding framework with the wider group, discussing emerging themes and report structure. |
| Online | 10th November 2023 | Updates on JSNA writing progress. |
| In-person | 16th November 2023 | Changing Futures Learning Event focusing on data. |
| In-person | 29th November 2023 | Discussing emerging themes and ways to structure the report, identifying key findings and potential recommendations based on the primary research. |
| Teams | December 8th 2023 | Consolidating timelines and next steps with the JSNA first draft and chapter governance. |
| Teams | December 15th 2023 | Structured session around recommendations for the JSNA, emerging findings were presented, and the group shared their ideas on priority actions. |
| In-person | 28th February 2024 | This session was dedicated to general discussion and updates. Topics included: • Peer research and setting up a formal LERO • Initial ideas for dissemination, suggestions included a virtual post-it note board, creating video, music etc. • We spoke about the value of VCSEs, power dynamics, equal relationships, intersectionality and training opportunities. |
| In-person | 5th March 2024 | Full day workshop held at Oakleaf to share the first draft of the JSNA. Discussion topics were lead by the group. |
| In-person | 6th March 2024 | Changing Future Learning Event: Learning through Data Session Objectives: • To get everyone in a similar frame of mind about what data is and why it’s important for multiple disadvantage. • To consider how we collect, share and use data to improve people’s lives. • To reflect on how we use data to learn and change systems. • To case-conference and network on local data challenges |
| Online | 15th March 2024 | Co-writing a preface for the JSNA chapter. |
| In-person | 27th March 2024 | Discussed the JSNA preface and made edits to the opening of the document. The group also discussed recent meetings they have attended (strategic spaces and boards) and their involvement as lived experience experts, some members of the LERO have felt that they have limited voice in some spaces and that some organisations are reluctant to accept Changing Futures and acknowledge the work carried out. The group spoke about recommendations for the JSNA in more detail, with particular interest in recommendations around inclusion and pathways into services. |
| Online | 12th April 2024 | Event planning and ideas for dissemination of the JSNA Chapter. This included discussion about ways to make the JSNA more accessible and digestible, ideas for the video and posters, leaflets, handouts, presentation styles, case studies, and workshop topics. |
| 24th April 2024 | Follow-on feedback from the JSNA recommendations prior to sharing with wider stakeholders. | |
| In-person | 19th June 2024 | Present findings and draft recommendations to the Health and Well-Being Board (HWBB). This included asking the following: • What collaborative actions can we take across the system to carry forward the draft recommendations that are currently being developed through this JSNA chapter and provide comprehensive support for those facing multiple disadvantage? • In what ways can we involve individuals with lived experience of multiple disadvantage in the planning and implementation of our strategies and decision-making to ensure their voices are heard and their needs are met? Minutes from the HWBB will be made available here: Browse meetings – Health and Wellbeing Board – Surrey County Council (surreycc.gov.uk) |
| Online and in-person | May-August 2024 | Dissemination of key findings and recommendations, including extensive engagement with key stakeholders for feedback and comments prior to publication. |
| Online and in-person | Ongoing from May 2023-March 2024 | The LERO (co-)facilitating interviews with stakeholders/service providers. Experts by experience have facilitated almost 30 stakeholder interviews, speaking to a range of organisations and roles from police, VCSEs, GPs, Councillors and ADs. There has been positive feedback from stakeholders on LERO involvement, we have also noticed a growth in confidence in leading interviews and asking new questions, have more of a discussion on points of interest. |
| Online and in-person | Ongoing from May 2023-March 2024 | The LERO informally interviewed as users of services in Surrey. interviewing service users and beneficiaries of bridge the gap via Smart meetings, recovery cafes…members of the LERO were interviewed by ET to gather their experiences of multiple disadvantage, some interviews took the format of journey mapping sessions, others were more general and spoke broadly of service experience in Surrey, some were very personal and addressing specific challenges relevant to their journey. |
Appendix 3: Methodology
Below is a breakdown of the methodological approach used for the JSNA chapter. Our approach consisted of:
- Literature review:
- A literature review of relevant national and local reports, policies, guidance and evaluations on multiple disadvantage and related factors.
- Secondary data analysis:
- Collation and interpretation of relevant quantitative data from service providers and organisations across Surrey.
- Primary research:
- A total of 86 in-depth interviews with key stakeholders either working to support people experiencing multiple disadvantage or working to address one of the multiple disadvantage core risk factors in Surrey.
- A series of seven focus group discussions with 36 frontline staff.
- An in-person qualitative survey with 28 service users with living experience of multiple disadvantage. Surveying was carried out at outreach provider settings such as peer support groups, SMART meetings, and recovery cafes.
- An online survey with 100 Surrey-based organisations whose services are accessed by people experiencing multiple disadvantage.
- A total of five in-depth interviews with members of the LERO.
The design, conduct, analysis, interpretation and dissemination of insights from each of the three research strands (literature review, secondary data analysis and primary research) were co-produced through regular sessions between the JSNA Chapter Delivery Group and the Changing Futures LERO. This included delivering a research skills training session for experts by experience to become peer researchers.
Results across all research strands were triangulated through iterative discussion within the JSNA Chapter Delivery Group and LERO to inform the chapter conclusions and recommendations as follows:
| JSNA Chapter Section | Data Source/Evidence-base |
|---|---|
| Section 2 | Literature review and secondary-data analysis. |
| Section 3 | Literature review and secondary-data analysis. |
| Section 4 | Literature review and secondary-data analysis. |
| Section 5 | Literature review. |
| Section 6 | Primary research and supporting evidence from the literature review. |
| Section 7 | Triangulation of all three research strands to inform chapter conclusions and recommendations. |
Literature review:
A review of relevant documentation was undertaken to frame the context of multiple disadvantage for this JSNA. The review also informed the design of our research questions and methodology tools. References to relevant documentation are made throughout this document, with a full list of references available at the end of this chapter. Key documentation includes:
- Publicly available reports around health inequalities and health inclusion
- Local and national reporting on severe and multiple disadvantage (e.g., Hard Edges Mapping, Making Every Adult Matter reports)
- Evaluations of the national Changing Futures programme
- Evaluations of Bridge the Gap
- Coroner’s records and suicide audits
- Socio-economic duty guidance
- Literature relating to the cost of living crisis in Surrey
Secondary Data Analysis
As there is currently no publicly available dataset that fully describes the population experiencing multiple disadvantage, relevant data were requested from service providers and organisations from across Surrey identified as providing support to this population group. This included those services that specifically support this cohort and those services that are focused on a single challenge but whose clients often include those experiencing multiple disadvantage, including housing and homelessness, mental health, domestic abuse, criminal justice system, substance use and NHS providers. In total, we contacted over 70 different people to request any relevant data.
The request was kept as flexible as possible to maximise the amount of data that we were likely to receive. Service providers were asked to share any data around service users experiencing two or more of the following challenges: substance use, mental health, homelessness or risk of homelessness, domestic abuse, contact with the criminal justice system, learning disabilities and difficulties, neurodivergence, physical disabilities, poverty/deprivation. We also requested that services provided any demographic information available around these service users experiencing multiple disadvantage. The full list of data sources is as follows:
- Data from Adult Social Care – people open to adult social care with multiple disadvantages.
- SECAmb data around Naloxone usage (Chertsey and Guildford areas)
- Cuckooing data from Catalyst
- Catalyst infographic and report
- HM Chief Inspector of Prisons for England and Wales: Annual Report 2022–23
- Summary of relevant national and regional statistics provided by Ministry of Justice analysis team
- Indices of Multiple Deprivation
- ECINS – people in contact with the criminal justice system
- Probation service data
- East Surrey Domestic Abuse outreach monitoring reports
- Surrey County Council Domestic Abuse Needs Assessment
- MARAC data
- NDTMS published data
- Frimley Connected Care system summary data
- District and Borough housing data returns
- Inclusion Health Groups reports for Surrey Heartlands and Frimley ICS
- OHID data – co-occurring mental health and substance use issues
- Oakleaf summary data
- Surrey Coalition of Disabled People Cost of Living Report
- Rentstart summary data
- Surrey Adults Matter summary data
- Surrey Sexual Health service summary data
- Surrey Heartlands hospital activity data
- Ashford and St Peter’s Hospital High Intensity Users service – summary data
- Surrey Suicide Audit
- Drugs Related Deaths Audit
- MEAM report – Surrey
- Surrey County Council Evaluation of High Impact Complex Drinkers Pilot Service
- Surrey County Council Health Inequalities Task Group report
- Map showing Surrey Food Banks
- Changing Futures evaluation dashboard
- Surrey GamCare helpline and treatment data
- GambleAware District and Borough level information for Surrey
Once received, each individual dataset was analysed for information that would be useful in describing this population and outcomes. A summary of findings is presented in the ‘Local Picture’ section.
Primary research
Primary research was led by the JSNA Lead Author with the support of the LERO. Four experts by experience from the LERO conducted interviews, either 1:1 or with the support of the JSNA Lead Author or Lived Experience Project Manager as requested. Some of the primary research activities, predominantly the in-depth interviews and focus group discussions, were also supported by the JSNA Project Manager and 5 members of the SCC Public Health team.
In-depth interviews with key stakeholders:
The team conducted a total of 86 in-depth interviews with a range of key stakeholders either working to support people experiencing multiple disadvantage or working to address one of the multiple disadvantage core risk factors in Surrey, including:
- Surrey County Council (SCC): including roles relating to the Changing Futures programme, Bridge the Gap Alliance, and Surrey Adults Matter services. Other roles across SCC included: System Convenors, Programme Managers, Coroner, Assistant Directors, Heads of Department, and those working to support Equality, Diversity and Inclusion, Adult Social Care, Care Leavers, Needle and Syringe provision, GRT communities, and rough sleepers)
- Local district and borough councils: including Commissioners and Directors
- County Councillors and Local Authority Leads
- Surrey and Borders Partnership (SaBP) and Surrey Heartlands (ICB/ICS): including roles relating to neurodiversity, substance use (i-access), adult mental health, Clinical Psychologists, Medical Officers, Service Managers, Therapies, Service Liaison and Diversion, GPs, GPIMHS, Clinical Leads and long-term planning.
- Voluntary, Community and Faith sector (VCFS): In total, 22 stakeholders from voluntary and community organisations across Surrey took part in an in-depth interview. VCFS stakeholders had varying remits to support people experiencing multiple disadvantage. Some VCFS organisations focused on supporting specific cohorts e.g., children and young people, others focused on supporting one specific challenge e.g., domestic abuse, housing and supported accommodation, night shelters, food banks. Through the interviews the team spoke to people in a range of roles from CEOs to Service Mangers, to a faith leader, community leads and frontline staff).
- Prison and Probation Services: including Probation Officers and Domestic Abuse Officers
- Surrey Police: including County Lines, policies and commissioning, mental health and suicide prevention
- Surrey Fire and Rescue Service (SFRS)
- Community Pharmacies
- Office for Health Improvement and Disparities (OHID)
- National Health Service England (NHSE)
- Children, young people, and families support providers: including professionals supporting Early Help, Family Centres, PSHE, Wellbeing, Healthy Schools, Team around the School, Targeted Youth Support, commissioning for adolescence and youth offending, youth homelessness, Children, Family and Lifelong Learning (CFLL), Early Years, SEND, education and the virtual school. Primary research relating to children, young and families will be analysed and presented in the Multiple Disadvantage JSNA Chapter: Phase 2. Phase 2 will focus of children, young and families experiencing multiple disadvantage in Surrey.
These interviews explored the following key areas:
- Understanding of multiple disadvantage
- Gaps and unmet needs in current service provision
- Barriers and challenges experienced by people accessing support
- What’s working well?
- Trauma informed approaches
- Training and reflective practice
- Suggestion on improvements
- Factors preventing or hampering change
To view the full co-designed interview guide for stakeholders, please see Appendix 4. Due to the wide range of stakeholders taking part in an interview, a generic guide was co-designed with experts by experience. For some interviews, the guide was adapted to suit the individual participant (where required).
Focus group discussions with frontline staff:
The team conducted a total of seven focus group discussions with a total of 36 stakeholders across Surrey, including representatives from various roles including:
- Practitioners
- Bridge the Gap Alliance providers
- Local Area and Coordinators
- Community Link Officers
These focus groups gained insight into client journeys and experiences, and allowed time and space for detailed discussion around the following key areas:
- Typical service users
- Service design
- Barriers and challenges (from both a service user and provider perspective)
- Positive outcomes
- What could be done differently?
- Systems change and service-level change
To view the full co-designed focus group discussion guide for frontline staff, please see Appendix 4.
In-person qualitative surveying with service users:
The team conducted qualitative surveying with 28 adults experiencing multiple disadvantage in Surrey who were accessing support services in Surrey at the time of the survey. The team attended the following settings to engage with survey participants:
- SMART meeting
- Recovery cafe
- Peer Support groups
- Bridge the Gap provider settings
This survey consisted of the following questions that were co-designed with experts by experience:
- What organisations or support services in Surrey have you accessed for support?
- What has been unhelpful for you in services?
- Is there anything you feel could have been done differently to make support more helpful for you?
- What has been helpful for you in services?
- Is there any phrasing/wording you think it is best to use when talking about people experiencing more than one challenge at any one time?
- Is there anything else that you would like to share?
- Demographic information (multiple disadvantage challenges experienced, age, sex, gender, ethnicity, sexual orientation)
To view the full co-designed qualitative survey for service users, please see Appendix 4. All survey questions were non-mandatory. Probes were provided for each questions to aid researchers when surveying participants.
Online survey:
An online survey was conducted with stakeholders to gain broader insight into the perspective of professionals whose service is accessed by people experiencing multiple disadvantage in Surrey. The survey was open to all Surrey-based organisations whose services are accessed by people experiencing multiple disadvantage, including providers and commissioners.
Survey was hosted on Surrey Says, Surrey County Council’s online consultation portal used to design surveys and consultations and was live throughout August 2023 to October 2023. The survey was shared with stakeholders via internal newsletters and e-briefs, targeted emails, group meetings with relevant stakeholder teams, and word-of-mouth.
The survey gathered insight around service provider perspectives of multiple disadvantage through questions focusing on the type of support their organisation provides, the extent to which current service provision meets the needs of people experiencing multiple disadvantage, feedback on person-centred care, equality diversity and inclusion, and trauma informed care, questions around training, barriers faced by service users, and factors preventing or hampering organisational change to better meet the needs of people experiencing multiple disadvantage.
The survey received a total of 100 responses from a range of stakeholders from the following sectors:
- Voluntary and community organisations (both organisations with a specific remit to support multiple disadvantages as well as wider support e.g., community centres). There were a variety of roles including CEOs, Service Managers, Social Workers, Outreach Workers)
- Surrey County Council
- District and Borough Councils
- Family Centres
- Faith groups
- Clinical and healthcare professionals
- Food banks
- Citizens Advice
To view the full co-designed survey questions, please see Appendix 4.
In-depth interviews with members of the LERO:
The team conducted a total of five in-depth interviews with members of the LERO.
These interviews covered the following points of discussion:
- Defining multiple disadvantage and language
- Current support provision
- Personal experiences
- Qualities of a good and bad service
- Barriers and challenges
- What could be done differently?
Analysis and reporting
For the online survey for stakeholders and qualitative survey for service users and beneficiaries, data were collected via Surrey Says and analysed using Excel. Qualitative data collected via in-depth interviews, and focus groups was coded by question using Dedoose and then thematically analysed using Word.
The team conducted a thematic analysis of the primary research conducted for the purpose of this JSNA. This included transcripts from in-depth interviews, focus groups, in-person surveys and free-text responses from the online survey. These preliminary insights were then triangulated with findings from the literature review and secondary data analysis in order to develop emerging themes. There themes were further refined through discussion with the JSNA Chapter Delivery Group and the LERO. Quantitative data collected in the online survey were also descriptively analysed, with findings presented either as percentages, averages, and/or through visualisations such as graphs and charts.
A two-phase sequential exploratory approach was taken to triangulate the findings from primary research, secondary data-analysis and literature review which then informed the final conclusions and recommendations. This approach placed a larger focus on qualitative data (including qualitative data collected through primary research and the literature review), followed by quantitative data (gathered predominantly through secondary data-analysis).
From the analysis, the team were able to gather insights on experiences of multiple disadvantage as evidenced by people currently experiencing multiple disadvantage as well as professionals providing support to this cohort. The analysis also enabled us to identify varying experiences of multiple disadvantage, unmet needs, barriers to accessing support, suggestions on improvements, and strategic and system level obstacles.
Any direct quotes used through this chapter are presented anonymously using the following codes followed by their unique number:
| Code | Descriptor | Explanation |
|---|---|---|
| IP | Interview participant | Service providers or individuals at organisations working to support people experiencing multiple disadvantage or one of the multiple disadvantage core risk factors in Surrey. |
| FG | Focus group participant | Frontline providers or outreach workers working to support people experiencing multiple disadvantage or one of the multiple disadvantage core risk factors in Surrey. |
| QS | Qualitative survey participant | Individuals with lived and/or living experience of multiple disadvantage, which includes both service users and people who are not currently engaged with statutory services. |
| OS | Online survey participant | Service providers or individuals at organisations working to support people experiencing multiple disadvantage or one of the multiple disadvantage core risk factors in Surrey. |
| LERO | Member of the Lived Experience Recovery Organisation | Expert by Experience that is a member of the LERO |
Where the broader term ‘research participant’ is used, this refers to any individual that took part in any primary research activities carried out for the purpose of this JSNA chapter, this includes in-depth interviews, focus groups, in-person surveys and online surveys. The term ‘research participant’ includes service providers, frontline staff, outreach staff, practitioners, health and care partners, system leaders, stakeholders working to support people experiencing multiple disadvantage or one of the multiple disadvantage core risk factors in Surrey. ‘Research participant’ also includes individuals with lived and/or living experience of multiple disadvantage, which includes both service users, and people who are not engaged with statutory services.
Limitations and challenges
A number of limitations and challenges were identified relating to the individual datasets received and also around data collection. The following limitations and challenges should be considered:
- In general, data available were viewed through one particular lens, e.g. people experiencing homelessness, and any information available around people experiencing multiple disadvantage was an add on to that main view of the data. Data were not available specifically on multiple disadvantage. It was challenging to find data which described multiple disadvantage rather than just a single disadvantage.
- It was difficult to tell a meaningful story from multiple disparate datasets, not all datasets covered the whole of Surrey. Much of the data and research was only available at higher level geographies e.g. local authorities, ICBs, Surrey as a whole or national.
- Surrey Changing Futures data is derived from a small sample size.
- Data quality issues for some datasets meant that we were unable to use them.
- Some national data (e.g. Fingertips) is not updated frequently and can be a number of years old.
- Where services were not specifically supporting people experiencing multiple disadvantage but often or sometimes included this cohort amongst their clients, demographic information was only available for their service users as a whole rather than just those experiencing multiple disadvantage.
- There was a general issue with defining multiple disadvantage and how wide to make the issue – e.g. data from the Alcohol Liaison Nurse (ALN) identifies that many people seen by their service have physical conditions, but these are as a result of alcohol use rather than a wider issue.
- Impact of Covid means that data before then can be less relevant.
- There was a challenge in identifying the right people and organisations to provide us with the data, and challenges in some organisations willingness to share data. External partners sometimes had limited capacity to collate and send data. The secondary data analysis may therefore not reflect a full picture of the broader population experiencing multiple disadvantage in Surrey.
- Some organisations, in particular the smaller service providers, operated with manual data collection systems, giving little flexibility as to what data could be extracted. For some services no robust data collection exists as data is only collated as and when it is needed
- Information governance considerations made sharing of data more difficult, and some restricted data or internal datasets were not able to be shared publicly in this report.
Safeguarding and research ethics
To ensure the safety of all participants and ethical best-practice, safeguarding policy and procedures and SCC’s Business Intelligence and Analysis Research Service – Privacy Notice were followed in the data collection and report structures of the evaluation. The LERO have a suite of documentation that was adhered to when co-producing this JSNA chapter. Documents include Safety, Safeguarding & Confidentiality Guide for individuals with lived experience and others, an Information & Consent pack, a co-production information pack (including support and safety, confidentiality and safeguarding), and a Renumeration and Invoicing policy.
All names and identifiable information have been removed from data presented in this report.
Appendix 4: Methodology tools
Below are the questions and discussions points used in interviews, focus groups and surveys with stakeholders, frontline staff, and service users. All methodology tools were co-designed with the Lived Experience Co-production group. Please note that interview and focus group questions were used as a guide and were adapted to suit the participant(s), with additional probing taking place where appropriate.
Appendix 4.1: Interview questions for stakeholders
- Would you like to start by introducing yourself, and telling me a bit about your role and organisation?
- What is your understanding of multiple disadvantage?
- Do you think other service providers in Surrey have a good understanding of multiple disadvantage?
- Are there any specific gaps in current service provision?
- What barriers and challenges are experienced by people accessing support?
- Reflecting on positives, can you give me an example of what you think is working well?
- Do you think organisations across Surrey implement trauma informed approaches and person-centred care?
- Are you aware of how often supervisions and reflective practice take place in your organisation?
- From your perspective, is there anything that could be done differently to improve the care and support offered?
- What are your suggestions of how to best influence strategic commissioning decisions to tackle blockages / services not up to date with the times?
- Are there any factors that you think have the potential to prevent or hamper change?
- Is there anything else that you would like to share with me that we have not covered in this interview today?
Appendix 4.2: Focus group discussion guide for frontline staff
- Would you like to start by introducing yourself, and maybe tell me a bit about your role and organisation?
- Thinking about the service users your organisation support; how would your organisation typically identify a person experiencing multiple disadvantage?
- To what extent would you say organisations across Surrey have a good understanding of what it means to be a person experiencing multiple disadvantage?
- Reflecting on support services available to people experiencing multiple disadvantage in Surrey, to what extent do you think they meet the current need?
- Have any service users you have worked with or know of from other support services in Surrey experienced barriers or challenges in accessing support?
- Reflecting on potential challenges, what would you say are the key challenges and barriers your organisation has faced in providing support?
- Reflecting on positives, can you share any examples of what you think is working well in support provision for this cohort, either specifically in your organisation or more widely across Surrey?
- From your perspective, is there any that could be done differently to improve the care and support offer to people experiencing multiple disadvantage in Surrey?
- Thinking about system change and service-level change in Surrey, are there any factors that you think have the potential to prevent or hamper change?
Appendix 4.3: Qualitative survey for service users and interviews with LERO members
- What organisations or support services in Surrey have you accessed for support?Prompts: this question is useful to provide an idea of the types of services you have accessed (e.g., statutory/voluntary, group support, 1:1, peer support networks etc.). Please do not feel like to you must share a full list of all services you have accessed if you do not wish.
- What has been unhelpful for you in services? Prompts: long waiting lists/times, eligibility criteria or thresholds, stigma, accessibility
- Is there anything you feel could have been done differently to make support more helpful for you?
- What has been helpful for you in services?
- Is there any phrasing/wording you think it is best to use when talking about people experiencing more than one challenge at any one time? Prompts: how do you feel about the term ‘multiple disadvantage’? Is there any alternative phase you would prefer such as ‘complex needs’, ‘multiple needs’, ‘multiple challenges’? Do you prefer to be referred to as a ‘service user’, ‘client’ or ‘individual’?
- Demographics and protected characteristics questions including multiple disadvantage challenges that have been experienced, age, sex, gender, ethnicity, and sexual orientation.
Appendix 4.4: Online survey with stakeholders
Please use the link below to access a copy of the online survey for stakeholders.