JSNA Loneliness and Social Isolation
Loneliness and Social Isolation Joint Strategic Needs Assessment
Publication date
This chapter was published in September 2024.
Contents
- Executive summary
- Recommendations
- Introduction
- Research methodology
- What do we know about loneliness and social isolation?
- Local insights on priority populations:
- Local insights on other high-risk populations:
- National best practice
- Local best practice
- What is this telling us?
- Lead Contributors
- Acknowledgements
- Appendices
- References
Executive summary
This chapter of the Joint Strategic Needs Assessment outlines what we know about loneliness and social isolation as wider determinants of health and wellbeing for Surrey residents of all ages. It provides a theoretical framework for understanding the complexities of loneliness and social isolation, recognising that both can be experienced by anyone at any time across the life course.
The chapter raises the profile of social connection as a key indicator of health and wellbeing for individuals and for communities. It considers the impact of Covid-19 and the cost of living on the prevalence of loneliness and social isolation for Surrey residents.
It draws on the Health and Wellbeing Strategy, stakeholder engagement, and lived experience to highlight priority populations who are most at risk of chronic (as opposed to transient) loneliness. Chronic loneliness is associated with poor physical health and emotional wellbeing outcomes and low economic activity.
The chapter outlines the key structural enablers of social connection, including Surrey’s support services for vulnerable groups and the essential contribution of voluntary and community organisations to creating and maintaining connected and thriving communities. However, it also shines a spotlight on populations who are marginalised and excluded from the social, cultural, and economic life of our communities.
This is a summary of the chapter’s main findings:
- Loneliness and social isolation arise from social, economic, and structural inequalities that put some individuals at higher risk than others. The poor health and wellbeing outcomes associated with few social connections and poor-quality personal relationships disproportionately affects people who already experience disadvantage.
- The intersectionality of loneliness and social isolation with other wider determinants of health and wellbeing calls for a whole systems approach to tackling its causes and consequences.
- Within a whole systems approach to loneliness and social isolation, social connection should be a cross-cutting theme – akin to equalities, diversity, and inclusion – that informs strategies, policy making, and commissioning across integrated care systems.
Based on these and further findings that can be read in the ‘What is this telling us?’ section, this chapter makes 10 key recommendations:
Recommendations
- System partners recognise chronic loneliness as a structural inequality that should be prioritised as part of Surrey’s broader ambitions to address health and social inequalities. This chapter recommends that a shared plan is agreed at system level at Surrey Health and Well-being Board/ Surrey Heartlands Integrated Care Partnership (HWB-ICP) and at Integrated Care Strategy (ICS) Place so that a coordinated, whole-systems approach can be implemented to address the issue across populations and place and monitor outcomes. Social connection should be prominent in Surrey’s emerging Prevention Strategy Framework.
- Any shared plan at system level adopts a life course approach to tackling loneliness and social isolation, recognising that anyone can experience loneliness and social isolation at any time. A life course approach should also acknowledge that experiences of and resilience to loneliness and social isolation will be mediated by protected characteristics including (but not limited to) health, disability, sexuality, gender, and race as well as by relative social and economic disadvantage.
- The complex intersectionality of loneliness, social isolation, mental ill-health, physical ill-health, disability, and unemployment is recognised and addressed at system and place level to prevent the escalation of poor health and wellbeing outcomes from economic inactivity.
- Surrey would benefit from improving the quality and quantity of its data on loneliness and social isolation so that there is deeper understanding at system, place, and neighbourhood levels of who is lonely or isolated, when and why people experience loneliness, and which initiatives show best outcomes and value for money. For example, Surrey should consider monitoring the Loneliness Index (GP Prescriptions for Loneliness) to track rates of loneliness at ward level and consider its inclusion as an indicator within the Health and Wellbeing Strategy Index. Further qualitative data is required for some population groups including men, LGBTQ+, recent ex-service personnel, farmers, and those who experience legal barriers to civic participation (refugees, asylum seekers, and all sanctuary-seeking peoples).
- Social connection should be recognised by system partners and at Place as a cross-cutting theme akin to equality, diversity, and inclusion. Funding decisions, changes to statutory services, and plans for community initiatives should be assessed for their impact on enabling or prohibiting social connection, particularly for vulnerable groups.
- The structural enablers of social connection – environment, transport, inclusive communities, digital skills – should be recognised and championed at system, place, and neighbourhood levels through strategies, policies, funding decisions and place-making approaches.
- The loneliness and social isolation experienced by children and young people – especially those with additional needs or disabilities, emotionally-based school non-attenders, and those on waiting lists for mental health and neuro-diversity assessments (and their families) – must be addressed through the delivery of the Children & Young People’s Emotional Well-being and Mental Health Strategy to protect the physical health, emotional wellbeing, and socio-economic productivity of a generation.
- The services, groups and activities delivered to communities by the VCSE sector is acknowledged as integral to a whole-system approach to tackling loneliness and social isolation. The VCSE should be supported to become inclusive so that all populations – including the most vulnerable – share in its social connectivity. Impacts on social connection should be considered as part of any decision-making process about cuts to VCSE funding.
- Services that connect people to their communities should ensure that they provide meaningful signposting, giving people appropriate time and support to build confidence to access community provision. Sign-posting services should take an asset-based approach that focuses on strengths and the contribution people can make to their communities. Sign-posting services must recognise that cultural or existential loneliness may require a different approach from emotional or social loneliness.
- Surrey must make a commitment at system level to reducing the stigma associated with loneliness and social isolation, particularly regarding protected characteristics and vulnerable groups, where stigma may prevent someone from seeking help and support. Surrey health and care professionals should be supported to develop the necessary skills and knowledge to have conversations about loneliness and social isolation as part of their everyday practice.
Introduction
The Health and Social Care Act (2012) states that there is a requirement for all Health & Wellbeing Boards working through local authorities and integrated care boards (ICBs) to produce a Joint Strategic Needs Assessment (JSNA) of the health and wellbeing of their local community.
Priority 2 of the Health and Wellbeing Strategy is focused on ‘supporting people’s mental health and emotional wellbeing by preventing mental ill-health and promoting emotional wellbeing’. As well as ensuring people with mental health needs have access to early, appropriate support to prevent escalation of need, this priority is also about ‘creating communities and social environments that tackle isolation and build good mental health’.[1]
Priority 2 has four outcomes:
- Adults, children, and young people at risk of and with depression, anxiety and other mental health issues access the right early help and resources.
- The emotional well-being of parents and caregivers, babies and children is supported.
- Isolation is prevented and those that feel isolated are supported.
- Environments and communities in which people live, work, and learn build good mental health.
This all-age JSNA chapter on loneliness and social isolation supports the delivery of the third outcome by providing insights into who may be isolated in Surrey, why they may be isolated, and what can be done to address isolation for adults, children, and young people.
The Local Government Association urges health and wellbeing boards to be mindful of the serious nature of loneliness, and its impact on wider health and wellbeing. As a public health concern, ‘it is correlated with socio-economic deprivation, housing status, and societal factors’.[2] Whilst loneliness is highly amenable to interventions at a population level as well as individual level, to be successful approaches to tackling loneliness and social isolation must consider ‘how and why an individual has become lonely in determining how best to address their loneliness’.[3]
Defining loneliness and social isolation
Loneliness is defined as ‘a subjective, unwelcome feeling of lack or loss of companionship’.[4] It is an emotional experience: a perceived deficiency in the amount and/or quality of someone’s existing relationships. Loneliness can affect anyone. Everyone’s experience of loneliness will be different but the impact of loneliness on health and wellbeing can be wide-ranging and profound. It may be ‘one of the largest public health challenges we face’.[5]
The Campaign to End Loneliness defines 3 types of loneliness:[6]
- Emotional loneliness – ‘the absence of meaningful relationships’.
- Social loneliness – a ‘perceived deficit in the quality of social connections’.
- Existential loneliness – a ‘feeling of fundamental separateness from others and the wider world’.
Loneliness may be a feeling that is experienced due to an event (such as bereavement) or a life transition (such as retirement or becoming a new parent), in which case feelings of loneliness may be temporary. For some people, however, loneliness can become a chronic condition with profound implications for their mental and physical health.
The Campaign to End Loneliness distinguishes between ‘transient’ and ‘chronic’ loneliness:
- Transient loneliness – a feeling that comes and goes.
- Situational loneliness – only occurring at certain times like Sundays, bank holidays or Christmas.
- Chronic loneliness – feeling lonely all or most of the time.
Social isolation is different from loneliness. Loneliness is an emotional experience, but social isolation is a lack of social contact and a deficit of meaningful relationships. ‘Social isolation is not a subjective feeling but the objective state of having few social relationships or infrequent social contact with others’.[7]
Not everyone who is socially isolated feels lonely. Some people value time spent alone or choose to limit their interactions with others. This JSNA chapter on loneliness and social isolation will focus on those for whom social isolation is not a choice and for whom the experience of loneliness has a negative impact on their health and wellbeing.
Figure 1: Loneliness and social isolation (Source: Campaign to End Loneliness).

Loneliness and social isolation correlate with wider determinants of health and wellbeing. Experiences of loneliness and social isolation – and their impact on health and wellbeing – are mediated by other experiences of inequality.
These inequalities may be shaped by geography (where someone lives), by population characteristics (how someone identifies), and by life experiences. Someone’s experiences of loneliness and social isolation will be influenced by the intersection of these inequalities of place and experience. This is illustrated in the diagram below.
Figure 2: Experiences of loneliness and social isolation are shaped by the intersection of inequalities of place and experience with wider social determinants.
Theoretical frameworks
Three theoretical frameworks are helpful for understanding the intersection between loneliness, social isolation, and wider determinants:
- The ‘critical exposure’ model.
- The ‘cumulative deficit’ model.
- The ‘social justice’ model.
The ‘critical exposure’ model asserts that exposure to risk factors for loneliness have a differential effect on outcomes if experienced at some life stages rather than others. For example, being widowed, a key loneliness risk factor, may be more impactful if experienced in early adulthood than later life. [8]
The ‘cumulative deficit’ model hypothesises that an individual’s outcomes are related to their cumulative exposure to disadvantage, and that those exposures influence short term and longer-term health outcomes. In other words, past and present experiences of loneliness are linked to other social, environmental, biological, and health factors. [9] It may, therefore, be more helpful to articulate loneliness in terms of ‘vulnerabilities’ as opposed to ‘risk factors’. [10] Rather than focusing on individuals, a vulnerabilities framework emphasises the broader context within which people live. One benefit of taking a vulnerabilities approach to loneliness is a focus on the resources available to prepare for, cope with, and recover from life events at individual, community, and societal levels. [11]
The ‘social justice’ model of loneliness takes the cumulative deficit approach to its logical conclusion by asserting that loneliness is heavily determined by social and structural conditions that render it unequally distributed in society. As such, loneliness qualifies as a social justice issue. [12] Rather than approach the issue of loneliness in terms of individual risk factors or deficits that lead to poor social engagement, the social justice model challenges policymakers to rethink loneliness, and interventions to address it, in terms of societal factors. Re-framing loneliness as a social justice issue has important implications for local authority and health planning in this area and calls for whole-system approaches to loneliness and its health and wellbeing impacts.
Social connection
Being curious about what might enable a Surrey resident to form satisfying social connections, at any age or stage in their life course, could change their life. It is never too late.
Social connection makes people happier and healthier across their lifespan. Social connections with family, friends, at school, at work, and in the community foster a sense of belonging that is fundamental to health and wellbeing. Babies begin to form social connections with parents and carers from birth.[13] Forming secure attachments with trusted adults – and knowing that through these attachments one’s needs will be met – is fundamental to healthy human development.
Trusted relationships are essential to secure attachment – without a secure attachment style, the world can feel more dangerous, unstable, and untrustworthy. The attachment styles we learn as children impact on our decisions about whether we feel able to ask people to help meet our needs, or even recognise in others and ourselves when we have needs, all of which has implications for mental health, emotional wellbeing, and personal resilience to experiences of being alone and loneliness throughout the life course. Adverse childhood experiences (ACEs) and other traumatic life events also significantly contribute to subsequent mistrust and fear of social connection.
In order to address loneliness and social isolation it is important to understand social connection and what good social connection looks like for individuals, for communities and for society. Several key questions arise:
- How can the places in which people learn, are cared for, live and work facilitate connection?
- How do the protected characteristics of individuals shape their experiences of social connection and what they need to live in connected communities?[14]
- What barriers are there to social connection for individuals and for communities?
- Is all loneliness relieved by social connectedness or are other interventions required?
Evidence suggests, for example, that in contrast to social loneliness, emotional and existential loneliness may not be relieved by interventions focused on social connectedness and integration into a social community.[15] We need to consider other options that acknowledge psychological pain and patterns of mistrust from childhood and give space to heal unprocessed traumatic experiences.
Social ‘support’ and social ‘connection’ are not one of the same things. Social support tends to be ‘done to’ people whereas social connection arises from reciprocity and relationships of mutual trust and support. People with insecure attachments or a history of ACEs and other traumatic life events will find social connection much harder to allow, trust and enjoy. In other words, the provision of social activity does not, in and of itself, address loneliness and social isolation if the social, psychological, emotional, and structural barriers to these activities for some populations are not also addressed.
Research Methodology
Stakeholder engagement
The findings presented in this chapter are based on evidence reviews provided by Surrey and Sussex Library and Knowledge Services, a review of relevant national and local policies and strategies, national data sets, quantitative Surrey data, local stakeholder engagement, community consultations, and focus groups with selected high-risk populations.
A survey of professionals working across Surrey was conducted to understand which local populations are most at risk of loneliness and social isolation and what the key drivers are for loneliness and social isolation within these populations. The survey ran from the 9th of January to the 23rd of February 2024. There were 105 completed responses. 31.4% of respondents worked in Adult Social Care, 16.2% worked in other roles within local authorities, 12.4% worked in health, mental health, or primary care, 16.2% worked within the VCSE sector, and 23.8% described themselves as working in ‘other’ sectors.
Table 1: Representatives from sectors completing the LSI survey (Source: Surrey Loneliness & Social Isolation Survey, January 2024).
| Sector | Number (n) | Percent (%) |
|---|---|---|
| Adult Social Care | 33 | 31.4 |
| Local Authority | 17 | 16.2 |
| VCSE | 17 | 16.2 |
| Health/mental health/primary care/community | 13 | 12.4 |
| Other | 25 | 23.8 |
The survey asked respondents to state if their role was a service user- or patient-facing role. 81% of respondents worked in service user- or patient-facing roles, and 19% did not.
Table 2: Survey respondents in service user- or patient-facing roles (Source: Surrey Loneliness & Social Isolation Survey, January 2024).
| Option | Total (n) | Percent (%) |
|---|---|---|
| Yes | 85 | 81% |
| No | 20 | 19% |
| Not answered | 0 | 0% |
Stakeholders were asked to select which population group or groups best described the population or populations they work with. 50.5% selected people with long term health conditions, disabilities, or sensory impairment:
Table 3: Population groups survey respondents work with in their professional roles (Source: Surrey Loneliness & Social Isolation Survey, January 2024).
| Option | Total (n) | Percent (%) |
|---|---|---|
| People with long term health conditions, disabilities or sensory impairment | 53 | 50.5% |
| Carers and young carers | 38 | 36.2% |
| Adults with learning disabilities and/or autism | 37 | 35.2% |
| Older people 80+ and those in care homes | 37 | 35.2% |
| People with serious mental illness | 36 | 34.3% |
| People experiencing domestic abuse | 28 | 26.7% |
| People with drug and alcohol problems | 25 | 23.8% |
| Black and Minority Ethnic groups | 22 | 21.0% |
| People experiencing homelessness | 22 | 21.0% |
| Other | 20 | 19.1% |
| Not Answered | 20 | 19.1% |
| Young people out of work | 17 | 16.2% |
| Children with Special Educational Needs and Disabilities (SEND) | 12 | 11.4% |
| Gypsy Roma Traveller community | 11 | 10.5% |
| Children in care and care leavers | 8 | 7.6% |
The survey also asked respondents the age of the populations they work with. Almost 65% of the professionals who responded work with working age adults, over half work with those of retirement age, and just over a third work with children and young people.
Table 4: Age range of the populations survey respondents work with (Source: Surrey Loneliness & Social Isolation Survey, January 2024).
| Option | Total (n) | Percent (%) |
|---|---|---|
| Working Age Adults | 68 | 64.8% |
| Retirement Age (65-80) | 62 | 59.1% |
| Older People (85+) | 50 | 47.6% |
| Children and Young People (up to 25) | 38 | 36.2% |
| Not Answered | 20 | 19.1% |
The survey asked stakeholders to rank the priority populations in Surrey’s Health and Wellbeing Strategy according to their risk of loneliness and social isolation. For the population most at risk of loneliness and social isolation, 27.6% of respondents identified older people 80+ and those in care homes, 23.8% selected people with long term health conditions, disabilities, or sensory impairments, 17.1% selected carers and young carers, 17.1% selected people with serious mental illness, and 4.8% of respondents ranked adults with learning disabilities and/or autism as most at risk.
Table 5: Surrey priority populations ranked most at risk of loneliness and social isolation (Source: Surrey Loneliness & Social Isolation Survey, January 2024).
| Population of loneliness and social isolation | Number (n) |
Percent (%) |
|---|---|---|
| Older people 80+ and those in care homes | 29 | 27.6% |
| People with long term health conditions, disabilities, or sensory impairment | 25 | 23.8% |
| Carers and young carers | 18 | 17.1% |
| People with serious mental illness | 18 | 17.1% |
| Adults with learning disabilities and/or autism | 5 | 4.8% |
For the population ranked second most at risk of loneliness and social isolation, 25% of respondents selected people with long term health conditions, disabilities, or sensory impairments, 12.8% identified people experiencing homelessness, 12.8% selected people with serious mental illness, 12.2% selected older people 80+ and those in care homes, and 11.5% selected carers and young carers as the second Surrey priority population most at risk of loneliness and social isolation.
Table 6: Second Surrey priority population most at risk of loneliness and social isolation (Source: Surrey Loneliness & Social Isolation Survey, January 2024).
| Second population most at risk of loneliness and social isolation | Count (n) | Percent (%) |
|---|---|---|
| People with long term health conditions, disabilities or sensory impairment | 76 | 25.0% |
| People experiencing homelessness | 39 | 12.8% |
| People with serious mental illness | 39 | 12.8% |
| Older people 80+ and those in care homes | 37 | 12.2% |
| Carers and young carers | 35 | 11.5% |
Survey respondents were also asked to identify ‘other’ populations at risk of loneliness and social isolation in Surrey who may not be one of Surrey’s Health and Wellbeing Strategy ‘priority populations’. 45.7% of all respondents answered this question. 9.5% identified people experiencing mental ill-health, anxiety and depression, 8.3% identified people with no friends or family networks, 7.1% identified people with autism, learning disabilities, SEND, or neurodiversity, 6% identified carers, 6% identified the LGBTQ+ population, 6% identified people with poor physical health, and 6% identified people at retirement.
Table 7: ‘Other’ population groups at risk of loneliness and social isolation in Surrey (Source: Surrey Loneliness & Social Isolation Survey, January 2024).
| Other populations at risk of loneliness and social isolation | Count (n) | Percent (%) |
|---|---|---|
| Mental Health/depression/anxiety | 8 | 9.5% |
| No Friends or Family Network | 7 | 8.3% |
| Autism/Learning Disabilities/Send/neurodiversity | 6 | 7.1% |
| Bereaved | 6 | 7.1% |
| Carers | 5 | 6.0% |
| LGBT | 5 | 6.0% |
| Poor physical health | 5 | 6.0% |
| Retired | 5 | 6.0% |
Additional qualitative evidence was provided during four loneliness and social isolation workshops for community-based wellbeing workers. Workshops were held across the four Places within Surrey Heartlands Integrated Care System:
Table 8: Breakdown of workshop locations, dates, and number of participants (Surrey loneliness and social isolation workshops, January 2024)
| Surrey Heartlands Place | Date of workshop | Number of participants |
|---|---|---|
| Surrey Downs | 11/01/2024 | 13 |
| East Surrey | 15/01/2024 | 11 |
| Guildford & Waverley | 19/01/2024 | 23 |
| Northwest | 22/01/2024 | 17 |
| Total | 64 |
Professionals who attended these sessions were from a range of wellbeing roles including social prescribing link worker, parenting coordinator, community connector, communities and prevention coordinator, wellbeing advisor, primary care network manager, health and wellbeing coach, community link officer, local area coordinator, care coordinator, mediator, and programme manager. Employers ranged from county council, district and borough councils, primary care networks, health sector, and voluntary and community sector.
Participants were asked five questions throughout the course of the workshops:
- In your professional experience, who is lonely?
- Why are they lonely?
- What gaps exist when it comes to resources in the community?
- What are some good examples of resources in the community?
- What makes the difference for people who are lonely and or social isolated? Why for some is loneliness a passing phase and for others it becomes chronic?
The answers to these questions were gathered and thematically analysed.
Who is lonely?
Professionals identified a range of people they have worked with who experience loneliness. These comments were gathered through either post-it notes or typed messages (for virtual sessions), and put into broader categories, as depicted below.
Figure 3: Cohorts identified as lonely by wellbeing professionals in Surrey through loneliness workshops, January 2024.
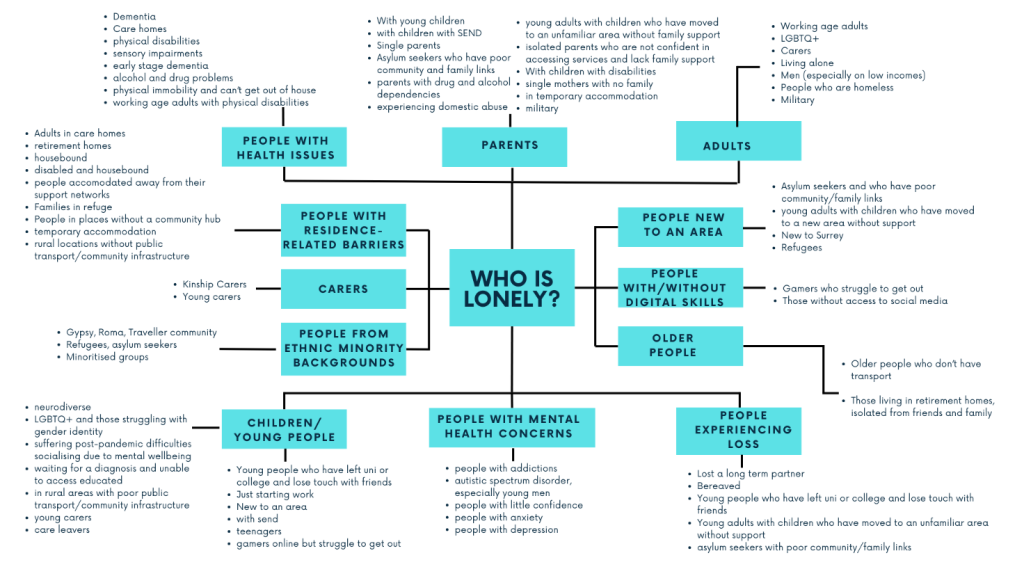
Table 9: Table showing cohorts identified as lonely by wellbeing professionals in Surrey through loneliness workshops, January 2024.
| Category | Further details of which groups are in each category |
|---|---|
| People with mental health concerns | • People with addictions • Autistic spectrum disorder, especially young men • People with little confidence • People with anxiety • People with depression |
| Children and young people (aged 0-25) | • Young people who have left university or college and lost touch with friends • Just starting work • New to an area • With SEND • Teenagers • Gamers online but struggle to get out • Neurodiverse • LGBTQ+ and those struggling with gender identity • Suffering post-pandemic difficulties socialising due to mental wellbeing • Waiting for a diagnosis and unable to access education • In rural areas with poor public transport/community infrastructure • Young carers • Care leavers |
| People from ethnic minority backgrounds | • Gypsy, Roma, Traveler community • Refugees, asylum seekers • Minoritised groups |
| Carers | • Kinship carers • Young carers |
| People with residence-related barriers | • Adults in care homes • Retirement homes • Housebound • Disabled and housebound • People accommodated away from their support network • Families in refuge • People in places without a community hub • Temporary accommodation • Rural locations without public transport/community infrastructure |
| People with health issues | • Dementia • Care homes • Physical disabilities • Sensory impairments • Early stage dementia • Alcohol and drug problems • Physical immobility and can’t get out of house • Working age adults with physical disabilities |
| Parents | • With young children • With children with SEND • Single parents • Asylum seekers who have poor community and family links • Parents with drug and alcohol dependencies • Experiencing domestic abuse • Young adults with children who have moved to an unfamiliar area without family support • Isolated parents who are not confident in accessing services and lack family support • With children with disabilities • Single mothers with no family • In temporary accommodation • Military |
| Adults | • Working age adults • LGBTQ+ • Carers • Living alone • Men (especially on low income) • People who are homeless • Military |
| People new to an area | • Asylum seekers and who have poor community/family links • Young adults with children who have moved to a new area without support • New to Surrey • Refugees |
| People with/without digital skills | • Gamers who struggle to get out • Those without access to social media |
| Older people | • Older people who don’t have transport • Those living in retirement homes, isolated from friends and family |
| People experiencing loss | • Lost a long term partner • Bereaved • Young people who have left university or college and lose touch with friends • Young adults with children who have moved to an unfamiliar area without support • Asylum seekers with poor community/family links |
Why are they lonely?
The next question posed to the professionals in the workshops was: Why are these people experiencing loneliness and/or social isolation? Participants were encouraged to reflect on this and respond through noting answers on posterboard, post-its or through virtual notes. These answers were gathered and thematically analysed into broad categories. These are depicted in the figure below.
Figure 4 Reasons for loneliness as identified by wellbeing professionals in Surrey through loneliness workshops, January 2024
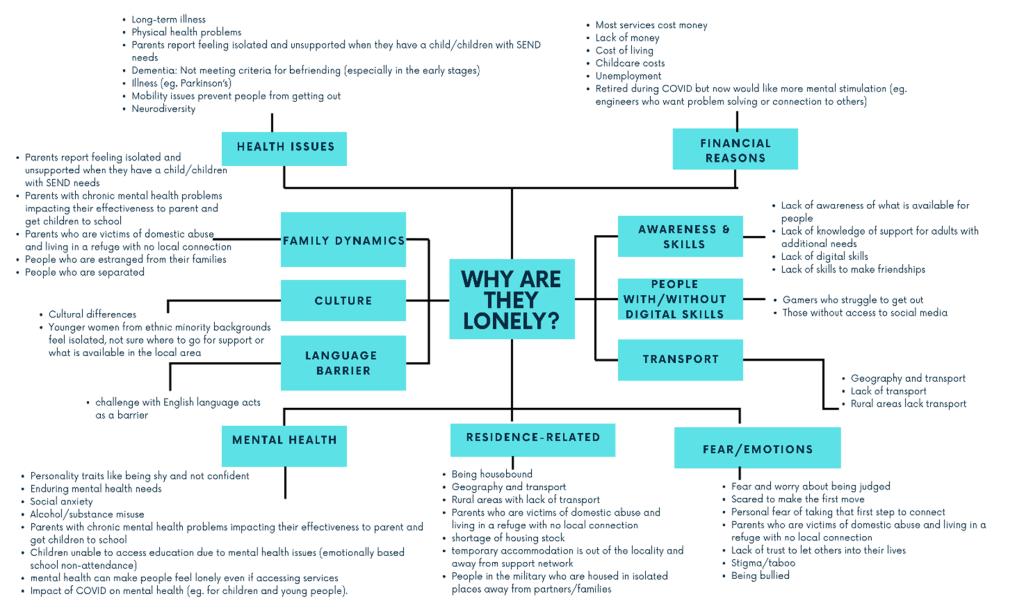
Table 10: Table of reasons for loneliness as identified by wellbeing professionals in Surrey through loneliness workshops, January 2024
| Category | Further details of reasons in each category |
|---|---|
| Health issues | • Long-term illness • Physical health problems • Parents report feeling isolated and unsupported when they have a child/children with SEND needs • Dementia – not meeting criteria for befriending (especially in the early stages) • Illness e.g. Parkinson’s disease • Mobility issues prevent people from getting out • Neurodiversity |
| Financial reasons | • Most services cost money • Lack of money • Cost of living • Childcare costs • Unemployment • Retired during COVID but now would like more mental stimulation (e.g. engineers who want problem solving or connection to others) |
| Awareness and skills | • Lack of awareness of what is available for people • Lack of knowledge of support for adults with additional needs • Lack of digital skills • Lack of skills to make friendships |
| People with/without digital skills | • Gamers who struggle to get out • Those without access to social media |
| Transport | • Geography and transport • Lack of transport • Rural areas lack transport |
| Fear/emotions | • Fear and worry about being judged • Scared to make the first move • Personal fear of taking that first step to connect • Parents who are victims of domestic abuse and living in a refuge with no local connection • Lack of trust to let others into their lives • Stigma/taboo • Being bullied |
| Residence related | • Being housebound • Geography and transport • Rural areas with lack of transport • Parents who are victims of domestic abuse and living in a refuge with no local connection • Shortage of housing stock • Temporary accommodation is out of the locality and away from support network • People in the military who are housed in isolated places away from partners/families |
| Mental health | • Personality traits like being shy and not confident • Enduring mental health needs • Social anxiety • Alcohol/substance misuse • Parents with chronic mental health problems impacting their effectiveness to parent and get children to school • Children unable to access education due to mental health issues (emotionally based school non-attendance) • Mental health can make people feel lonely even if accessing services • Impact of COVID on mental health (e.g. for children and young people) |
| Language barrier | • Challenge with English language acts as a barrier |
| Culture | • Cultural differences • Younger women from ethnic minority backgrounds feel isolated, not sure where to go for support or what is available in the local area |
| Family dynamics | • Parents report feeling isolated and unsupported when they have a child/children with SEND needs • Parents with chronic mental health problems impacting their effectiveness to parent and get children to school • Parents who are victims of domestic abuse and living in a refuge with no local connection • People who are estranged from their families • People who are separated |
Gaps in Resources
Wellbeing professionals in the workshops identified gaps in resources they have encountered when supporting people with loneliness and/or social isolation. Gaps were noted for particular cohorts, namely people with dementia, adults and young adults. The types of resources most cited by professionals were face to face support and befriending. Face to face activities and support were seen as important for young adults who may need the opportunity to socialise in person. Professionals also felt that buddying services were needed to help residents who may struggle to access community resources on their own. Having a buddy to ‘hold your hand’ to attend a first activity or session could be the difference between someone accessing a community group or resource, or not. Befriending for different age groups was also cited as a key gap. Befriending for younger residents and residents with dementia were of particular interest. Finally, peer support groups were seen as a need, as well as activities that run on weekends.
Supporting people who are lonely
Professionals reflected on what makes the difference when supporting someone who is lonely and/or socially isolated. Why is loneliness a passing phase for some people and for others it becomes chronic? Numerous factors were recorded by workshop participants and organised into themes (see below).
Figure 5: Factors that make a difference to the experience of loneliness, as identified by wellbeing professionals in loneliness workshops, January 2024
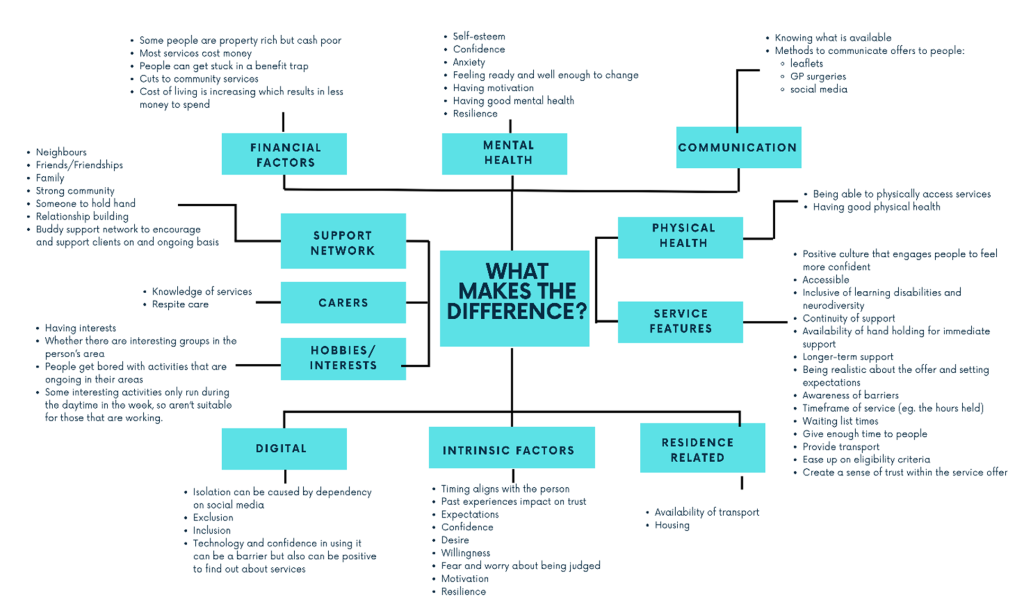
Table 11: Table of factors that make a difference to the experience of loneliness, as identified by wellbeing professionals in loneliness workshops, January 2024
| Category | Further details of factors in each category |
|---|---|
| Financial factors | • Some people are property rich but cash poor • Most services cost money • People can get stuck in a benefit trap • Cuts to community services • Cost of living is increasing which results in less money to spend |
| Mental health | • Self-esteem • Confidence • Anxiety • Feeling ready and well enough to change • Having motivation • Having good mental health • Resilience |
| Communication | • Knowing what is available • Methods to communicate offers to people: (leaflets, GP surgeries, social media) |
| Physical health | • Being able to physically access services • Having good physical health |
| Service features | • Positive culture that engages people to feel more confident • Accessible • Inclusive of learning disabilities and neurodiversity • Continuity of support • Availability of hand holding for immediate support • Longer-term support • Being realistic about the offer and setting expectations • Awareness of barriers • Timeframe of service (e.g. the hours held) • Waiting list times • Give enough time to people • Provide transport • Ease up on eligibility criteria • Create a sense of trust within the service offer |
| Residence related | • Availability of transport • Housing |
| Intrinsic factors | • Timing aligns with the person • Past experiences impact on trust • Expectations • Confidence • Desire • Willingness • Fear and worry about being judged • Motivation • Resilience |
| Digital | • Isolation can be caused by dependency on social media • Exclusion • Inclusion • Technology and confidence in using it can be a barrier but can be positive to find out about services |
| Hobbies/interests | • Having interests • Whether there are interesting groups in the person’s area • People get bored with activities that are ongoing in their areas • Some interesting activities only run during the daytime in the week, so aren’t suitable for those that are working |
| Carers | • Knowledge of services • Respite care |
| Support network | • Neighbours • Friends/friendships • Family • Strong community • Someone to hold hand • Relationship building • Buddy support network to encourage and support clients on an ongoing basis |
Approach to primary research
In addition to professional stakeholder engagement, the insights and experiences of residents and communities were sought using three approaches:
- A Citizens’ Panel survey.
- A Facebook community poll.
- Focus groups.
The Surrey County Council and Surrey Heartlands Health & Care Partnership (NHS) Citizens’ Panel brings together a selection of 2,000 local people to help the integrated care system understand residents’ views and ideas about a range of issues such as health, the environment, and the local economy. In February 2024 the Citizens’ Panel was asked to respond to a survey on loneliness and social isolation in Surrey. The total number of respondents was 940. The results were then weighted to make them more representative of the Surrey population.
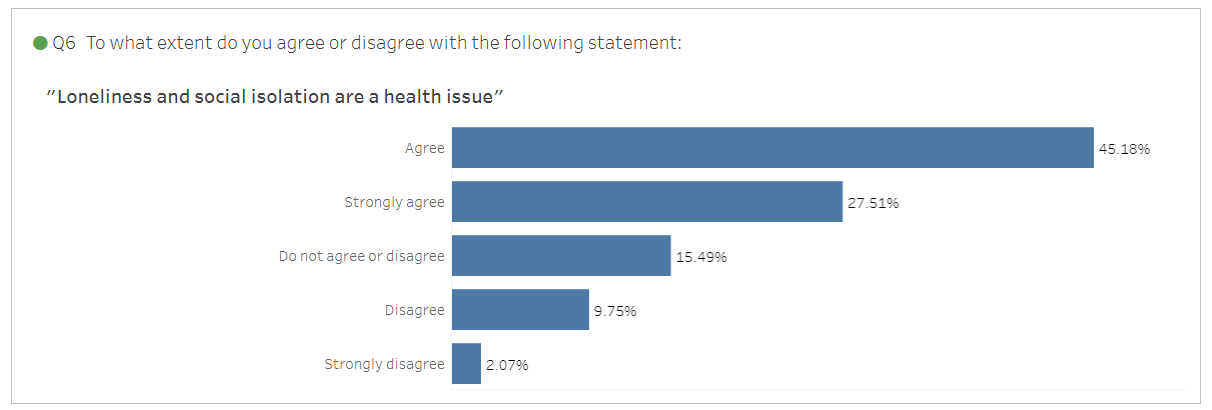
The Citizens’ Panel was asked to agree or disagree with the statement: ‘Loneliness and social isolation are a health issue’. 45.18% of respondents agreed with the statement, 27.51% strongly agreed, 15.49% neither agreed nor disagreed, 9.75% disagreed, and 2.07% strongly disagreed.
Figure 6: Citizens’ Panel Loneliness & Social Isolation Survey, February 2024 (Source: published on Tableau 19th March 2024).
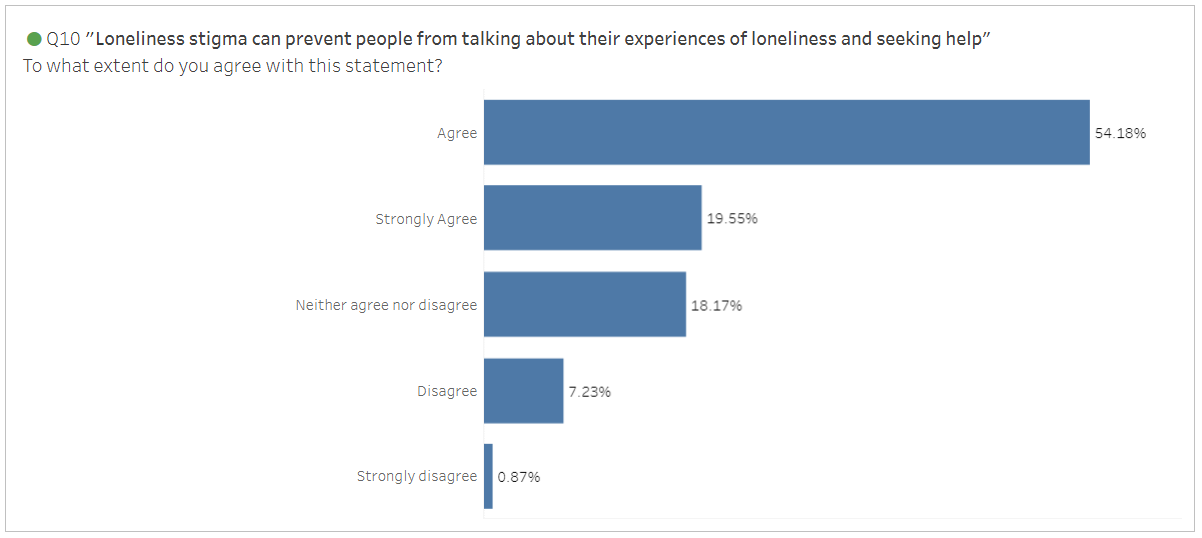
The Citizens’ Panel were also asked to agree or disagree with the statement: ‘Loneliness stigma can prevent people from talking about their experiences of loneliness and seeking help’. 54.18% of respondents agreed with this statement, 19.55% strongly agreed, 18.17% neither agreed nor disagreed, 7.23% disagreed, and 0.87% strongly disagreed.
Figure 7: Citizens’ Panel Loneliness & Social Isolation Survey, February 2024 (Source: published on Tableau 19th March 2024).
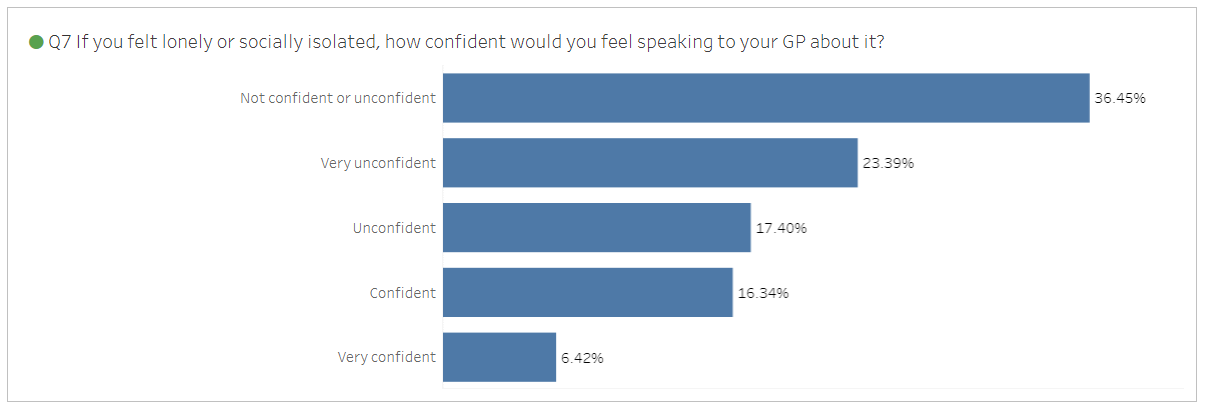
The Citizens’ Panel were asked to describe how confident they would feel talking to their GP about being lonely or isolated. 36.45% responded that they would not be neither confident nor unconfident talking to their GP, 23.39% would be very unconfident, 17.40% would be unconfident, 16.34% would be confident, and 6.42% would be very confident
Figure 8: Citizens’ Panel Loneliness & Social Isolation Survey, February 2024 (Source: published on Tableau 19th March 2024).
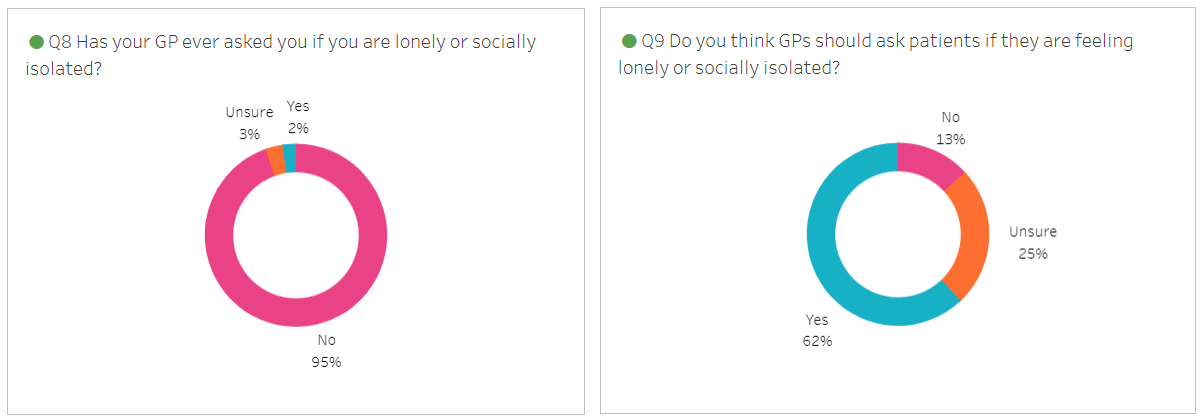
Respondents were also asked if their GP had ever spoken to them about loneliness and social isolation. 95% responded no, 2% said yes, and 3% were unsure. To the question, ‘Do you think GPs should ask patients if they are feeling lonely or isolated’, 62% responded yes, 13% responded no, and 25% were unsure.
Figure 9: Citizens’ Panel Loneliness & Social Isolation Survey, February 2024 (Source: published on Tableau 19th March 2024).
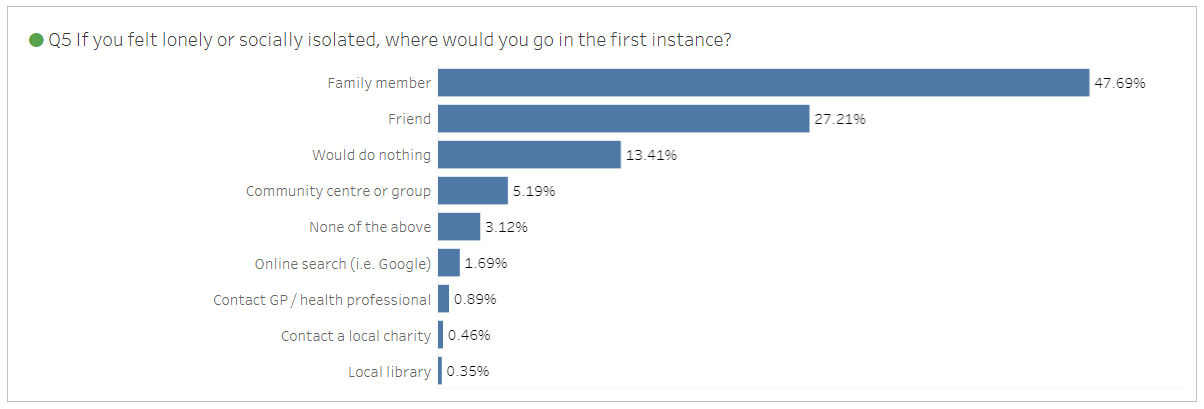
The Citizens’ Panel were asked where they would go for support if they felt lonely or isolated. Nearly half of respondents (47.69%) said they would go to a family member, 27.21% said they would go to a friend, 13.41% said they would do nothing, and the remainder said they would seek support from the community, online, or from a health professional.
Figure 10: Citizens’ Panel Loneliness & Social Isolation Survey, February 2024 (Source: published on Tableau 19th March 2024).
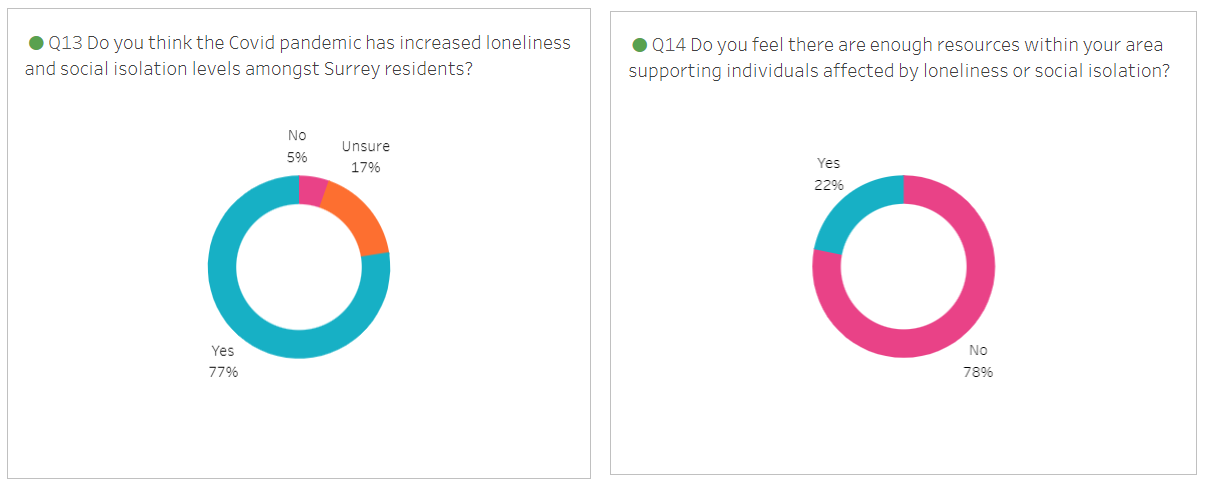
The Citizens’ Panel were asked if they thought Covid-19 had increased loneliness and social isolation for Surrey residents, and if they thought there were adequate community resources to address loneliness and social isolation in their area. Over three quarters (77%) of respondents thought that Covid-19 had increased levels of loneliness and social isolation in Surrey. 5% thought it had not and 17% were unsure. Nearly four fifths of respondents (78%) felt there were not enough community resources in their area to support people with loneliness and social isolation. 22% of respondents felt there were adequate community resources where they live.
Figure 11: Citizens’ Panel Loneliness & Social Isolation Survey, February 2024 (Source: published on Tableau 19th March 2024).
Surrey County Council’s 11 Community Link Officers (CLOs) work alongside partners, District & Borough Councils, County Councillors, and residents to increase connections within communities and build relationships to make meaningful change. CLOs work in the 21 key neighbourhoods that have been identified across Surrey as the areas that are experiencing the most economic and health challenges. They host community events and online sessions to develop deeper conversations with communities, asking residents what it’s like to live in their area.
A community poll on loneliness and social isolation was hosted on community Facebook pages managed by CLOs. The poll was also conducted in person at two ‘Community Lounge’ events. There were a total of 1208 responses to the poll, which included the following questions:
| 1. How friendly do you find your neighbourhood? | a. Very friendly b. Quite friendly c. Not very friendly d. Unfriendly |
| 2. Where you live, which of these is most important for helping people to feel connected to other people: | a. Community activities b. Public transport c. Access to health services d. Personal relationships |
| 3. Where I live the Covid pandemic has made people more isolated and/or lonely: | a. True b. False c. Don’t know |
| 4. Where I live the cost of living has made people more isolated and/or lonely: | a. True b. False c. Don’t know |
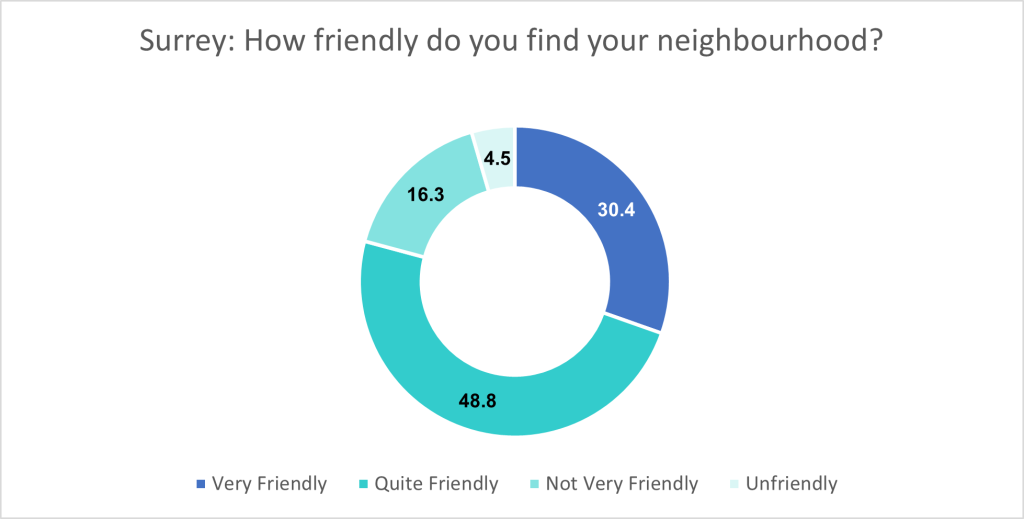
There were over 500 responses to the Facebook poll question ‘How friendly do you find your neighbourhood?’ In Surrey, 162 (30.4%) indicated their neighbourhood was ‘very friendly’, 260 (48.8%) ‘quite friendly’, and a fifth felt their neighbourhood was either ‘Not very friendly’ or ‘Unfriendly’.
Figure 12: Surrey Community Lounge Facebook poll, 2024.
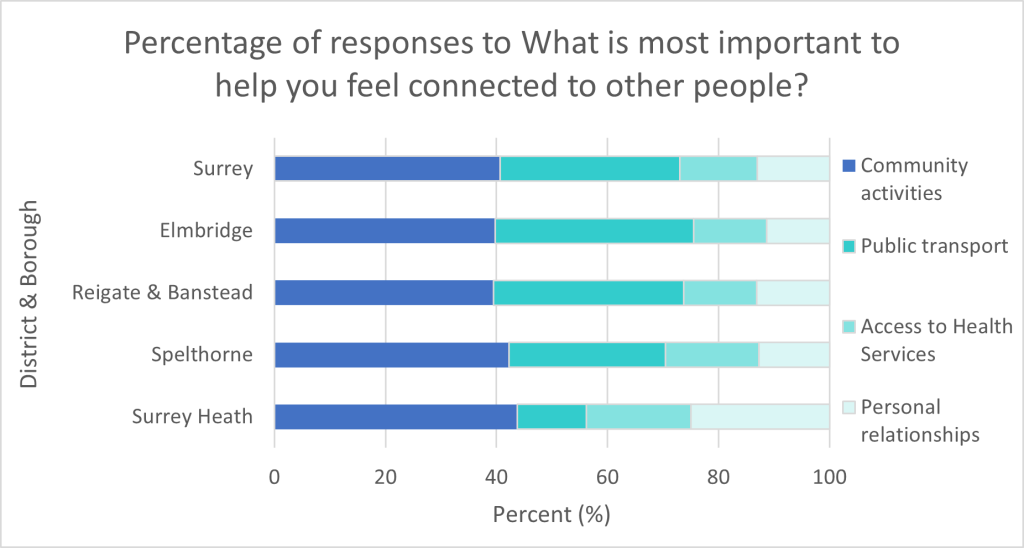
There were 416 responses to the question ‘Where you live, which of these is most important for helping people to feel connected to other people?’
Elmbridge (42.3%) had the highest number of responses to this question, followed by Reigate & Banstead (18.3%) and Spelthorne (17.1%).
Community activities was felt the most important to help people get connected to other people, except for Mole Valley (an urban area with significant rural areas), where more than half the responders felt public transport was more important.
Surrey Heath (25.0%) and Waverley (25.0%) thought personal relationships would help people to feel connected to other people.
Figure 13: Surrey Community Lounge Facebook poll, 2024.
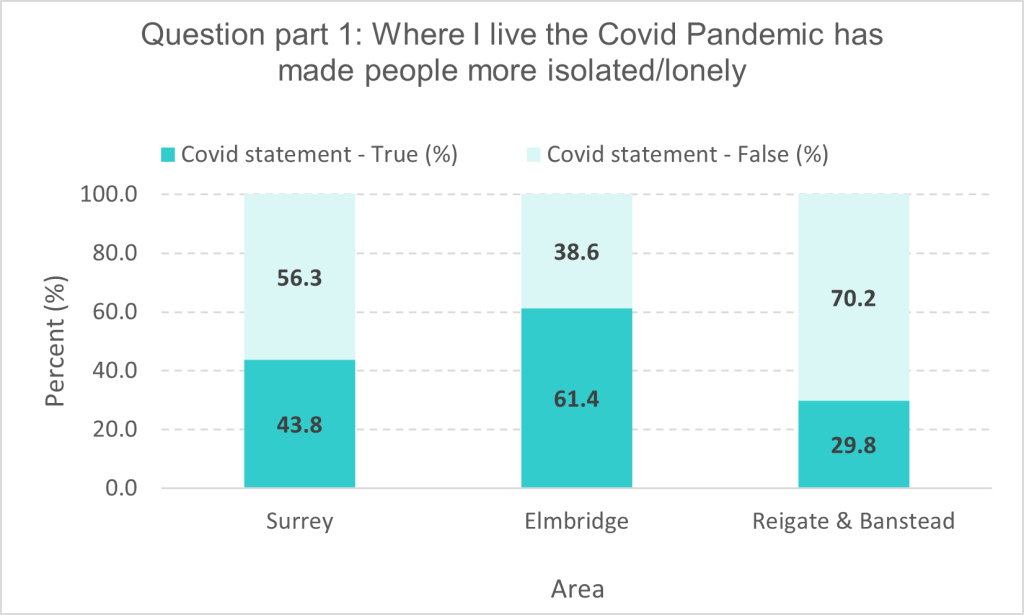
Statement 1 required a true or false response: ‘Where I live the Covid Pandemic has made people more isolated/lonely’. There were 112 responses of those 49 (43.8%) felt the Covid statement was true, whilst 63 (56.3%) felt the Covid statement was false. Elmbridge 27 (61.4%) and Reigate & Banstead 17(29.8%) responses indicated the covid statement was true.
Figure 14: Surrey Community Lounge Facebook poll, 2024. (Numbers of responses from other district and boroughs were too low to present.)
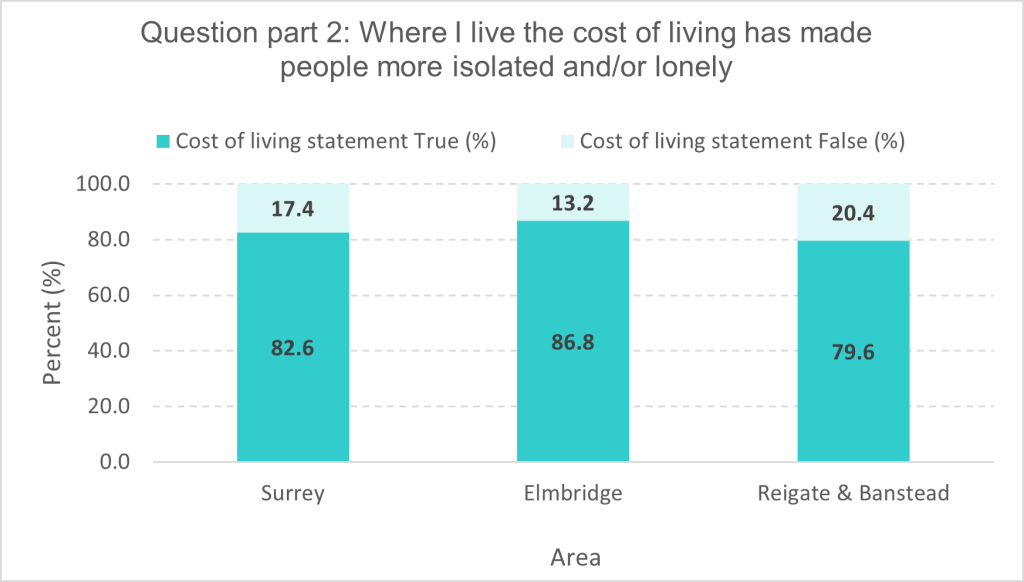
Statement 2 also required a true or false response: ‘Where I live the cost of living has made people feel more isolated and/or lonely’. There were 121 responses of those 100 (82.6%) felt the cost-of-living statement was true, whilst 21 (17.4%) felt the cost-of-living statement was false.
Elmbridge 46 (86.8%) and Reigate & Banstead 43 (79.6%) responses felt the cost of living had made people more isolated and/or lonely.
Figure 15: Surrey Community Lounge Facebook poll, 2024. (Numbers of responses from other district and boroughs were too low to present.)
Four focus groups were conducted to explore in more depth some of the themes arising from stakeholder engagement. Two of the focus groups were with young people, one for young people with emotional wellbeing and mental health needs and one for young people with additional needs and disabilities. Two further focus groups were with adults: one with disabled people and one with men who have emotional wellbeing and mental health needs.
Table 12: Table showing schedule of focus groups. (For an example of a focus group discussion guide, see Appendix 1).
| Focus Group | Cohort | Date & Time | Number of Participants |
|---|---|---|---|
| CYA Emotional Wellbeing & Mental Health | Young people with emotional wellbeing and mental health needs. | 11/04/24 18:30-19:15 | 6 |
| Surrey Coalition of Disabled People – Virtual Cafe | Adults with physical disabilities, long-term conditions, and sensory impairment. | 15/04/24 10:30-12:30 | 8 |
| ATLAS Group for Young People | Young people with additional needs and disabilities. | 17/04/24 17:00-18:30 | 6 |
| Andy’s Man Club | Men with emotional wellbeing and mental health needs. | 22/04/24 17:00-18:30 | 6 |
What do we know about loneliness and social isolation?
LSI research and health & wellbeing impacts of LSI
It is difficult to estimate precisely the prevalence of loneliness and social isolation. This is due to variation across the life course, ‘cultural and gender differences with respect to how prepared individuals are to talk about them from a personal perspective and the use of many different measurement scales, some of which are based on self-report questionnaires while others involve more objective assessment of social contact or networks (or a combination of both)’.[16]
Loneliness and social isolation are important social determinants of health that impact on wellbeing, longevity, physical and mental health. This is a public health concern that can impact people from all socio-economic groups, ages, ethnicities, and backgrounds.
Loneliness impacts on health and wellbeing in three primary ways[17]:
- Behavioural: People who experience loneliness are more likely to take part in unhealthy behaviours such as smoking.
- Psychological: Loneliness impacts on mental wellbeing with evidence showing a decrease in coping mechanisms and lower self-esteem.
- Physiological: The physical health impacts of loneliness are increasingly demonstrated and include increased risk of high blood pressure, heart disease, stroke[18], and type 2 diabetes[19].
Intersecting social determinants of health influence both the risk of being socially isolated and lonely as well as the access and uptake of interventions[20]. The risk of loneliness and social isolation on mortality are comparable to other social determinants of health, such as smoking, obesity, and physical inactivity[21]. Research has shown that loneliness is a predictor of suicidal ideation and behaviour[22]. Loneliness and social isolation increase the risk of suicide, particularly among men aged 40 to 54 and young people aged 20 to 24. Of these men who died by suicide in the UK, 45% reported living alone and 11% had reported recent social isolation[23]. Of the suicide by children and young people, 15% had reported social isolation[24].
Social isolation and loneliness could be linked to increased inflammation in the body[25].
Social connection can support people to improve their mental and physical health. People who belong to groups and have a social identity can take advantage of the “social cure”, which promotes adjustment, coping and well-being for individuals dealing with a range of illnesses, injuries, trauma, and stressors[26].
There is growing evidence on the impact of loneliness and social isolation on health and care systems. Loneliness is associated with more general practice contacts, emergency treatments, hospital admissions[27], and higher mental health expenditure[28]. Furthermore, the collective wellbeing, health, and work productivity cost of severe loneliness is approximately £9,900 per person/year[29]. The breakdown of estimated costs of mild, moderate, and severe loneliness can be seen in the table below.
Table 13: The impacts of loneliness per person per year in monetary terms[30]
| Impacts: | Lack of, to mild loneliness |
Mild to moderate loneliness |
Moderate to severe loneliness |
|---|---|---|---|
| Health | Evidence NA | Evidence NA | £109 |
| Productivity | Evidence NA | Evidence NA | £330 |
| Wellbeing | £6,429 | £8,157 to £9,537 | (at least) £9,537 |
| Total | £6,429 | £8,157 to £9,537 | (at least) £9,976 |
The cost of loneliness to employers in the United Kingdom has been estimated as being £2.5 billion due to increased staff turnover, reduced productivity, the impact of caring responsibilities and sickness absence related to ill health[31].
An overview of systematic reviews recommends that: ‘Policy makers and health and local government commissioners should consider social isolation and loneliness as important upstream factors impacting on morbidity and mortality due to their effects on cardiovascular and mental health. Prevention strategies should therefore be developed across the public and voluntary sectors, using an asset-based approach’ [32].
Impact of COVID-19
Office for National Statistics data shows that lockdowns during the Covid-19 pandemic drove up levels of chronic loneliness. By the beginning of 2021, 3.7 million adults reported feeling lonely ‘often’ or ‘always’[33]. This was up from 2.6 million in 2020. However, the pandemic largely exacerbated existing inequalities so that people who were already lonely became lonelier and people with good family and social support networks were more resilient. Whilst the high rates of loneliness associated with the pandemic are not expected to persist, one group emerged as still struggling with the impact of Covid-19 on social connection. People aged 18-29 continue to report levels of anxiety and depression that are above pre-pandemic rates [34], and whilst objective levels of social isolation have decreased young people continue to experience subjective feelings of loneliness.
People living in urban areas were more likely to be lonely (8.3%) than those living in rural areas (5.7%)[35]. Feelings of loneliness intensified for people with a learning disability during the pandemic [36]. Loneliness during Covid-19 also disproportionately affected disabled people, people on low incomes, people with a mental health condition, people who live alone, people from ethnic minority communities, parents with young children, and people who are digitally excluded [37].
Changing work patterns during Covid-19 lockdowns that saw more people working from home or hybrid working increased people’s feelings of loneliness at work. However, a report by the British Red Cross on behalf of the All Party Parliamentary Group (APPG) on Tackling Loneliness and Connected Communities found that post-pandemic home workers are no more likely to experience loneliness than those working on site [38]. Loneliness at work disproportionately affects disabled workers and those with a long-term health condition with 24% likely to experience loneliness compared with 9% of workers not affected by disability or ill-health. Senior managers are twice as likely than average to report higher levels of loneliness [39].
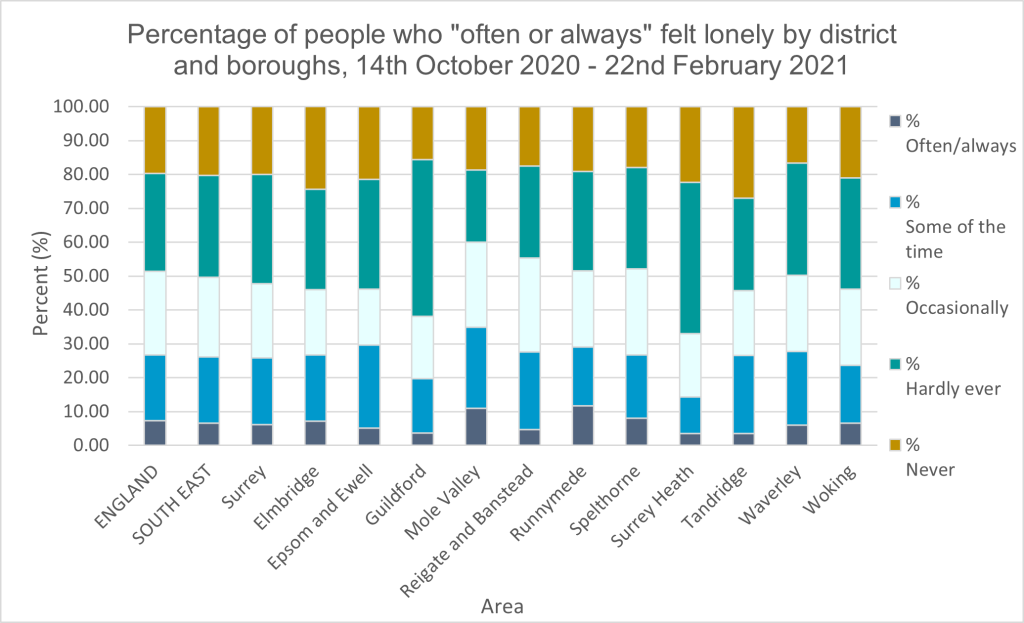
The data below shows those adults aged 16 years and over across Surrey who were asked how often they felt lonely and responded with “often or always”. Other response options included: “some of the time”, “occasionally”, “hardly ever” and “never”.
Figure 16: Office for National Statistics – Opinion and Lifestyle Survey.
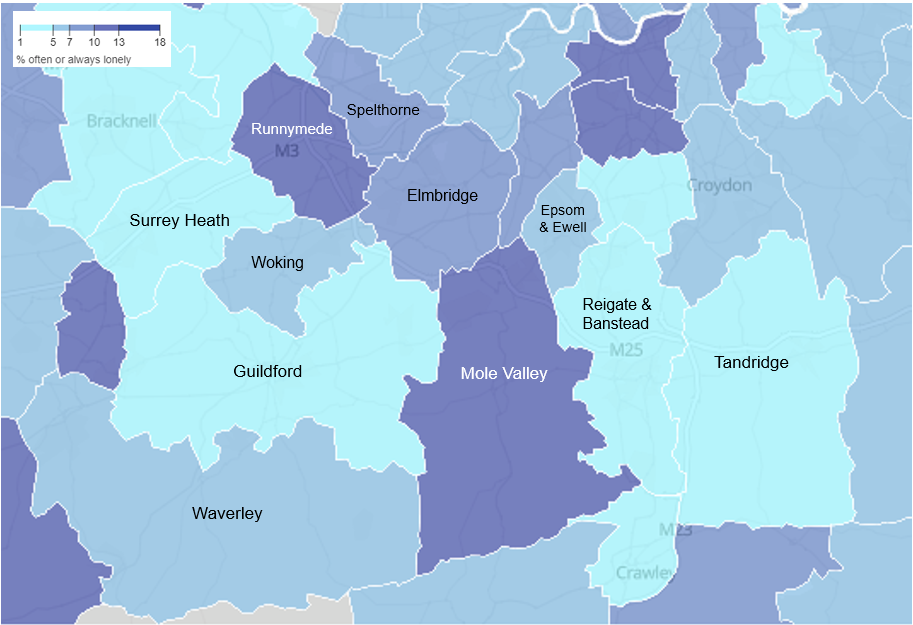
The map shows percentage of adults aged 16 years and over who were asked how often they felt lonely, responding to “often or always”. Feeling lonely ‘often or always’ does not seem to correlate with living in areas that are either more urban or more rural.
Figure 17: Office for National Statistics – Opinion and Lifestyle Survey.
Surrey’s Covid-19 Community Impact Assessment on health and wellbeing highlights the disproportionate impact of the pandemic and associated lockdown measures on:
- Domestic abuse survivors
- Dementia patients
- Individuals in residential care
- Older individuals shielding
- People with disabilities and chronic conditions
- Newly unemployed people
- Unpaid carers
- Working-age adults living alone
- Parents and families of children with additional needs and disabilities.
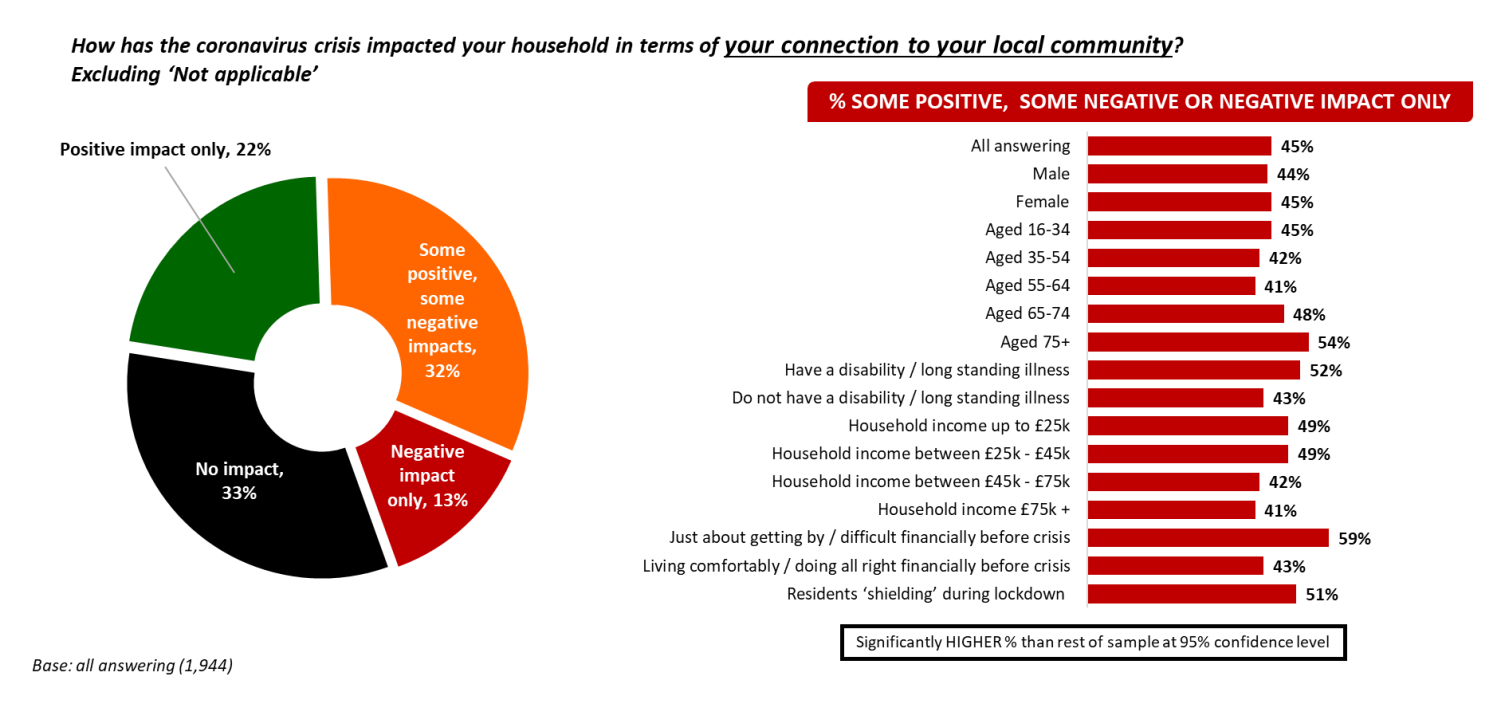
Findings from the Surrey COVID-19 Impact Survey suggest that the pandemic had an impact on community cohesion and peoples’ sense of belonging. Just under half of residents reported that the coronavirus crisis had a negative impact on their connection to their local community. This perceived negative impact was highest amongst residents aged 75 or over, residents with a disability or long-standing illness, lower income households as well as shielding residents. This indicates that Covid disproportionately affected those less physically and socially mobile.
Figure 18: Surrey Covid-19 Community Impact Assessment (Social Cohesion, Community and Place Findings).
Those who live rurally reported an overall sense of community in their town or village, whilst those in urban or suburban areas reported only becoming more neighbourly with those near them. In urban and suburban areas, a sense of community was limited to the few people living in close proximity.
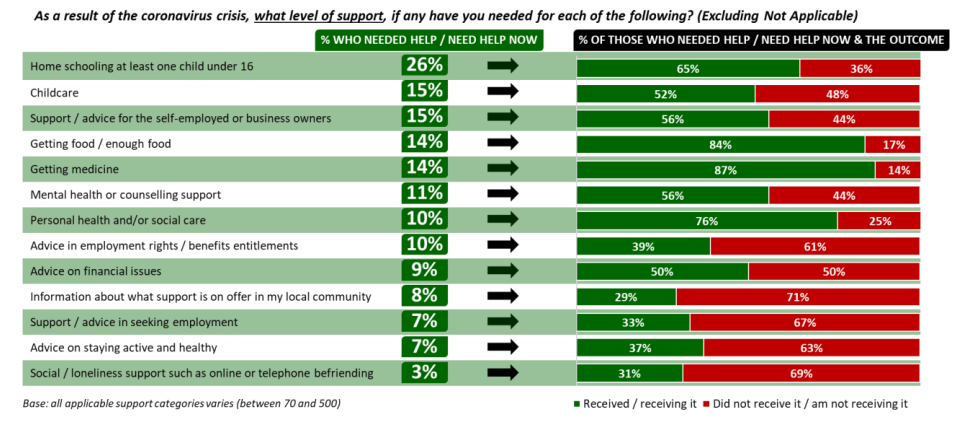
Whilst there was good support for people who needed help with food or medicine during the pandemic, 69% of those who reported needing support with social isolation or loneliness did not receive it[40].
Figure 19: Surrey Covid-19 Community Impact Assessment (Access and Use of Services Findings).
In terms of the geographical impact of Covid-19 at the Middle Layer Super Output Areas (MSOA) level, Surrey’s Covid-19 Recovery Community Impact Assessment (Geographical Impact Assessment) found that high combined impacts on health, economics and vulnerable groups are found in the North, South East and South West of the county, with the highest numbers in Spelthorne, Mole Valley and Waverley. The findings on vulnerable groups are most relevant to this chapter because of the correlation between key vulnerabilities and experiences of loneliness and social isolation.
Figure 20: Surrey Covid-19 Community Impact Assessment (Geographical Impact Assessment).
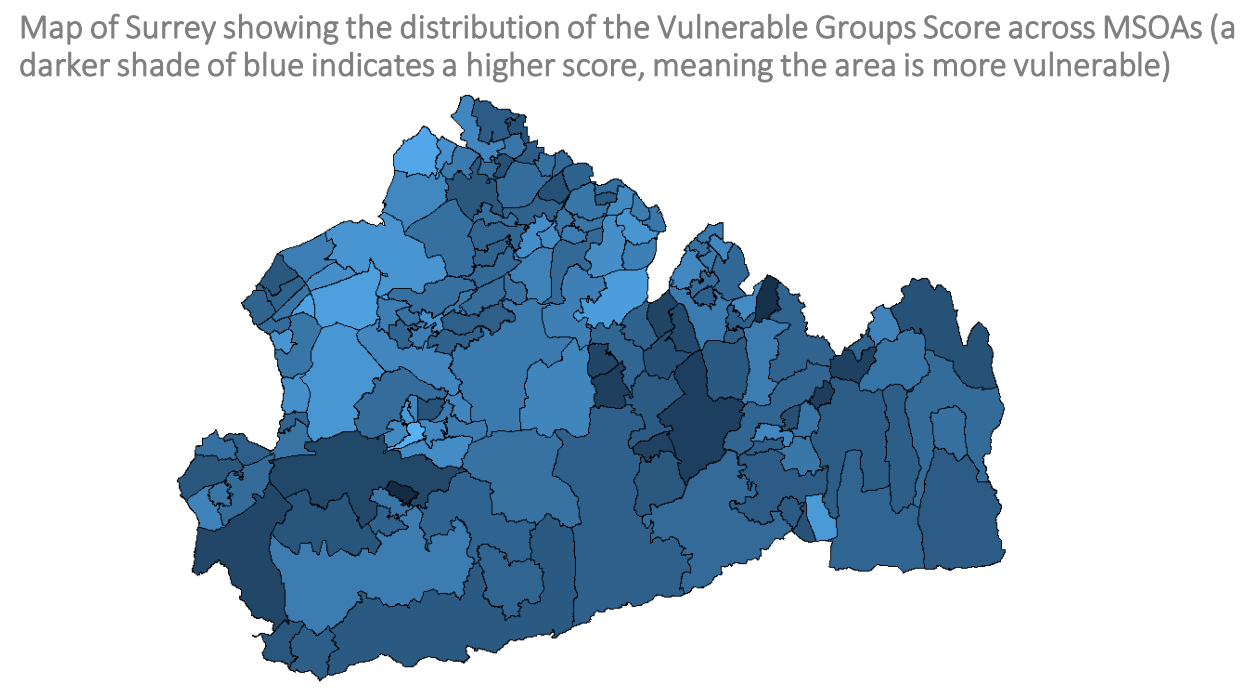
The top 5 most impact MSOAs in the vulnerable groups dimension are:
- Farncombe (Waverley)
- Banstead (Reigate & Banstead)
- Merstham (Reigate & Banstead)
- Bookham South (Mole Valley)
- Box Hill and Brockham (Mole Valley).
The MSOAs that have higher numbers of vulnerable groups are not necessarily the most deprived.
Cost of living crisis
The level of poverty in the UK is high, worsened by the pandemic and the cost-of-living crisis. The 2019 Indices of Multiple Deprivation show that in Surrey there are several pockets of deprivation and four areas in the most deprived 20% nationally.
The cost-of-living crisis is pulling more people into poverty in the UK, and this has implications for health and wellbeing, including loneliness and social isolation. According to the Joseph Rowntree Foundation’s UK Poverty 2024 report[41], more than one in five people in the UK were in poverty in 2021/22 – 14.4 million people. This included:
- 8.1 million working age adults.
- 4.2 million children
- 2.1 million pensioners.
The report identifies groups of people who face particularly high levels of poverty:
- Larger families
- Families whose childcare responsibilities limit their abilities to work
- Many minority ethnic groups
- Disabled people
- Informal carers
- Families not in work
- Part-time workers and the self-employed
- People living in rented accommodation
- Families claiming income-related benefit.
Evidence shows that poverty and the cost-of-living crisis is having an impact on social connections and may be causing people to feel lonelier. In a 2023 YouGov survey from FareShare, charities that provide community meals reported being extremely concerned about the wellbeing of people they support, due to increased loneliness and isolation linked to food insecurity[42]. The same survey revealed that almost half (42%) of 18 to 24 year-olds in the UK are cutting back on socialising with friends due to the cost of living crisis, and over half (52%) of 25 to 34 year olds will avoid meeting with friends, suggesting the rising costs of socialising are adding to the rising rate of loneliness in the UK.
The YouGov survey also showed that people in the UK are increasingly concerned with how rising costs impact their community’s lives. Six out of 10 agreed that people were at higher risk of loneliness due to the cost-of-living crisis. Voluntary and community groups are facing both rising costs and rising demand because of the cost-of-living crisis[43].
According to ethnographic research in five of Surrey’s key neighbourhoods, the cost of living crisis is having an acute impact on the health and wellbeing of residents. It is also causing people to feel lonelier. Among adult women on low incomes living in Chertsey St Anne’s, Goldworth Park, Old Dean, Stoke or Court Ward, for example, 54% felt more alone due to the cost of living. The cost-of-living crisis and its impact on loneliness disproportionately affects residents on lower incomes. In neighbourhoods with strong support networks and community infrastructure there is greater resilience to the impact of rising living costs and associated loneliness.
The HWB Strategy and the Surrey Heartlands Integrated Care Strategy both acknowledge poverty as a key determinant of health. The first HWB Strategy Index Annual Scorecard includes key indicators related to poverty and the cost of living. 8% of households in Surrey are now experiencing fuel poverty, an increase of 1% / nearly 5,000 households in 12 months (Office for National Statistics) and 28% of those surveyed in Spelthorne had accessed a food bank or other community food provision in the last 6 months (new Joint Neighbourhood survey)[44]. The Chair of the Health and Well-Being Board has signed the Good Company’s End Poverty Pledge, which states: ‘We commit to do what we can to work towards a poverty-free future in Surrey’[45].
Surrey geographical data
According to Office for Health Improvement and Disparities (OHID) figures, the number of adults aged 16+ who feel lonely often or always, or some of the time is lower in the Southeast than the national average, and Surrey scores lower than the average for the Southeast.
Figure 21: Percentage of adults aged 16+ who feel lonely often, always or some of the time. (Source: OHID, 2019/20).
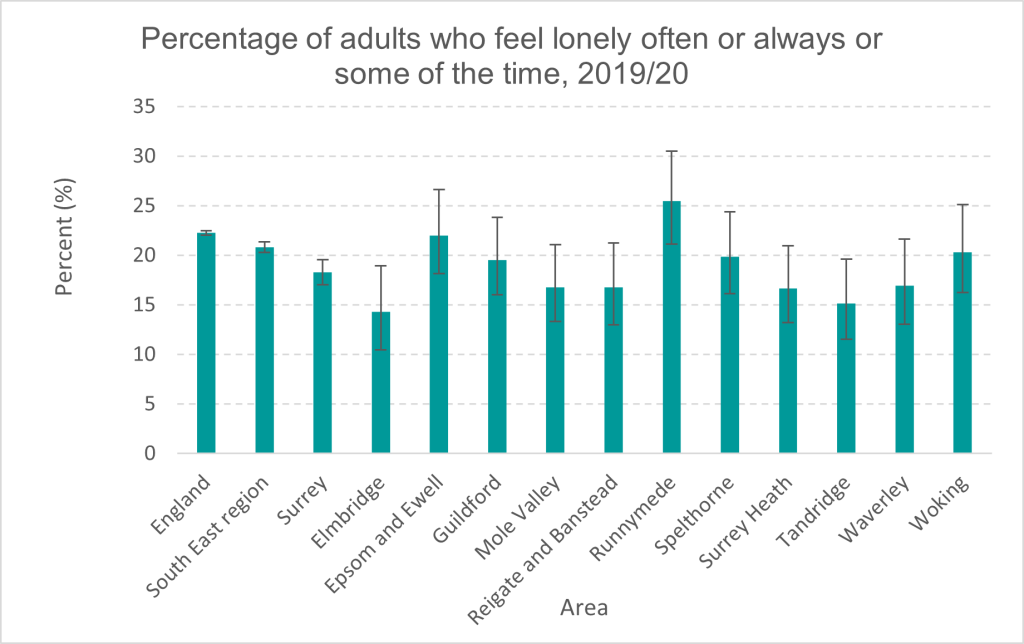
Runnymede (25.46%) identified more adults who felt lonely “often always or some of the time”, which is higher than the national average (22.26%). Elmbridge (14.30%) and Tandridge (15.16%) identified the least number of responders who felt lonely “often always or some of the time”.
The GP Patient Survey is an annual survey of patient experience of British general practice. It is one of the largest ever survey programmes of patients registered to receive primary health care. It is now sent out to over two million people across England. The results are weighted to provide a statistically valid picture of how all patients at a practice might feel if everyone has responded. The GP Patient Survey asks respondents to self-report on their experiences of several areas of health that are relevant to loneliness:
- Feeling isolated from others
- Problems with physical mobility
- Experience of two or more falls requiring medical attention.
The results for Surrey Heartlands ICB and Frimley ICB can be compared with other ICBs within the Southeast region:
Table 14: Table showing comparable data for ICBs in the Southeast (Source: GP Patient Survey, January to March 2023).
| Have you experienced any of the following over the last 12 months? | Buckingham, Oxfordshire and Berkshire Percent (%) |
Frimley Percent (%) |
Hampshire and Isle of Wight Percent (%) |
Kent and Medway Percent (%) |
Surrey Heartlands Percent (%) |
Sussex Percent (%) |
|---|---|---|---|---|---|---|
| Feeling isolated from others | 7% | 7% | 8% | 8% | 6% | 8% |
| Problems with your physical mobility, for example, difficulty getting about your home | 11% | 11% | 13% | 14% | 10% | 13% |
| Two or more falls that have needed medical attention | 2% | 2% | 2% | 2% | 2% | 2% |
Figure 22: Chart showing comparable data for ICBs in the Southeast (Source: GP Patient Survey, January to March 2023).
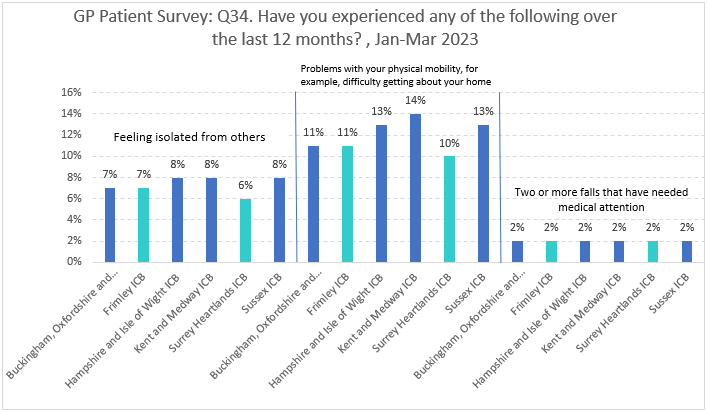
The results show that 6% of GP patients in Surrey Heartlands ICB and 7% in Frimley ICB felt isolated from others. These figures are comparable with or lower than the other ICBs in the Southeast. 10% of GP patients in Surrey Heartlands and 11% in Frimley reported problems with physical mobility, which is also comparable with or lower than other ICBs in the Southeast. Across all ICBs 2% of patients reported having two or more falls that required medical attention.
Patients feeling isolated from others can also be analysed by age.
Table 15: Table showing percentage of patients by age feeling isolated from others. (Source: GP Patient Survey, January to March 2023).
| Integrated Care Board | Total | Aged 16 to 24 |
Aged 25 to 34 |
Aged 35 to 44 |
Aged 45 to 54 |
Aged 55 to 64 |
Aged 65 to 74 |
Aged 75 to 84 |
Aged 85 and over |
|---|---|---|---|---|---|---|---|---|---|
| Buckingham, Oxfordshire, and Berkshire ICB | 7% | 11% | 9% | 6% | 8% | 5% | 4% | 5% | 11% |
| Frimley ICB | 7% | 12% | 10% | 8% | 6% | 5% | 4% | 5% | 9% |
| Hampshire & Isle of Wight ICB | 8% | 13% | 11% | 8% | 9% | 7% | 5% | 5% | 9% |
| Kent and Medway ICB | 8% | 15% | 11% | 8% | 8% | 7% | 6% | 6% | 11% |
| Surrey Heartlands ICB | 6% | 10% | 8% | 5% | 6% | 6% | 4% | 5% | 10% |
| Sussex ICB | 8% | 12% | 11% | 10% | 9% | 6% | 5% | 6% | 11% |
Figure 23: Chart showing percentage of patients by age feeling isolated from others. (Source: GP Patient Survey, January to March 2023).
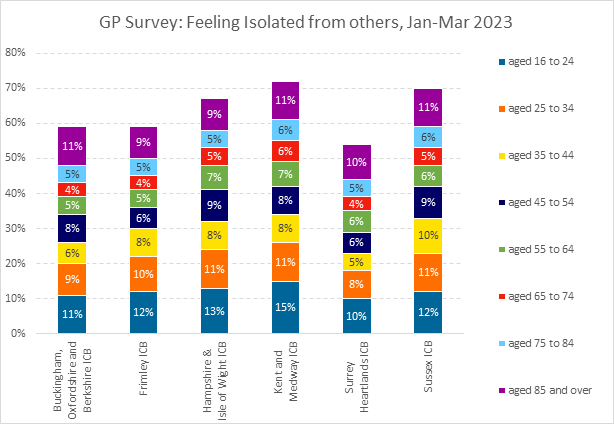
Table 16: Table showing percentage of patients by age feeling isolated from others. (Source: GP Patient Survey, January to March 2023).
| Integrated Care Board | Aged 16 to 24 |
Aged 25 to 34 |
Aged 35 to 44 |
Aged 45 to 54 |
Aged 55 to 64 |
Aged 65 to 74 |
Aged 75 to 84 |
Aged 85 and over |
|---|---|---|---|---|---|---|---|---|
| Buckingham, Oxfordshire, and Berkshire ICB | 11% | 9% | 6% | 8% | 5% | 4% | 5% | 11% |
| Frimley ICB | 12% | 10% | 8% | 6% | 5% | 4% | 5% | 9% |
| Hampshire & Isle of Wight ICB | 13% | 11% | 8% | 9% | 7% | 5% | 5% | 9% |
| Kent and Medway ICB | 15% | 11% | 8% | 8% | 7% | 6% | 6% | 11% |
| Surrey Heartlands ICB | 10% | 8% | 5% | 6% | 6% | 4% | 5% | 10% |
| Sussex ICB | 12% | 11% | 10% | 9% | 6% | 5% | 6% | 11% |
Data shows an even distribution of feeling isolated from others across the life course. In Surrey Heartlands ICB 19% of patients aged 65 and over reported feeling isolated from others but 18% of 16 to 34 year olds also felt isolated. In Frimley ICB 18% of patients aged 65 and over reported feeling isolated from others but 22% of 16 to 34 year olds felt isolated.
GP Patient Survey data on isolation can also be shown at Place level and for Primary Care Networks (PCNs).
Figure 24: GP Patient Survey data on isolation by Place
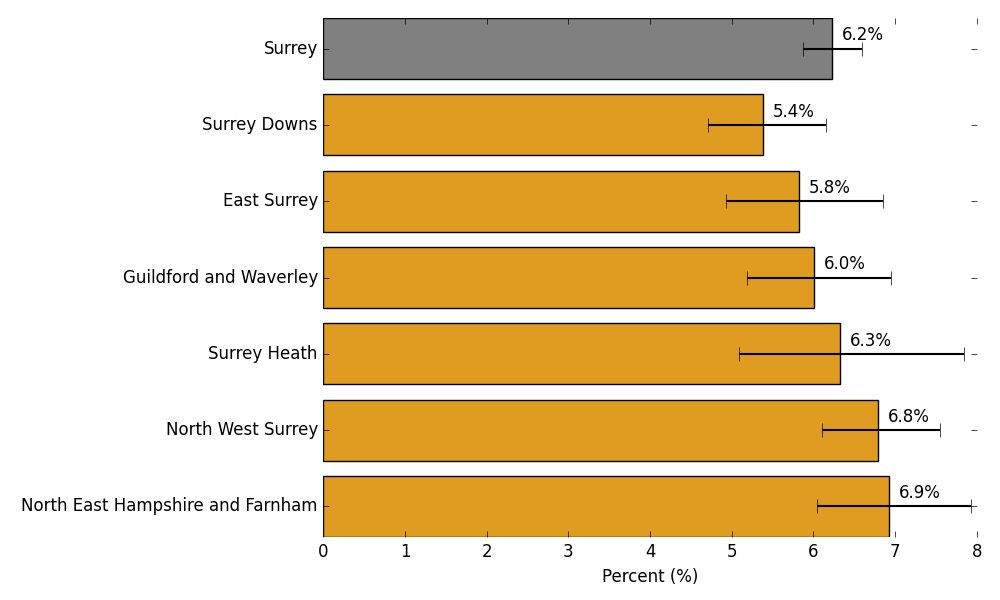
Northeast Hampshire and Farnham in Frimley ICB report the highest percentage of patients feeling isolated from others. Surrey Downs in Surrey Heartlands ICB reports the lowest percentage of patients feeling isolated from others. The value for England is 8.7% and 6.2% for Surrey.
Figure 25: Patients feeling isolated from others by Primary Care Network. (Source: GP Patient Survey, January to March 2023).
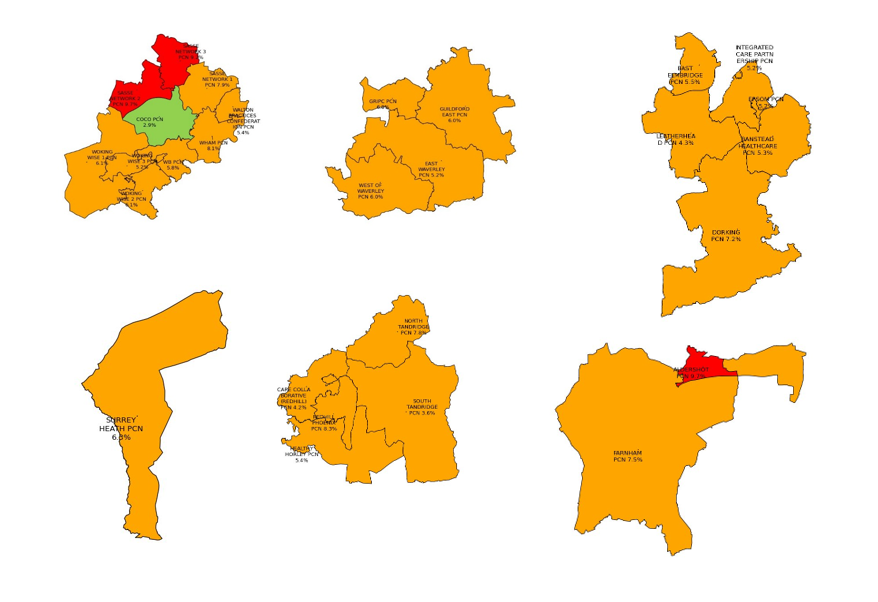
SASSE Network 2 (9.7%), SASSE Network 3 (9.2%), and Redhill Pheonix PCN (8.3%) have the highest percentage of patients who report feeling isolated from others. Aldershot PCN (9.7%) is in Hampshire. CoCo PCN has the lowest percentage. If this data is combined with the Loneliness Index, we can start to identify PCNs with the highest proportion of patients at risk of loneliness and social isolation.
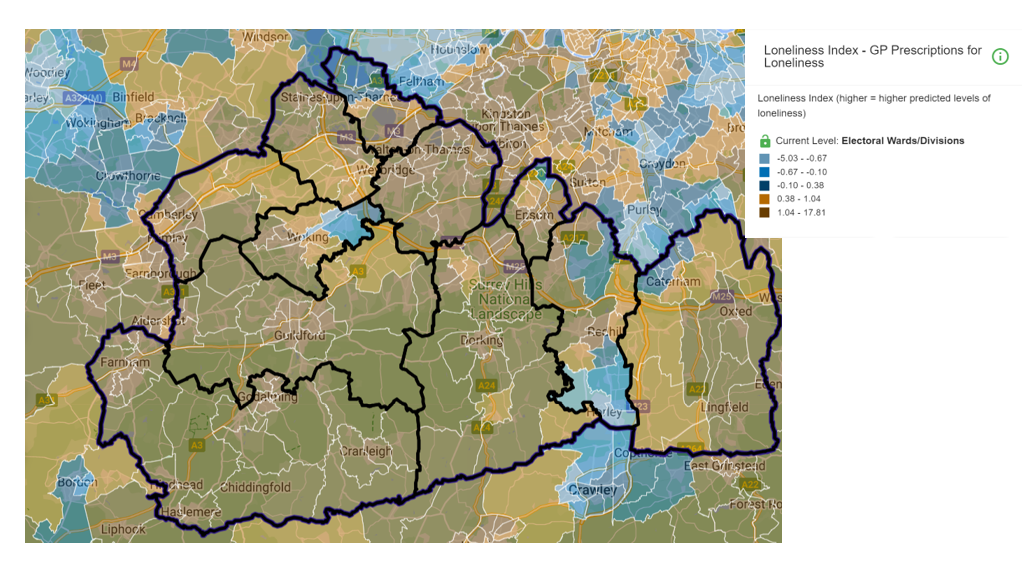
The Loneliness Index is created by using GP prescription data to find areas with above average prescriptions for five conditions where loneliness has been shown to be a risk factor: Alzheimer’s, depression, high blood pressure, anxiety, and insomnia. An index was created for each condition by standardising the proportion of a practices prescriptions that were given for the condition relative to the levels in other practices (into z scores). The index for each condition had a value that was negative if prescribing was lower than typical and positive if it was greater than typical. The loneliness index is generated by summing together these standardised scores for each condition[46].
Figure 26: Loneliness Index – GP Prescriptions for Loneliness map.
Many factors impact on people’s experiences of feeling lonely or socially isolated across the life course but where people live, how connected a community is, and the extent to which people feel they belong in their communities can be an influence alongside life events, health status, and other vulnerabilities. The Community Dynamics data set has been developed by Social Life with the aim of quantifying how people feel about the area they live in. By modelling responses from the annual Community Life Survey and Understanding Society Survey to Output Areas, Social Life have created small area measures of:
- strength of local social relationships
- strength of belonging to a local area
- satisfaction with a local area as a place to live.
Positive values represent greater belonging/relationship strength/satisfaction than the national average. Negative figures represent less belonging/relationship strength/satisfaction than the national average. The values presented here offer an indication of community belonging, strength and satisfaction rather than an absolute measure.
Data sets for Surrey’s Key Neighbourhoods showing the individual satisfaction, relationship and belonging scores are shown in Appendix 2.
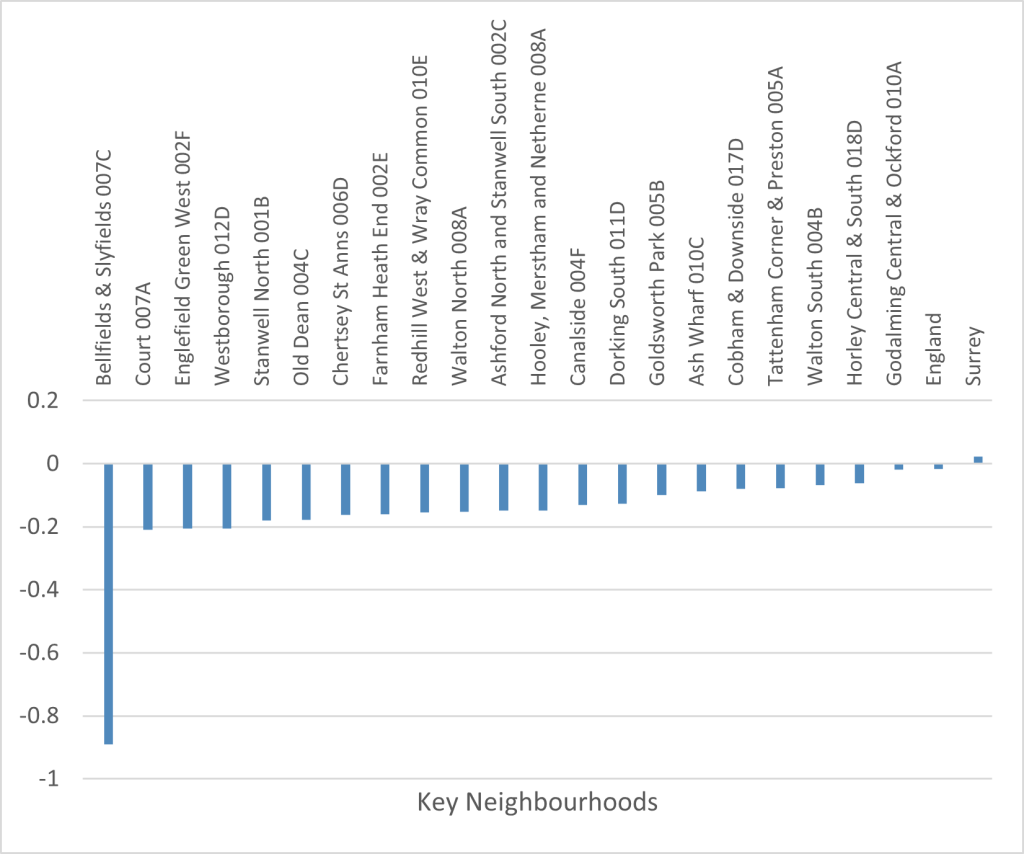
The combined scores for satisfaction, relationships, and belonging show that Bellfields & Slyfields (007C) in Guildford has the lowest combined neighbourhood satisfaction score (-0.89). Godalming Central and Ockford (010A) in Waverley has the highest combine score of Surrey’s key neighbourhoods. Surrey’s combined score (0.022) is higher than the combined score for England (-0.016). All the key neighbourhoods have a lower combined score for neighbourhood satisfaction than the combined average for England.
Table 17: Table showing combined neighbourhood satisfaction scores for key neighbourhoods, Surrey, and England (Source: Community Insight Report, April 2023).
| Key Neighbourhood | District & Borough | Neighbourhood Satisfaction – combined score |
|---|---|---|
| England | England | -0.016 |
| Surrey | Surrey | 0.022 |
| Bellfields & Slyfields 007C | Guildford | -0.89 |
| Court 007A | Epsom & Ewell | -0.209 |
| Englefield Green West 002F | Runnymede | -0.206 |
| Westborough 012D | Guildford | -0.205 |
| Stanwell North 001B | Spelthorne | -0.18 |
| Old Dean 004C | Surrey Heath | -0.178 |
| Chertsey St Anns 006D | Runnymede | -0.162 |
| Farnham Heath End 002E | Waverley | -0.16 |
| Redhill West & Wray Common 010E | Reigate & Banstead | -0.154 |
| Walton North 008A | Elmbridge | -0.153 |
| Ashford North and Stanwell South 002C | Spelthorne | -0.149 |
| Hooley, Merstham and Netherne 008A | Reigate & Banstead | -0.149 |
| Canalside 004F | Woking | -0.131 |
| Dorking South 011D | Mole Valley | -0.126 |
| Goldsworth Park 005B | Woking | -0.1 |
| Ash Wharf 010C | Guildford | -0.088 |
| Cobham & Downside 017D | Elmbridge | -0.079 |
| Tattenham Corner & Preston 005A | Reigate & Banstead | -0.077 |
| Walton South 004B | Elmbridge | -0.068 |
| Horley Central & South 018D | Reigate & Banstead | -0.061 |
| Godalming Central & Ockford 010A | Waverley | -0.018 |
Figure 27: Chart showing combined neighbourhood satisfaction scores for key neighbourhoods, Surrey, and England (Source: Community Insight Report, April 2023).
The Community Needs Index was developed to identify areas experiencing poor community and civic infrastructure, relative isolation, and low levels of participation in community life. The index was created by combining a series of 19 indicators, conceptualised under three domains: Civic Assets, Connectedness and Active and Engaged Community. A high score indicates that the area has high levels of need.
- Civic Assets: measures the presence of key community, civic, educational and cultural assets in a close proximity of the area. These include pubs, libraries, green space, community centres, swimming pools – facilities that provide things to do often, at no or little cost, which are important to how positive a community feels about its area.
- Connectedness: measures the connectivity to key services, digital infrastructure, isolation and strength of the local jobs market. It looks at whether residents have access to key services, such as health services, within a reasonable travel distance. It considers how good public transport and digital infrastructure are and how strong the local job market is.
- Active and Engaged Community: measures the levels of third sector civic and community activity and barriers to participation and engagement. It shows whether charities are active in the area, and whether people appear to be engaged in the broader civic life of their community.
The full Community Needs scores for Surrey’s key neighbourhoods are shown in Appendix 3.
Ashford North and Stanwell South (Spelthorne 002C) scores highest for Community Needs (124.2), meaning it has the highest level of need in terms of community and civic infrastructure, isolation, and participation in community life of Surrey’s key neighbourhoods. Godalming Central and Ockford (Waverley 010A) has the lowest Community Needs Score (10.8).
Table 18: Table showing Community Needs Scores for key neighbourhoods – ranked highest to lowest (Source: Community Insight Report, April 2023).
| Key Neighbourhood | District & Borough | Community Needs Score |
|---|---|---|
| Ashford North and Stanwell South 002C | Spelthorne | 124.2 |
| Stanwell North 001B | Spelthorne | 121.3 |
| Tattenham Corner & Preston 005A | Reigate & Banstead | 110.8 |
| Dorking South 011D | Mole Valley | 109.3 |
| Old Dean 004C | Surrey Heath | 105.7 |
| Horley Central & South 018D | Reigate & Banstead | 94.5 |
| Hooley, Merstham and Netherne 008A | Reigate & Banstead | 68.1 |
| Goldsworth Park 005B | Woking | 66.9 |
| Englefield Green West 002F | Runnymede | 63.6 |
| Walton North 008A | Elmbridge | 61.7 |
| Cobham & Downside 017D | Elmbridge | 56.9 |
| Court 007A | Epsom & Ewell | 53.9 |
| Chertsey St Anns 006D | Runnymede | 52.5 |
| Redhill West & Wray Common 010E | Reigate & Banstead | 47.7 |
| Westborough 012D | Guildford | 42.1 |
| Walton South 004B | Elmbridge | 40.5 |
| Ash Wharf 010C | Guildford | 38.4 |
| Bellfields & Slyfields 007C | Guildford | 31.4 |
| Canalside 004F | Woking | 31.31 |
| Farnham Heath End 002E | Waverley | 20.8 |
| Godalming Central & Ockford 010A | Waverley | 10.8 |
Figure 28: Chart showing Community Needs Scores for key neighbourhoods (Source: Community Insight Report, April 2023).
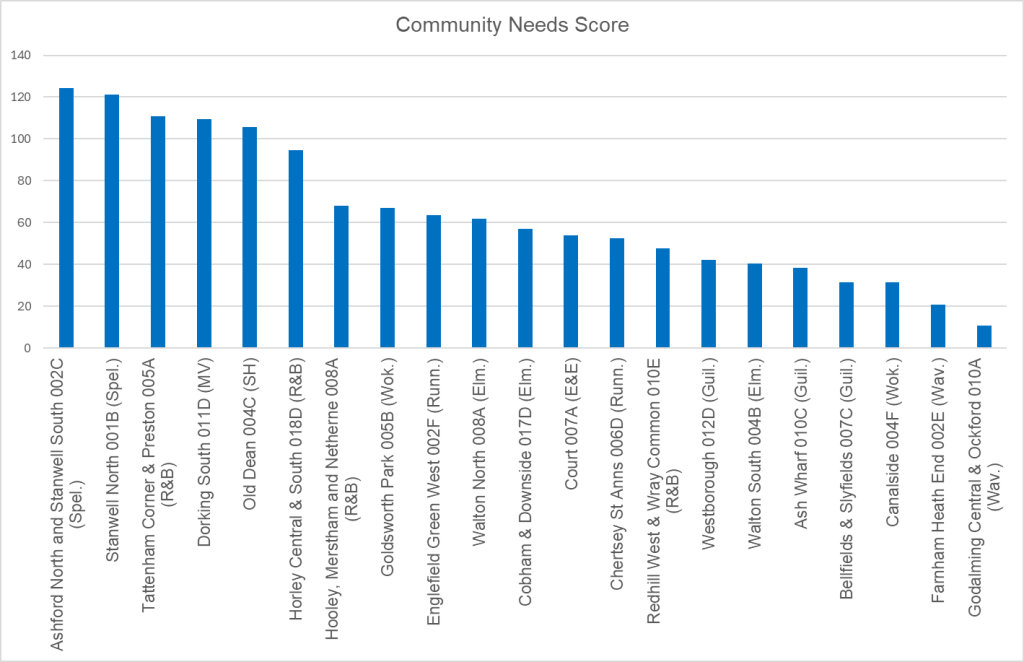
For comparison, the average Community Needs Score for Surrey is 44.8 which is lower than the national average for England of 68.4. Six of Surrey’s key neighbourhoods have a higher Community Needs Score than the average for England, and 14 have a higher score than the average for Surrey.
Table 19: Table showing Community Needs Scores for District & Boroughs – ranked highest to lowest (Source: Community Insight Report, April 2023).
| District & Borough | Community Needs Score |
|---|---|
| Spelthorne | 89.0 |
| Reigate & Banstead | 59.4 |
| Surrey Heath | 54.2 |
| Runnymede | 52.4 |
| Mole Valley | 43.9 |
| Woking | 43.0 |
| Elmbridge | 36.7 |
| Tandridge | 34.9 |
| Epsom & Ewell | 32.4 |
| Waverley | 30.1 |
| Guildford | 24.2 |
Figure 29: Chart showing Community Needs Scores for District & Boroughs (Source: Community Insight Report, April 2023).
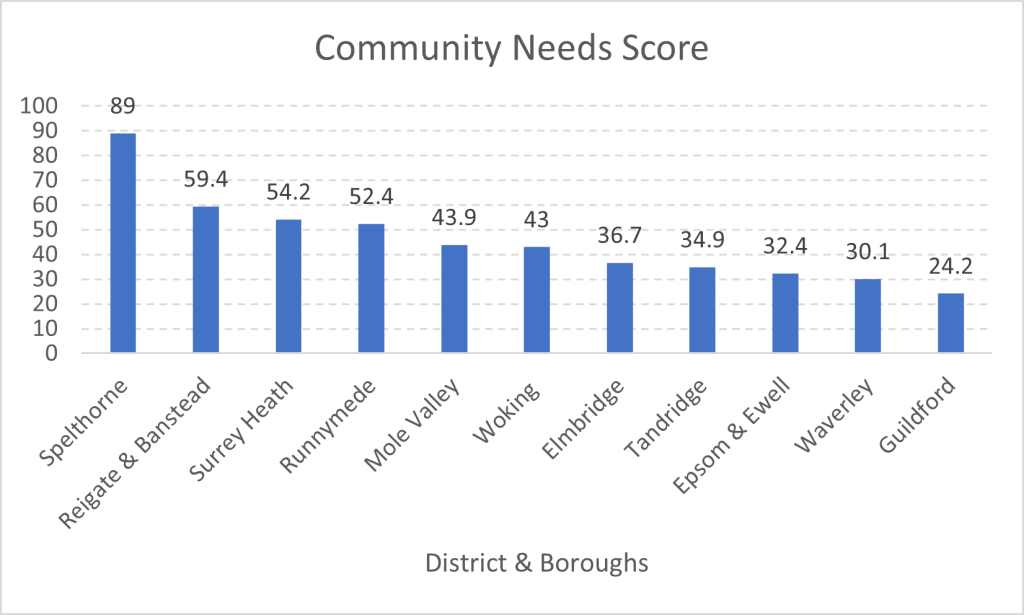
The District & Borough with the highest Community Needs Score is Spelthorne (89). Guildford has the lowest score (24.2). All District & Boroughs in Surrey, except for Spelthorne, have lower Community Needs Scores than the average for England (68.4).
Global and national LSI policies
Current global estimates by the World Health Organisation (WHO) suggest that 1 in 4 older adults experience social isolation and between 5 and 15 per cent of adolescents experience loneliness. Social isolation and loneliness do not just harm individuals, they also have a negative impact on entire communities and societies.
Research shows that safety, prosperity, and effective governance in communities and societies depend greatly on the quality of the social connections within its neighbourhoods, workplaces, and schools[47].
The WHO Commission on Social Connection (2024–2026) aims to see the issue recognised and resourced as a global public health priority. The Commission will propose a global agenda on social connection, working with high-level Commissioners to make the case for action, marshal support to scale up proven solutions and measure progress[48].
Social connectedness is critical for good health. People with limited social connectedness have poorer mental and physical health, including increased depression, and die earlier than those with strong social connectedness[49].
Personal relations, even those that we maintain for non-economic reasons, often give us access to information and provide us with social collateral for economic transactions – from buying a house to getting a job. The implication from this is that social connections are not only important because they affect our emotional well-being, but also because they affect our material well-being too[50].
The Department for Digital, Media, Culture & Sport’s A Connected Society: A Strategy for Tackling Loneliness strategy (DCMS, 2018) set out the government’s approach to tackling loneliness in England[51]. It set out to improve the evidence base for what causes loneliness, impact, and how to tackle it; to embed loneliness as a consideration across government policy; and to build a national conversation on loneliness and understand social connections as key to wellbeing.
The 4th annual progress report (2023) on the strategy cites research showing that some groups are disproportionately affected by loneliness, including young people and disabled people[52].
In 2021, the government convened the Tackling Loneliness Evidence Group to bring together experts and academics in the loneliness field. The Group published an evidence review in 2022 to provide non-specialists with an informed, expert overview of the evidence gaps that still need to be filled[53].
In 2022, the government also published qualitative mental health research that shows the relationship between loneliness and mental health is bidirectional and cyclical; so that mental health issues can lead to greater feelings of loneliness, while loneliness can also lead to a decline in mental health[54].
The Tackling Loneliness Evidence Review (2023) established that there are a range of official statistics on loneliness produced by the government, but little local level demographic data exists, meaning some users, including charitable organisations, are producing their own statistics to fill data gaps. This has informed the approach taken in the production of this JSNA chapter in Surrey.
The Review set out that while loneliness affects most people, chronic loneliness has been linked to poor physical health, mental health and poor personal wellbeing. Reported loneliness is higher for those who are or have:
- 16-24 years old
- female
- single or widowed
- living with a limiting mental health condition
- renters
- lower neighbourhood belonging
- lower local social trust.
Further steers offered by the Review to inform this JSNA include that it will be helpful to look at what driving factors can be changed, e.g. structural, physical spaces, policies etc, that offer maximum change. There is also the question of trying to answer ‘how do passing feelings of loneliness become chronic’, and knowing when loneliness becomes a problem for individuals.
The Tackling Loneliness Hub, funded by DCMS and delivered by Campaign to End Loneliness, is an online community for professionals working on loneliness, enabling members working across England to connect with others through events and workshops, share the latest research and insights on what works, and collaborate on new initiatives[55].
Surrey LSI policies
The JSNA chapters, including this one, inform the Surrey Health and Wellbeing Strategy (HWS) that was refreshed in 2022. This outlines the collective health priorities for all partners across Surrey and identifies specific groups of people who experience health inequalities[56].
The Strategy’s renewed focus is on a commitment to working in creative partnerships with communities to achieve the overarching aim of the Surrey Health & Wellbeing Board – to reduce health inequalities so no-one is left behind[57]. There is a particular focus on people who experience the poorest health outcomes (the ‘priority populations’), including those living in geographic areas that experience the poorest outcomes (the ‘key neighbourhoods’)[58].
The Strategy has adopted the following principles (‘the Four Cs’) for working with communities to guide this commitment across the system, which have informed the development of this JSNA chapter:
- Community capacity building: ‘Building trust and relationships’
- Co-designing: ‘Deciding together’
- Co-producing: ‘Delivering together’
- Community-led action: ‘Communities leading, with support when they need it’.
Priority two of the HWB Strategy is ‘Supporting people’s mental health and emotional well-being by preventing mental ill health and promoting emotional well-being’. This includes creating communities and social environments that tackle isolation and build good mental health. This JSNA chapter specifically relates to supporting priority two, outcome three: ‘Isolation is prevented and those that feel isolated are supported’.
The Surrey Heartlands ICS Joint Forward Plan 2023-2028 sets out how the county’s Integrated Care System will work together over the next five years to deliver on local strategies, including the Surrey HWB Strategy [59]. It states that ‘we will reduce health inequalities and support our priority populations to… prevent mental ill health and promote mental health and emotional well-being’. Similarly, ‘supporting people’s mental health and emotional well-being by preventing mental ill health and promoting emotional well-being’ is one of the strategic ambitions of the Surrey Heartlands’ Clinical Strategy 2024-29 [60].
‘Well-connected communities’ are one of four overarching objectives of Surrey’s fourth Local Transport Plan (LTP4), which sets out plans for transforming the county’s transport network from 2022 2032 [61]. It contains proposals which could have a positive bearing on tackling loneliness and social isolation – for example, redesigned neighbourhoods for easier and quicker access to shops, leisure facilities and essential local services [62]; reliable, safe, and affordable public transport [63]; better rural connections [64]; support for those with accessibility needs [65]; and improved health and wellbeing through safer routes to promote more active forms of travel [66].
In the recently updated JSNA chapter on Emotional and Mental Wellbeing in Surrey Adults (2023), social isolation in social care users in Surrey is shown to be comparable to the region and England, with over half of social care users reporting not having as much social contact as they would like [67]. In addition, less than a quarter of adult carers in Surrey reported having as much social contact as they would like, which is significantly worse than the regional and national reports on social contact. The highest levels of loneliness were reported in the Mole Valley (10.9%).
Table 20: Social isolation in adult carers
| Indicator | Period | Surrey | Region | England | Worst | Best |
|---|---|---|---|---|---|---|
| Adult social care users who have as much social contact as they would like 18+yrs | 2019/20 | 47.3% | 45.9% | 45.9% | 34.3% | 56.6% |
| Adult social care users who have as much social contact as they would like 65+yrs | 2019/20 | 43.7% | 42.9% | 43.4% | 30.4% | 53.8% |
| Adult carers who have as much social contact as they would like 18+yrs | 2018/19 | 22.4% | 31.4% | 32.5% | 11.7% | 45.7% |
| Adult carers who have as much social contact as they would like 65+yrs | 2018/19 | 24.2% | 32.7% | 34.5% | 11.1% | 50.9% |
The chapter’s recommendations relevant to loneliness and social isolation are 2.9: “Interventions to address social isolation and loneliness to be applied at scale with an explicit consideration of carers” and 3.7: “To develop mature, sustainable, and integrated social prescribing offer in Surrey linking residents to community offers”.
In a 2023 Healthwatch Surrey study, under their ‘Giving Carers a Voice Contract’, one of the three main support or benefits that are the most valuable to carers was ‘mental load and responsibility’”, including to counter isolation. The study captured 649 people’s views, and it concluded that carers will judge the support they are offered in terms of how much time, mental load and cost it reduces or adds to their lives[68].
A small scale, survey-based study in 2021 among regular Day Centre users in Surrey found that key drivers for most were meeting and chatting with friends, sharing activities, interacting with different kinds of people, and being out in the world. It concluded that ‘Day Centres play a vital role in preventing social isolation and enhancing mental health’[69].
The JSNA chapter, Children and Young People’s Emotional and Mental Health Strategy 2022-2027, reports that care leavers in Surrey (19%) were more likely to report they felt lonely ‘often/ always’ compared to peers (10%) in the general population[70]. ‘Often/always’ feeling lonely is associated with overall low well-being.
While it does not directly reference loneliness and social isolation, the recent JSNA chapter, ‘People with learning disabilities’ (2023), outlines what we know about the lives of people with learning disabilities of all ages in Surrey, their health outcomes and access including the experience of Covid, social care needs and provision, their living circumstances, education and employment and how much of a voice they have in their lives, services they use and their communities[71].
Local insights on priority populations
Loneliness can be experienced by anyone at any point in their life. For many people the experience will be transient. However, for people with key risk factors loneliness is more likely to become chronic and to have detrimental impact on health and wellbeing. We also know that experiences of loneliness and social isolation intersect with population characteristics and other determinants of health and wellbeing. It is necessary, therefore, to consider the needs of population groups in turn. This section draws on the insights from stakeholder engagement to identify key populations at risk of loneliness and social isolation in Surrey.
The stakeholder survey identified the six ‘priority populations’ who are considered most at risk of loneliness and social isolation. These are:
- Older people and people in care homes
- People with long term health conditions, disabilities, or sensory impairments
- Carers and young carers
- People with serious mental illness
- Adults with learning disabilities and/or autistic adults
- People experiencing homelessness.
Wider stakeholder engagement, and the insights of community-based wellbeing workers who support lonely and isolated residents, highlighted numerous population groups at risk of poorer health and wellbeing outcomes due to loneliness and social isolation. Some of these groups are a priority population within Surrey’s Health and Wellbeing Strategy but some are not:
- No friends or family network
- New parents
- Domestic abuse survivors
- Children & young people
- Students
- Bereaved
- LGBTQ+
- Retire, unemployed and economically inactive
- Farmers and agricultural workers
- Veterans
- Refugees and asylum seekers
- Men.
The loneliness and social isolation experiences of each of these populations are outlined in the next section.
Older people & people in care homes
Over 10 million people are currently aged 65 and over in the UK, which is 18 percent of the population. The number of people aged 65-79 is set to increase by thirty percent (to over 10 million) in the next 40 years, while the number of people aged 80 and over is set to double to over 6 million. This is the faster growing segment of the UK population[72].
The proportion of people aged 65 and over who feel they belong has fallen to below pre-pandemic levels[73]. Age UK predict that if loneliness in older people is not addressed, by 2026 two million people aged 50+ in England will often feel lonely[74]. This will adversely affect the health and wellbeing of those individuals. It will also have serious implications for health and care services. Older people living alone are 50% more likely to access emergency care services, and 40% more likely to have more than 12 GP appointments over a year[75]. Loneliness is also a risk factor for care home admission[76]. Tackling loneliness amongst older adults is therefore a way of enhancing personal wellbeing and delaying or reducing the demand for institutional care.
Figure 30 All the Lonely People: Loneliness in Later Life, Age UK September 2018.
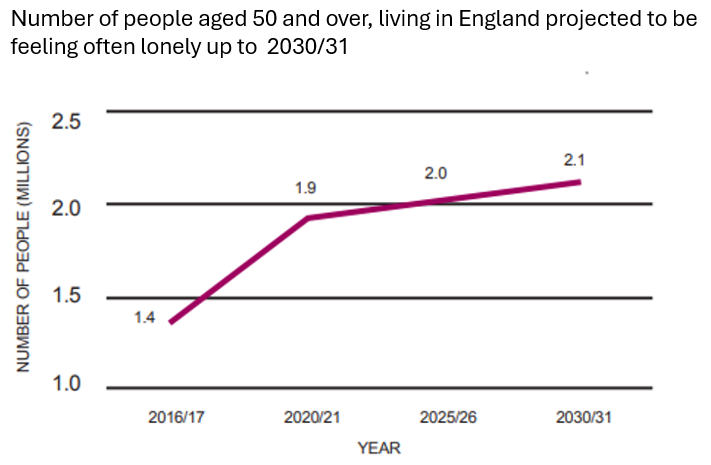
Older people are not a homogeneous group. Experiences of ageing and of age-related loneliness and social isolation are mediated by other characteristics including gender, ethnicity, sexuality, health, and socio-economic status. Those older people with Black Asian and Minority Ethnic backgrounds, for example, may be less likely to both feel satisfied with their local communities and feel they belong to their neighbourhoods than people with White backgrounds[77].
Age does not cause loneliness. Older people become lonely when they are unable to have relationships and social connections that provide purpose and meaning. This could be due to bereavement or a decline in health or mobility. Various risk factors increase the likelihood of older people experiencing loneliness and social isolation. These include:
- living alone
- poor health
- being aged 80+
- loss of friends
- having no access to a car/ never using public transport
- living in rented accommodation
- living on low income or on benefits as main income
- having no access to a telephone
- hearing and sight loss.
According to the Jo Cox Commission on Loneliness, eight million men (of all ages) in the UK feel lonely at least once a week. Nearly 3 million men report feeling lonely daily. However, older men may be less likely to report feeling lonely. One in ten men would not admit to feeling lonely[78]. Cultural ideals of masculinity may mean that men are less likely to report feeling lonely, but research also suggests that socially isolated older women may be more likely to experience loneliness than socially isolated older men[79]. Socially isolated older men are more likely than socially isolated older women to perceive their isolation as being ‘alone’ but ‘not lonely’[80]. Men show a greater association between loneliness and alcohol consumption. In contrast to older women, alcohol consumption for older men is not associated with increased social contact[81].
Research shows that the link between falls for people over the age of 60 and loneliness and social isolation is bidirectional. Loneliness, social isolation and living alone are significantly associated with falls in older people. Older people who are lonely and socially isolated lose their physical abilities when they are not supported to keep physically and socially active. Conversely, falls can lead to higher levels of loneliness and social isolation because older people who have experienced a fall tend to avoid physical and social activities[82]. Falls prevention programmes can be understood as not just a means of reducing costly hospital admissions, but also an opportunity to maintain mobility and existing social connections[83].
Technology can be both a barrier to social connection for older people and an enabler. In 2018, according to Age UK, 36 percent of people aged 65+ had lapsed in their use of the internet or had never been online[84]. The Covid-19 pandemic accelerated the use of digital connectivity for many older people. However, for those older people who continue to face barriers to digital technology, the acceleration of online platforms during Covid-19 lockdowns has created an even wider gulf between those digitally included and those digitally excluded. Digital exclusion is closely related to social isolation. The people most likely to be lonely are also the people least likely to be digitally literate[85].
Loneliness represents a potential risk factor for poor cognitive function within otherwise healthy older people. People experiencing loneliness are at heightened risk of developing dementia-related disorders compared to non-lonely individuals, possibly by as much as 49-60%[86]. Social isolation may also occur because of dementia[87]. However, further research and longitudinal studies are needed to draw conclusive links between loneliness, social isolation and dementia[88].
In Surrey one fifth of the population is aged 65 and over (20.1%) and of those 16.2% are aged 85 and over. These figures are set to increase by 2030.
Figure 31 compares the Surrey population in 2024 and 2030. Source: 2018-based subnational population projections, 2024, 2030.
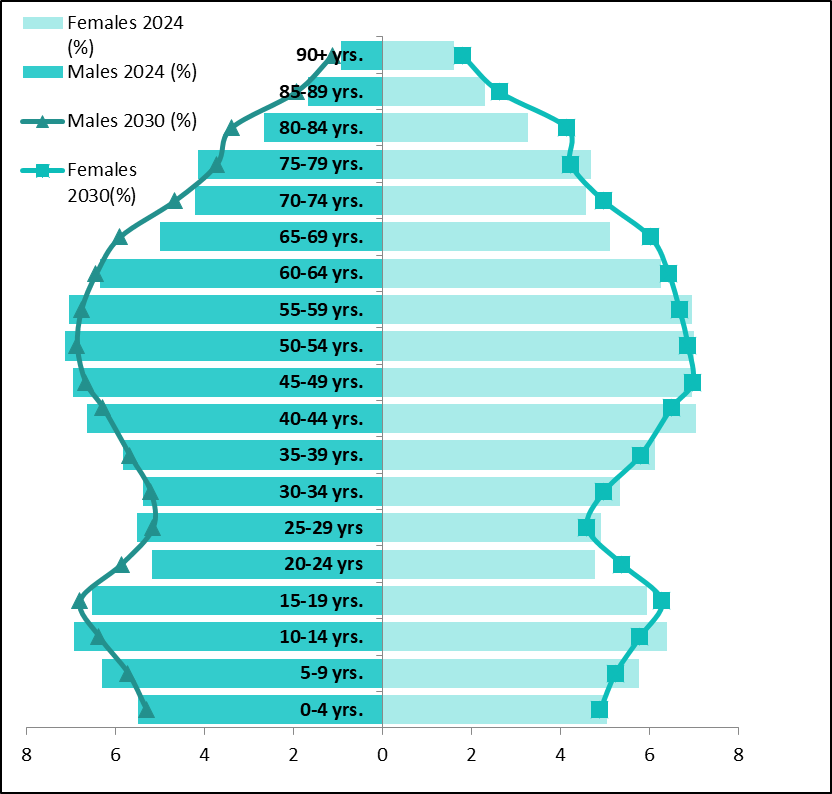
At District & Borough level, Mole Valley, Waverley, Tandridge and Surrey Heath are projected to have the highest numbers of residents aged 65-84 by 2038.
Figure 32: Source: 2018-based subnational population projections, 2023 to 2030.
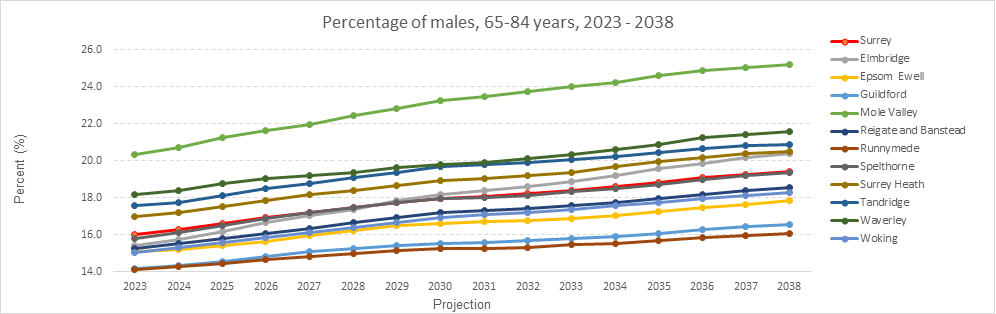
Figure 33: Source: 2018-based subnational population projections, 2023, 2030.
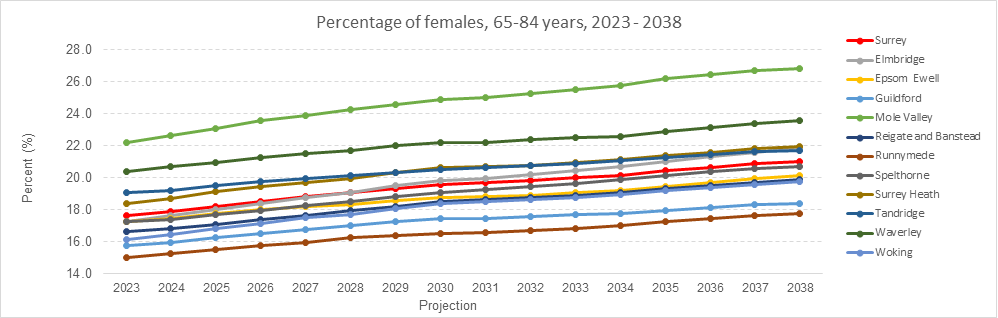
Relative risk of loneliness for older people can be measured according to four risk factors:
- Marital status
- Self-reported health status
- Age
- Household size.
Age UK’s loneliness index based on 2011 Census data has been used to create heat maps of loneliness risk for people aged 65+ at LSOA level in Surrey. Mapping loneliness hot spots for older people can help identify and target those who are experiencing loneliness in local populations. Twelve wards are ‘very high risk’ areas for loneliness in residents aged 65 and over.
Table 21: Surrey wards in the first quintile nationally for risk of loneliness aged 65+. 1 = highest risk, 32,844 = lowest risk. (N.B. Loneliness Heat Maps are based on 2011 Census Data.) * entries have updated ward names.
| District & Borough | LSOA | Ward | Rank in England |
|---|---|---|---|
| Woking | 004F | Canalside | 1, 019 |
| Reigate & Banstead | 008A | Hooley, Merstham & Netherne | 1, 068 |
| Reigate & Banstead | 005A | Tattenham Corner & Preston | 2, 779 |
| Spelthorne | 007B | Staines South | 3, 051 |
| Waverley | 005E | Godalming Farncombe & Catteshall | 3, 340 |
| Epsom & Ewell | 007A | Court | 4, 065 |
| Epsom & Ewell | 008B | Town | 4, 888 |
| Elmbridge | 003D | Molesey West* | 5,321 |
| Runnymede | 003A | Egham Hythe* | 5, 499 |
| Runnymede | 009A | Addlestone South | 5, 942 |
| Waverley | 003B | Farnham Castle | 5, 969 |
| Mole Valley | 009C | Dorking North* | 6, 019 |
Loneliness heat maps should be used alongside local knowledge and an understanding of local neighbourhoods to improve the allocation of resources to reduce age-related loneliness across a geographic area and help understand whether existing services are reaching areas of need.
Figure 34: Source: SAPE population (65 plus), 2022, Connect to Support Surrey – 65 and over (search date March 2024)
Table 22: Connect to Support services for older people
| Area Name | Number of Connect Support 65 years and over | Online/ telephone Service | Ramblers and guided walks | Total Number of Services |
|---|---|---|---|---|
| Surrey | 142 | 4 | 6 | 146 |
| Elmbridge | 14 | 0 | 0 | 14 |
| Epsom & Ewell | 7 | 1 | 0 | 8 |
| Guildford | 12 | 2 | 0 | 14 |
| Mole Valley | 2 | 0 | 0 | 2 |
| Reigate & Banstead | 21 | 0 | 0 | 21 |
| Runnymede | 5 | 0 | 0 | 5 |
| Spelthorne | 29 | 0 | 0 | 29 |
| Surrey Heath | 7 | 0 | 0 | 7 |
| Tandridge | 17 | 0 | 0 | 17 |
| Waverley | 16 | 1 | 0 | 17 |
| Woking | 12 | 0 | 0 | 12 |
| Outside Surrey | 21 | 0 | 0 | 21 |
| Total | 163 | 4 | 6 | 167 |
8,668 people live in care homes in Surrey[89]. Evidence on loneliness within care homes is limited, though one study suggests that severe loneliness among older people in care homes could be double that of community populations[90]. Whilst social isolation and loneliness can be associated with living in a care home setting, they can also be a risk factor for entering care. A 2018 study of English Longitudinal Study of Ageing data found loneliness increases the risk of admission into care homes. Researchers concluded that by tackling loneliness, older adults may also benefit from delaying or reducing the demand for institutional care[91].
Applying an age-friendly lens to place-based policies can help to combat loneliness[92].
Age-friendly Communities
The number of Age-friendly Communities – places that commit to enabling people to live a good later life – has more than doubled in the UK since 2020[93].
An Age-friendly Community is a place that enables people to age well and live a good later life. Somewhere that people can stay living in their homes, participate in the activities they value, and contribute to their communities, for as long as possible.
The UK Network of Age-friendly Communities is a growing movement, with over 75 places across the country committed to making their community a better place to age in. Over 26 million people are living in an Age-friendly Community, including places like Greater Manchester and Cardiff. The Centre for Ageing Better works with the Network to provide guidance, connect places and offer support to member communities as they work towards making their services and infrastructure more age friendly.
View a map of Age-friendly Communities here.
The UK Network is part of a global movement led by the World Health Organisation, affiliated to the Global Network of Age-friendly Cities and Communities.
UK Network of Age-friendly Communities | Centre for Ageing Better (ageing-better.org.uk).
Dementia Aware Banstead
The ‘Dementia Aware Banstead’ initiative is helping to raise awareness of dementia within the area and help local retailers and community organisations to understand how they can help towards making the high street more dementia friendly.
The initiative is a collaborative effort between Surrey County Council, Reigate and Banstead Borough Council, the Banstead Primary Care Network and local partner organisations and residents.
The initiative has been informed by Banstead residents living with dementia and their carers.
‘The “Intergenerational Approach” is a deliberate and thoughtful strategy that harnesses the connections between and among people across the life course. It recognises the value of diverse experiences and fosters meaningful interactions that transcend age boundaries. Intergenerational power works to link sectors and professionals, as well as people, to ensure holistic approaches to tackle loneliness are at the forefront of agendas.
Adopting an Intergenerational paradigm can actively challenge and break down stereotypes and prejudices that tend to be associated with age. By showcasing that people of different generations can relate, connect, and learn from one another, these interactions become powerful catalysts for promoting inclusivity. Building mutual exchange of care and companionship can go a long way in nurturing a profound sense of unity and belonging, thus dismantling the barriers of isolation. It goes beyond promoting reintegration into society; but, highlighting the intrinsic worth of every individual, regardless of their age.’ Unravelling The Threads of Loneliness: An Intergenerational Approach (intergenerationalengland.org)
Intergenerational Music Making brings together care home residents and school children in their ‘Together with Music’ programme in Surrey Downs. Through music, intergenerational connections are forged so that older people in care homes, and the visiting children, experience greater community cohesion and a sense of shared purpose.
Guildford Town Centre Chaplaincy’s Community Angels offer befriending to adults of all ages in Guildford who are experiencing loneliness and social isolation. The service provides 6 months of weekly one-to-one, face-to-face befriending with a trained and DBS checked befriending volunteer. This might take place in someone’s home, or they may be supported to get out and about in their community. Support is personalised so may range from chatting over a cup of tea to going for walks, trying a new activity, or accessing other types of help. Community Angels empowers people to make decisions and take actions to improve their wellbeing.
Last year, Community Angels’ 42 volunteers made 736 befriending visits over 2,276 volunteering hours.
Re-Engage works with the UK’s ‘oldest old’ to understand their priorities, challenge perceptions of ageing, increase social connection for the over 75s, and reduce loneliness and social isolation. Its monthly ‘tea parties’ – hosted in the homes of volunteers in the Guildford area and supported by a team of volunteer drivers – provide people over the age of 75 who are lonely or isolated the opportunity to share companionship over a cup of tea and cake.
People with long term health conditions, disabilities, or sensory impairment
Adults with disabilities are more likely to experience loneliness, become lonely and remain lonely over time than their peers. Analysis of data from the UK’s annual household panel study, Understanding Society, showed that the prevalence of persistent loneliness was 46% for respondents with disabilities compared with 22% for respondents without disabilities[94].
In a cross-section study of the English Community Life survey, researchers found adults aged 16-64 with disability in England are 51% more likely to be socially isolated, 24.6% more likely to report low levels of perceived social support and 43.8% more likely to be lonely than adults without disability’[95]. Loneliness (and other indicators of low social connectedness) was higher among people with disabilities who are experiencing other risk factors as well, such as being economically inactive, living in rented or other accommodation, living alone and with low levels of access to environmental assets.
For people with sensory impairments, the positive association with loneliness and social isolation remains. Analysis of the English Longitudinal Study on Ageing showed that hearing impairment is related to higher loneliness and social isolation scores, which are linked to cognitive decline[96].
For people living with cancer in the UK, 73% report having emotional concerns and of those, 28% report experiencing loneliness and social isolation.
How many people living with cancer are concerned with emotional needs? Overall, 73% of people living with cancer report a type of emotional concern.
A breakdown of specific types of emotional needs, and proportion of people living with cancer reported being concerned about them are shown below:
Figure 35: People Living with Cancer Research Survey, 2020.
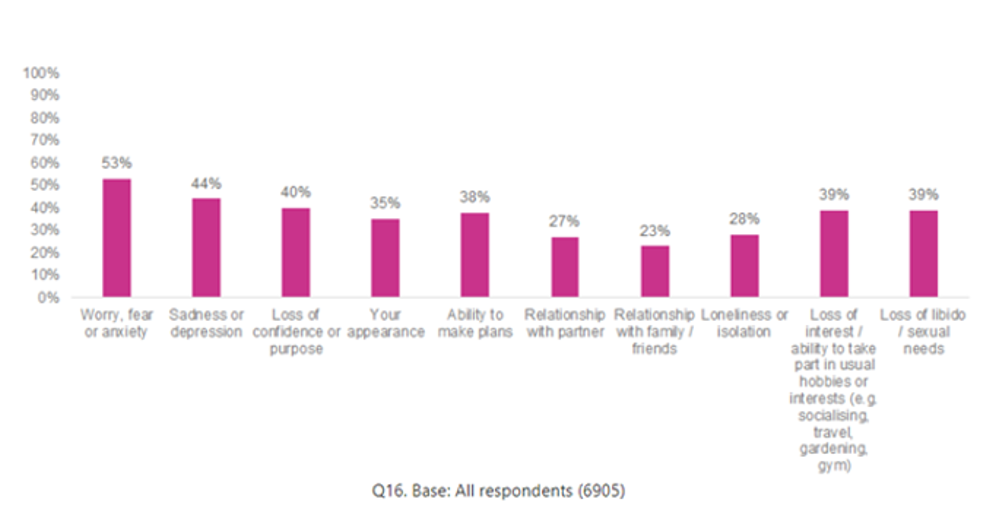
Social connection and a reduction in loneliness for people with long-term health conditions can be achieved through applying a ‘social cure’ approach to interventions (where the belonging to social groups that members identify with enhances health/wellbeing)[97]. Wakefield et al. (2022) studied the impact of social prescribing over time on patients with long-term health conditions who felt isolated, lonely, and/or anxious. They found that individuals on a social prescribing pathway increased their social group memberships which enhanced their quality of life.
The 2021 Census data shows just under a quarter of Surrey residents (21.3%) were classified as having a disability under the Equality Act or had a long term physical or mental health condition (but day-to-day activities were not limited).
Figure 36: Non-age-standardised proportion of Surrey residents with a disability, 2021. (Source: 2021 Census: Disability | Surrey-i (surreyi.gov.uk))
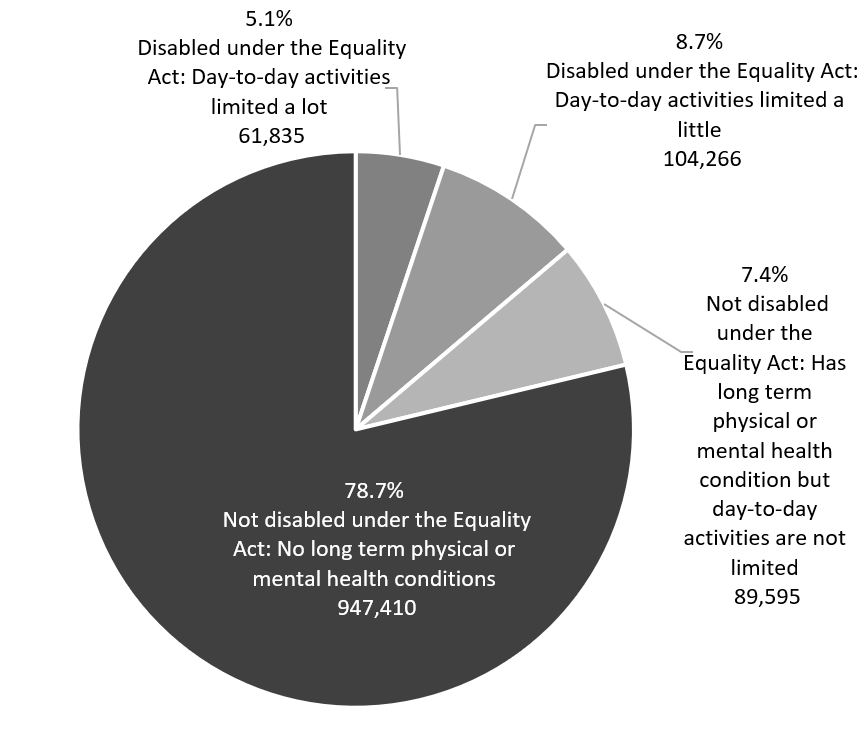
Data from the GP Patient Survey shows percentage of patients self-reporting a long-term physical or mental health condition, disabilities, or illnesses by age.
Figure 37: GP Patient Survey data on percentage of patients reporting a long term physical or mental health condition, disability or illness by ICB and age group
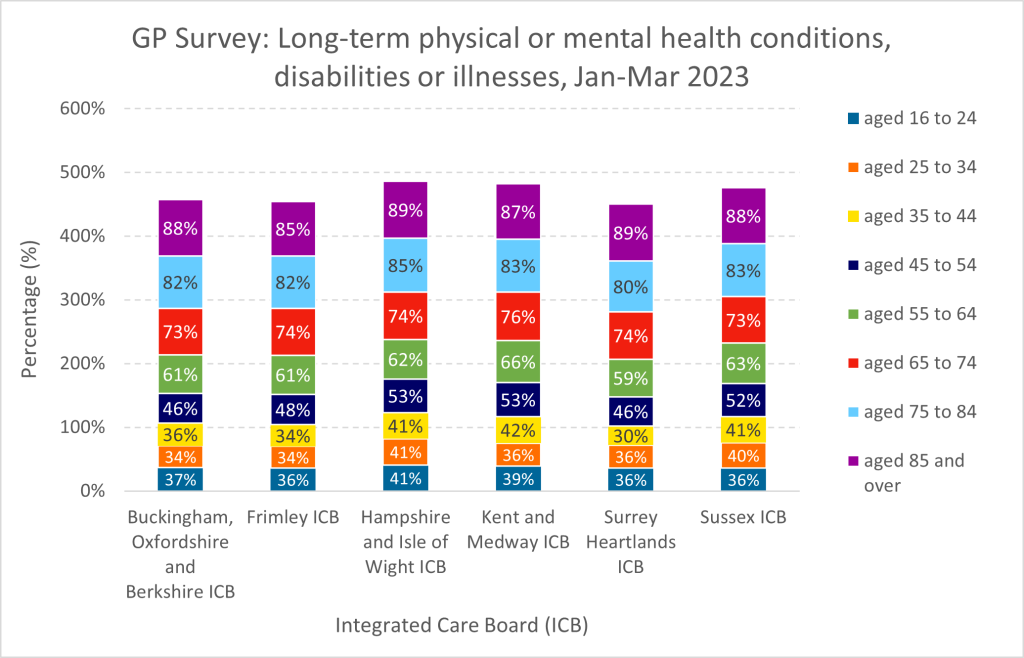
Table 23: Table of GP Patient Survey data on percentage of patients reporting a long term physical or mental health condition, disability or illness by ICB and age group
| ICB | Aged 16-24 | Aged 25-34 |
Aged 35-44 |
Aged 45-54 | Aged 55-64 |
Aged 65-74 |
Aged 75-84 |
Aged 85+ |
|---|---|---|---|---|---|---|---|---|
| Buckinghamshire, Oxfordshire, and Berkshire ICB | 37% | 34% | 36% | 46% | 61% | 73% | 82% | 88% |
| Frimley ICB | 36% | 34% | 34% | 48% | 61% | 74% | 82% | 85% |
| Hampshire and Isle of Wight ICB | 41% | 41% | 41% | 53% | 62% | 74% | 85% | 89% |
| Kent and Medway ICB | 39% | 36% | 42% | 53% | 66% | 76% | 83% | 87% |
| Surrey Heartlands ICB | 36% | 36% | 30% | 46% | 59% | 74% | 80% | 89% |
| Sussex ICB | 36% | 40% | 41% | 52% | 63% | 73% | 83% | 88% |
In Surrey, respondents to the Surrey Loneliness and Social Isolation Stakeholder Survey ranked people with long-term health conditions, disabilities, or sensory impairments as one of the top three groups most at risk of loneliness and social isolation[98].
‘You can’t do everything on Zoom.’
The Surrey Coalition of Disabled People’s weekly virtual café is an informal place for people to chat and connect with others. Members of the group shared their experiences and views with the JSNA on loneliness, social isolation, and how good social connection can be achieved in Surrey.
Although the online meet up is popular and well-received, group members felt that getting out of the house is also important. Having access to the right support and information in the right format is a key part of social connection. Information leaflets at GP practices, online resources such as accessible wheelchair maps, and virtual spaces were listed as helpful ways to keep up to date.
‘Getting out and about is not that easy if you can’t get in contact with organisations,’ says one member. ‘Some bus companies have an SMS contact so you can confidently go somewhere. We need that across the whole of Surrey because getting out to places is important to addressing loneliness. You can’t do everything on Zoom.’
Transport is a widely acknowledged barrier for people to get out and about. Where there is transport available, it isn’t always clear whether wheelchairs are accepted. This stress was exacerbated for individuals who would be traveling on their own, with some deciding not to leave the house:
‘If you’re a single person and you want to get out with a wheelchair and you don’t get help from drivers, that stops you going out. It’s sad because it’s not for the not wanting to get out. It’s about not being able to access these things.’
The lack of availability of accessible public transport in the evenings was seen as creating inequality of access to social opportunities:
‘We don’t go to bed early just because we have disabilities or health conditions. We like to get out and about at night too, but we can’t because there’s no way we can get back. It’s not right.’
When the group were supported to get out into the community, they reported feeling like a contributing member of society, having fun, and being enabled to take part in meaningful activities. To ensure that more spaces and places are accessible, the group strongly felt that including people with lived experience in the design and decision making was the key to success.
‘All the codesign work that we do is worthwhile because it makes all of us feel valued. It also makes sure money is used in a wise way because it is following the expertise of people who live with these challenges on a day-to-day basis.’
Surrey Coalition’s Get More Active project encourages Disabled People or those living with a long term health condition to take part in physical activities.
Tech Angels provides devices, digital literacy training and confidence-boosting support to people in Surrey who are most at risk of digital exclusion. This includes people who are Disabled, people with a long-term health condition, people with mental ill-health, carers, older people, and people from Black and minoritised ethnic groups.
As part of its mission to tackle the loneliness and isolation caused by digital exclusion, Surrey Coalition offers virtual social activities every weekday.
Carers and young carers
6.5 million people in the UK are caring for a loved one who is older, disabled, or seriously ill[99]. Groups that are most likely to be carers include women in their 50s, older people who already face disadvantage because of where they live or disability, and older women from minority ethnic communities[100].
Carers UK conducted a State of Caring survey in 2017 of 7,286 carers and former carers. This survey revealed that 81% of carers have felt lonely or socially isolated because of their caring role[101]. This figure increases to 89% for young carers who are under 24 years old, and to 91% for carers who are caring for a disabled child. The main reasons for this feeling of loneliness or being socially isolated include a lack of time to spend on social activities, not being able to afford activities, difficulty getting out of the house as often, and not feeling comfortable talking about caring with their friends.
The 2021 report on carers and loneliness by Carers UK, The world shrinks, further highlights some of the supports that carers surveyed say would help them stop feeling lonely. These include regular breaks from their caring role, more understanding from society and the workplace, being in touch with other carers, taking part in education, feeling able to talk to family and friends, being able to take part in and afford leisure and social activities. Restrictions on Carers Allowance may act as a disincentive for carers to juggle their caring responsibilities with paid employment, compounding carers’ experiences of loneliness and social isolation.
The National Institute for Health and Care Research conducted a study of carers of people with mild to moderate dementia. They found that almost two-thirds of these carers reported being lonely, and the factors associated with higher levels of loneliness were social isolation, stress of the carer, poor wellbeing, and the quality of the carer’s relationship with the person with dementia[102].
The Surrey Health and Wellbeing Strategy Score Card (June 2024) published data on adult carers (aged 18+) who have as much social contact as they would like. Surrey has generally performed below the national average on this survey-based measure, although Surrey has gone against the continued downward trend seen regionally and nationally to be slightly above the national average in 2021-22 (this difference is reported as being not statistically significant). Please see the data below.
Figure 38 Adult carers with enough social contact, England, South East, and Surrey. Health and Wellbeing Strategy Scorecard.
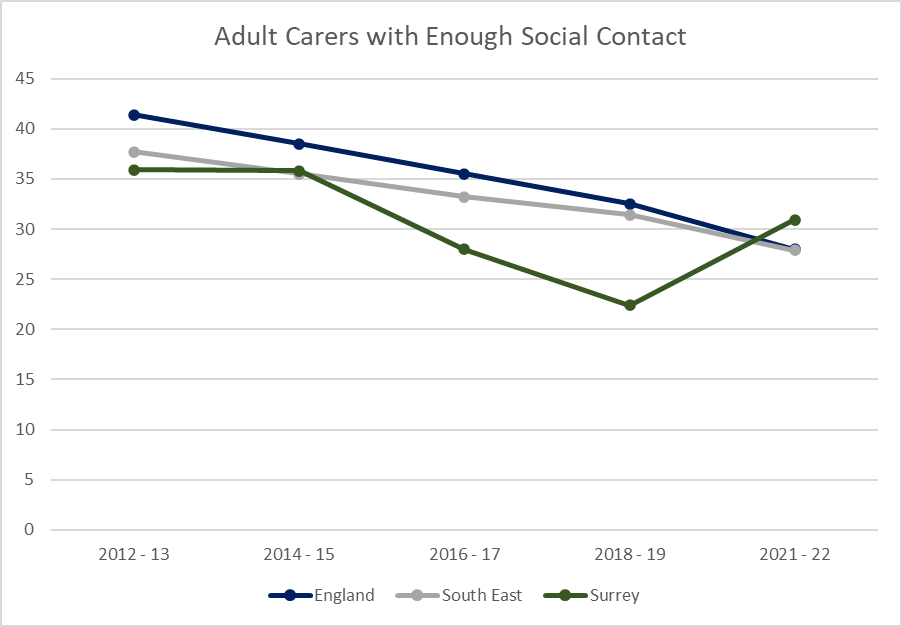

One in five young people in the UK are categorised as young carers who are under the age of 18 and care for a family member, relative or friend with a long-term condition, disability, or problem with alcohol and/or drugs[103]. Action for Carers Surrey finds that there are at least 14,000 young carers in our county[104].
Barnardo’s completed a study on young carers who experience loneliness and social isolation[105]. The study found that young carers had some common needs when accessing support services which fell into the following categories: mental health and emotional wellbeing, lack of respite and time away from home, and parental and family needs. Based on their analysis of cases, the report proposes seven best practices to support young carers with loneliness and social isolation. These are outlined in the table below.
Seven key good practice principles to support young carers to address loneliness and social isolation:
Figure 39 Barnardo’s (2021) Seven Good Practice Principles, See Hear Respond, Supporting Young Carers with Loneliness and Social Isolation.
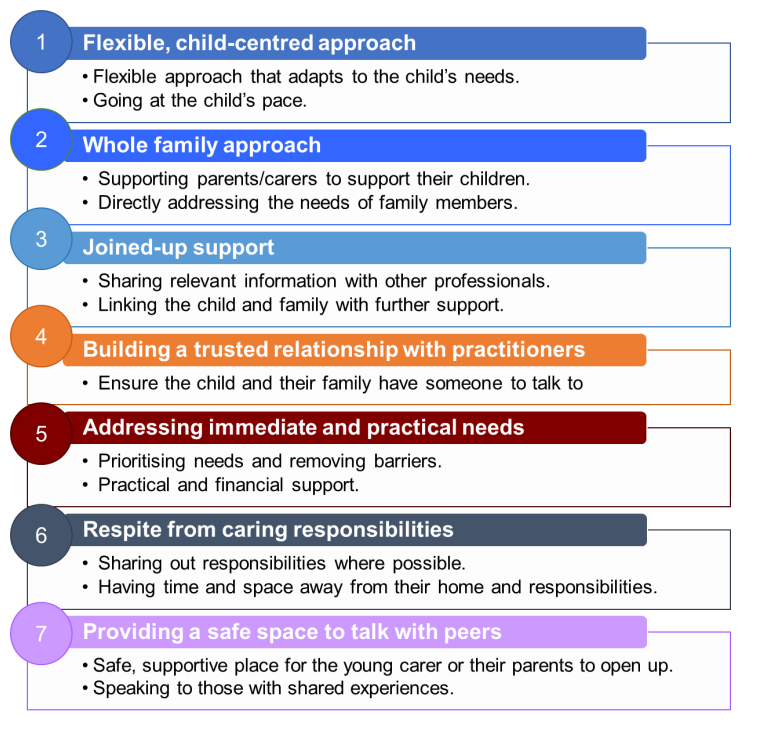
People with serious mental illness
Serious mental illness (SMI) refers to mental health problems so significant, they impact a person’s functional ability as well as their ability to work, attend education or in other ways achieve their potential. The SMI register includes patients with a diagnosis of schizophrenia, bipolar affective disorder and other psychoses, and major depressive disorder. Long term mental illness, where mental ill health lasts longer than 12 months, also limits people’s functional ability to perform daily activities such as going to work, forming relationships, or completing household tasks[106].
People living with serious mental illness are more likely to experience loneliness than people who do not have serious mental illness. The subjective experience of loneliness and perception of social isolation impacts a person’s self-rated mental well-being and the frequency of bothersome symptoms that accompany their SMI[107]. In a 2022 UK-based study, people with a diagnosis of psychosis, family caregivers, and mental health professionals participated in focus groups and interviews to share insights on social isolation and community integration of people with psychosis. Several themes from this study emerged, highlighting potential barriers and enablers to social integration[108]:
- Service pressure and hospitalisation – Closures of mental health services and centres and lengthy hospital stays without contact from others.
- Impact of symptoms – Symptoms included anxiety, exhaustion, and paranoia.
- Stigma – Fear of stigma and a need of public understanding of mental illness.
- Communities Promoting Agency and Independence from Services – Participants felt that integration into the community is the best way to recover and live with mental illness; This means having opportunities for meaningful engagement with a wide range of people, not just those within the mental health system.
In 2020/21, 9,343 (0.73%) people in Surrey had been diagnosed with SMI[109]. Data from Surrey Heartlands shows that 55% of people with SMI are between the ages of 40 and 69[110]. In the 2022 GP Patient Survey (GPPS), of those respondents registered with a GP in NHS Surrey Heartlands Integrated Care System, 9.1% reported having a long-term mental health condition[111].
Addressing the risk factors will be important to deliver Surrey’s Suicide Prevention Strategy, 2023-26[112]. This provides an opportunity for effective early intervention, as well as providing appropriate, tailored support for those experiencing suicidal thoughts or feelings. Many risk factors are common across the different individuals, groups and communities. Therefore, actions to address these risk factors are likely to prevent suicides at a population level with potential benefits for some groups.
There are four population-based risks that have been identified:
- Economy
- Alcohol
- Social isolation and loneliness
- Mental health
Current suicide prevention work in Surrey includes sharing common risk factors with commissioners, strategic leads, and service providers, and delivering campaigns and targeted messages that address common risk factors linked to suicide. The Strategy identifies that we need to do more on continuing to gather evidence and intelligence to understand common risk factors and develop evidence based early intervention and tailored support.
Following national policy changes, a ‘Draft Surrey Suicide Prevention Strategy 2024- 2027’ is being developed over summer 2024. Loneliness and social isolation are cited as a proposed action area under more ‘tailored support high risk groups and circumstances’:
‘Loneliness and isolation can affect anyone at any point in their lives. Nationally, loneliness and isolation have been seen as a risk factor to suicide. The lack of support and social connectedness have left people isolated’.
A key population-based action proposed is:
‘Promote connectedness and building social capital together by decreasing isolation, encouraging adaptive coping behaviours, increasing belongingness and to help build resilience in the face of adversity. Engage with wider community initiatives to demonstrate the contribution to this agenda’.
In 2021, Time to Change Surrey ran a survey to gather the experiences and insights from people with experience of mental health problems and any stigma or discrimination they may have faced. 72% of respondents indicated that they had experienced stigma. Those respondents selected where they had experienced stigma, highlighting that family, colleagues, and friends were the top three sources. The results of this question are below.
Figure 40: Time to Change Surrey survey, 2021, Where have you experienced stigma/discrimination? (n=90)
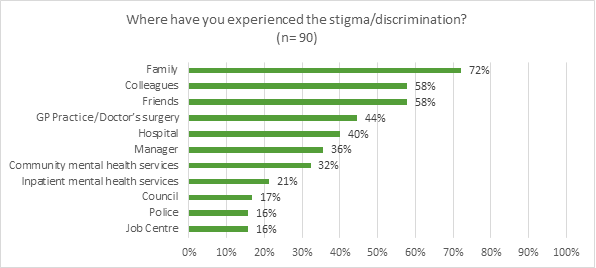
Reinforcing the research findings in national studies, the Surrey survey also finds that stigma and discrimination resulted in 78% of respondents withdrawing from others/their community and isolating socially.
Adults with learning disabilities and/or autistic adults
Adults with learning disabilities and/or autistic adults are at risk of loneliness and social isolation. This risk is exacerbated by the poorer mental and physical health outcomes experienced by these groups as compared to people without learning disabilities and/or autism[113].
There are additional barriers that adults with learning disabilities and/or autistic adults face when trying to form relationships, particularly romantic ones. The National Institute for Health and Care Research (2021) found barriers to forming romantic relationships for people with learning disabilities included a lack of accessibility in mainstream dating agencies, fewer opportunities for social events, lack of finances, inability to have a partner stay over for people in residential housing, and a general lack of autonomy and privacy within social life[114].
The estimated number of adults in Surrey aged 18+ with a learning disability is expected to increase by around 4.5% over time from 21,980 in 2023 to 22,971 in 2040 The estimated number of autistic people in Surrey aged 18+ is expected to increase by 5.2% from 2023 to 2040 (9,661)[115].
Creating environments that are welcoming and accessible to autistic people and people with learning disabilities can support social inclusion and opportunities to develop connections with others. Integrated approaches to developing communities can be seen in initiatives such as Autism Friendly Surrey: Autism Friendly Surrey – Surrey County Council (surreycc.gov.uk).
The Include Choir in Epsom, Reigate and Redhill provides inclusive in-person and online social and musical opportunities for people with communication needs, learning disabilities and autism. Through practice and training in Makaton signing and other inclusive communication best practise, Include Choir builds confidence in people with communication and learning needs, and increases wellbeing in people with communication and learning needs. The development of inclusive communication skills creates more inclusive communities where everyone can flourish.
Figures 41 and 42 map Surrey support services and social activities for people with learning disabilities and/or neurodiversity with further information available at Connect to Support Surrey.
Figure 41: Source: SAPE population, 2020, Connect to Support Surrey – Learning Disabilities (Search date March 2024).
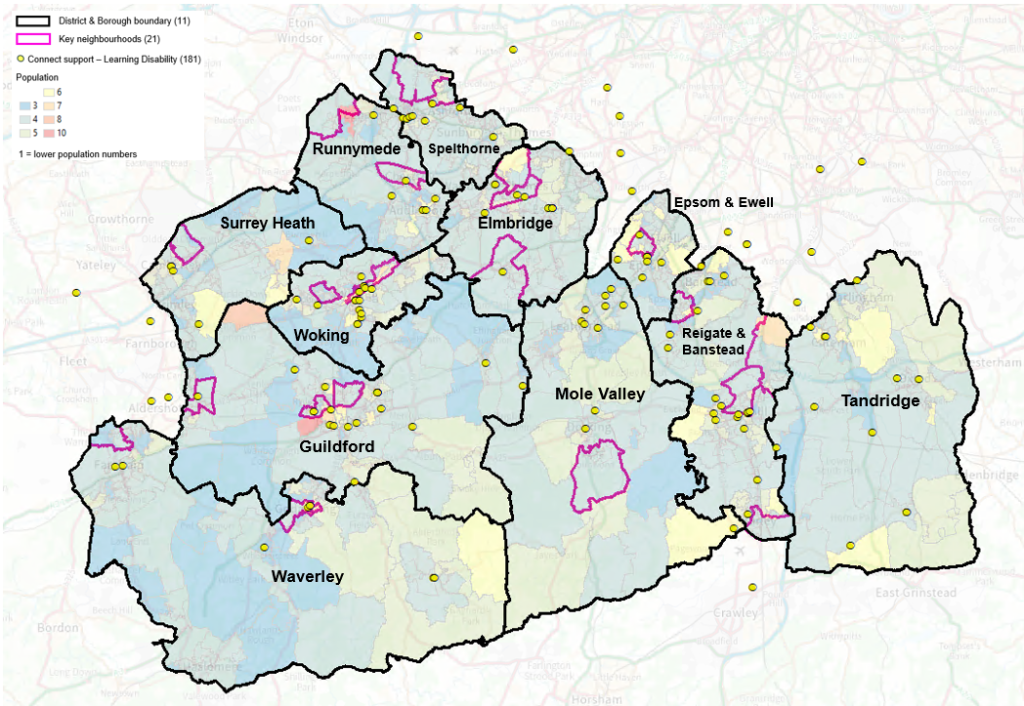
Table 24: Connect to Support services for those with Learning Disabilities
| Area Name | Number of Connect Support Learning Disability | Online/ telephone service | Total Number of Services |
|---|---|---|---|
| Surrey | 139 | 5 | 144 |
| Elmbridge | 11 | 0 | 11 |
| Epsom & Ewell | 8 | 1 | 9 |
| Guildford | 22 | 1 | 23 |
| Mole Valley | 12 | 0 | 12 |
| Reigate & Banstead | 20 | 0 | 20 |
| Runnymede | 7 | 0 | 7 |
| Spelthorne | 10 | 0 | 10 |
| Surrey Heath | 5 | 0 | 5 |
| Tandridge | 9 | 0 | 9 |
| Waverley | 8 | 0 | 8 |
| Woking | 27 | 3 | 30 |
| Outside Surrey | 19 | 0 | 19 |
| Total | 158 | 5 | 163 |
Figure 42: Source: SAPE population, 2020, Connect to Support Surrey – Neurodiversity (search date March 2024).
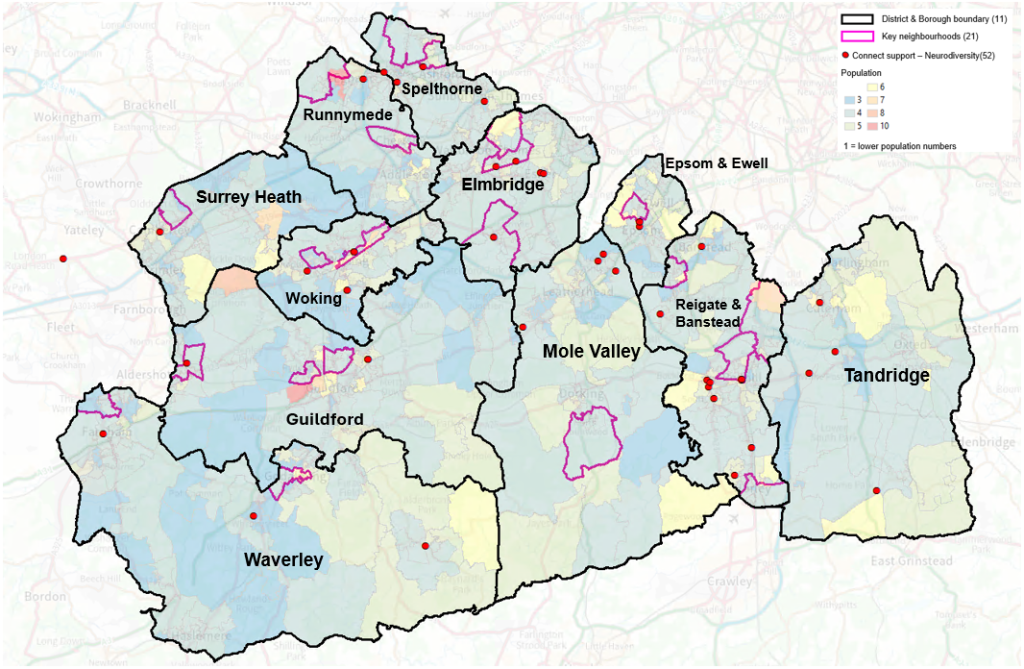
Table 25: Connect to Support services for Neurodiversity
| Area Name | Number of Connect Support Neurodiversity | Online/ telephone service | Total Number of Services |
|---|---|---|---|
| Surrey | 46 | 2 | 48 |
| Elmbridge | 5 | 0 | 5 |
| Epsom & Ewell | 3 | 1 | 4 |
| Guildford | 3 | 1 | 4 |
| Mole Valley | 4 | 0 | 4 |
| Reigate & Banstead | 11 | 0 | 11 |
| Runnymede | 1 | 0 | 1 |
| Spelthorne | 4 | 0 | 4 |
| Surrey Heath | 1 | 0 | 1 |
| Tandridge | 4 | 0 | 4 |
| Waverley | 3 | 0 | 3 |
| Woking | 7 | 0 | 7 |
| Outside Surrey | 2 | 0 | 2 |
| Total | 48 | 2 | 50 |
People experiencing homelessness
Housing is a wider determinant of health, and the experience of homelessness is associated with poor physical and mental health. The challenges faced by people experiencing homelessness increase the risk of loneliness and/or social isolation. This rise in loneliness can persist after the experience of homelessness. Rates of loneliness are elevated for people who have had a history of homelessness, indicating that this impacts on longer-term health and wellbeing outcomes as well as those during the experienced period of homelessness[116].
Relationship breakdown is a common precedent to experiences of homelessness. Homelessness is also stigmatised in society which increases challenges in both creating and maintaining connection. People experiencing homelessness have been found to withdraw from potential social support because of this stigma[117].
Keeping in contact with friends from the past (prior to becoming homeless) has been shown to improve mental health and the feeling of social inclusion, even when that contact is done virtually. Support workers also have a key role to play for people experiencing homelessness. Where there is perceived emotional support from a support worker, there is also better mental health[118].
Surrey data on homelessness, households threatened with homelessness, and rough sleepers can be found in the JSNA Housing and Related Support.
Local insights on other high-risk populations
No Friends or Family Network
According to the OECD, 93.2% of people in the UK report having friends or relatives they can count on.
Figure 43: https://ourworldindata.org/social-connections-and-loneliness
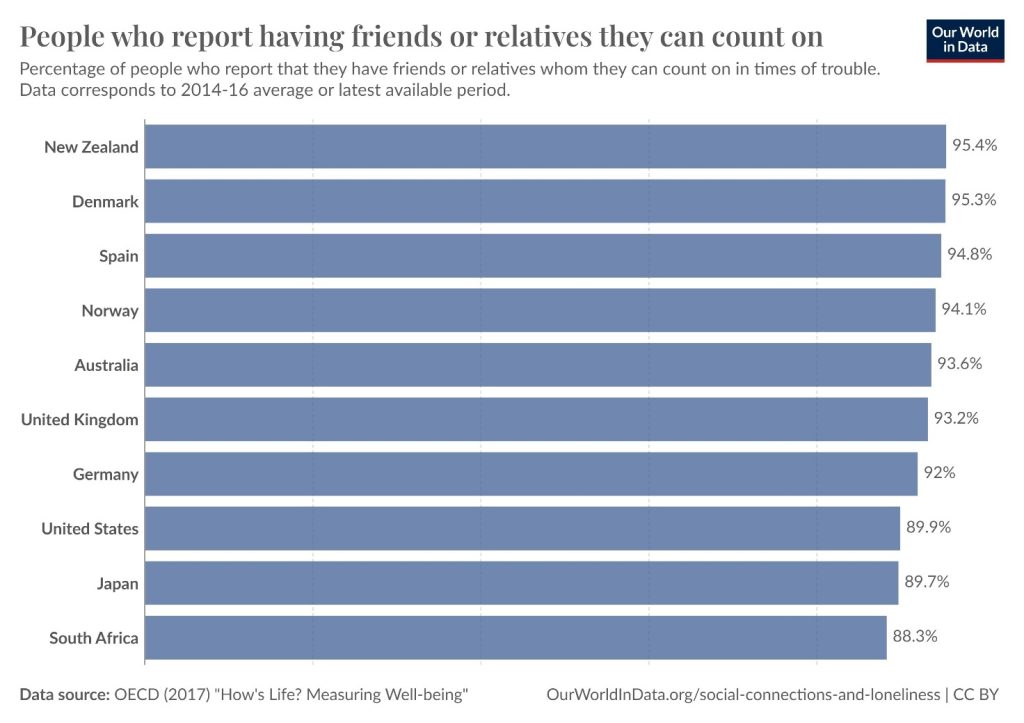
However, for people who do not have good social connections and support networks, loneliness and social isolation may increase their risk of poor health and wellbeing outcomes. A unique longitudinal study of human wellbeing, the Harvard Study of Human Development, concludes that social connections are one of the most important factors for people’s happiness and health. In a study in the United States of 724 boys that spanned 80 years, the individuals who lived longest had the strongest relationships and those who were lonely died younger[119].
In an online survey launched in April 2022 as part of the Department of Health and Social Care’s call for evidence on mental health and wellbeing, 77% of respondents said that ‘Social and family relationships’ have the biggest influence on their mental health[120]. A small number of close friendships and strong connections to family may be more important, in terms of reducing risks of loneliness and social isolation, than many acquaintances[121]. For older people, and for adolescents, the quality of social relationships is of more importance than the quantity of relationships[122].
Evidence suggests that the experience of ‘romantic loneliness’ may have a greater impact on suicide ideation than other types of loneliness, particularly among young men[123].
Mediation Surrey aims to bring people together through improved resilience, communication and understanding, to help them cope with, resolve, and prevent disputes.
Its Community Mediation and Intergenerational Mediation services can help to resolve disputes and work towards good family and community relationships.
New parents
Even before the Covid-19 pandemic new parents were reporting high levels of loneliness and social isolation. A British Red Cross report suggests that 82% of mothers under the age of 30 felt lonely ‘some of the time’ and 43% of mothers under the age of 30 felt lonely ‘often’ or ‘always’ prior to the pandemic[124]. Anxiety, depression and loneliness increased among expectant mothers during the pandemic[125]. There is evidence that parental loneliness has direct and intergenerational impacts on parent and child mental health[126].
A Ipsos MORI survey, commissioned by Movember in 2019 about men’s social connections and the impact of becoming a father, revealed that almost a quarter (23%) say they felt isolated when first becoming a parent. A fifth of fathers surveyed say they lost friendships once they became a parent. Young fathers are most likely to feel isolated (40% of those aged between 18 and 35, compared to 11% of fathers aged 55 or above)[127]. The focus of perinatal and postnatal services and support on women can contribute to men’s sense of isolation on becoming a parent[128].
Young parents (under the age of 25) can find the experience of becoming a parent particularly isolating due to financial constraints and discrimination and negative judgement from society and health professionals. According to a report by The Young Women’s Trust, over a quarter of young mothers (26%) left the house once a week or less[129].
New parents from ethnic minority communities are at high risk of loneliness and social isolation following the birth of a child. Evidence points to the cultural isolation many new parents from ethnic minority backgrounds experience, particularly when there are problems with the baby. Discrimination and language barriers also contribute to feelings of loneliness and a sense of isolation from the community[130].
Home-Start Spelthorne is a charity that offers bespoke support and friendship through a unique model of parents supporting parents. Volunteers are trained in the art of listening, safeguarding and scaffolding care and support to engage and empower families to build a resilience to deal with challenging times. Home Start Spelthorne is part of Home Start Surrey, a consortium of eight Home Start organisations across Surrey.
Loneliness and Social Isolation is a key factor in most families that are referred by health, education, or statutory professionals to Home-Starts around the country. Families can also self-refer. Isolation can be due to many reasons: poor mental health, fleeing domestic abuse, relationship breakdowns, multiple births, or many children under 5 years old, disabilities, or health problems.
A Home-Start coordinator meets with the family to listen and co-produce a bespoke plan, empowering the parent to guide and influence the change they want for themselves and their children. A carefully selected volunteer is matched, plan discussed, and safety guidance reiterated to be clear the professional friend relationship is established.
Support is not time limited, allowing relationships and trust to develop. Through gentle guidance families are introduced to community groups in which the family have the volunteer to help prepare and support the family to attend. Home-Start uses the scaffolding theory – step by step building the frame and then as confidence and skills are acquired the frame gets slowly lowered leaving families empowered. 94% of families feel less isolated after receiving support from a Home Start volunteer. (Source: Annual Report 2022/23).
‘I was so alone, I never the left the house, I was too scared to go to the local play and stay. Having 3 children under 5, meant I just didn’t have enough hands when they all go in different directions, having my own volunteer friend made it possible to get ready, leave the house and attend somewhere’.
‘The volunteer showed me how to strike up a conversation with strangers and this helped me start talking to other parents in the park and other groups, now I am more confident to see and speak to people and my children get to play and experience more social opportunities.’
As part of the Best Start for Surrey Strategy 2022 – 2027, Surrey Minority Ethnic Forum (SMEF) ran ‘Baby Steps’ sessions for pregnant people (and those with young children) from ethnic minority populations. Some participants were also refugees and asylum seekers. Most participants who were surveyed as part of the evaluation had felt isolated in their communities. The Baby Steps sessions provided opportunities to connect to peer support, improve English language skills, develop digital literacy, increase physical activity, and feel less isolated in their role as parents[131].
Domestic abuse
Survivors of domestic abuse are vulnerable to becoming socially isolated and at high risk of experiencing loneliness. Many survivors of domestic abuse are isolated from friends and family by their abuser as a form of control that makes it harder to seek support[132]. Relocating to a refuge or temporary accommodation, often some distance away from support networks, compounds the isolation and loneliness experienced by survivors of domestic abuse. For the children of domestic abuse survivors, relocation sometimes means changing schools, long waits for specialist school places, and other disruptions to social networks[133].
Police data for the year ending March 2023 show that Surrey has a lower rate of domestic abuse crimes and incidences than its statistical neighbours. In 2022-23 there were 9,995 domestic abuse related crimes (8.3 per 1,000 population).
Table 26: Number and Rate of police recorded domestic abuse related incidents and crimes recorded for year ending March 2023.
| Area | Combined incidents and crimes |
Rate per 1,000 population |
|---|---|---|
| England and Wales | 1,453,867 | 24.4 |
| South East | 194,017 | 20.9 |
| Surrey | 9,995 | 8.3 |
| Kent | 54,899 | 29.5 |
| Hampshire | 45,116 | 22.5 |
| Essex | 39,583 | 21.2 |
| Gloucestershire | 13,590 | 21.0 |
| Hertfordshire | 20,850 | 17.4 |
In Surrey, Reigate and Banstead are the areas with the highest identified need around domestic abuse. The Surrey Domestic Abuse Needs assessment sought feedback from survivors, children, and partners which highlighted a need for holistic support and warm handovers when seeking support from other agencies (rather than just signposting). Furthermore, the response to a first disclosure of abuse sets a precedent to future interactions with services[134]. This finding aligns with the feedback from Surrey’s wellbeing professionals during loneliness workshops, where professionals felt that trust in a service could make the difference between someone getting out of loneliness or for the experience of loneliness to become chronic. Trust in services was also stated to be influenced by previous experiences[135].
Surrey’s Violence Against Women and Girls Partnership Strategy for 2023-2025 is a county-wide strategy to ensure collaborative commitment and action in tackling violence against women and girls, in all its forms. This strategy was created in partnership with the expertise of survivors, specialist service provision, community organisations, and statutory agencies.
Children & Young People
Loneliness and social isolation are often perceived as experiences mostly affecting older people, but they can be felt at any time across the life course. Research shows that young people can be more susceptible to loneliness than older people[136].
Global estimates suggest that between five and 15 percent of adolescents experience loneliness[137]. In a 2018 ONS survey, one third of young people reported feeling lonely and more than 20 percent reported feeling lonely often or always[138]. The Community Life Survey (2021/22) found people aged 16-24 more likely to say they feel lonely often/always (10%) than every other age group (3 to 6%) aside from those aged 25-34 (9%)[139]. The number of children who say they feel lonely at school more than doubled between 2012 and 2018. Some speculate that the current generation of young people may the loneliest generation there’s ever been[140].
Some feelings of loneliness during adolescence are a normal part of growing up and growing apart from childhood and parents[141]. However, during the Covid-19 pandemic, lockdowns had an adverse impact on children and young people in terms of loneliness and social isolation. Older people seem to have been more resilient to periods of social isolation than young people. Significantly more under 30s reported feeling lonely during the Covid-19 lockdowns with self-reported loneliness declining with age[142].
The use of social media is prevalent among children and young people. In developed countries around the world more than 90 percent of adolescents and young adults subscribe to social media platforms. Evidence suggests that social media may be detrimental to face to face relationships, leading to loneliness, social isolation, and poor mental health[143]. However, social media can also foster a sense of belonging for young people and therefore be an enabler of social connection. Whether young peoples’ social media use encourages social connection or triggers feelings of loneliness depends on numerous variables including, personality type, extent of use, and how social media is used. ‘Active use that aims to establish meaningful social connections can have positive effects. Passive use likely has negative effects’[144].
Any child or young person may experience transient feelings of loneliness but adverse events during childhood or adolescence can be triggers for chronic loneliness which may persist into adulthood and is detrimental to physical and mental health[145]. The loneliness and social isolation felt by children and young people with additional needs and disabilities was exacerbated by the Covid-19 pandemic and continues to have a detrimental impact on mental health and wellbeing[146]. For children and young people with learning disabilities, evidence suggests that fear of being bullied is keeping them socially isolated. According to Mencap, over 1 in 3 people with a learning disability worry about being bullied when they go out[147]. Neurodiverse children and young people are more likely to experience loneliness than their neurotypical peers. Loneliness among neurodiverse children and young people is associated with negative consequences for mental health, behaviour, and psychosocial/emotional development, with a likely long-term impact in adulthood[148].
For children and young people who experience mental ill-health, stigma is shown to disrupt social relationships, and lead to loneliness, social isolation, and depression. Research suggests that a lack of understanding from others can increase feelings of loneliness and social isolation for young people with mental health needs. Stigma also reduces their self-esteem and confidence, compounding their sense of isolation from their peers[149].
The JSNA authors met with two groups of young people, surveyed others, and sought insights from partners to understand how Surrey’s children and young people experience loneliness and social isolation, and what good social connection looks like to them. Some key themes emerged:
Covid-19
Generally, Covid-19 impacted negatively on young people’s feelings of social connection. Studying virtually was challenging (though it suited some). The pandemic lockdowns increased social isolation: “It felt like I had no friends in COVID because you couldn’t see them. Not seeing them face to face made them feel more distant.”
Trusted relationships
Trust and support were key themes raised by focus group participants. Levels of trust in other people and in services impacts on young people’s experiences of interacting with support. “I don’t trust a lot of people due to bad experiences of people in the past”, said one participant.
This theme of trust was also raised in Healthwatch Surrey’s qualitative research into children and young people[150]. Their interviews highlight the importance of community organisations as safe spaces to socialise and find others to connect with. Children and young people felt that trust was a necessary element for them to feel supported and have a positive experience with community organisations. Trust is created through staff taking time to get to know them, understand their needs and how best to support them.
The JSNA loneliness and social isolation focus groups also found that the perception of support from others for mental health, for example, was critical for creating trust and maintaining social connection. Where there was a low sense of perceived trust and support, the young person was more likely to feel a disconnect.
“I think feeling understood by the adults around you is really important for not feeling lonely. When you feel misunderstood and feel your problems are dismissed and are ‘normal teen problems’ it makes you feel so alone and unworthy. This can stop you reaching out in the future and continue to make you feel lonely.”
Peer support
Focus group participants emphasised the value of peer support and being able to socialise with people with shared experiences. Some services support mental health and some groups provide opportunities to socialise, but focus group participants raised a lack of groups that are both supportive and provide opportunities for social connection.
“There aren’t groups that are supportive of mental health and are for socialising.”
“You can be surrounded by people trying to help you but when you don’t know anyone who’s ill in the same way you are, that can feel really lonely.”
Neuro-divergence
Neurodiverse focus group participants highlighted a lack of understanding from their neurotypical peers about their needs or behaviour, which made social connection challenging:
“It’s hard when friends don’t understand or respect the boundary.”
“That’s when socialising for autistic people or neurodivergent people is much more difficult.”
Social media
Whilst the isolating effects of social media use were acknowledged by focus group participants, social media was also identified as an enabler to social connection in a way that parents and other adults may not understand.
“I feel parents need to be educated on how social media is not bad and is a lifeline for many young people, especially when struggling with loneliness.”
Young people in Surrey with care-experience issued the action card below to decision makers. An action card is raised when 4 or more children and young people tell Surrey County Council something they want to stop, start, or change about a service. Action cards are a way for children and young people to get important messages to decision makers. Action cards are allocated to the relevant service or individual for feedback and it is only within the power of children and young people to close the action cards.
OPEN ACTION STATEMENT:
‘As young people in Surrey with care-experience, we would like help to develop a sense of community, friendships, and support networks. We would like social workers and other professionals to help us attend participation groups for care-experienced young people and find new hobbies or activities so that we can develop relationships in our local area.’
For the parents and families of children with additional needs and disabilities, cuts to services can have a serious impact on the social opportunities available to their children and on the quality of their family life. Disability Challengers provides play for disabled children and young people and respite for their families. A Disability Challengers Parent Survey (2023) shows that the impact the service has on reducing isolation for their children drops when children have less access to placements because of funding cuts.
Figure 44: ‘Attending Challengers reduces my child’s isolation’. (Source: Disability Challengers Parents Survey 2023).
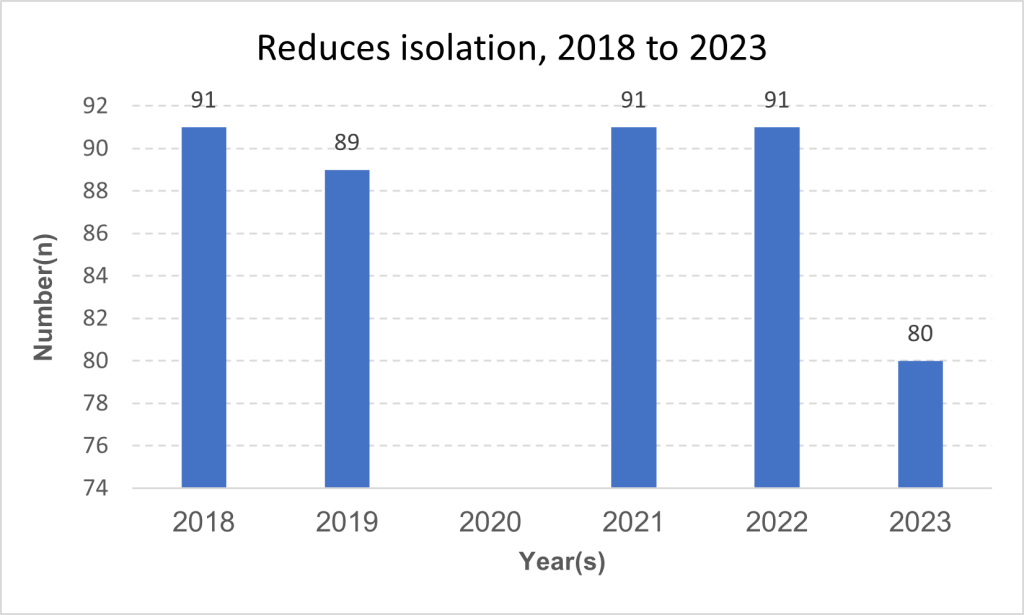
Respondents to the Parent Survey commented that fewer placements and reduced opportunities for respite care has a negative impact on family life. One parent said: “The lack of break does restrict the chance of social interaction and employment for me.”
Absence from school
The Education and Lifelong Learning Strategy’s priority workstreams for the Surrey Education Partnership (2024-26) include to ‘ensure providers, settings, schools and colleges have the skills, confidence and understanding to support children, young people and adult’s emotional well- being to enable them to thrive and learn’[151].
Exclusion from school can have a profound impact on children and young people. Evidence shows that when a young person is excluded from school the adverse effects of exclusion – combined with loneliness and social isolation, declining mental health and risk of homelessness – can be a self-perpetuating cycle whereby inequality is entrenched[152].
Children in Surrey are generally absent less than the national and South East average. This changes when examining data from selected vulnerable groups. In Surrey, the absence rates for children eligible for free school meals is higher than both the national and South East average. This is also true for absence of children from the Gypsy, Roma and Traveller community[153].
Emotionally Based School Non-attendance
Emotionally based school non-attendance (ESBNA) is when children find attending school difficult due to emotional factors that lead to anxiety. This can lead to absences from school and affects approximately 2% of the school population[154].
Table 27: Surrey school attendance data. (Source: DfE Attendance Returns}.
| School Absence | Overall absence rate 2018/19 |
Overall absence rate 2020/21 |
Overall absence rate 2021/22 |
% persistent absentees (10% or more missed) 2018/19 |
% persistent absentees (10% or more missed) 2020/21 |
% persistent absentees (10% or more missed) 2021/22 |
|---|---|---|---|---|---|---|
| England Total | 4.7% | 4.6% | 7.6% | 10.9% | 12.1% | 22.5% |
| England Special | 10.1% | 15.2% | 13.2% | 28.8% | 48.9% | 40.4% |
| England State funded primary | 4.0% | 3.6% | 6.3% | 8.2% | 8.8% | 17.7% |
| England State funded secondary | 5.5% | 5.5% | 9.0% | 13.7% | 14.8% | 27.7% |
| South East Total | 4.7% | 4.4% | 7.5% | 10.6% | 11.4% | 22.0% |
| South East Special | 10.2% | 15.6% | 13.1% | 29.0% | 50.8% | 40.1% |
| South East State funded primary | 4.0% | 3.4% | 6.2% | 7.8% | 8.0% | 17.0% |
| South East State funded secondary | 5.6% | 5.3% | 9.0% | 13.7% | 14.1% | 27.5% |
| Surrey Total | 4.4% | 4.0% | 7.1% | 9.3% | 9.7% | 19.6% |
| Surrey Special | 9.7% | 16.9% | 12.3% | 26.5% | 55.8% | 35.4% |
| Surrey State funded primary | 3.8% | 3.1% | 6.0% | 6.9% | 6.7% | 14.9% |
| Surrey State funded secondary | 5.2% | 4.7% | 8.4% | 12.1% | 11.8% | 25.1% |
Surrey’s Family Voice Survey (2021) and EBSNA support group found that families struggling with EBSNA can feel guilt at “forcing” their child to attend school, feel lonely and isolated, and struggle to find and access support. One respondent shared:
‘It is extremely isolating, and I feel very judged for not trying hard enough to ‘force’ my daughter to school. The trust is we’ve been asking for help for 5 years.’
To support families through this, the Psychology Service highlights some protective factors which can be boosted through various initiatives. One of these protective factors is ‘bonding’, in which the individual feels a sense of connection to their world.
Each District and Borough in Surrey has additional support provided through a school-based needs/ Mindworks cluster of staff which includes a named practitioner as a point of contact who will offer consultation, support and advice. The cluster teams can support parents with workshops to help manage stress and anxiety, group interventions, school consultations and individual support.
Home schooling
Between 2020 and 2024 the number of children registered as electively home schooled has increased in Surrey[155]. Further insights are required on the experiences of home-schooled children and young people and how these relate to loneliness and social isolation. We need to understand differences between the experiences of children and young people in the elective home education community, those who are being educated at home because their needs are not being met in school, and those children who are at home but not receiving any education.
Mental health waiting lists
The report on commissioned services across the Children, Families and Lifelong Learning directorate gathers data on thematic service areas in Surrey. The January 2024 report highlighted that waiting times for children and young people to access neurodevelopmental and learning disability pathways appointments were at their highest point recorded within the life of the contract at 200 working days[156]. Pressures on delivery partners is high, with referrals outweighing commissioned capacity.
Students
Government research shows that nearly all students (92%) experience loneliness and nearly half (43%) worry about being judged if they admit to feeling lonely[157]. Over half (53%) of students feel uncomfortable seeking help for loneliness. Loneliness was more of a concern for students than money, housing or managing their course.
Mental health problems can increase a sense of isolation and feelings of loneliness for students. The stigma associated with mental health compounds this. In the Surrey Stigma Survey 2024, 11.4% of respondents report experiencing stigma or discrimination at university[158].
Student Mind is the UK’s student mental health charity and has created different peer support groups, two of which are run in Surrey. Positive Minds is a 6-week programme for students experiencing low mood, loneliness, or depression whilst at university. The group is led by trained students and offers a non-judgemental, safe, and confidential space.
Bereaved
People experiencing bereavement are particularly vulnerable to loneliness. The Covid-19 pandemic is likely to have exacerbated this for many people. In a survey conducted by the UK Commission on Bereavement, ‘social isolation and loneliness’ was the second most difficult experience related to grief during lockdown (after ‘not being able to have a funeral as desired’)[159]. Even before the pandemic, loneliness was shown to be the biggest challenge to coping with daily life following the death of a partner[160]. Bereavement is associated with emotional loneliness (the perceived absence of intimate or emotional attachment) rather than social loneliness (the absence of a social network), and social support from others may not alleviate this emotional loneliness[161]. Loneliness may also play a key role in how people adapt to bereavement[162].
A review of risk factors for experiencing loneliness after a bereavement found the following variables to be indicators of the intensity of loneliness felt by people[163]. First, being a care giver can be associated with more intense loneliness post-loss. Second, people with lower mental and physical health are likely to experience increased loneliness after loss. Third, heightened loneliness is found among bereaved people with low levels of social support among family and friends. Fourth, individual behaviours and approaches to loss, such as adopting a flexible coping style, may protect people from heightened or chronic loneliness. The review found no evidence that age or gender are relevant to determining experiences of loneliness after loss.
Evidence shows that the loneliness and isolation people experience following loss is affected by the type of bereavement they experience. Bereavement through violent or sudden causes is associated with more severe negative health and wellbeing outcomes compared to other types of loss[164]. People bereaved by suicide may be at an increased risk of adverse outcomes associated with grief. ‘Factors such as stigmatisation and shame may lead to feelings of social isolation, loneliness, and social withdrawal among people bereaved by suicide’[165]. Though the positive impact of social support after traumatic events is less evident for traumatic bereavement[166] an Australian evaluation of a community-based suicide bereavement service suggests that crisis support provided close to the time of suicide reduces feelings of social loneliness and protects against grief reactions associated with suicide, including suicide ideation[167].
Evidence also suggests an association between post-bereavement loneliness and suicide attempt or suicide ideation[168]. Loneliness, therefore, may be a potential target for suicide prevention interventions among bereaved people.
Based on figures for 2019-2020 there were 11,390 deaths in Surrey over 12 months[169]. It is estimated that for every death, nine people are affected by bereavement[170]. So, between 2019 and 2020, 102,510 people were affected by the death of a Surrey resident.
The Brigitte Trust provides support for people living with a life limiting illness in Surrey. Bereavement support for families may continue for up to three months after the death of a relative. It also runs free structured 8-week bereavement programmes run by a professional facilitator for anyone in Surrey struggling with their own grief and bereavement. The aims of the programme are to:
- provide support with focus
- encourage mutual support
- share experiences
- learn new coping strategies
- develop some altered thought patterns.
For support with dealing with and planning for death, the Brigitte Trust hosts regular Death Café and Coffin Club sessions in Surrey.
LGBTQ+
LQBTQ+ people are at high risk of loneliness, social isolation, and mental health issues. There are particularly high rates of social isolation and loneliness among transgender and gender diverse people. Other determinants (education, physical and mental health, unemployment) intersect with gender identity to increase levels of loneliness and social isolation[171]. Globally LGBTQ+ people are more likely to be socially and emotionally lonely when they experience minority stress – the negative impact of living with a stigmatised identity – or they feel marginalised. LGBTQ+ people who are involved with their local LGBTQ+ community are less likely to feel lonely or social isolated[172].
During COVID-19 lockdowns self-reported loneliness increased from one fifth of LGBTQ+ people to over fifty percent of LGBTQ+ people. Transgender and gender diverse people reported higher rates of loneliness in lockdown than cis gender people. Self-reported loneliness was higher for LGBTQ+ people from minority ethnic groups[173].
Evidence suggests that transgender and gender diverse people are more vulnerable to loneliness and social isolation than cis gender people. A German study indicates a correlation between the loneliness and social isolation experienced by transgender and gender diverse people and low levels of education, poor health, and unemployment. It identifies a vicious cycle of discrimination that leads to poorer education and health outcomes which isolate people and contribute to feelings of loneliness. The loneliness and social isolation that transgender and gender diverse people experience perpetuates their risk of poor health and wellbeing outcomes[174].
Older LGBTQ+ people are especially vulnerable to loneliness because they are more likely to be single, live alone, and have less contact with relatives[175]. They are also less likely to engage in services. Four-fifths of older LGBTQ+ people do not trust professionals to understand their culture or lifestyle[176]. They may feel isolated from the LGBTQ+ community by age, frailty, or disability, and isolated within older people spaces by discrimination, fear of discrimination, or internalised stigma. Evidence shows that social care environments can severely compromise ‘the identity and relationships that older LGBT people developed over their life course’[177]. LGBTQ+ focused social groups are important to older people receiving social care for offsetting loneliness and social isolation. However gay and bisexual men may be more likely to access support from social groups than lesbian and bisexual women[178].
Youth Workers from Surrey County Council run Twister, which is a safe space where young people can meet to get support, make friends, and take part in fun, creative and awareness raising activities. It is for young people age 11 to 19 and up to 25 if the young adult has additional needs or disabilities.
There are four Twister groups in Surrey: Guildford, Redhill, Epsom, and Woking. Woking Twister host a fortnightly group on a Thursday for anyone with caring responsibility for an LGBTQ+ young person.
The Eikon Charity runs youth groups in Guildford for LGBTQ+ young people aged 11-18 and online groups for LGBTQ+ young people aged 18-24 with additional needs and disabilities. Eikon also provides LGBTQ+ focused wellbeing sessions for young people exploring their identity and emotions.
Blossom in Woking provides a social space, an employability and mentoring service, and arts workshops for young LGTBQ+ people (ages 18-30). Blossom’s LGBT Wellbeing and Social Space supports social connections and ongoing friendships with like-minded people.
Outline is a Catalyst helpline giving support, advice, and information to LGBTQ+ people.
Figure 45: Source: SAPE population, 2020, Connect to Support Surrey – LGBT (search date March 2024)
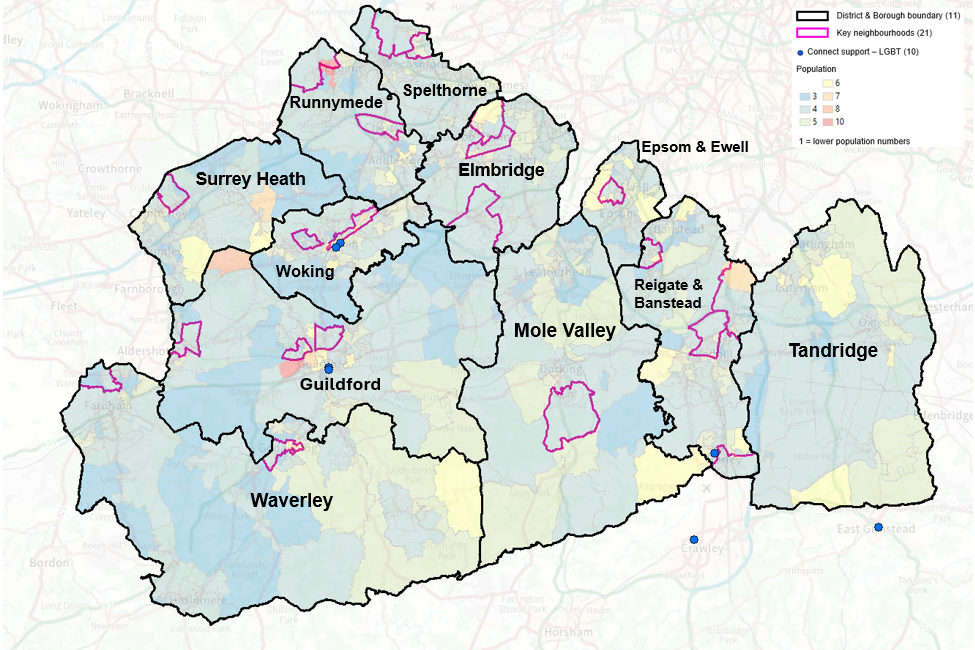
Table 28: Source: SAPE male population, 2020, Connect Support LGBT.
| Area Name | Number of Connect Support LGBT | Online/ telephone service | Total Number of Services |
|---|---|---|---|
| Surrey | 5 | 2 | 7 |
| Elmbridge | 0 | 0 | 0 |
| Epsom & Ewell | 1 | 0 | 1 |
| Guildford | 2 | 0 | 2 |
| Mole Valley | 0 | 0 | 0 |
| Reigate & Banstead | 1 | 0 | 1 |
| Runnymede | 0 | 0 | 0 |
| Spelthorne | 0 | 0 | 0 |
| Surrey Heath | 0 | 0 | 0 |
| Tandridge | 0 | 0 | 0 |
| Waverley | 0 | 0 | 0 |
| Woking | 1 | 2 | 3 |
| Outside Surrey | 2 | 0 | 2 |
| Total | 7 | 2 | 9 |
Retired, unemployed, and economically inactive.
Evidence at national level points to a correlation between economic status and self-reported loneliness and social isolation. Men and women with lower economic status are more likely to report loneliness, social isolation, and lack of social support [179]. Social isolation and loneliness are worse for the poorest and most socially disadvantaged older adults [180]. Over 50s with poorest economic status are more likely to experience decreased enjoyment of life and increased loneliness [181].
Studies show for people of working age there is a 40 percent increase in likelihood of reporting loneliness when unemployed. The severity of loneliness for people who are unemployed peaks at the ages of 30-34 and 50-59. Not only is loneliness more likely to be experienced following job loss but loneliness is also shown to be predictive of unemployment ‘suggesting potential bi-directionality in the relationship‘, which may ‘create a multiplier effect between loneliness and unemployment to form a self-reinforcing relationship and greater health concerns for those most at risk‘ [182]. The impact of loneliness on unemployment is exacerbated by poor physical health [183]. Evidence suggests a need to tackle loneliness in order to address unemployment. ‘Decreased loneliness could mitigate unemployment, and employment abate loneliness, which may in turn relate positively to other factors including health and quality of life.‘. [184]
An annual (summary) score card of progress in delivery of the Health & Wellbeing Strategy to help gauge system-wide success (or otherwise) has been developed in June 2024. It shows that Surrey is performing significantly worse – by 8% compared with the South East and nationally – for adults in contact with secondary mental health services in terms of the employment gap between them and the general population (and in terms of the numbers in stable and appropriate accommodation) [185].
At the time of the 2021 Census, 28,023 usual residents of Surrey were economically active and unemployed (2.9%). This included people who were looking for work and could start within two weeks, or waiting to start a job that had been offered and accepted.
The percentage of usual residents aged 16 years and over who were economically active and unemployed was lower in Surrey (2.9%) than the South East (3.0%) and England (3.5%). At the time of the 2021 Census, Runnymede and Spelthorne had the highest proportions of residents aged 16 and over who were unemployed at 3.6 per cent compared to Mole Valley and Waverley which had the lowest proportions at 2.3 per cent.
The table below also includes the total numbers of unemployed residents by whether they were also full-time students. Of the 28,023 unemployed residents of Surrey, 17.8 per cent were also full-time students (which represented 4,982 residents). Runnymede had one of the highest proportions of unemployed residents (3.6%), however, just under a third of these unemployed residents were also full-time students (30.4%). Guildford also had a high proportion of those unemployed also being full-time students (32.8%) which represent different employment requirements for these areas where individuals want to find work to go alongside their studies.
Table 29: Status of unemployed Surrey residents
| Local authority | Of all residents, the % unemployed |
Total unemployed | Of those unemployed, % who were FT students |
Total unemployed who were FT students | Total unemployed (excluding FT students) |
|---|---|---|---|---|---|
| England | 3.50% | 1,596,288 | 17.80% | 283,559 | 1,312,729 |
| South East | 3.00% | 229,763 | 17.80% | 40,871 | 188,892 |
| Surrey | 2.90% | 28,023 | 17.80% | 4,982 | 23,041 |
| Runnymede | 3.60% | 2,647 | 30.40% | 805 | 1,842 |
| Spelthorne | 3.60% | 3,015 | 13.00% | 393 | 2,622 |
| Guildford | 3.10% | 3,655 | 32.80% | 1,200 | 2,455 |
| Woking | 3.00% | 2,494 | 13.40% | 333 | 2,161 |
| Surrey Heath | 2.80% | 2,083 | 14.40% | 299 | 1,784 |
| Epsom and Ewell | 2.80% | 1,807 | 17.40% | 314 | 1,493 |
| Reigate and Banstead | 2.80% | 3,347 | 13.20% | 442 | 2,905 |
| Elmbridge | 2.80% | 3,020 | 11.20% | 338 | 2,682 |
| Tandridge | 2.60% | 1,876 | 12.50% | 235 | 1,641 |
| Mole Valley | 2.30% | 1,686 | 12.20% | 206 | 1,480 |
| Waverley | 2.30% | 2,396 | 17.50% | 419 | 1,977 |
Residents who were unemployed on the 2021 Census Day were also asked how long they had been unemployed for. Two thirds of Surrey residents who were unemployed on Census Day had not worked in the last 12 months (66%, which represented 251,254 residents), a longer-term period of unemployment. In contrast, 14 per cent of those unemployed on Census Day in March 2021 had worked in the last 12 months and so this group had a shorter period of unemployment (which represented 54,445 residents). Of those unemployed at the time of the Census, 20 per cent had never worked (which represented 77,287 Surrey residents).
Surrey had a lower proportion of unemployed residents who had never worked (20%) than the South East (21%) and England (26%). Every district and borough in Surrey had lower proportions of unemployed residents who had never worked than the England average, and only four districts and boroughs (Runnymede, Woking, Epsom and Ewell, Spelthorne, and Guildford) had higher proportions than the South East average.
Within Surrey districts and boroughs, Runnymede had the highest proportion of unemployed residents who had never worked at 23 per cent, compared to Mole Valley which had the lowest at 17 per cent.
Figure 46: Percentage of Surrey residents in each District and Borough who had never worked, of those who were unemployed at the time of the 2021 Census
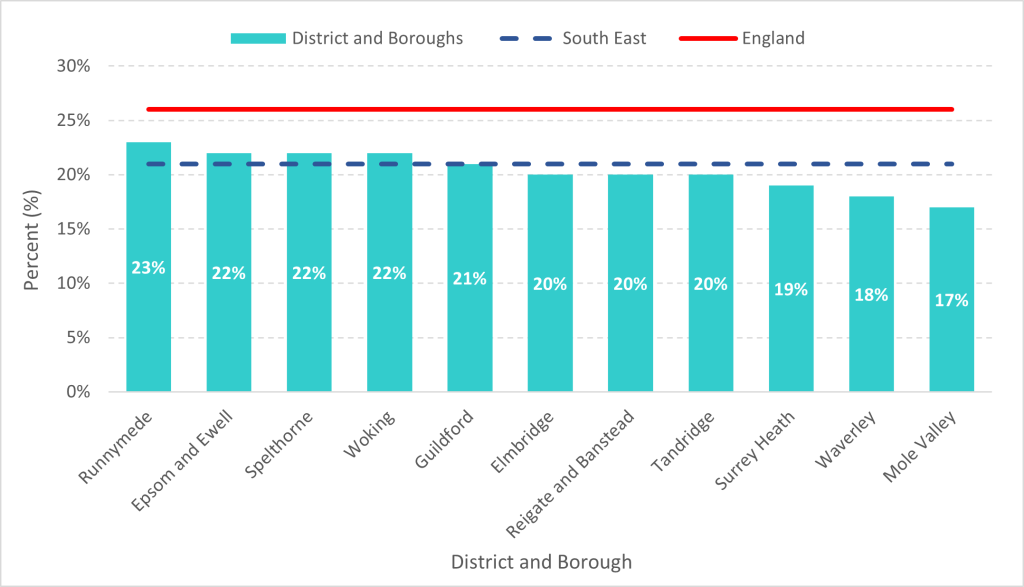
Over one third of Surrey residents aged 16 and over were economically inactive around the time of the 2021 Census. A lower proportion of those aged 16 and over were economically inactive in Surrey (36.5%) than in the South East (37.8%) or England (39.1%). Mole Valley and Waverley had the highest proportions of residents aged 16 and over who were economically inactive (39.1%), which represented 28,311 and 40,518 residents respectively. Woking had the lowest proportion of residents aged 16 and over who were economically inactive (33.4%).
Table 30: the breakdown of reasons for being economically active at the time of the 2021 census
| Reason cited | Surrey total who cited | Of all Surrey residents, % who cited |
Of all Southeast residents, % who cited |
Of all England residents, % who cited |
|---|---|---|---|---|
| Retired | 210,964 | 21.7% | 22.5% | 21.5% |
| Student | 53,252 | 5.5% | 5.1% | 5.6% |
| Looking after home or family | 43,702 | 4.5% | 4.4% | 4.8% |
| Long-term sick or disabled | 22,944 | 2.4% | 3.1% | 4.1% |
| Other | 24,099 | 2.5% | 2.7% | 3.1% |
Surrey residents who were economically inactive due to long-term sickness or disability consisted of 22,944 individuals, which is 2.4% of all Surrey residents aged 16 and over. This group makes up a lower proportion of all residents aged 16 and above in Surrey (2.4%) compared to the South East (3.1%) and England (4.1%).
Table 31: Residents who were economically inactive due to long-term sickness or disability, 2021
| Local authority | % Economically inactive due to long-term sickness or disability (out of all residents) | Total long-term sick or disabled |
|---|---|---|
| England | 4.10% | 1,874,300 |
| South East | 3.10% | 234,601 |
| Surrey | 2.40% | 22,944 |
| Spelthorne | 2.80% | 2,332 |
| Reigate and Banstead | 2.70% | 3,234 |
| Tandridge | 2.60% | 1,816 |
| Mole Valley | 2.60% | 1,849 |
| Woking | 2.40% | 2,011 |
| Waverley | 2.30% | 2,405 |
| Epsom and Ewell | 2.30% | 1,463 |
| Runnymede | 2.20% | 1,597 |
| Surrey Heath | 2.20% | 1,594 |
| Guildford | 2.10% | 2,519 |
| Elmbridge | 2.00% | 2,125 |
Spelthorne and Reigate & Banstead had the highest proportion of residents aged 16 and over who were economically inactive due to long-term sickness or disability[186].
Farmers
People who work in the agricultural sector are known to be at risk of loneliness and social isolation, which in turn have been identified as factors commonly contributing to mental health problems and suicide among farmers. More than one farmer a week loses their life to suicide in England and Wales[187]. The drivers of loneliness and social isolation within the farming community are multi-dimensional and specific to the farming context. Farmers experience social loneliness from long working hours often spent alone. There is little time for social activities or maintaining social connections. The emotional loneliness of farming is compounded by the blurring of lines between work life and family life, and by the stigma of talking about mental health issues. Farmers may also experience a cultural loneliness that stems from the disconnection between farming and the wider public who may have little knowledge of farming life and its unique challenges including financially[188].
253,000 of residents aged 16 years and over, work in agriculture and related industries, 27.4% (69,300) are farmers. Approximately eight percent of those farmers are in the Southeast region. In Surrey, of the 589,586 residents aged 16 years and over in employment, 1,128 are managers and proprietors in agriculture related services and 7,704 are employed in agricultural and related trades.
Waverley and Mole Valley have the highest percentage of residents employed in agricultural and related trades. Of Surrey’s key neighbourhoods, Canalside, Holmwoods, and Tattenham Corner & Preston have the highest percentage of residents employed in agricultural and related trades.
Figure 47: Number of people in occupations in agriculture and related trades (Source: Nomis 2021).
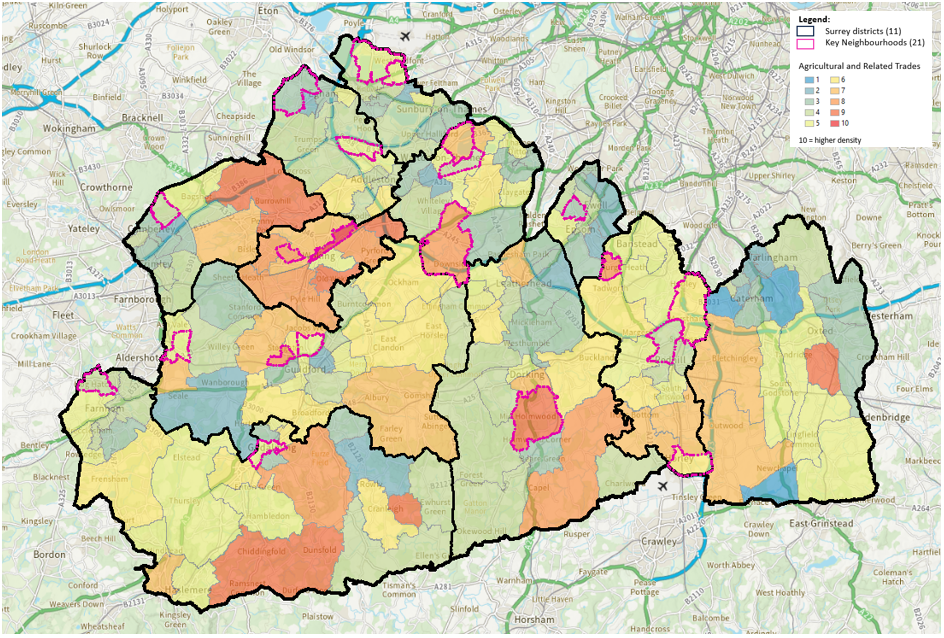
Table 32: Top wards of occupations in Agriculture and related trades. (Source: Nomis 2021.)
| District & Borough | Ward Name | All usual residents aged 16 years and over in employment the week before the census (Number) |
Agricultural and Related Trades (Number) |
Agricultural and Related Trades (Percent) |
Key Neighbourhood |
|---|---|---|---|---|---|
| Elmbridge | Cobham and Downside | 3,868 | 77 | 1 | N |
| Guildford | Westborough | 4,550 | 72 | 0.93 | Y |
| Mole Valley | Capel, Leigh and Newdigate | 2,088 | 79 | 1.03 | N |
| Mole Valley | Holmwoods | 3,164 | 85 | 1.1 | Y |
| Reigate & Banstead | Tattenham Corner & Preston | 5,066 | 79 | 1.03 | Y |
| Surrey Heath | Windlesham & Chobham | 3,364 | 89 | 1.16 | N |
| Tandridge | Bletchingley and Nutfield | 2,896 | 69 | 0.9 | N |
| Tandridge | Oxted South, | 3,175 | 82 | 1.06 | N |
| Waverley | Bramley, Busbridge and Hascombe | 2,414 | 70 | 0.91 | N |
| Waverley | Chiddingfold and Dunsfold | 1,983 | 85 | 1.1 | N |
| Waverley | Cranleigh East | 3,123 | 89 | 1.16 | N |
| Waverley | Haslemere Critchmere and Shottermill | 3,011 | 69 | 0.9 | N |
| Woking | Bisley & West End | 5,061 | 69 | 0.9 | N |
| Woking | Byfleet and West Byfleet | 6,112 | 80 | 1.04 | N |
| Woking | Canalside | 5,265 | 100 | 1.3 | Y |
| Woking | Goldsworth Park | 4,885 | 70 | 0.91 | Y |
| Woking | Heathlands | 4,737 | 73 | 0.95 | N |
| Woking | Hoe Valley | 5,130 | 81 | 1.05 | N |
| Woking | Knaphill | 5,895 | 73 | 0.95 | N |
| Woking | Pyrford | 4,698 | 75 | 0.97 | N |
Farmers interviewed for a UK research study described the challenges in connecting with others: ‘I don’t think people who haven’t been involved in agriculture – or even those who are but haven’t farmed themselves – can relate to the problems at all. When I speak to non-farmers, I just feel like banging my head against a brick wall.’[189]
Addressing loneliness and social isolation among farmers requires a thoughtful approach. As one farm support practitioner said, ‘There needs to be an element of compassion and empathy and understanding of the multi-layer complexity that farmers are going through’.[190]
Veterans
It is estimated that seven percent (1.75 million) of all households in England and Wales contain at least one person who has previously served in the UK armed forces[191].
Loneliness and social isolation are prevalent issues for veterans of all ages. Experiences of loneliness and isolation are linked to various factors including, the transition from military service to civilian life, the geographical mobility of life in the forces, and the disruption of close bonds that are formed during service[192]. Ex-service personnel may also feel socially or culturally isolated because others are perceived not to understand their experiences[193]. This may be more acute for young and middle-aged veterans. SSAFA report ex-military personnel aged 18-49 feeling ‘undervalued’ and ‘misunderstood’ by civilian society[194].
Evidence from the United States points to a connection between PTSD and loneliness[195], and loneliness and social isolation is linked to poor mental health and suicide ideation among veterans of all ages[196]. In the UK, relationship status and socio-economic status have an impact on how lonely or social isolated veterans feel. One study identified key risk factors for poor psychosocial health and wellbeing as ‘not being in a relationship, discharge from military Service for reasons other than end of Service contract, lower veteran rank on discharge and working in lower skilled civilian occupations’[197]. Research also shows a link between discrimination and loneliness. LGBTQ+ populations, women, and UK Commonwealth service personnel, particularly Gurkhas, face discrimination, which can be a profoundly isolating experience[198].
The families of service personnel and ex-service personnel are at risk of loneliness and social isolation due to geographical mobility, poor financial literacy, and caring for veterans with physical disabilities, mental health problems or PTSD[199].
Peer support and a sense of shared identity are important to interventions that support veterans and their families to address loneliness and social isolation. Though initiatives focused on civilians can adapt their services for veterans of the armed forces, an understanding of military culture and the involvement of the military community is essential[200].
In 2021 the census recorded 1,853,112 people (residents 16 years and over) in England and Wales as served in the UK armed forces, of those 32,597 (2%) percent were Surrey veterans. In 2021 32,597 people had reported serving in the UK armed forces, 2.7% of Surrey residents. 72.9% (23,771) of the armed force veterans reported previously serving in the armed forces, 23.7% served in the UK reserve army forces and 4.6% (1,434) had served in both the regular and reserved UK armed forces.
Waverley (13.3%) has the highest proportion of veterans, followed by Guildford (12%) and Reigate & Banstead (11.7%).
Table 33: Table showing the number and percentage of veteran population compared to the population of the district and borough, Census 2021.
| Area name | Previously served in regular UK armed forces (number) | Previously served in reserve UK armed forces (number) | Previously served in both regular and reserve UK armed forces (number) | Has previously served in any UK armed forces (number) | Has not previously served in any UK armed forces (number) | Previously served in regular UK armed forces (percent) | Previously served in reserve UK armed forces (percent) | Previously served in both regular and reserve UK armed forces (percent) | Has previously served in any UK armed forces (percent) | Has not previously served in any UK armed forces (percent) |
|---|---|---|---|---|---|---|---|---|---|---|
| Elmbridge | 2,229 | 829 | 133 | 3,191 | 105,582 | 2.0 | 0.8 | 0.1 | 2.9 | 97.1 |
| Epsom and Ewell | 1,143 | 438 | 90 | 1,671 | 62,935 | 1.8 | 0.7 | 0.1 | 2.6 | 97.4 |
| Guildford | 3,038 | 936 | 164 | 4,138 | 115,218 | 2.5 | 0.8 | 0.1 | 3.5 | 96.5 |
| Mole Valley | 1,965 | 630 | 102 | 2,697 | 69,643 | 2.7 | 0.9 | 0.1 | 3.7 | 96.3 |
| Reigate and Banstead | 2,714 | 924 | 174 | 3,812 | 116,317 | 2.3 | 0.8 | 0.1 | 3.2 | 96.8 |
| Runnymede | 1,494 | 487 | 80 | 2,061 | 70,657 | 2.1 | 0.7 | 0.1 | 2.8 | 97.2 |
| Spelthorne | 1,905 | 495 | 112 | 2,512 | 80,850 | 2.3 | 0.6 | 0.1 | 3.0 | 97.0 |
| Surrey Heath | 2,519 | 584 | 143 | 3,246 | 70,538 | 3.4 | 0.8 | 0.2 | 4.4 | 95.6 |
| Tandridge | 1,727 | 633 | 136 | 2,496 | 68,329 | 2.4 | 0.9 | 0.2 | 3.5 | 96.5 |
| Waverley | 3,261 | 898 | 188 | 4,347 | 99,288 | 3.1 | 0.9 | 0.2 | 4.2 | 95.8 |
| Woking | 1,776 | 548 | 102 | 2,426 | 80,558 | 2.1 | 0.7 | 0.1 | 2.9 | 97.1 |
The highest proportion of veterans is in the 85 and over age group and this is followed by 75-84 age groups. The Reserve group has a larger proportion of 45-59 year age groups. Regular and regular and reserved UK armed forces have less than 1% of the veteran population aged between 16-29 years, compared to the reserve UK armed forces which range from 1% to 3.5%.
Figure 48: Source Census 2021
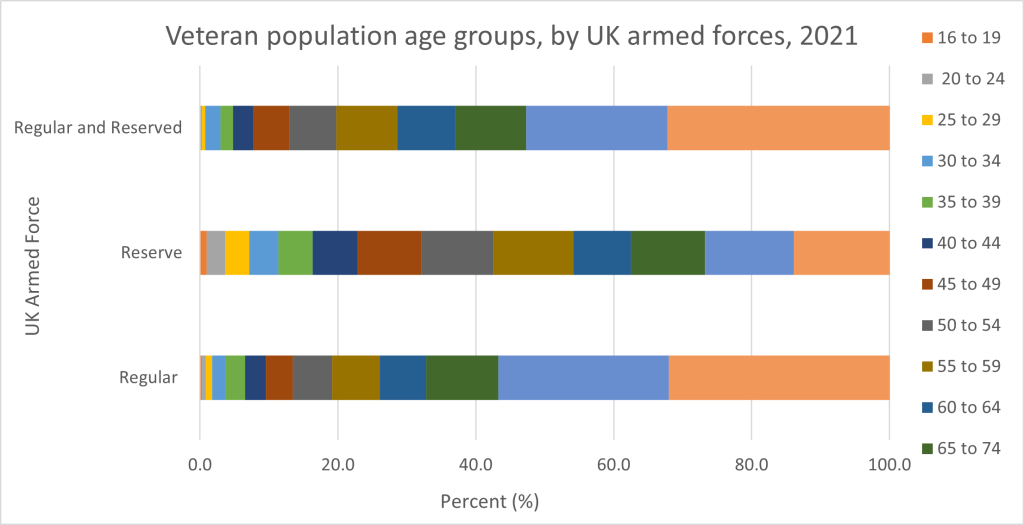
Figure 49: Source: SAPE population, 2020, Connect to Support Surrey – Veterans (search date March 2024).
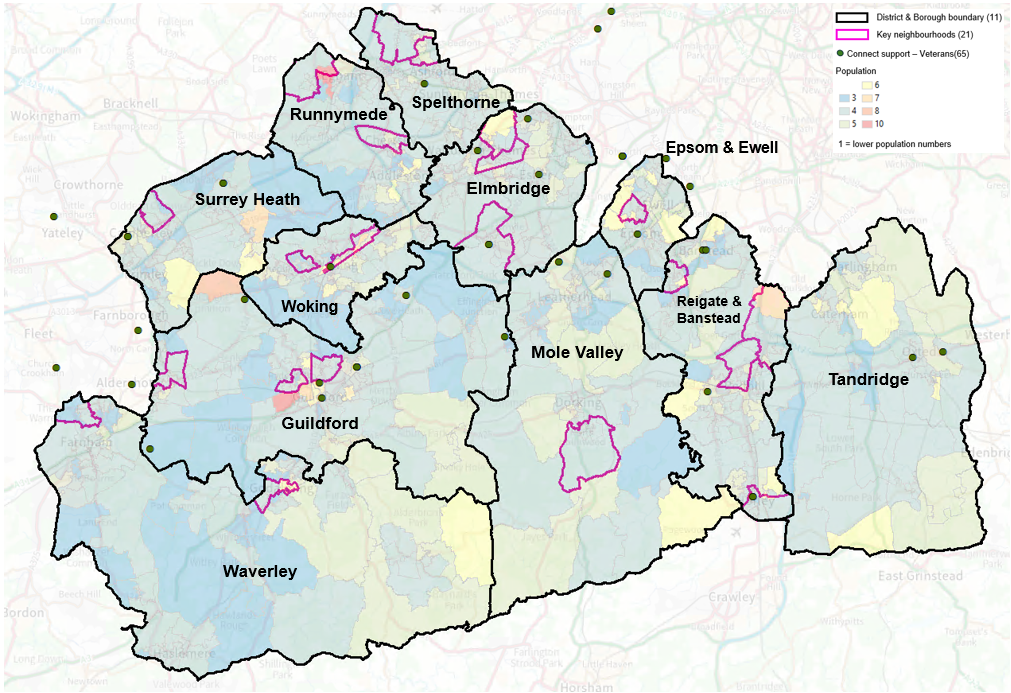
Table 34: Connect to Support services for Veterans
| Area Name | Number of Connect Support Veterans | Online/ telephone service | Total Number of Services |
|---|---|---|---|
| Surrey | 30 | 4 | 34 |
| Elmbridge | 5 | 0 | 5 |
| Epsom & Ewell | 2 | 0 | 2 |
| Guildford | 9 | 2 | 11 |
| Mole Valley | 2 | 1 | 3 |
| Reigate & Banstead | 4 | 1 | 5 |
| Runnymede | 0 | 0 | 0 |
| Spelthorne | 1 | 0 | 1 |
| Surrey Heath | 4 | 0 | 4 |
| Tandridge | 2 | 0 | 2 |
| Waverley | 0 | 0 | 0 |
| Woking | 1 | 0 | 1 |
| Outside Surrey | 18 | 5 | 23 |
| Total | 48 | 9 | 57 |
A JSNA chapter on the Armed Forces Community was published in December 2024: Armed Forces Community | Surrey-i.
Refugees and Asylum Seekers
In the year ending September 2023, over 90,000 people applied for asylum in the UK. 59% of these applicants were males aged 18-49. 13,000 were accompanied children. Over 4,000 applicants were unaccompanied asylum-seeking children[201].
The challenges and barriers that refugees and asylum seekers face around employment, accessing services, cultural differences, discrimination, and stigma increase their individual and collective risk of experiencing loneliness[202]. In 2020, 3 in 10 people who applied for asylum in the UK were women and girls. Many will have experienced gender-based violence and trauma. Pregnant women seeking asylum are particularly susceptible to financial and social isolation, which is disempowering and leads to poor mental health and emotional wellbeing[203]. For accompanied children, not being able to speak English is a barrier to making connections and building relationships that foster a sense of belonging[204].
Meaningful social contact and stable and supportive relationships alleviate loneliness and enhance the mental health and emotional wellbeing of refugees and asylum seekers. For unaccompanied asylum-seeking minors, social isolation is addressed by access to education, which creates new relationships and support networks[205]. Evidence suggests that peer support interventions can be effective in reducing feelings of loneliness in asylum-seeking adults and allows individuals to meet other people in their communities facing similar situations. Peer support groups aid community integration, increase access to community support, and enhance emotional wellbeing[206].
A breakdown of migrants from the different migrant schemes can be found below table[207].
Figure 50: Select Migration Schemes, total numbers
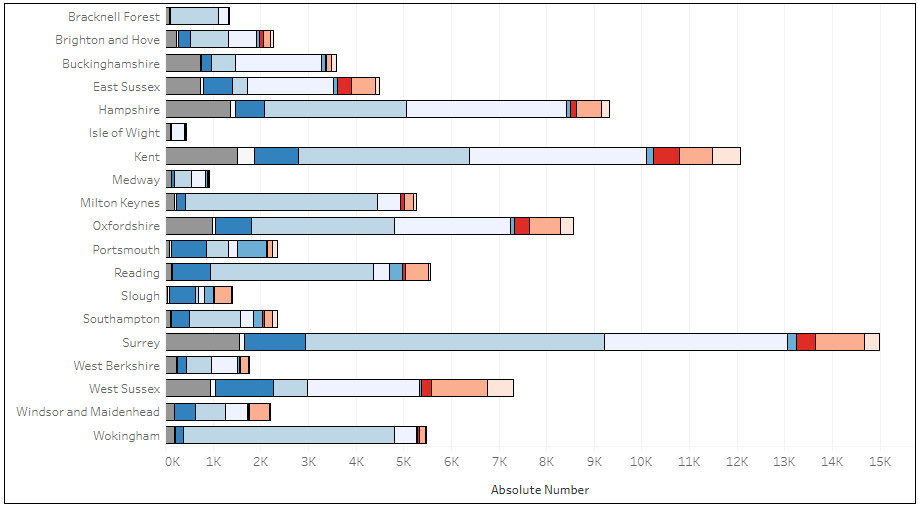

Analysis of the health needs of migrants living in Surrey can be found in the Migrant Health: Rapid Needs Assessment. Meaningful social contact and stable and supportive relationships alleviate loneliness and enhance the mental health and emotional wellbeing of refugees and asylum seekers. For unaccompanied asylum-seeking minors, social isolation is addressed by access to education, which creates new relationships and support networks. Evidence suggests that peer support interventions can be effective in reducing feelings of loneliness in asylum-seeking adults and allows individuals to meet other people in their communities facing similar situations. Peer support groups aid community integration, increase access to community support, and enhance emotional wellbeing[208] , though local authorities ‘should consider how peer support and community initiatives can be accessible to asylum seekers and refugees, who may have difficulties affording public transport, or feel intimidated when they use it.’[209]
Connecting refugees to welcoming community spaces and places.
With the likelihood of increased numbers of displaced people, who often have experienced trauma, a welcoming community serves integration and comfort. Community groups for displaced men and women serve as safe places to make connections, chat, practice English, take part in activities, and bring children along for some time to play.
One of these groups, supported by charity Elmbridge CAN, welcomes women and men from Afghanistan, Syria, Iran, Eritrea, and Ukraine to take part in volunteer-led sessions. Organisers of the project held focus groups to understand common barriers and enablers to social connection and found that building trust is a particularly important precursor to connection, especially among Afghan men. Furthermore, participation in activities was found to be at the heart of the community and helps to embed a sense of home and belonging.
To enable a sense of trust and an opportunity for participation in community spaces, the organisers visited key neighbourhood assets including community gardens, sports clubs, museums, and historical sites, to identify allies and welcoming spaces for these refugees. They agreed opportunities for involvement in activities such as volunteering, ensuring that the community spaces would be welcoming and understanding of the unique situations and challenged that displaced people may bring. A directory of welcoming spaces and places was shared with the women and men, enabling them a choice of activities to support their integration to their new communities.
Men
There is a ‘silent health crisis’ among men in the UK[210]. Men have a lower life expectancy than women. They are more likely to smoke and more likely to drink to excess. Four out of every five suicides are by men. Poor health and wellbeing outcomes for men are mediated by socio-economic inequalities. The gap in healthy life expectancy between men in the most deprived areas of England and those in the least deprived is nearly twenty years. Men are less likely to access traditional health services.
It is estimated that eight million men in the UK feel lonely at least once a week and nearly three million men report feeling lonely daily[211]. Men’s gendered experiences of loneliness and social isolation intersect with other determinants such as ethnicity, age, sexuality and living arrangements[212]. Experiences of loneliness and social isolation, and the help-seeking behaviours of men, are also influenced by expectations of masculinity and maleness[213].
Through the men’s mental health work in Surrey, men have shared that they find themselves grappling with a profound sense of disconnection from the world around them. They struggle to forge genuine connections with others, leaving them feeling isolated and adrift in a sea of loneliness and despair. They have said that pervasive isolation takes a toll on their mental health, leading to a vicious cycle of withdrawal from friends, family, and colleagues. The reluctance to seek help or act further exacerbates their plight, trapping them in a downward spiral of despair[214].
Studies have shown that robust social ties are instrumental in mitigating stress, anxiety, and depression. By fostering healthy habits like proper nutrition, regular exercise, and quality sleep, social connections bolster overall well-being and diminish the risk of suicidal ideation. Yet, despite these benefits, men continue to be disproportionately affected by suicide[215].
A focus group of men from Andy’s Man Club spoke with the JSNA team in April 2024 to share their thoughts on loneliness and social isolation. When asked whether certain life events or stages could act as a trigger, men stated that over-work, poor health and marital breakdown contribute to feelings of loneliness and social isolation. Other key themes emerged:
Changing work patterns since Covid:
“One of my causes of loneliness is working at home. I live alone. I’ve been WFH since pandemic. I’m going round ground hog day. There is no office. If I went to the office I’d be the only one to go. I spend nearly all my time alone. The banter with the Tesco man is the only contact. How did it come to this? I used to have so much fun. I’m stressed from the minute I log on. I’m living on adrenaline with nowhere to unload it.”
“It’s underestimated – the knock-on effect of the pandemic – my daily routine is the same as it was 3 years ago. I’ve suffered depressive episodes and physical pain.”
Relationships:
“I live on my own – was in 17-year relationship that ended. It affected me quite badly. You can have all these connections and still feel isolated.”
“If your needs aren’t met, you can be in company but feel lonely.”
“Socialising can make it worse – I work with younger guys and sometimes we go out for a couple of drinks, and you feel a bit out of the group.”
Cultural loneliness:
Some focus group participants expressed the cultural or existential loneliness they experience as men’s roles in society and in the family change.
“I struggle with what it means to be a man in this modern age.”
“Society is confusing many men – they don’t know what they should be now. A lot of guys are thinking they don’t know where they sit now. They don’t know what their role is.”
“Whatever you do you’re always wrong just because of the body you were born into. You’re always the bad guy. And you’re expected to be self-sufficient and emotionally self-sustaining.”
By raising awareness, breaking down stigmas, and fostering supportive environments, we can empower individuals to seek help and embark on a journey of healing and recovery. In light of these challenges, organisations like Andy’s Man Club, Men’s Pit Stop and Mentell are beacons of hope for men struggling with isolation and mental health issues.
Through their support groups and initiatives in Surrey, they provide a lifeline for those in need, offering a safe space where men can come together to share their experiences, find solidarity, and access resources for healing and growth.
- “Andy’s man club is a service to help reach men. It is so rewarding, and the advice and non-judgemental nature of the sessions means everyone walks away brighter than when they enter.”
- I was very much at the end and had given up on life, through a family member they forced me to attend AMC Woking, it is genuinely life changing, I am not that person I was 8 months ago, I have a future”.
- “I now know I matter”.
Figure 51: Source: SAPE male population, 2020, Connect to Support Surrey – Men only (search date March 2024).
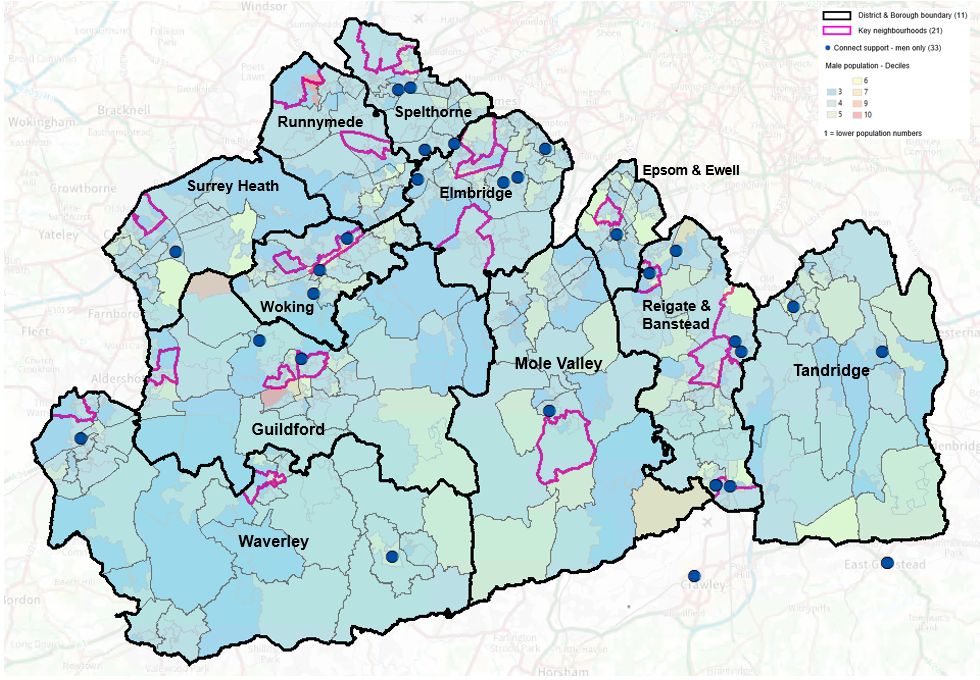
Table 35: Source: SAPE male population, 2020, Connect Support Men only.
| Area Name | Number of Connect Support Men only | Online Service | Total Number of Services |
|---|---|---|---|
| Surrey | 28 | 3 | 31 |
| Elmbridge | 4 | 0 | 4 |
| Epsom & Ewell | 2 | 1 | 3 |
| Guildford | 2 | 0 | 2 |
| Mole Valley | 1 | 0 | 1 |
| Reigate & Banstead | 7 | 0 | 7 |
| Runnymede | 0 | 0 | 0 |
| Spelthorne | 4 | 0 | 4 |
| Surrey Heath | 1 | 0 | 1 |
| Tandridge | 2 | 0 | 2 |
| Waverley | 2 | 0 | 2 |
| Woking | 3 | 2 | 5 |
| Outside Surrey | 3 | 0 | 3 |
| Total | 31 | 3 | 34 |
Physically inactive
People who are physically inactive are at greater risk of loneliness and social isolation, and at the same time, those who are socially isolated are less physically active[216]. This interrelationship between loneliness, social isolation, and physical activity not only impacts on each other, but also on a person’s overall health and wellbeing outcomes.
The health impacts of physical inactivity are also linked to the physical health conditions which contribute to loneliness and social isolation. Up to 40% of long-term health conditions could be prevented by reduced inactivity and adults who exercise regularly have a lower risk of developing many long-term conditions, such as heart disease, type 2 diabetes, dementia, and some cancers[217]. but also can better live with these conditions.
In Surrey almost one in five people – 198,000 adults (aged 16+) – are classified as wholly ‘inactive’, meaning they do less than 30 minutes of physical activity per week[218]. Data from the Active Lives Report shows physical activity levels in Surrey[219].
The table below shows county-wide trends between May 2015 and November 2023. Data is split into three activity levels: ‘Inactive’ (less than 30 minutes a week), ‘Fairly active’ (30-149 minutes a week), and ‘Active’ (150 minutes or more a week).
Figure 52 Activity trends in Surrey 2015-2023 (Source: Active Lives report, 2023)
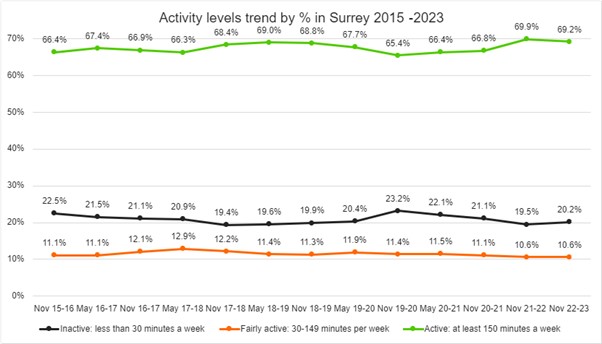
This data can be examined from a district and borough level. For the year from November 2022 to November 2023, the percentage of residents aged 16+ who reported being inactive is shown in the table below. Spelthorne had the highest percentage of inactive residents for that year.
Percentage of residents by district and borough, aged 16+, who are inactive (less than 30 minutes per week)
Table 36: Percentage of residents inactive by district and borough, 2022-2023
| District/Borough | Percentage of residents inactive, 2022 – 2023 |
|---|---|
| Spelthorne | 28.2% |
| Woking | 23.3% |
| Tandridge | 21.7% |
| Mole Valley | 21.3% |
| Reigate and Banstead | 20.4% |
| Surrey | 20.2% |
| Waverley | 20.1% |
| Runnymede | 19.7% |
| Surrey Heath | 18.0% |
| Elmbridge | 17.3% |
| Epsom & Ewell | 17.2% |
| Guildford | 16.8% |
The table below shows our most active residents within the same timeframe by district and borough. Elmbridge, Epsom & Ewell, and Guildford had the highest percentage of active residents.
Percentage of residents by district and borough, aged 16+, who are active (at least 150 minutes per week)
Table 37: Percentage of residents active at least 150 minutes a week by district and borough, 2022-2023
| District/Borough | Percentage of residents active, 2022 – 2023 |
|---|---|
| Elmbridge | 75.3% |
| Epsom & Ewell | 74.5% |
| Guildford | 73.7% |
| Waverley | 71.0% |
| Surrey Heath | 70.9% |
| Mole Valley | 70.3% |
| Surrey | 69.2% |
| Tandridge | 68.7% |
| Runnymede | 67.9% |
| Reigate and Banstead | 65.2% |
| Woking | 64.8% |
| Spelthorne | 57.7% |
Research has shown that physical activity helps tackle loneliness and social isolation. A 2022 research study found moderate and high physical activity lowered the likelihood of loneliness and social isolation in older adults by 15-30%, as well as improve resilience and protective factors[220].
A systematic review examined the links between interventions aimed at loneliness and interventions aimed at physical activity[221]. Researchers sought to understand:
- whether interventions focused on physical inactivity alleviate loneliness.
- whether interventions focused on loneliness increase physical activity.
- whether interventions that target broader levels of physical and mental well-being improve both loneliness and physical activity.
The review found that interventions targeting physical activity can also alleviate loneliness. Some of these benefits may arise from social experiences within the settings.
With around 1 in 3 over 65s falling every year, rising to 1 in 2 amongst those over 80, falls can result in detrimental physical harm, such as hip fractures or broken bones. However, they also cause mental upset – including loss of confidence, independence and increasing anxiety which in turn leads to loneliness and isolation.
To address this issue Active Surrey set out to provide accessible and social falls prevention classes to older people in Surrey, to empower residents to make positive changes to their health and happiness through exercise. In collaboration with Hale Community Centre in Waverley, Active Surrey funded local Otago strength and balance classes to help local older people manage pain, feel more mobile, and reduce their isolation.
Led by a friendly instructor, the classes developed participants strength and balance through gentle exercises on / around a chair, but also- by having coffee after class- encouraged social interaction. This meant that participants were exceedingly committed to the course – with many attending sessions even through injury and illness.
“I enjoy coming. It’s painful straight after the class but I’ve definitely noticed an improvement in my strength and movement as the day goes on.”
“I also enjoy the conversation. I live on my own and can feel quite isolated, so it’s nice to be able to spend time with other people.”
‘’At the start I wasn’t sure how much I’d be able to do. Now I feel I want to keep doing it as it’s been good for my mobility, strength and I enjoy being with others.’’
‘’ After several classes I could feel my leg muscles had improved in strength. I felt less wobbly. I enjoyed the class and getting to know the other people, being sociable and having fun.’’
As a result of the success of the partnership and the commitment of all involved, a regular weekly falls class has been set up at the Hale Community Centre. This was requested by both current participants and newcomers who had heard about the project.
For those that struggle to get out and about, virtual options can provide an option for people to stay physically and mentally active, socially engaged and have fun. One option is the Royal Voluntary Service’s Virtual Village Hall, a free online activity hub that offers sessions from exercise and dance, yoga and meditation to crafts, cooking, and creative writing[222].
National Best Practice
Loneliness interventions fall under four core themes, based on their aims, core components and the mechanisms that lead to loneliness improvements.
Social support: including medium to longer-term and semi-structured to structured social support interventions, or projects that equip individuals with the necessary skills to facilitate social connection. Befriending/mentoring/peer-support programmes, followed by social and emotional skills development were the most common types.
Social interaction-based interventions: Arts/music/culture and social activities with multiple themes are common social interaction programmes. They work to reduce loneliness by increasing opportunities for social contact and growing an individual’s social relationships or network.
Psychological interventions: These provide targeted non-pharmacological therapeutic support/treatment and structured therapy interventions.
There is consistent evidence to suggest that interventions that combine social and psychological support, 8 to 12 week social prescribing link worker schemes, and government funded programmes that provide social activities and support through voluntary sector organisations, work to alleviate loneliness[223].
Local Best Practice
Social prescribing for adults
In 2019 social prescribing link workers were introduced into primary care networks (PCNs) in Surrey to help to address the social, emotional, and practical needs that affect peoples’ health and wellbeing. Social prescribing is a holistic, person-centred approach to health and the wider determinants of health. It recognises that many things that affect health and wellbeing cannot be treated by doctors or medicine alone. In 2022/23, more than 9,000 adults were given social prescriptions in Surrey. Social prescribing connects people to groups, activities, and services within their local community.
Social prescribing is an all-age, whole population approach that works particularly well for people who:
- have one or more long term conditions
- who need support with low level mental health issues
- who are lonely or isolated
- who have complex social needs which affect their wellbeing.
Connecting people to physical activity, arts, culture, creativity, and nature can improve health and wellbeing, reduce loneliness, and empower people to self-manage long-term conditions. Social prescribing can help to address loneliness, social isolation, stress, mild to moderate depression, and anxiety. Evidence suggests that social prescribing can also save costs and reduce pressure on health services by reducing the need for GP appointments and medical prescriptions.
Since 2022/23, PCNs have been encouraged to provide proactive social prescribing to their patients, which means they should work with a population experiencing health inequalities to proactively offer social prescribing interventions.
At national level, social isolation and loneliness were the most common reason for referral to social prescribing after ‘symptoms relating to anxiety and depression’[224]. Referral data for Surrey social prescribing services reflects this national trend.
Figure 53: Chart showing top three referral reasons for each Place within Surrey Heartlands ICB. (Source: Social Prescription Surrey Dashboard, 2023/24 Q2).
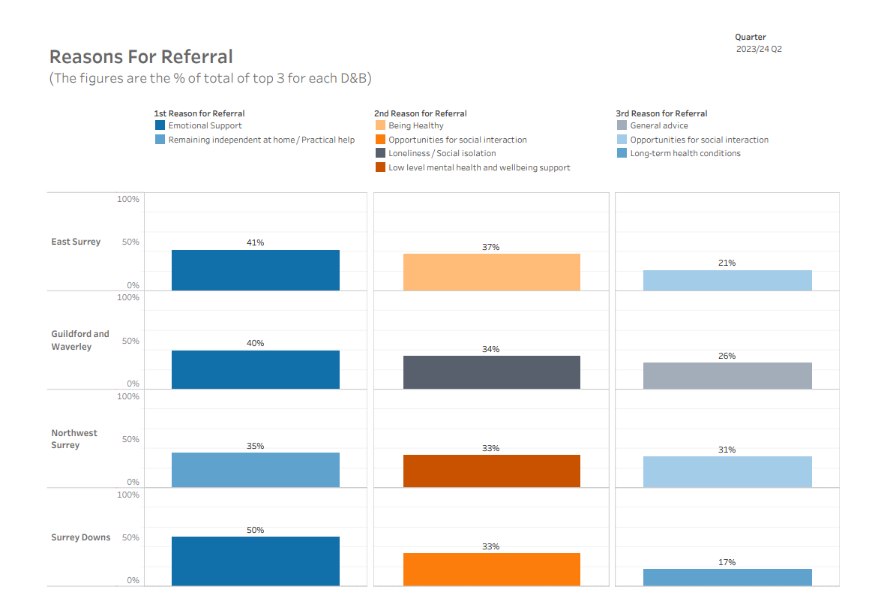
Figure 54: Chart showing age demographics for each Place within Surrey Heartlands ICB. (Source: Social Prescription Surrey Dashboard, 2023/24 Q2).
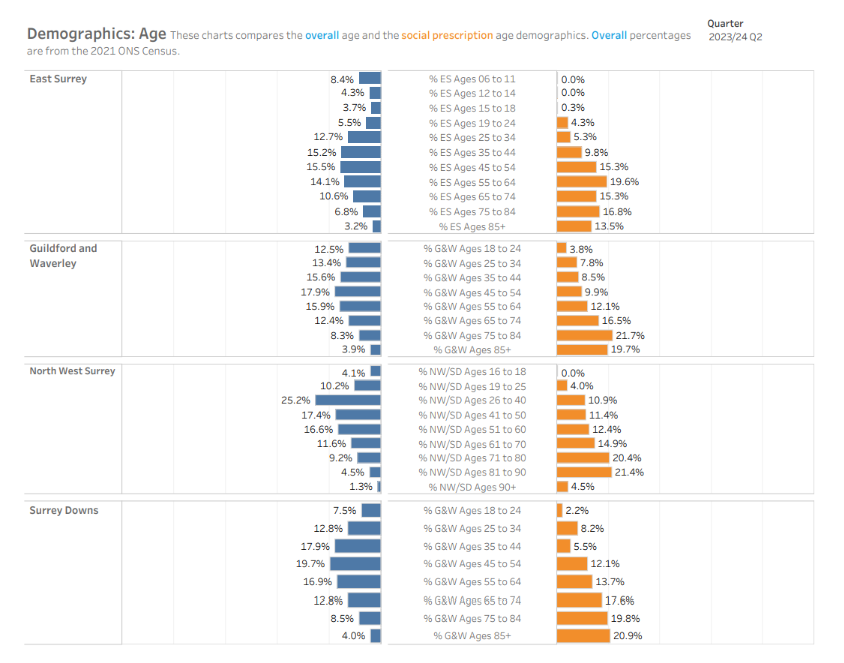
Demographics data suggest that the people accessing social prescribing services in Surrey are most likely to be female and over the age of 65. GPs, who are the main referrers for social prescribing services, may be more aware of the risks to health and wellbeing of loneliness and social isolation for older people. However, more proactive approaches to social prescribing may help to target other populations also at risk of poorer health and wellbeing outcomes due to loneliness and social isolation.
Martin (not his real name) has COPD. His GP had concerns about his anxiety and social isolation, so referred him to social prescribing. Martin thought his life could be better if he spent less time at home on his own watching television, so his link worker shared options that were available to him in his community. This included Men in Sheds and a local coffee and chat group.
His link worker also connected Martin to his local neighbourhood support group. This helped Martin feel much calmer, so he wanted to continue to increase his social contact. Martin visited Surrey’s Virtual Wellbeing Hub and he selected an online coffee morning.
To help his anxiety, Martin’s link worker referred him to a talking therapy service (IAPT) that offered six weeks of free cognitive behavioural therapy (CBT) by telephone. He got on well with his therapist and felt it made a difference to his ability to manage. Martin was very grateful for the support he had received. He no longer felt alone, and he is now looking forward to getting involved with a new community garden project.
Surrey County Council have partnered with the Health and Justice Partnership (Ministry of Justice) to pilot a specialist social prescribing service for prison leavers and adults on Probation. The pilot will address the wider determinants of health for this population of vulnerable adults whom evidence shows experience health inequalities, stigma, and social isolation from friends, family and their communities[225].
Children and young people social prescribing
There are seven specialist children and young people social prescribing link workers in Surrey, who work within either GP surgeries or The Learning Space, which is a children’s mental health charity based in Redhill. Emerging evidence suggests that the benefits of social prescribing for children and young people include alleviating loneliness and improving mental wellbeing. There is also preliminary evidence for the cost benefit of children and young people’s social prescribing[226].
In comparison to adults, social prescribing for children and young people is underdeveloped with fewer services available. However, early evidence suggests that social prescribing is an effective preventative and early intervention service for children and young people with mild or non-clinical mental health problems[227].
Increasing evidence suggests that the sorts of activities that can be socially prescribed, such as involvement in arts, music, social groups, physical activity and connecting more with nature benefits children and young people by improving young people’s development, health and wellbeing[228]. Children’s and young people’s social prescribing may have a positive impact on cognitive performance[229].
Barnardo’s conducted a cost benefit analysis that demonstrates a benefit of £1.80 for every £1 invested in the Cumbria LINK social prescribing service. The analysis finds that social prescribing not only improves mental health and wellbeing outcomes but also reduces primary care appointments[230]. A separate analysis by the Open Data Institute suggests that if social prescribing was operating at a national scale, and reducing GP appointments by 2.5-3%, this could save 2.8-3 million appointments annually[231]. Barnardo’s analysis is based on the interventions and services delivered by Link Workers for children and young people referred with mental health problems. The analysis was unable to account for benefits of the service beyond those of improved mental health and wellbeing. The analysis therefore is likely to underestimate the benefits of social prescribing on education, families, and wider society, but provides valuable insight into the impact of services.
The Green Hub is a local community charity serving residents of Godalming, Milford and Witley, along with the broader Waverley and Surrey areas. A weekly Green Teens programme offers social and therapeutic gardening to stressed, anxious and neuro-diverse young people. The Green Hub provides a safe and non-judgemental environment to learn new skills, meet new people and connect to nature.
Recognising how lonely and isolating it can be parenting a child or young person with mental health or emotional wellbeing needs, The Parent Hub provides an opportunity for parents to talk to other parents, learn new approaches and share experiences in a tranquil environment.
Early Help and Family Support Services
Children and families are also supported in Surrey by an approach called Helping Families Early. Local services work together to support children, young people, and families to receive the right help as soon as a problem emerges. ‘Early help is support for children of all ages that improves a family’s resilience and outcomes or reduces the chance of a problem getting worse. It is not an individual service, but a system of support delivered by local authorities and their partners working together and taking collective responsibility to provide the right provision in their area.’[232] This approach is guided by the Early Help Strategy ‘Families First’ which describes how effective partnership working can ensure families receive the right support at the right time.
Surrey also provides one to one family support, or targeted multi-agency support for families with more complex needs, at home or at one of its family centres which are located across Surrey’s 11 district and borough areas. Further details are available from the Family Information Service.
Surrey’s Healthy Schools initiative is a whole-system, evidence-based approach to promoting physical, emotional and mental health and wellbeing to infant, junior and secondary aged pupils. The Healthy Schools approach aims to empower schools to identify strengths and areas of development. The Surrey Healthy Schools Self-Evaluation Tool has been developed to assist schools in identifying, implementing and developing effective practice.
Green social prescribing
Evidence highlights the benefits of nature to mental health and shows that both contact with nature and connection with nature have a positive impact on health and wellbeing. Living near natural environments is associated with lower stress and faster recovery from mental health issues[233]. Green social prescribing can have a positive impact on loneliness given the bidirectional relationship between mental health and loneliness and social isolation. Peer-reviewed research by the University of Derby[234] on the health and wellbeing benefits of Forest Bathing shows:
- 42% reduction in anxiety (Profile of Moods State )
- 34% increase in nature connection
- 25% increase in social connection.
- 34% improvement in mobility
- 18% improvement in pain.
Green interventions for health and wellbeing have also been shown to deliver a positive return on investment and help to reduce health inequalities. An evidence review commissioned by Natural England found that nature-based initiatives for people with mental health issues gave returns from £2.35 to £10.70 for every £1 invested[235].
Surrey Heartlands ICB was one of seven national ‘test & learn’ sites for embedding and scaling up green social prescribing between 2021 and 2023. Surrey’s green social prescribing programme set out to tackle health inequalities by improving equity of access to green space, address wider determinants of health such as loneliness and social isolation, and empower people to practice self-care by providing opportunities for social connection and skill development. This short film shows how green social prescribing has supported people in Surrey who are socially isolated and unemployed helping them back into employment, training, education, and community life. A site evaluation report can be read here.
Local Area Coordination
Local Area Coordinators (LACs) ‘walk alongside’ people to empower them to connect to their communities, build social relationships, utilise their strengths and skills, and find non-service solutions to the issues that matter to them. They work within Surrey’s key neighbourhoods at a hyper-local level, covering a population of approximately ten to fifteen thousand. As well as providing one to one support for residents, Local Area Coordinators identify common issues or opportunities that require wider action from local agencies, policy makers, or commissioning plans.
Surrey County Council currently employs LACs in:
- Stanwell
- Sheerwater & Maybury
- Goldsworth Park
- Old Dean & St Michael’s
- Horley
- Hurst Green
- Bellfields
- Upper Hale.
Local Area Coordination
Mr C is a British citizen of Pakistani origin who at one stage lived in a 4-bedroom house
in central London with his wife and children. He was working and doing well.
However, unexpectedly he needed to go and stay in Pakistan for 12 years to look after
orphaned family members following the sudden death of his mother and brother. When he returned to the UK in May this year, his life started to rapidly fall apart.
His wife rejected him due to his choice to remain in Pakistan and so he came to Camberley where he knew only one person and he slept on the sofa of her home for 3 months. Following a stroke which left him paralysed down one side Mr C was discharged from hospital into temporary emergency accommodation with only universal credit to live on as he was unable to claim Personal Independence Payments (PIP) at that time as he had been out of the country for too long.
The emergency accommodation was an almost empty room with no bed, other furniture or curtains. This is standard procedure for those moving into this accommodation. For the first few days he slept on the lino floor with his backpack as a pillow, no privacy and no hope. His floating housing support officer managed to get him a broken camp bed and a sleeping bag in the interim and at this point she connected him with me.
When I first met Mr C in August 2023 he was extremely frail, depressed and severely anxious. He cried often and spoke with a heavy sense of loss and hopelessness. In particular when he spoke about his story he focused on the fact he didn’t even have curtains for the windows of his ground floor accommodation and so couldn’t even get changed in his own bedroom. Instead, he had to climb the flight of stairs with his crutch to support him to get the bathroom (ground floor toilet wasn’t working for some time) just so that he could change his clothes. He felt he had no dignity, no hope and no privacy.
During our first meeting I listened to him for 2 hours, telling me about his story, and how he came to be in this situation. He cried, he was angry and he was hurting but by the end of the conversation he said he felt better and that his “heart hurt a little less than this morning”. I made a plan to come back and see him in a few days so we could keep talking and think about how I might support him. He was extremely grateful.
In the time between our first and second meeting I saw that someone locally was getting rid of some net curtains and poles. I contacted them and asked if they would be willing to donate them for free to someone locally who was in great need – they agreed. So when I arrived to see Mr C at our next meeting I came with some curtains for his windows (which by complete luck managed to just about fit the four huge windows!). He was blown away and cried again.
During our second meeting I introduced him to a few different people in the community that I knew and spent time with including local vicar who introduced him to other people in the area and even the barber who warmly welcomed him with a free haircut and beard trim. From this introductions Mr C went on to attend the local community café run at the church and because he is so warm and kind by nature, he made many friends. Through these friends and their contacts, he was provided with a bed, fridge-freezer, dining table, electric blanket and curtains. Volunteers regularly dropped off food bank donations and I supported him (through CAB and the library) to obtain a bus pass which meant he could independently attend more community events as his friendships grew with people.
Work Wise (IPSPC) and Work Well
The Department of Work and Pensions have provided funding to Surrey County Council to deliver Individual Placement and Support in Primary Care (IPSPC) as part of a national vanguard programme, known as Work Wise in Surrey. IPS is an evidenced based employment support method, predominantly delivered for people with severe mental health issues (SMI). Within these settings IPS has shown superior employment and health outcomes, achieving up to twice as many job outcomes compared to traditional programmes. Since 2018, trials have been delivered in the West Midlands and South Yorkshire to test delivering IPS in primary care settings. The success of these trials has led to the IPSPC vanguard programme.
Work Wise is the response to IPSPC funding in Surrey. It is a free employment service available to any person in Surrey with a mental or physical health condition, disability, or neurodivergence, who wants to work. Work Wise supports people to find, maintain and sustain meaningful, long-term paid employment or to support people already in work to continue their employment. The programme aims to ensure adults living with health conditions can access the health and wellbeing benefits of being in secure and meaningful employment.
WorkWell is a new work and health support service that will be rolled out across 15 areas of England, including Surrey, as part of the Government’s plan to help people with health conditions back to work. The service will deliver personalised work and health plans to people in receipt of fit notes from their GP.
WorkWell in Surrey will support residents:
- on sickness absence from work under a fit note.
- referred to primary care mental health services, such as talking therapies, or musculoskeletal interventions such as physiotherapy.
- accessing social prescribing and raising concerns related to their employment.
It will also support individuals personally concerned about their work-related health in special focus populations:
- geographic areas in Epsom and Ewell, Spelthorne, Guildford and Woking, which are also named in CORE20PLUS 5.
- sector specific (health and care, leisure, construction, and driving).
Surrey participants will receive a holistic assessment by a WorkWell Coach, followed by a bespoke package of immediate support from:
- Mental health advisors – one-to-one support to bridge the waiting time for access to existing mental health services.
- Physical activity advisors – providing expertise in safe access to physical activity, including additional assessment.
- Skills and employment advisors – training and skills development opportunities and funding, employer liaison, advice on reasonable adjustments and other employment-based support.
The Surrey pilot expects to support 7,200 people between September 2024 and March 2026.
Libraries
In Surrey, 37.3% of the adult population use a library within a 12-month period. Whilst many older adults use libraries, ‘service use among children and young people is disproportionately high compared to their share of the overall population’ in Surrey [236]. People attend libraries for a variety of reasons beside book borrowing, including adult learning, skills, and social activities.
According to Surrey’s Library and Cultural Service Strategy (2020-2025) library use has been shown to have a range of health and social benefits including ‘socialisation and respite for carers and new parents, improved health literacy through health drop-ins, and reduced loneliness and isolation especially for older people living alone. These benefits can be experienced by ordinary users and volunteer alike. SCC libraries are also adapting libraries to make them more welcoming for children on the autistic spectrum or with dyslexia’.
Libraries also form an important element of the social fabric and can help to create connected and supportive communities. Libraries are places where people have the opportunity to engage through groups, activities, or simply by coming to a public social space. Libraries also function as engagement hubs where local groups meet and display or promote their activities in settings which are neutral, non-commercial, and without faith or political affiliation. This supports the formation of social capital and helps combat social isolation. Libraries provide specialist resources to those who might otherwise be excluded, for example people with sight or hearing loss, learning disabilities, or a long-term illness.
Surrey libraries are the second most visited in the country according to UK Chartered Institute of Public Finance and Accountancy (CIPFA) data, and they play an important role in connecting people to their communities.
“Being able to attend Rhyme Time with my children helped me feel less isolated during maternity leave.”
“The library staff are so kind and friendly, they are sometimes the only people I speak to during the day. I don’t know what I would do without them.”
The CIPFA results show that of the customers who felt lonely 62% felt a visit to a Surrey library helped to reduce feelings of loneliness and isolation[237].
Figure 55 (Source: CIPFA).
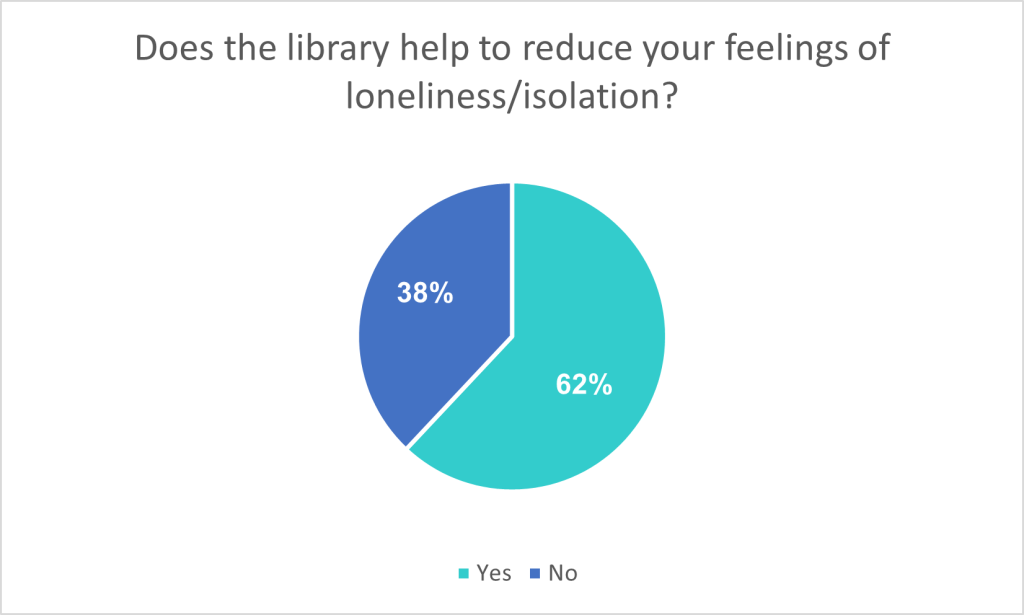
Communities & Prevention Coordinator Service
Surrey County Council’s Communities & Prevention Coordinators (CPCs) work within each of the 11 Adult Social Care locality teams across the county. They take referrals from Adult Social Care teams for social care recipients who would benefit from improving their connection with their local community to reduce social isolation and prevent the escalation of care needs. For the period March 2023 to May 2024, 100% of referrals from Adult Social Care to the CPC Service included ‘social isolation’ as a reason for referral.
The CPCs produce a database of free and low-cost community services for each locality and regular topic specific ‘What’s On’ leaflets. By mapping local assets, CPCs identify gaps in provision and work with Adult Social Care teams to develop community projects that address these gaps. Recent projects include:
- Memory Café (for people with Dementia and their carers).
- Multi-Connections (for refugee and asylum-seeking families).
- Veterans Community Hub.
Mental Health Investment Fund
The Surrey Mental Health Investment Fund (MHIF) is an all-age integrated funding programme with a total budget of £10.5 million providing innovative, community-focused programmes to support the prevention of mental ill health and improvement of emotional well-being across the county. Funding is used to support services which are non-statutory, and developed by local, community-based groups. 22 projects have been funded since MHIF’s launch in 2022.
The table below details MHIF funded projects that directly address loneliness and social isolation.
Table 38: MHIF funded projects that directly address loneliness and social isolation
| Organisation | Project | Delivery |
|---|---|---|
| Merstham Community Facility Trust | Merstham Community Resilience | Three separate projects have been funded under one bid: 1. Starting Point – a support group for adults meeting weekly. Already active however funding will support the provision of supervision for the voluntary facilitators and room rental for a 24 month period to enable this to continue. 2. Support group for children and young people – this is establishing a new group which will be an inclusive, safe space for young people to explore and learn about mental health issues. 3. Expand and enhance Health & Wellbeing Community Champions (HWCCs) provision – currently 4 HWCC and funding will support expansion to 20. |
| Catalyst Support | Catalyst Wellbeing Garden | Funding will be used to establish a gardening space which aims to increase access to nature-based therapy, creating the time and space for bespoke, holistic support. |
| Prospero Theatre Community Interest Company | Creative and Wellbeing Hub | Prospero is an inclusive theatre company, founded in 2015, that uses drama to improve the quality of life for adults and young people with disabilities and mental health challenges. |
| Appeer Community Interest Company | Enhancing the mental health and wellbeing of autistic girls and their parents/carers in Surrey | A project which aims to address the social isolation of young autistic girls, provide early help and resources and support parents and care givers of autistic daughters. |
| Active Prospects | Inclusive Wellbeing Coaches | There is a long-standing gap in MH services for people who have an additional neurodiversity need in Surrey, with people experiencing poorer outcomes and higher levels of suicide. This funding will enable Active Prospects to create a team of 3 Inclusive Wellbeing Coaches (IWCs) to help people aged 18+ with multiple challenges to their wellbeing and MH to attain greater quality of life. |
| Barnardo’s | Barnardo’s Paediatric Parenting Service | The service will provide support to parents/carers of children under 6 years old and who have a diagnosis of, or who are awaiting a diagnosis of, autism and/or ADHD. |
| Emerge Advocacy | Expanding follow-up capacity | Emerge Advocacy supports people aged 10-25 who are in A&E because of self-harm, a suicide attempt or emotional crisis, 7pm – 11pm when many other services are closed, and hospital staff are very busy. The MHIF funding will allow Emerge to expand their post hospital follow up support so that young people and their families do not have to endure long waits for support during their most vulnerable moments. |
| Re-Engage | Reducing Loneliness and Isolation in Over 75s | The MHIF funding will fund an engagement officer to build on Re-engage’s network of referral partners in Surrey and to recruit older people and volunteers into Re-engage’s offer. |
| Richmond Fellowship | Support for Parents of Young Families | The project aims to offer early intervention outreach for parents of young families, focusing on maintaining positive mental health and well-being by enhancing support and social networks. |
| Schools Alliance for Excellence | Nurturing Approach | This project is to support and train 100 mainstream Surrey schools to deliver a graduated approach to nurture, working with nurture UK. There is comprehensive national and international evidence that a whole school nurture approach and nurture groups can make a significant difference to all Children and Young People’s unmet mental health and emotional wellbeing needs but in particular to those children that have specific Social, emotional, and mental health challenges. |
| Sport in Mind | Sport in Mind | Sport in Mind provide 14 weekly sport and physical activity sessions in key locations in Surrey to support people experiencing mental health problems. The therapeutic programmes are non-clinical and are co-designed by people with mental health problems for people with mental health problems. |
| Surrey Care Trust | Steps2Work Wellbeing | Steps2Work Wellbeing, will tackle the mental health of Surrey residents who are unemployed; a group highly vulnerable to mental ill health. The programme will sustainably improve the mental health of the unemployed, combining 1:1 support from trained staff with long-term volunteer mentoring & nature-therapy. |
| YMCA | Step Forward | Step Forward is addressing a gap in service provision for young adults with poor mental health, especially “at risk” groups and those transitioning from child to adult services, who are often left without support at a time when they need it most. Step Forward, offers one to one and group-based support for young people from age 17 through to age 24 (up to their 25th birthday) who have experienced or are experiencing emotional wellbeing and mental health challenges. |
Surrey Connect Bus Service
The Surrey Connect Bus Service has grown from a pilot scheme (funded by the Department for Transport’s Rural Mobility Fund in 2020) to tackle social and geographical isolation in Mole Valley. This Digital Demand Responsive Transport (DDRT) service now runs in Mole Valley, Tandridge, Farnham, Cranleigh, West Guildford and Longcross. It is an all-age service that uses fully accessible minibuses to connect people living in rural areas of the county to nearby town centres, transport links, employment, education, training, and healthcare. The service is priced according to age and miles travelled.
Figure 56: Surrey Connect DDRT zones (darker green areas show the areas where these services run).
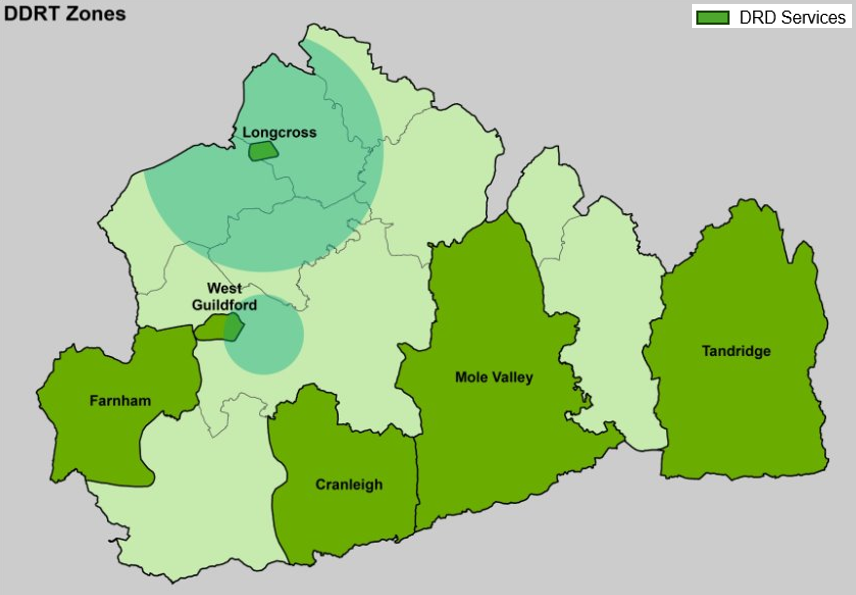
What is this telling us? What are the key inequalities?
Loneliness and social isolation affect everyone. Although loneliness and social isolation tend to be associated with ageing, not all lonely or socially isolated people are older and not all older people are lonely or social isolated. Young people (aged 16-24) are more likely to report feeling lonely than people over the age of 65. Recognising the intersectionality between age-related loneliness and a range of protected characteristics, including gender, sexuality, ethnicity, and health status, is key to understanding how and why people become lonely or social isolated and why for some the experience becomes chronic.
This chapter recognises that the loneliness and social isolation experienced by children and young people – especially those with additional needs or disabilities, emotionally-based school non-attenders, and those on waiting lists for mental health and neuro-diversity assessments (and their families) – is an urgent issue with medium- and long-term implications for the physical health, emotional wellbeing, and socio-economic productivity of a generation.
Loneliness and social isolation are experiences that can occur across the life course, and understanding risk factors based on ‘exposure’, ‘cumulative deficit’ and socio-structural ‘injustice’ is helpful for anticipating and preventing the chronic and severe loneliness and social isolation that is linked to worse health and wellbeing outcomes, reduction in productivity, and increased costs to the health and care system alongside a focus on priority populations and key neighbourhoods. Some population and place trends do emerge:
- Spelthorne consistently emerges as the area of Surrey most in need in terms of population risk factors, community cohesion, and a place-making approach to tackling loneliness and social isolation.
- People with mental health needs and/or poor physical health emerge as being particularly vulnerable to loneliness and social isolation regardless of age or where they live.
- People who are lonely or socially isolated are more likely to experience worse health and wellbeing outcomes, regardless of age or where they live, than people who have good social connections with friends and family.
The bi-directional relationship between loneliness and mental ill health is another key finding of this chapter. People with mental health needs are more likely to feel lonely and experience social isolation than those who do not. Equally, being socially isolated can lead to the development or escalation of mental health concerns.
Bidirectionality between wider determinants and loneliness and social isolation is shown to be relevant also to:
- Poverty/low income.
- Unemployment.
- Physical ill-health.
Loneliness and social isolation can be both a contributing factor and a consequence of each of these wider determinants. For policy makers, this means that the problem of loneliness and social isolation will not be solved separately from the broader health and socio-structural contexts within which people live.
Understanding how good social connection is created and maintained for individuals and for communities is as important as understanding how and why people feel lonely or become socially isolated. The chapter shows that people who maintain good relationships with family and friends are less likely to experience loneliness and social isolation but where people live in connected and supportive communities their resilience to loneliness and social isolation, which may affect anyone over the life course, is likely to be stronger. In other words, empowering thriving and supportive communities is an essential element of addressing loneliness and social isolation, alongside supporting individuals to maintain good social relationships.
The VCSE sector plays a key role in both, and this chapter provides a snapshot of the immense contribution that voluntary and community organisations make to preventing loneliness and social isolation for some of Surrey’s most vulnerable residents.
This chapter makes clear, however, that people who struggle to form social connections (due to childhood experiences, trauma, or mental health) will be less able to access the benefits of connected communities or a thriving VCSE offer without additional psychological support. For this cohort, signposting services are unlikely to result in meaningful outcomes, in terms of addressing loneliness and social isolation, without the provision of additional person-centred services that support people to build confidence through trusted relationships.
‘Existential’ or ‘cultural’ loneliness require a different approach from ‘emotional’ or ‘social’ loneliness. Opportunities to develop meaningful relationships with peers and people who share similar experiences may be more impactful than social activities alone. Recognising personal experiences in the lives of others is a central component of preventing feelings of being existentially isolated from society and the communities in which people live.
Loneliness and social isolation are not caused solely by individual behaviour or addressed only by individual behavioural change. As the social justice model of loneliness makes clear, loneliness is heavily determined by social and structural conditions that render it unequally distributed in society. Initiatives to alleviate loneliness and social isolation must be targeted, therefore, at the structural enablers that create the social conditions in which people can make behaviour change choices. This chapter has identified some of Surrey’s key structural enablers, including public transport, digital access, employment, household income, and inclusive communities.
A place-making approach to communities, and to Surrey’s towns and villages, has a role to play in tackling loneliness and creating the conditions in which social connection can thrive. Evidence shows that the physical environment in which people live can encourage or discourage social connection. Urban road traffic, for example, reduces social contact, increases isolation, and contributes to poorer health and wellbeing outcomes. Conversely, urban environments with better walking, cycling and public transport connectivity support social contact and reduce loneliness[238].
Digital access is a key structural enabler of social connection. As this chapter shows, populations who are digitally excluded are more likely to feel lonely and be socially isolated. Digital is a powerful enabler of social connection for people who face other structural barriers to maintaining social connection. For children and young people, however, digital platforms enable social connection but also feed the emotional and existential loneliness that can leave them feeling left out and isolated.
The VCSE sector makes an essential contribution to fostering social connection and to tackling loneliness and social isolation. Community groups and services provide socialisation opportunities, peer to peer engagement, skills development, and specialist support across the life course. A thriving and sustainable VCSE sector is a vital social lubricant that connects communities and enables the development of personal resilience. In turn, this helps to protect people from the severe and chronic loneliness that is most detrimental to physical health and emotional wellbeing. Understanding who is socially marginalised by structural disadvantage and consequentially excluded from the health and wellbeing benefits of VCSE engagement, however, is of equal importance in terms of addressing loneliness and social isolation for the most vulnerable of Surrey’s residents.
Challenges around access to statutory services and long wait times for mental health support and neurodiversity assessments (particularly for children and young people) can be an isolating experience for individuals and their families that exacerbates feelings of social and emotional loneliness. Surrey stakeholders ranked ‘improved statutory services’ above ‘individual behaviour change’ as an enabler for addressing loneliness and social isolation.
Figure 57: Surrey Loneliness & Social Isolation Stakeholder Survey, January 2024.
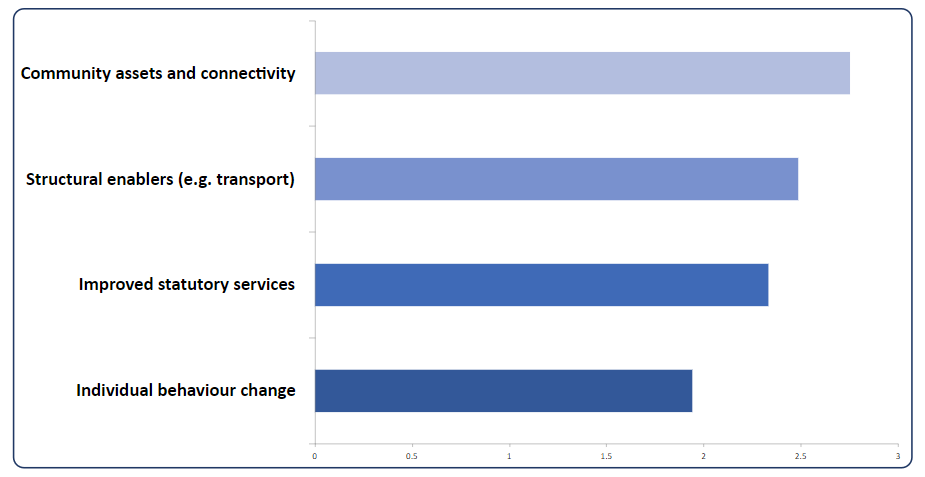
The social stigma associated with feeling lonely can prevent people from talking about their experiences and seeking support. Making sure health and care professionals understand the serious impacts of chronic loneliness on health and wellbeing and have the skills to talk to people about it, may be an important element of system-wide measures to address the issue.
The Surrey Loneliness and Social Isolation Stakeholder Survey asked frontline professionals: ‘As part of your role do you routinely talk to people about loneliness and social isolation?’ Nearly half of respondents said they spoke to people in their care about loneliness and social isolation ‘often’ or ‘always’. 26.67% of respondents ‘sometimes’ did and 4.76% of respondents ‘rarely’ did.
Figure 58: Surrey Loneliness & Social Isolation Stakeholder Survey, January 2024.
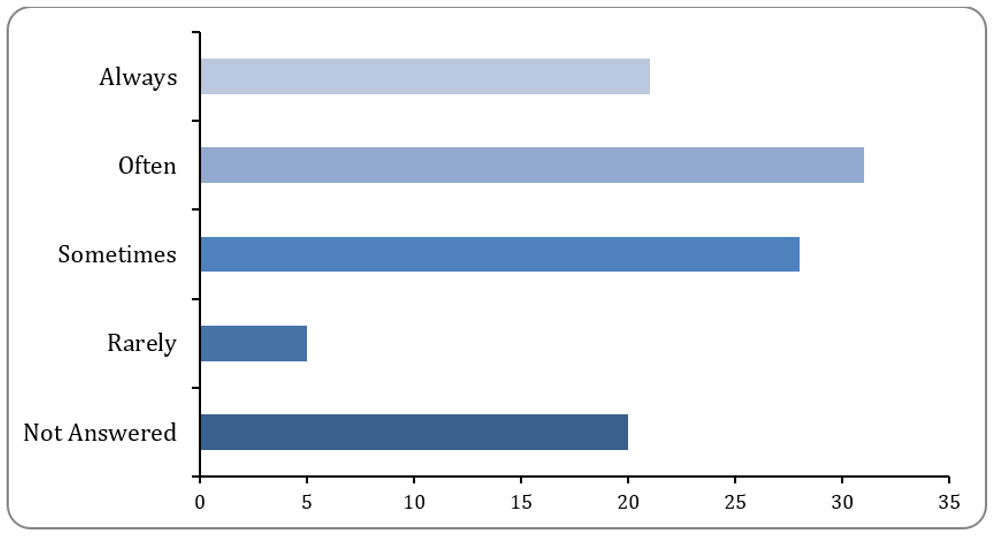
Table 39: Surrey Loneliness & Social Isolation Stakeholder Survey, January 2024
| Option | Total | Percent |
|---|---|---|
| Always | 21 | 20.00% |
| Often | 31 | 29.52% |
| Sometimes | 28 | 26.67% |
| Rarely | 5 | 4.76% |
| Never | 0 | 0.00% |
| Not Answered | 20 | 19.05% |
Friends and family have been identified in this chapter as key ‘actors’ for loneliness and social isolation interventions, so they too should be targeted by any campaigns to reduce stigma, including Surrey’s See Change programme, which has a focus on reducing loneliness.
The intersectionality of loneliness and social isolation with wider determinants of health and wellbeing calls for a whole system approach to tackling its causes and consequences. Loneliness and social isolation arise from social, economic, and structural inequalities that put some individuals at higher risk than others. The poor health and wellbeing outcomes associated with few social connections and poor-quality personal relationships disproportionately affects people who already experience disadvantage.
Social connection – the relationships people have with each other and the feeling of belonging to a community (geographic or otherwise) – is essential to individual health and wellbeing and a fundamental enabler of a healthy society. The findings in this chapter require a whole systems approach to loneliness and social isolation, one in which social connection is a cross-cutting theme – akin to equalities, diversity, and inclusion – informing and shaping strategies, policymaking, and commissioning across integrated care systems.
Recommendations
- System partners recognise chronic loneliness as a structural inequality that should be prioritised as part of Surrey’s broader ambitions to address health and social inequalities. This chapter recommends that a shared plan is agreed at system level at Surrey Health and Well-being Board/ Surrey Heartlands Integrated Care Partnership (HWB-ICP) and at Integrated Care Strategy (ICS) Place so that a coordinated, whole-systems approach can be implemented to address the issue across populations and place and monitor outcomes. Social connection should be prominent in Surrey’s emerging Prevention Strategy Framework.
- Any shared plan at system level adopts a life course approach to tackling loneliness and social isolation, recognising that anyone can experience loneliness and social isolation at any time. A life course approach should also acknowledge that experiences of and resilience to loneliness and social isolation will be mediated by protected characteristics including (but not limited to) health, disability, sexuality, gender, and race as well as by relative social and economic disadvantage.
- The complex intersectionality of loneliness, social isolation, mental ill-health, physical ill-health, disability, and unemployment is recognised and addressed at system and place level to prevent the escalation of poor health and wellbeing outcomes from economic inactivity.
- Surrey would benefit from improving the quality and quantity of its data on loneliness and social isolation so that there is deeper understanding at system, place, and neighbourhood levels of who is lonely or isolated, when and why people experience loneliness, and which initiatives show best outcomes and value for money. For example, Surrey should consider monitoring the Loneliness Index (GP Prescriptions for Loneliness) to track rates of loneliness at ward level and consider its inclusion as an indicator within the Health and Wellbeing Strategy Index. Further qualitative data is required for some population groups including men, LGBTQ+, recent ex-service personnel, farmers, and those who experience legal barriers to civic participation (refugees, asylum seekers, and all sanctuary-seeking peoples).
- Social connection should be recognised by system partners and at Place as a cross-cutting theme akin to equality, diversity, and inclusion. Funding decisions, changes to statutory services, and plans for community initiatives should be assessed for their impact on enabling or prohibiting social connection, particularly for vulnerable groups.
- The structural enablers of social connection – environment, transport, inclusive communities, digital skills – should be recognised and championed at system, place, and neighbourhood levels through strategies, policies, funding decisions and place-making approaches.
- The loneliness and social isolation experienced by children and young people – especially those with additional needs or disabilities, emotionally-based school non-attenders, and those on waiting lists for mental health and neuro-diversity assessments (and their families) – must be addressed through the delivery of the Children & Young People’s Emotional Well-being and Mental Health Strategy to protect the physical health, emotional wellbeing, and socio-economic productivity of a generation.
- The services, groups and activities delivered to communities by the VCSE sector is acknowledged as integral to a whole-system approach to tackling loneliness and social isolation. The VCSE should be supported to become inclusive so that all populations – including the most vulnerable – share in its social connectivity. Impacts on social connection should be considered as part of any decision-making process about cuts to VCSE funding.
- Services that connect people to their communities should ensure that they provide meaningful signposting, giving people appropriate time and support to build confidence to access community provision. Sign-posting services should take an asset-based approach that focuses on strengths and the contribution people can make to their communities. Sign-posting services must recognise that cultural or existential loneliness may require a different approach from emotional or social loneliness.
- Surrey must make a commitment at system level to reducing the stigma associated with loneliness and social isolation, particularly regarding protected characteristics and vulnerable groups, where stigma may prevent someone from seeking help and support. Surrey health and care professionals should be supported to develop the necessary skills and knowledge to have conversations about loneliness and social isolation as part of their everyday practice.
Lead Contributors
Lead author: Jane Soothill
Contributing authors: Helen Rotonen, Jason Lever
Acknowledgements
The authors are grateful to Karen Skinner (REDHILL, UK: Surrey and Sussex Library and Knowledge Services) for the following evidence searches:
- LSI: Older people 80+ and those in care homes. Karen Skinner. (1st May, 2024).
- Evidence search: LSI: People with long term health conditions, disabilities or sensory impairment. Karen Skinner. (1st May, 2024).
- Evidence search: LSI: Carers and young carers. Karen Skinner. (1st May, 2024).
- Evidence search: LSI: People with serious mental illness. Karen Skinner. (1st May, 2024).
- Evidence search: LSI: Adults with learning disabilities and/or autism. Karen Skinner. ( 1st May, 2024).
- Evidence search: LSI: People experiencing homelessness. Karen Skinner. (2nd May, 2024).
- Evidence search: LSI: LGBTQ+ population. Karen Skinner. (3rd May, 2024).
- Evidence search: LSI: Unemployment/economically inactive. Karen Skinner. ( 7th May, 2024).
- Evidence search: LSI: Men. Karen Skinner. (7th May, 2024).
- Evidence search: LSI: Retirement aged. Karen Skinner. (7th May, 2024).
- Evidence search: LSI: Refugees and asylum seekers. Karen Skinner. (8th May, 2024).
- Evidence search: LSI: Veterans. Karen Skinner. (8th May, 2024).
- Evidence search: LSI: Bereaved. Karen Skinner. (8th May, 2024).
- Evidence search: LSI: Children & Young People with additional needs and disabilities. Karen Skinner. (9th May, 2024).
- Evidence search: LSI: Emotionally-based school non-attenders and CYP excluded from school. Karen Skinner. (9th May, 2024).
- Evidence search: LSI: Children & families on waiting lists for MH or ND assessments. Karen Skinner. (9th May, 2024).
- Evidence search: Causes of and impact on Health & Wellbeing of Loneliness and Social Isolation. Karen Skinner. (9th May, 2024).
Appendices
Appendix 1: Focus Group discussion guide.
Loneliness & Social Isolation Focus Group Discussion
Guide for Facilitators
April – May 2024
Date: 15th April 2024 (10:30 – 12:30)
Location: via Teams
Attendees: Surrey Coalition for Disabled People (Virtual Cafe) – number TBC – approx. 5-8
Welcome and session briefing
| Timing | Discussion | Comments |
|---|---|---|
| 5 mins | Opening: Thank you for agreeing to take part in this focus group today, I’m excited to chat with you and I really appreciate your willingness to participate in the research for the JSNA Chapter. Why we are here: We’d like to ask you some questions about your perspective of peoples’ experiences of loneliness & social isolation when they have mental health needs. We’d also like to hear about any challenges you may have encountered, anything that has worked well, and your thoughts around gaps and improvements in support. What you tell us will be used to used help to inform the Loneliness & Social Isolation JSNA Chapter. Through the session today we will be speaking about: – Your perspective on LSI among people in Surrey who are disabled or have sensory impairments. – Your experiences of LSI. – Causes of LSI for people who are disabled or have sensory impairments. – Positive approaches to LSI in Surrey. – Hopes for the future of support including suggestions for improvement. Ethics: – As part of this focus group, we would like to ask you to share your experiences and opinions as much as you feel comfortable doing so. – You don’t have to answer any questions that you don’t feel like answering/ you don’t have to share any experiences or feedback if you don’t want to. You can leave the group at any point. – There are no right or wrong answers, and you can say as little or as much as you like. This is an informal chat to gather your thoughts and feedback. – Everything you say is confidential. – Your name/identifiable information won’t be linked with anything that you say in this session, you will remain anonymous when we come to write up any findings. Group rules: – It’s important that we listen to each other and agree that there are no right or wrong answers. It’s ok for people to have different opinions. – Please keep everything you hear confidential. – Give everyone space and time to talk. – Please do ask questions if things aren’t clear. We’ve got about 30 minutes today but if you’d like to pause at any time or take a break then please do so. Please do feel free to jump in and talk whenever. [IF ONLINE] if you’d prefer you can also use the reaction functions to raise your hand or pop any comments or questions in the chat function too. Final questions before starting: – We would like to record the session today – are you all happy for this to be recorded? – Do you have any questions before we get started? |
If online: Participants to message in the chat function if issues with connection. Facilitators will aim to support and resolve any problems. |
Introduction
| Timing | Discussion | Comments |
|---|---|---|
| 5 minutes | Let’s kick-off with some quick introductions: – Would you like to start by introducing yourself, and maybe tell me one thing about yourself – a hobby or unusual fact? |
Introductions in the chat if more than 5 people. |
Your perspectives of LSI among people in Surrey with experience of mental ill-health
| Timing | Discussion | Comments |
|---|---|---|
| 10 minutes | – Thinking about yourself and/or the people you know in Surrey how do you think physical disability affects loneliness & social isolation? – To what extent would you say the LSI experiences of people who are physically disabled are understood? – How would you describe the health & wellbeing impacts of feeling lonely or being socially isolated? |
Note to participant: this doesn’t need to be your experience but maybe you know people with experience or have a view to share. |
Your experiences of LSI
| Timing | Discussion | Comments |
|---|---|---|
| 5 minutes | Reflecting on your own experiences, to what extend is LSI something you feel, think about, or worry about? Is it something you’ve experienced at a particular time in your life or something you feel you might experience in the future? | n/a |
Causes of LSI for people who are physically disabled
| Timing | Discussion | Comments |
|---|---|---|
| 15 minutes | We’re now going to move on to some questions around the causes of loneliness & social isolation for people who are physically disabled or have sensory impairments. – From your experience, and the experiences of people you know, what are the key causes of LSI for people who are physically disabled? – From your experience, and the experiences of people you know, what are the key barriers to disabled people feeling less lonely or socially isolated? – When you think about feeling connected to other people, what does good social connection look like for you? |
E.g., mental health, cost of living, social media, stigma, housing & transport, community facilities, COVID-19 etc. e.g., can you be sociable but still feel disconnected from peers? Which social connections stop you from feeling lonely? (Peers, friends, family) |
Positive approaches to LSI among physically disabled people
| Timing | Discussion | Comments |
|---|---|---|
| 5 minutes | Reflecting on positives, can you share any examples of what you think is working well in Surrey in terms of supporting physically disabled people to have good social connections? | n/a |
Looking forward (Improvements)
| Timing | Discussion | Comments |
|---|---|---|
| 10 minutes | – From your perspective, is there anything that could be done differently to improve support for people who are physically disabled and lonely or social isolated? Or to prevent disabled people from becoming lonely or socially isolated? (Probe: Are there any specific areas with gaps?) – Thinking about improvements to support, are there any factors that you think have the potential to prevent or hamper change? |
E.g. how can physically disabled people be supported to develop good social connections? |
Closing
| Timing | Discussion | Comments |
|---|---|---|
| 5 minutes | Thanks for taking the time to talk to us. It has been interesting and very useful. Just before we end, is there anything else you’d like to share before we draw the session to a close? | n/a |
END OF DISCUSSION
Appendix 2: Community Dynamics datasets for Surrey’s Key Neighbourhoods
The charts below show the Community Dynamics datasets for each of Surrey’s Key Neighbourhoods.
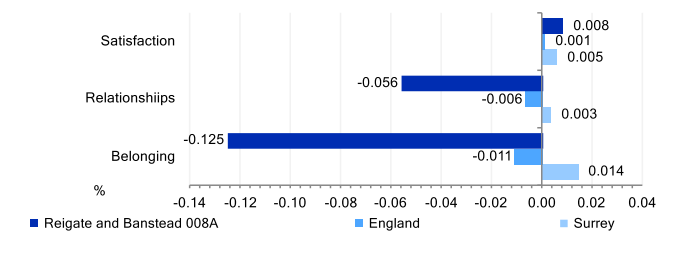
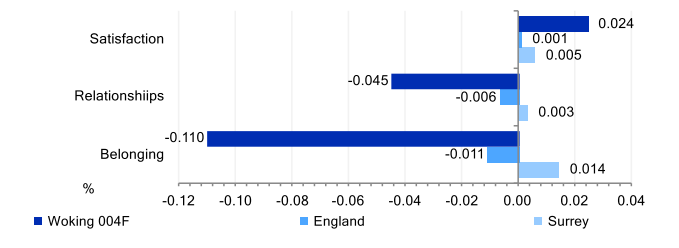
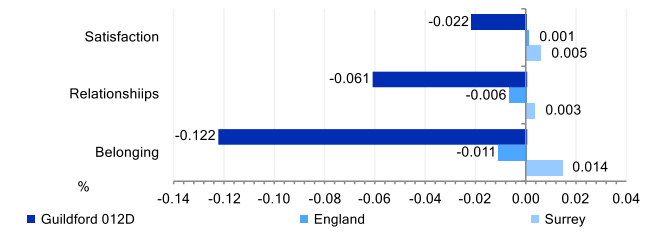
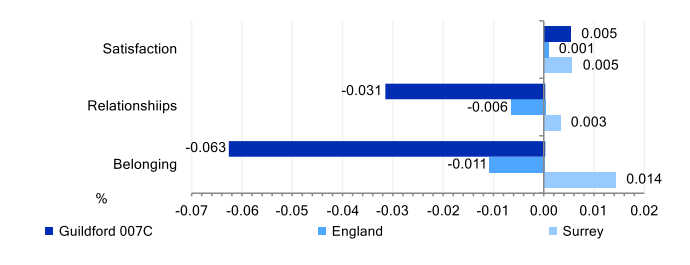
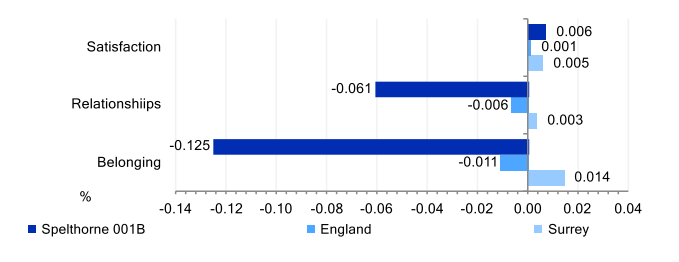
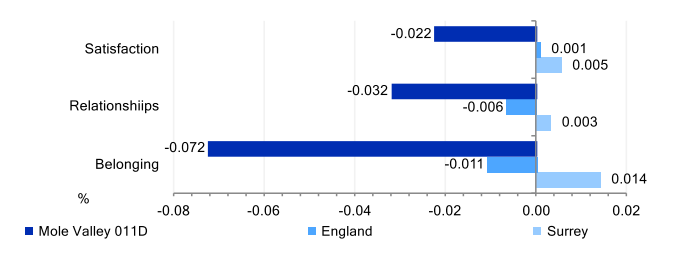
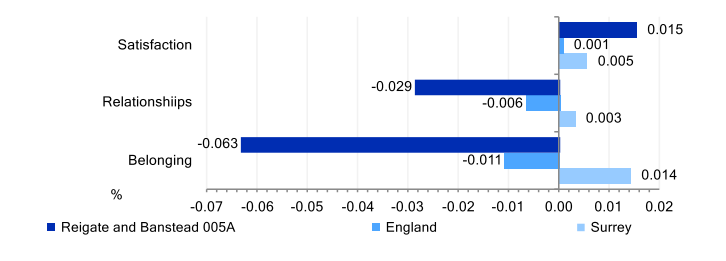
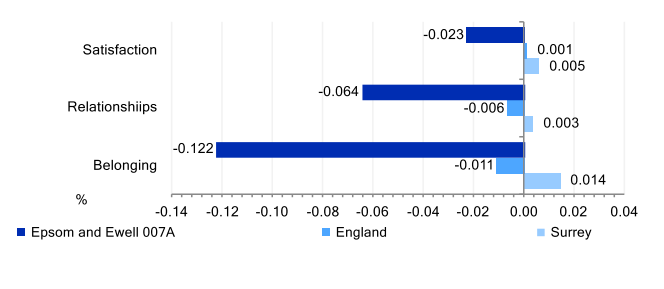
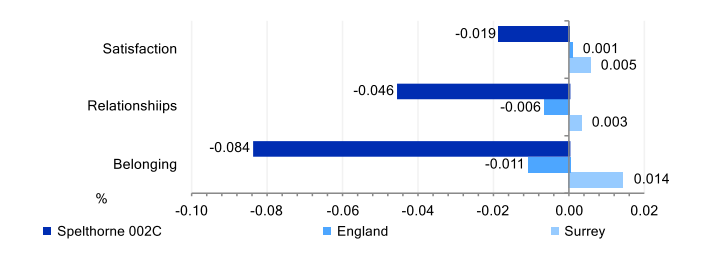
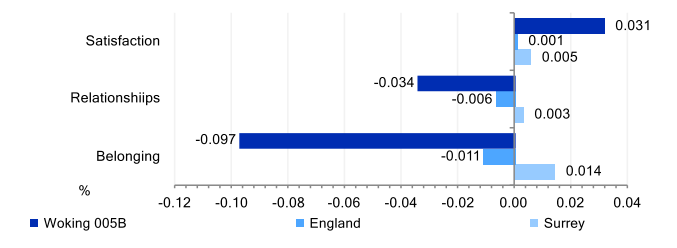
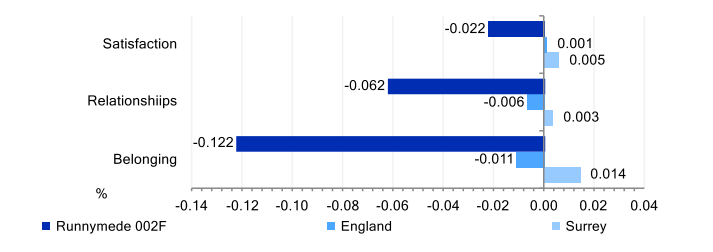
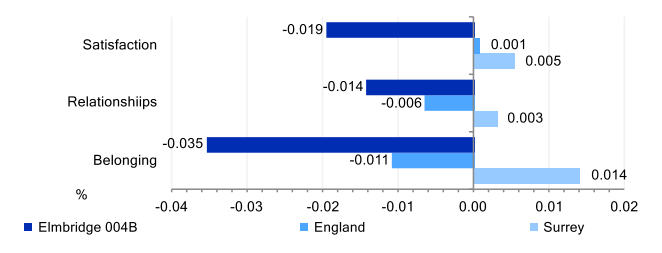
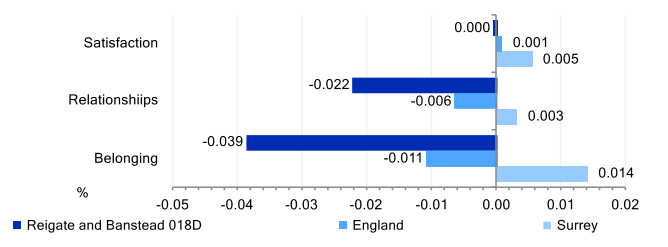
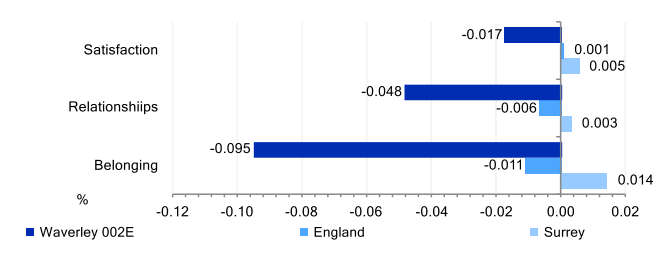
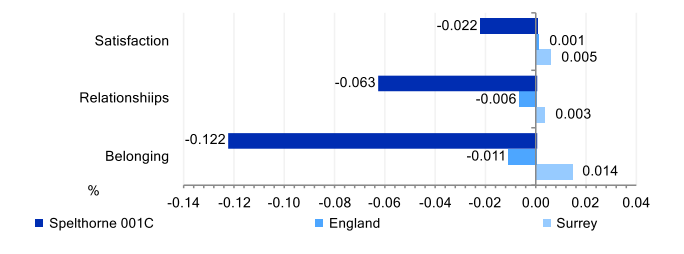
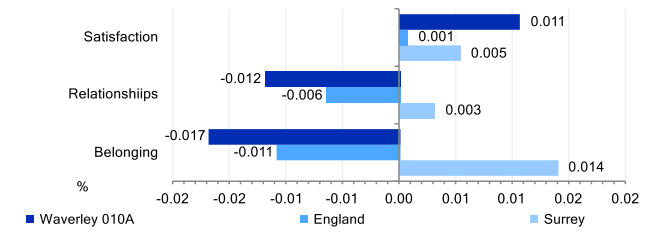
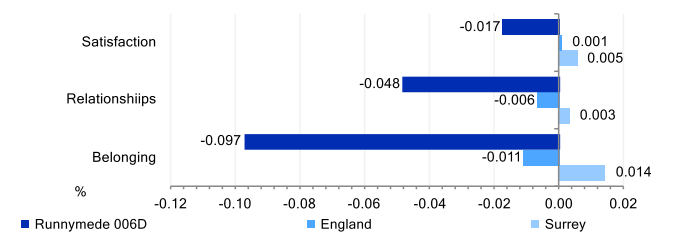
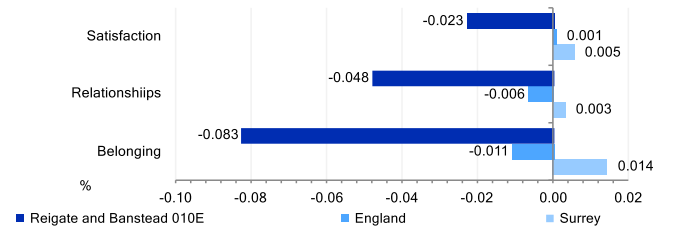
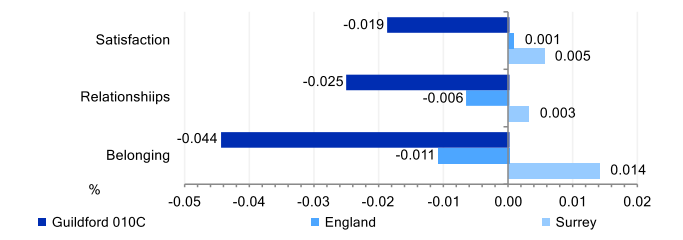
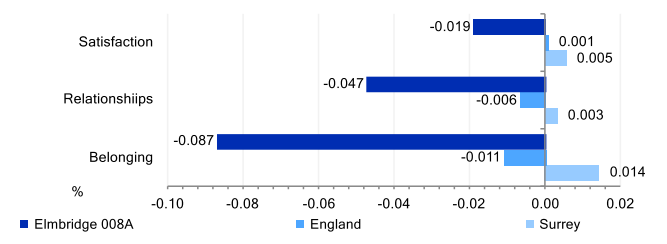
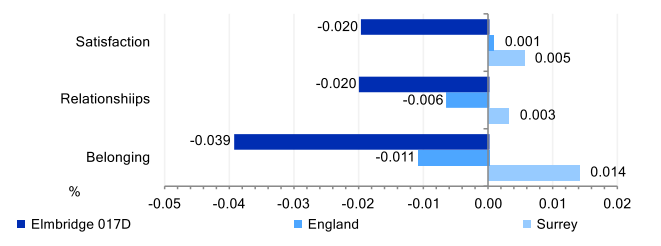
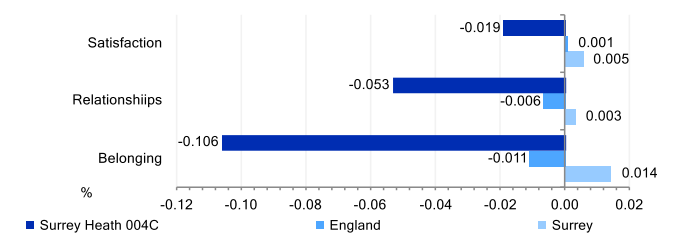
Appendix 3: Community Needs Index scores for Surrey’s Key Neighbourhoods
The charts below show the Community Needs Index Scores for each of Surrey’s Key Neighbourhoods.
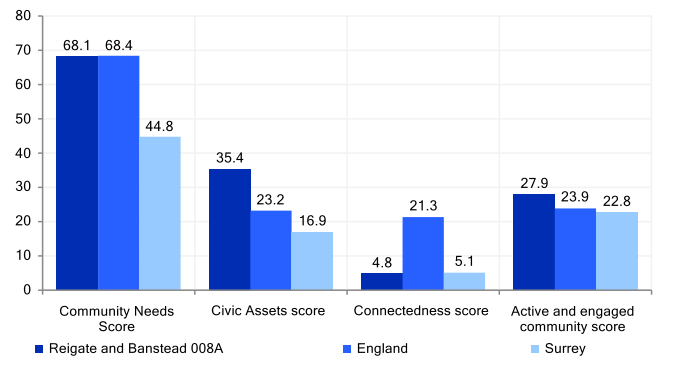
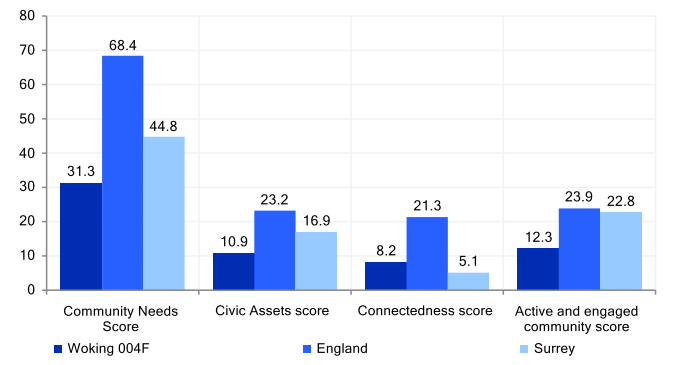
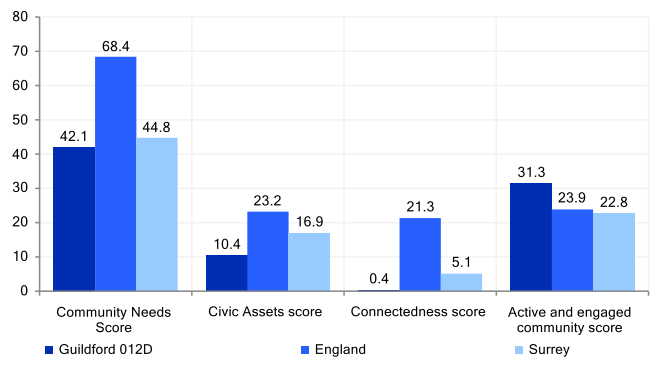
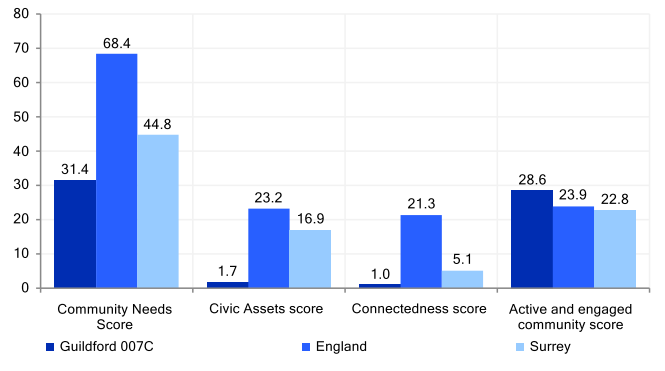
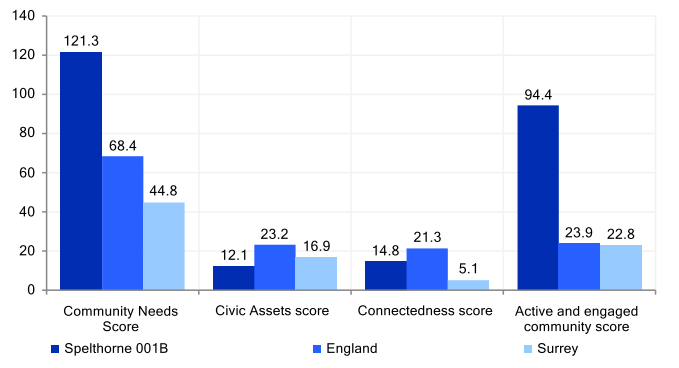
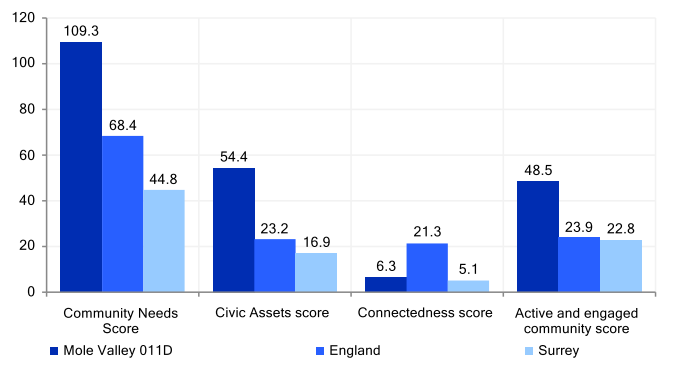
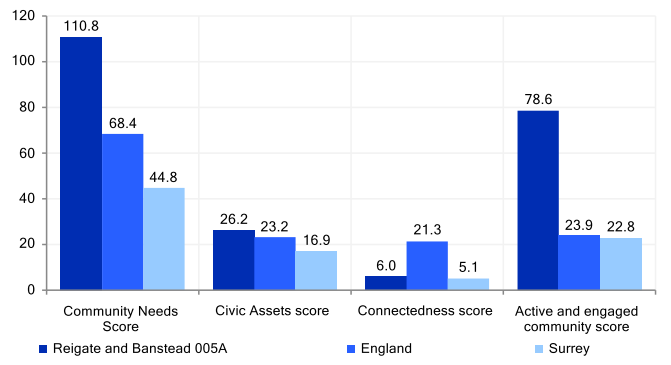
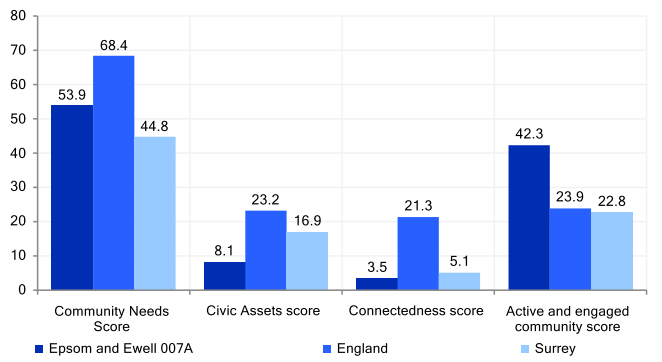
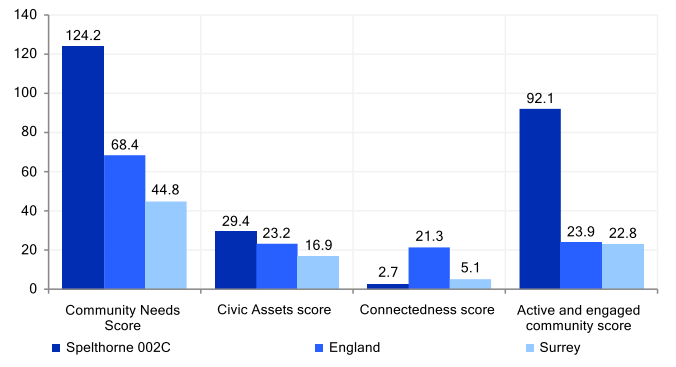
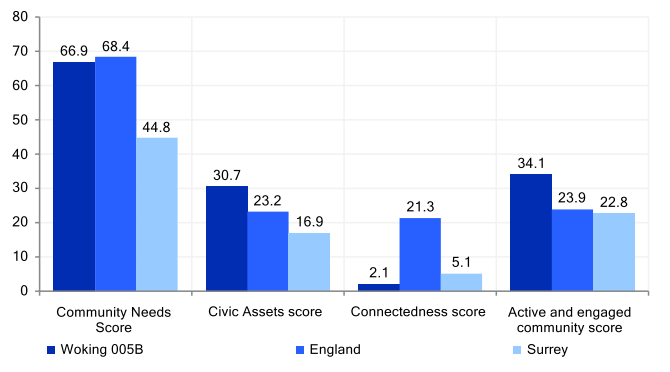
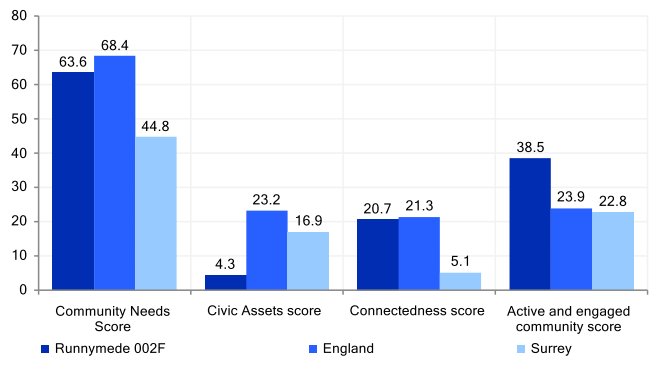
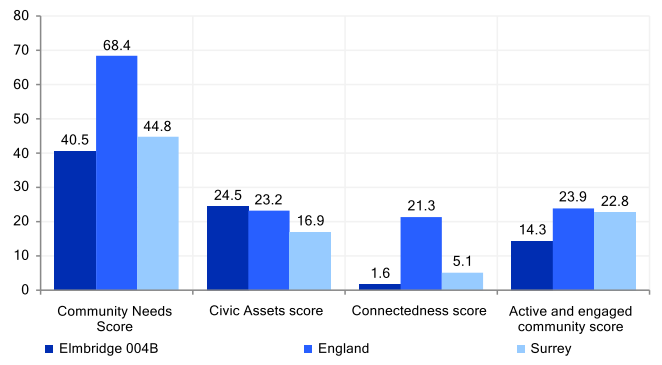
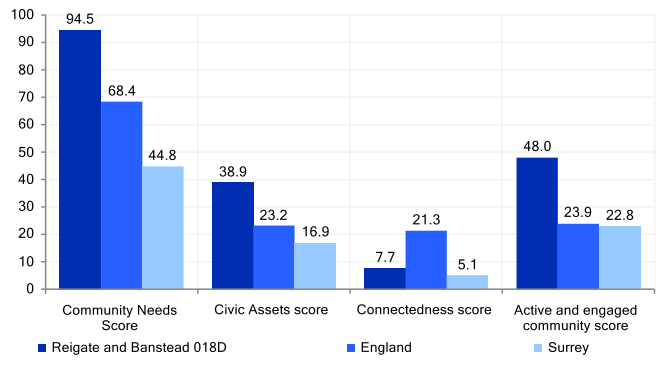
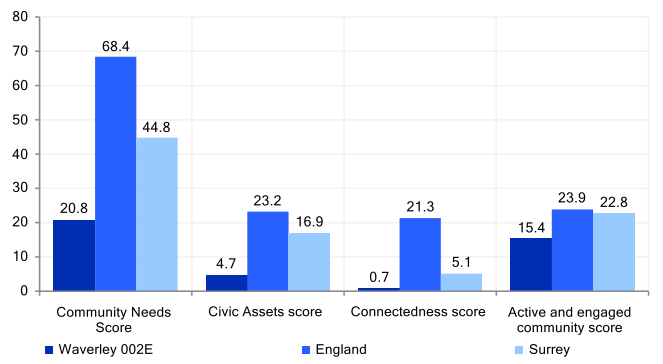
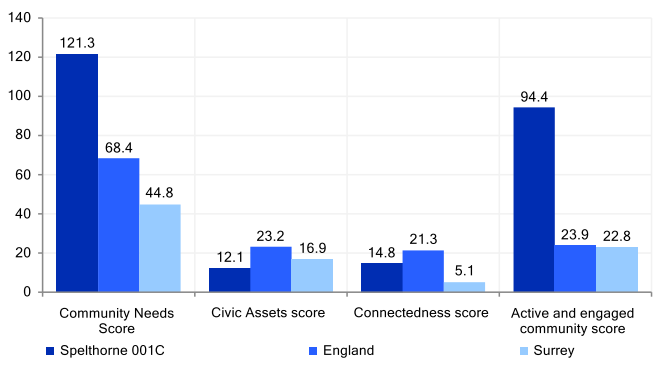
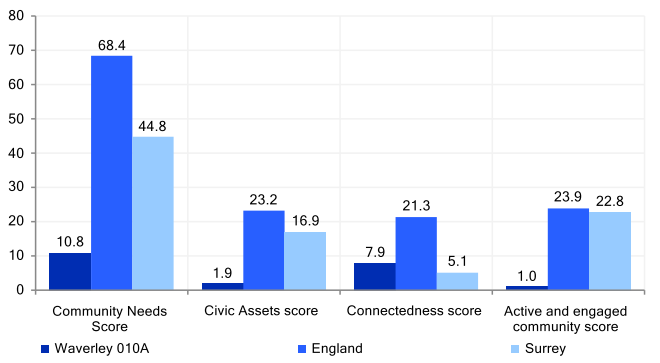
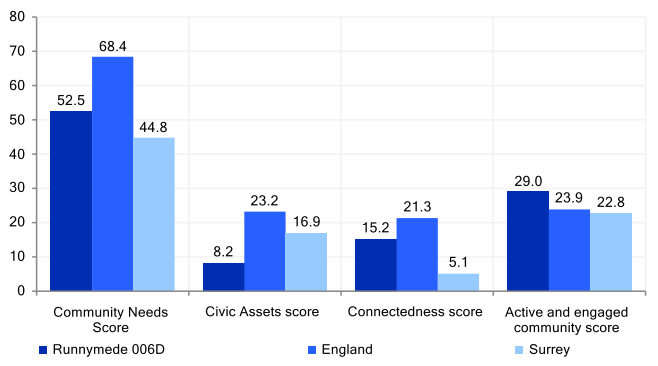
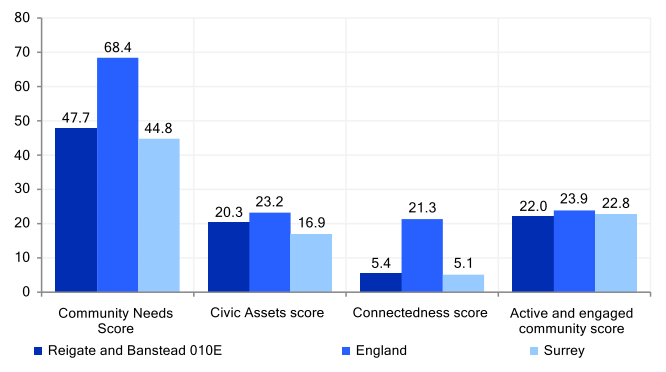
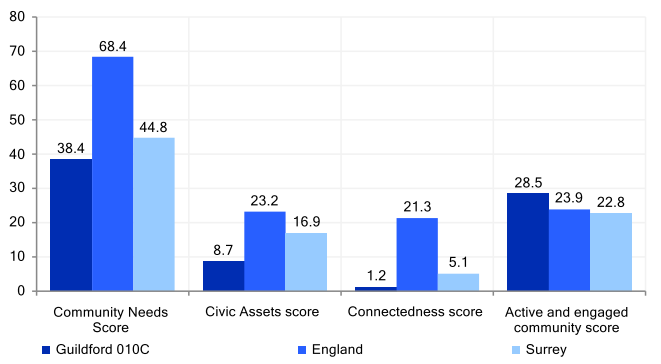
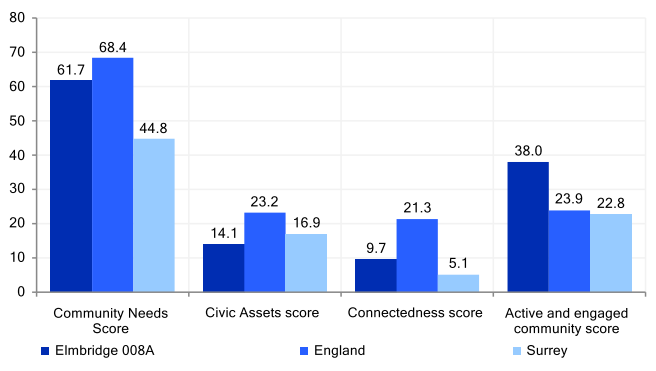
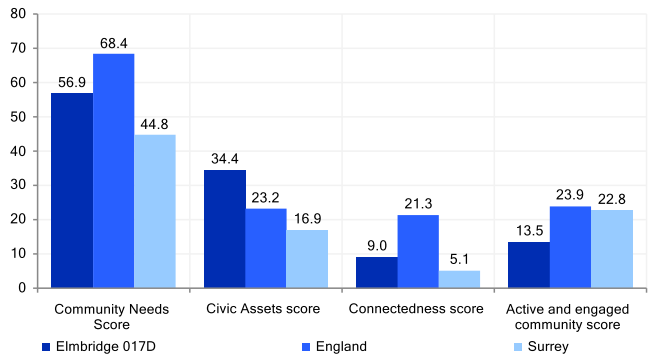
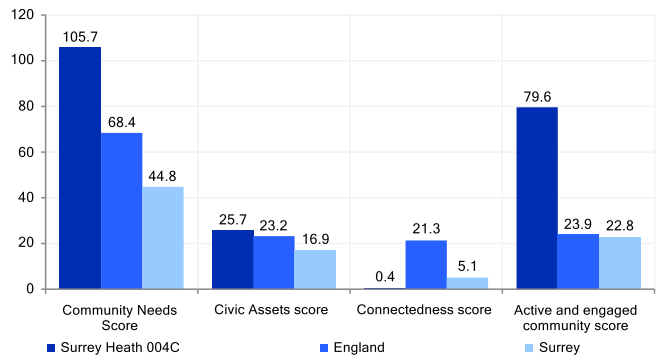
References
[1] Surrey Health and Well-Being Strategy – update 2022 | Healthy Surrey
[2] Combating loneliness: a guide for local authorities
[3] loneliness-report_final_2409.pdf (ageuk.org.uk)
[4] Department for Digital, Culture, Media & Sport, A connected society: a strategy for tackling loneliness, 2018
[5] Facts and Statistics | Campaign to End Loneliness
[6] Facts and Statistics | Campaign to End Loneliness
[7] Wu, B. ‘Social isolation and loneliness among older adults in the context of COVID-19: a global challenge’, Global Health Research and Policy 5.27, 2020
[8] Tackling loneliness evidence review: main report – GOV.UK (www.gov.uk)
[9] Tackling loneliness evidence review: main report – GOV.UK (www.gov.uk)
[10] D Spini et. al. ‘Vulnerability across the life course’, Research in Human Development, 14 (1), 1-4, January 2017.
[11] Tackling loneliness evidence review: main report – GOV.UK (www.gov.uk)
[12] Manuela Barreto, David Matthew Doyle, Pamela Qualter, ‘Changing the Narrative: Loneliness as a social justice issue’, Political Psychology, 6th March 2024 .
[13] Lynne Murray and Liz Andrews, The Social Baby: Understanding babies’ communication from birth, CP Publishing, 2005.
[14] Tackling loneliness evidence review: main report – GOV.UK (www.gov.uk)
[15] A Conceptual Review of Loneliness in Adults: Qualitative Evidence Synthesis – PMC (nih.gov)
[16] An overview of systematic reviews on the public health consequences of social isolation and loneliness – ScienceDirect
[17] Valtorta et al., ‘Loneliness and social isolation as risk factors for coronary heart disease and stroke: systematic review and meta-analysis of longitudinal observational studies’, Heart 102 (2016) (pp. 1009-1016)
[18] Hawkley, et al., ‘Loneliness predicts increased blood pressure: 5-year cross-lagged analyses in middle-aged and older adults’, Psychology and Aging 25.1 (2010), p.132.
[19] Hackett, Hudson and Chilcot, ‘Loneliness and type 2 diabetes incidence: findings from the English Longitudinal Study of Ageing’, Diabetologia 63.11 (2020) (pp. 2329-2338).
[20] ‘Is equity considered in systematic reviews of interventions for mitigating social isolation and loneliness in older adults?’ Madani Mohamad Tarek, Madani Leen, Ghogomu Elizabeth Tanjong, Dahrouge Simone, Hébert Paul C., Juando-Prats Clara, Mulligan Kate, Welch Vivian. BMC Public Health, 2022
[21] https://www.who.int/teams/social-determinants-of-health/demographic-change-and-healthy-ageing/social-isolation-and-loneliness
[22] McClelland, H., Evans, J. J., Nowland, R., Ferguson, E., & O’Connor, R. C. (2020). Loneliness as a predictor of suicidal ideation and behaviour: a systematic review and meta-analysis of prospective studies. Journal of affective disorders, 274, 880–896. https://doi.org/10.1016/j.jad.2020.05.004
[23] The National Confidential Inquiry into Suicide and Safety in Mental Health (NCISH). Suicide by middle-aged men. 2021. The University of Manchester. https://documents.manchester.ac.uk/display.aspx?DocID=55305
[24] Suicide by children and young people. National Confidential Inquiry into Suicide and Homicide by People with Mental Illness (NCISH). Manchester: University of Manchester, 2017. Suicide in Children & Young People 2017 (manchester.ac.uk)
[25] Social isolation could cause physical inflammation | University of Surrey
[26] Jetten, J., Haslam, C., & Haslam, S. A. (Eds.). (2012). The social cure: Identity, health and well-being. Psychology Press
[27] Christiansen et al., ‘Loneliness, social isolation, and healthcare utilization in the general population’, Health Psychology 42.2 (2023) (pp. 63-72).
[28] Meisters et al., ‘Does Loneliness Have a Cost? A Population-Wide Study of the Association Between Loneliness and Healthcare Expenditure’, International Journal of Public Health 66 (2021)
[29] Loneliness Monetisation Report (publishing.service.gov.uk)
[30] Loneliness Monetisation Report (publishing.service.gov.uk)
[31] Friendships, loneliness and psychological wellbeing in older adults: a limit to the benefit of the number of friends | Ageing & Society | Cambridge Core
[32] An overview of systematic reviews on the public health consequences of social isolation and loneliness – ScienceDirect
[33] Loneliness-beyond-Covid-19-July-2021.pdf (campaigntoendloneliness.org)
[34] Loneliness-beyond-Covid-19-July-2021.pdf (campaigntoendloneliness.org)
[35] The chronic loneliness pandemic: UK rates have surged since COVID-19 | World Economic Forum (weforum.org)
[36] LONELINESS ENGAGEMENT FUND REPORT.pdf (mencap.org.uk)
[37] Section 3 – Our starting point: How connected are we now? – Social isolation and loneliness: Recovering our Connections 2023 to 2026 – gov.scot (www.gov.scot)
[38] Loneliness at work report | research | British Red Cross
[39] New report into loneliness at work | British Red Cross
[40] Covid-19 CIA Access and Use of Services Findings.pdf (surreyi.gov.uk)
[41] UK Poverty 2024: The essential guide to understanding poverty in the UK | Joseph Rowntree Foundation (jrf.org.uk)
[42] Cost of living crisis causing loneliness epidemic for young people – FareShare
[43] Can small charities survive the cost of living crisis – The Jo Cox Foundation.docx
[44] Health and Wellbeing Strategy Index | Surrey-i (surreyi.gov.uk)
[45] https://goodcompany.org.uk/end-poverty-surrey/
[46] Loneliness Index, data accessed via Local Insights
[47] Social Isolation and Loneliness (who.int)
[48] WHO Commission on Social Connection
[49] Social connectedness improves public mental health: Investigating bidirectional relationships in the New Zealand attitudes and values survey
[50] Loneliness and Social Connections – Our World in Data
[51] DDCMS Loneliness Strategy (publishing.service.gov.uk)
[52] Tackling Loneliness annual report March 2023: the fourth year – GOV.UK (www.gov.uk)
[53] https://www.gov.uk/government/publications/tackling-loneliness-evidence-review
[54] https://www.gov.uk/government/publications/mental-health-and-loneliness-the-relationship-across-life-stages/mental-health-and-loneliness-the-relationship-across-life-stages
[55] https://tacklinglonelinesshub.org/
[56] Health and wellbeing strategy | Healthy Surrey
[57] About us | Healthy Surrey
[58] Surrey Health and Well-Being Strategy – update 2022 | Healthy Surrey
[59] Joint Forward Plan – ICS (surreyheartlands.org)
[60] Surrey Heartlands, Draft Clinical Strategy 2024-29 (due to be published in autumn 2024).
[61] Why we need our new local transport plan – Surrey County Council (surreycc.gov.uk)
[62] https://www.surreycc.gov.uk/roads-and-transport/policies-plans-consultations/transport-plan/policy-areas/planning-for-place#liveable
[63] https://www.surreycc.gov.uk/roads-and-transport/policies-plans-consultations/transport-plan/policy-areas/public-transport
[64] https://www.surreycc.gov.uk/roads-and-transport/policies-plans-consultations/transport-plan/policy-areas/public-transport#rural
[65] https://www.surreycc.gov.uk/roads-and-transport/policies-plans-consultations/transport-plan/your-travel/accessibility-needs
[66] https://www.surreycc.gov.uk/roads-and-transport/policies-plans-consultations/transport-plan/policy-areas/planning-for-place
[67] Emotional and Mental Wellbeing in Surrey Adults | Surrey-i (surreyi.gov.uk)
[68] Healthwatch Surrey , Identifying as a Carer: Understanding how and why people identify or register as an unpaid carer, and the perceived or experienced benefits of registering (March 2023).
[69] Healthwatch Surrey, Day Centres: Understanding the value of Day Centres for their regular users (2021).
[70] Children and Young People’s Emotional Wellbeing and Mental Health Strategy 2022-2027 | Surrey-i (surreyi.gov.uk)
[71] People with learning disabilities | Surrey-i (surreyi.gov.uk)
[72] Our Ageing Population | The State of Ageing 2023-24 | Centre for Ageing Better (ageing-better.org.uk)
[73] Society | The State of Ageing 2023-24 | Centre for Ageing Better (ageing-better.org.uk)
[74] loneliness-report_final_2409.pdf (ageuk.org.uk)
[75] Meisters et al., ‘Does Loneliness Have a Cost? A Population-Wide Study of the Association Between Loneliness and Healthcare Expenditure’, International Journal of Public Health 66 (2021)
[76] ‘Loneliness as a risk factor for care home admission in the English Longitudinal Study of Ageing’. Hanratty Barbara, Stow Daniel, Moore Danni et al. Age & Ageing 2018;47(6): 896-900. Available online at this link
[77] Society | The State of Ageing 2023-24 | Centre for Ageing Better (ageing-better.org.uk)
[78] Jo Cox Commission on Loneliness | Age UK
[79] Ratcliffe, J., Galdas, P. & Kanaan, M. Older men and loneliness: a cross-sectional study of sex differences in the English Longitudinal Study of Ageing. BMC Public Health 24, 354 (2024). https://doi.org/10.1186/s12889-024-17892-5
[80] “Why can’t a man be more like a woman?”: marital status and social networking of older men. Davidson K. J Men’s Stud. 2004;13(1):25–43.
[81] Ratcliffe, J., Galdas, P. & Kanaan, M. Older men and loneliness: a cross-sectional study of sex differences in the English Longitudinal Study of Ageing. BMC Public Health 24, 354 (2024). https://doi.org/10.1186/s12889-024-17892-5
[82] ‘The link between falls, social isolation and loneliness: A systematic review’, Nicola Petersen, Hans-Helmut König, André Hajek, Archives of Gerontology and Geriatrics, Volume 88, 2020.
[83] Combating loneliness: a guide for local authorities
[84] age_uk_digital_inclusion_evidence_review_2018.pdf (ageuk.org.uk)
[85] Tackling the inequalities of the digital divide in later life | Campaign to End Loneliness
[86] The Impact of Loneliness and Social Isolation on Cognitive Aging: A Narrative Review – PMC (nih.gov)
[87] Social isolation and dementia risk | Alzheimer’s Society (alzheimers.org.uk)
[88] Frontiers | Is Loneliness a Cause or Consequence of Dementia? A Public Health Analysis of the Literature (frontiersin.org)
[89] 2021 Census: Communal Establishment Residents | Surrey-i (surreyi.gov.uk)
[90] Victor, C. R. (2012). Loneliness in Care Homes: A Neglected Area of Research? Aging Health, 8(6), 637–646. https://doi.org/10.2217/ahe.12.65
[91] Barbara Hanratty, Daniel Stow, Danni Collingridge Moore, Nicole K Valtorta, Fiona Matthews, Loneliness as a risk factor for care home admission in the English Longitudinal Study of Ageing, Age and Ageing, Volume 47, Issue 6, November 2018, Pages 896–900, https://doi.org/10.1093/ageing/afy095
[92] Combating loneliness: a guide for local authorities
[93] Society | The State of Ageing 2023-24 | Centre for Ageing Better (ageing-better.org.uk)
[94] Disability and loneliness in the United Kingdom: cross-sectional and longitudinal analyses of trends and transitions. E Emerson et al. BMC Public Health, 2023: Disability and loneliness in the United Kingdom: cross-sectional and longitudinal analyses of trends and transitions – PMC (nih.gov)
[95] Loneliness, social support, social isolation and wellbeing among working age adults with and without disability: Cross-sectional study: Loneliness, social support, social isolation and wellbeing among working age adults with and without disability: Cross-sectional study – PMC (nih.gov) E Emerson et al. Disability and Health Journal, 2021
[96] Hearing Impairment, Loneliness, Social Isolation, and Cognitive Function: Longitudinal Analysis Using English Longitudinal Study on Ageing Asri Maharani, Neil Pendleton, Iracema Leroi. American Journal of Geriatric Psychiatry, 2019
[97] Social Prescribing as ‘Social Cure’: A longitudinal study of the health benefits of social connectedness within a Social Prescribing pathway.
[98] Surrey loneliness and social isolation survey (2024).
[99] The-world-shrinks-carer-loneliness.pdf (tacklinglonelinesshub.org)
[100] Our Ageing Population | The State of Ageing 2023-24 | Centre for Ageing Better (ageing-better.org.uk)
[101] The-world-shrinks-carer-loneliness.pdf (tacklinglonelinesshub.org)
[102] Most people caring for relatives with dementia experience loneliness Health & Social Care Services Research. National Institute for Health and Care Research (NIHR), 2020: Most people caring for relatives with dementia experience loneliness (nihr.ac.uk)
[103] Young carers | Barnardo’s (barnardos.org.uk)
[104] Helping schools and colleges support young carers | Surrey Education Services (surreycc.gov.uk)
[105] Supporting young carers with isolation & loneliness Barnado’s, 2021
[106] Emotional and Mental Wellbeing in Surrey Adults | Surrey-i (surreyi.gov.uk)
[107] Social isolation and mental health: Evidence from adults with serious mental illness Jenkins G. Trey, Janich Nicole, Wu Shiyou, Shafer Michael. Psychiatric Rehabilitation Journal, 2023
[108] Social Isolation and Psychosis: Perspectives from People with Psychosis, Family Caregivers and Mental Health Professionals Penny D. Xanthopoulou, Jennifer Mbanu, Agnes Chevalier et al. Community Mental Health Journal, 2022
[109] The Surrey Context. https://www.surreyi.gov.uk/jsna/surrey-context/#scpp-smi
[110] Emotional and Mental Wellbeing in Surrey Adults | Surrey-i (surreyi.gov.uk)
[111] Emotional and Mental Wellbeing in Surrey Adults | Surrey-i (surreyi.gov.uk)
[112] Surrey Suicide Prevention Strategy 2023 – 2026 | Healthy Surrey
[113] Surrey Joint Strategic Needs Assessment, People with learning disabilities | Surrey-i (surreyi.gov.uk)
[114] National Institute for Health and Care Research, 2021. Adults with learning disabilities need support to find love – NIHR Evidence
[115] Surrey Joint Strategic Needs Assessment, People with learning disabilities | Surrey-i (surreyi.gov.uk)
[116] Health behaviours and mental and physical health status in older adults with a history of homelessness: a cross-sectional population-based study in England. Smith Lee, Veronese Nicola, López-Sánchez Guillermo Felipe, Moller Eloise, Johnstone James, Firth Joseph, Grabovac Igor, Yang Lin, Soysal Pinar, Jackson Sarah E. 2019 BMJ Open
[117] Social relationships, stigma, and wellbeing through experiences of homelessness in the United Kingdom Jessica Rea. Journal of Social issues, 2022
[118] Social relationships, stigma, and wellbeing through experiences of homelessness in the United Kingdom Jessica Rea. Journal of Social issues, 2022
[119] Loneliness and Social Connections – Our World in Data
[120] Mental health and wellbeing plan: discussion paper and call for evidence – results – GOV.UK (www.gov.uk)
[121] Friendships, loneliness and psychological wellbeing in older adults: a limit to the benefit of the number of friends | Ageing & Society | Cambridge Core
[122] Friendships, loneliness and psychological wellbeing in older adults: a limit to the benefit of the number of friends | Ageing & Society | Cambridge Core
[123] Loneliness entrapment suicide: family, social and romantic loneliness (nationalelfservice.net)
[124] Shocking extent of loneliness faced by young mothers revealed – Co-op (co-operative.coop)
[125] Impact of Covid-19 on new parents: one year on (parliament.uk)
[126] Experiencing loneliness in parenthood: a scoping review (sagepub.com)
[127] Movember Fathers & Social Connections Report.pdf
[128] A qualitative exploratory study of UK first-time fathers’ experiences, mental health and wellbeing needs during their transition to fatherhood | BMJ Open
[129] What matters to young mums | Young Women’s Trust (youngwomenstrust.org)
[130] R Nowland et. al. ‘Experiencing loneliness in parenthood: a scoping review’, Perspectives in Public Health Volume 141 No.4, July 2021.
[131] Health and Race Perinatal Equity End of Project Report
[132] Why don’t women leave? – Women’s Aid (womensaid.org.uk)
[133] Women who have survived domestic abuse and their experiences of temporary safe accommodation in England – Office for National Statistics (ons.gov.uk)
[134] Domestic abuse in Surrey | Healthy Surrey
[135] Loneliness workshops for wellbeing professionals, January 2024.
[136] What we know about loneliness and connection 2014 – 2024 – What Works Wellbeing
[137] Social Isolation and Loneliness (who.int)
[138] Full article: Belonging and loneliness in cyberspace: impacts of social media on adolescents’ well-being (tandfonline.com)
[139] Community Life Survey 2021/22: Wellbeing and loneliness – GOV.UK (www.gov.uk)
[140] The lonely land – New Statesman
[141] How Adolescence Increases Loneliness for Teenager and Parent | Psychology Today United Kingdom
[142] ONS Report (tacklinglonelinesshub.org)
[143] Full article: Belonging and loneliness in cyberspace: impacts of social media on adolescents’ well-being (tandfonline.com)
[144] Full article: The impact of digital technology use on adolescent well-being (tandfonline.com)
[145] Mental health and loneliness: the relationship across life stages – GOV.UK (www.gov.uk)
[146] Disabled children still face social isolation | WellChild
[147] New research from Mencap shows bullying of people with a learning disability leading to social isolation | Mencap
[148] ‘Effects of Social Isolation and Loneliness in Children with Neurodevelopmental Disabilities: A Scoping Review’. Celia Kwan, Mojgan Gitimoghaddam and Jean-Paul Collet. Brain Sciences, 2020
[149] ‘Effects of mental health stigma on loneliness, social isolation, and relationships in young people with depression symptoms’. Prizeman Katie, Weinstein Netta, McCabe Ciara. 2023
[150] What we’re hearing from children and young people | Healthwatch Data
[151] Surrey County Council, Draft Education and Lifelong Learning Strategy, Surrey Education Partnership (2024-26).
[152] Exploring the Links Between School Exclusion and Youth Homelessness – Excluded Lives (ox.ac.uk)
[153] Surrey Deep Dive data sheet, February 2024.
[154] Dr. Hens, C. and Dr. Damon, D. (2024). Emotionally based school non-attendance (EBSNA). Support at the Whole School, Preventative Level. Surrey Educational Psychology Service.
[155] Surrey Deep Dive data sheet, February 2024.
[156] Reporting on the performance of commissioned services across the Children, Families and Lifelong Learning directorate (January 2024 report).
[157] New government research shows ‘lonely’ seems to be the hardest word for students – GOV.UK (www.gov.uk)
[158] End stigma: Survey (endstigmasurrey.org.uk)
[159] Bereavement is everyone’s business. Online. Available at: UK Bereavement Commission | Marie Curie
[160] Lund DA: Conclusions about bereavement in later life and implications for interventions and future research. In Older bereaved spouses: research with practical applications. Edited by Lund, Amityville, NY: Taylor and Francis/Hemisphere; 1989: 217-231.
[161] Stroebe W, Stroebe M, Abakoumkin G, Schut H: The role of loneliness and social support in adjustment to loss: a test of attachment versus stress theory. J Pers Soc Psychol 1996, 70: 1241-1249.
[162] Fried EI, Bockting C, Arjadi R, Borsboom D, Amshoff M, Cramer AOJ, Epskamp S, Tuerlinckx F, Carr D, Stroebe M: From loss to loneliness: the relationship between bereavement and depressive symptoms. J Abnorm Psychol 2015, 124: 256-265.
[163] A systematic review of loneliness in bereavement: Current research and future directions. Anneke Vedder , Kathrin Boerner , Jeffrey E. Stokes ,. Current Opinion in Psychology, 2022
[164] A systematic review of studies describing the influence of informal social support on psychological wellbeing in people bereaved by sudden or violent causes of death. Hannah Rachel Scott, Alexandra Pitman, Petya Kozhuharova, Brynmor Lloyd-Evans. BMC Psychiatry, 2020
[165] [1] Evaluating the outcomes for bereaved people supported by a community-based suicide bereavement service. Gehrmann Marc, Dixon Sara Dawn, Visser Victoria Suzanne, Griffin Mark. Crisis, 2020
[166] A systematic review of studies describing the influence of informal social support on psychological wellbeing in people bereaved by sudden or violent causes of death. Hannah Rachel Scott, Alexandra Pitman, Petya Kozhuharova, Brynmor Lloyd-Evans. BMC Psychiatry, 2020
[167] Evaluating the outcomes for bereaved people supported by a community-based suicide bereavement service. Gehrmann Marc, Dixon Sara Dawn, Visser Victoria Suzanne, Griffin Mark. Crisis, 2020
[168] The association of loneliness after sudden bereavement with risk of suicide attempt: a nationwide survey of bereaved adults. Pitman Alexandra L., King Michael B., Marston Louise, Osborn David P. J. 2020
[169] https://www.surreyi.gov.uk/dataset/em0ym/population-estimates
[170] A silent epidemic of grief (cam.ac.uk)
[171] Hajek et al., ‘Loneliness and Social Isolation among Transgender and Gender Diverse People’, Healthcare 11.10 (2023).
[172] [1] Elmer, van Tilburg and Fokkema, ‘Minority Stress and Loneliness in a Global Sample of Sexual Minority Adults: The Roles of Social Anxiety, Social Inhibition, and Community Involvement’, Archives of Sexual Behaviour 51 (2022) (pp. 2269-2298).
[173] LGBT Hero, The LGBTQ+ Lockdown Wellbeing Report (2020).
[174] Hajek et al., ‘Loneliness and Social Isolation among Transgender and Gender Diverse People’, Healthcare 11.10 (2023).
[175] Kim and Fredriksen-Goldsen, ‘Living Arrangement and Loneliness Among Lesbian, Gay, and Bisexual Older Adults’, Gerontologist 56.3 (2016) (pp. 548-558).
[176] https://www.ageuk.org.uk/information-advice/health-wellbeing/relationships-family/lgbt/lgbt-groups/
[177] [1] ‘Inequalities in older LGBT people’s health and care needs in the United Kingdom: a systematic scoping review.’ Kneale D. Henley J. Thomas J. French R. Ageing & Society, 2021. S0144686X19001326jra 493..515 (nih.gov)
[178] ‘All the lonely people, where do they all belong? An interpretive synthesis of loneliness and social support in older lesbian, gay and bisexual communities’. Fish Julie, Weis Christina. Quality in Ageing & Older Adults 2019;20(3): 130-142. Available online at this link
[179] Economic gradients in loneliness, social isolation and social support: Evidence from the UK Biobank Claryn S.J. Kung, Stephen E. Pudney , Michael A. Shields. Social Science & Medicine, 2022.
[180] ‘Is equity considered in systematic reviews of interventions for mitigating social isolation and loneliness in older adults?’ Madani Mohamad Tarek, Madani Leen, Ghogomu Elizabeth Tanjong, Dahrouge Simone, Hébert Paul C., Juando-Prats Clara, Mulligan Kate, Welch Vivian. BMC Public Health, 2022
[181] ‘Financial-related discrimination and socioeconomic inequalities in psychological well-being related measures: a longitudinal study.’ Bridson Lucy, Robinson Eric, Putra I. Gusti Ngurah Edi. 2024
[182] ‘Does unemployment lead to greater levels of loneliness? A systematic review.’
Morrish N., Medina-Lara A. Social Science and Medicine, 2021
[183] ‘Understanding the effect of loneliness on unemployment: propensity score matching.’ Morrish N., Mujica-Mota R., Medina-Lara A. 2022.
[184] ‘Understanding the effect of loneliness on unemployment: propensity score matching.’ Morrish N., Mujica-Mota R., Medina-Lara A. 2022.
[185] Health and Wellbeing Strategy Index | Surrey-i (surreyi.gov.uk)
[186] Census 2021: Economic Activity | Surrey-i (surreyi.gov.uk)
[187] The Royal Agricultural Benevolent Institution, The Big Farming Survey: The health & wellbeing of the farming community in England and Wales in the 2020s, October 2021.
[188] Wheeler, Rebecca, et.al. ‘It’s a lonely old world: Developing a Multi-Dimensional Understanding of Loneliness in Farming’, Sociologia Ruralis, 2023 (63): 11-36.
[189] Wheeler, R., Lobley, M., McCann, J. and Phillimore, A. (2021) Loneliness and Social Isolation in Farming Communities: Summary of research findings. ISBN 978-0-902746-56-5
[190] Wheeler, R., Lobley, M., McCann, J. and Phillimore, A. (2021) Loneliness and Social Isolation in Farming Communities: Summary of research findings. ISBN 978-0-902746-56-5
[191] Findings from the UK Veterans Family Study: Psychological health, wellbeing, and social support. (kcmhr.org)
[192] ‘Loneliness and social isolation of military veterans: systematic narrative review’, G Wilson, M Hill , M D. Kiernan. Occupational Medicine, 2018
[193] Stein JY, Tuval-Mashiach R. Loneliness and isolation in life-stories of Israeli veterans of combat and captivity. Psychol Trauma 2015; 7: 122–130.
[194] the-nations-duty-ssafa-research-report.pdf
[195] Kuwert P, Knaevelsrud C, Pietrzak RH. Loneliness among older veterans in the United States: results from the national health and resilience in veterans study. Am J Geriatr Psychiatry 2014;22:564–569.
[196] ‘Loneliness and social isolation of military veterans: systematic narrative review’, G Wilson, M Hill , M D. Kiernan. Occupational Medicine, 2018.
[197] Findings from the UK Veterans Family Study: Psychological health, wellbeing, and social support. (kcmhr.org)
[198] KCMHR Publication Database: Tackling Armed Forces Loneliness: Evaluation of the Armed Forces Covenant Fund Trust’s Tackling Loneliness Programme
[199] Findings from the UK Veterans Family Study: Psychological health, wellbeing, and social support. (kcmhr.org)
[200] KCMHR Publication Database: Tackling Armed Forces Loneliness: Evaluation of the Armed Forces Covenant Fund Trust’s Tackling Loneliness Programme
[201] How many people do we grant protection to? – GOV.UK (www.gov.uk)
[202] MHF_Mental-Health-of-Asylum-Seekers_REPORT_A4_SINGLE-PAGES_0.pdf (mentalhealth.org.uk)
[203] P. McKnight, L. Goodwin, S. Kenyon, ‘A systematic review of asylum-seeking women’s views and experiences of UK maternity care’, Midwifery, Volume 77, 2019, 16-23.
[204] Experiences of displaced young people living in England – Office for National Statistics (ons.gov.uk)
[205] What are the experiences of education for unaccompanied asylum‐seeking minors in the UK? – Fuller – 2020 – Child: Care, Health and Development – Wiley Online Library
[206] MHF_Mental-Health-of-Asylum-Seekers_REPORT_A4_SINGLE-PAGES_0.pdf (mentalhealth.org.uk)
[207] Workbook: Redacted South East Explorer (tableau.com)
[208] Migrant Health | Surrey-i (surreyi.gov.uk)
[209] MHF_Mental-Health-of-Asylum-Seekers_REPORT_A4_SINGLE-PAGES_0.pdf (mentalhealth.org.uk)
[210] Men’s health: The lives of men in our communities | Local Government Association
[211] Tackling the growing crisis of lonely men | Age UK
[212] Willis Paul, Vickery Alex, Jessiman Tricia, Loneliness, social dislocation and invisibility experienced by older men who are single or living alone: Accounting for differences across sexual identity and social context, Ageing & Society, 2020.
[213] Paul Willis, Alex Vickery, Loneliness, coping practices and masculinities in later life: Findings from a study of older men living alone in England, Health and Social Care in the Community, 2022.
[214] Blair Parrott, Men’s Mental Health, Public Health Bulletin, Surrey County Council (May 2024)
[215] Parrott, ibid.
[216] Schrempft, S., Jackowska, M., Hamer, M. et al. Associations between social isolation, loneliness, and objective physical activity in older men and women. BMC Public Health 19, 74 (2019). https://doi.org/10.1186/s12889-019-6424-y
[217] Everybody active, every day, An evidence-based approach to physical activity Framework_13.pdf (publishing.service.gov.uk)
[218] Active Lives Report, Sport England 2023 https://www.activesurrey.com/movement-for-change#1355
[219] https://www.activesurrey.com/movement-for-change#1355
[220] Shirley Musich, Shaohung S. Wang, James A. Schaeffer, Sandra Kraemer, Ellen Wicker, Charlotte S. Yeh, The association of physical activity with loneliness, social isolation, and selected psychological protective factors among older adults, Geriatric Nursing, Volume 47, 2022, Pages 87-94, ISSN 0197-4572, https://doi.org/10.1016/j.gerinurse.2022.07.006
[221] Jeesung Ahn, Emily B. Falk, Yoona Kang, Relationships between physical activity and loneliness: A systematic review of intervention studies, Current Research in Behavioral Sciences, Volume 6, 2024, 100141, ISSN 2666-5182, https://doi.org/10.1016/j.crbeha.2023.100141
[222] Royal Voluntary Service Virtual Village Hall
[223] Loneliness interventions across the life-course: (publishing.service.gov.uk)
[224] Evidence – National Academy for Social Prescribing | NASP (socialprescribingacademy.org.uk)
[225] NHS England » Health and justice framework for integration 2022-2025: Improving lives – reducing inequality
[226] Children and young people’s social prescribing – NASP evidence | NASP (socialprescribingacademy.org.uk)
[227] Children and young people’s social prescribing – NASP evidence | NASP (socialprescribingacademy.org.uk)
[228] Cartwright L, Burns L, Akinyemi O, Carder-Gilbert H, Tierney S, Elston J, Chatterjee H. [On behalf of the NASP Academic Partners Collaborative]. (2022). ‘Who is and isn’t being referred to social prescribing?’. London: National Academy for Social Prescribing.
[229] McCormick R. Does Access to Green Space Impact the Mental Well-being of Children: A Systematic Review. J Pediatr Nurs. 2017 Nov-Dec;37:3-7. doi: 10.1016/j.pedn.2017.08.027. Epub 2017 Sep 4. PMID: 28882650.
[230] https://www.barnardos.org.uk/sites/default/files/2023-10/report-missing-link-social-prescribing-children-young-people.pdf
[231] [1] The Open Data Institute and Frontier Economics, 2021; The Role of Data in Unlocking the Potential of Social Prescribing. https://theodi.org/wp-content/ uploads/2021/11/2021-11-01_14-50_PRS_Reportlinks-added.pdf
[232] 4.2 Continuum of Support for children and families living in Surrey | Surrey Safeguarding Children Partnership (procedures.org.uk)
[233] Natural England (2022) Links between natural environments and mental health Evidence
Information Note EIN065 Available at: https://publications.naturalengland.org.uk/publication/4973580642418688
[234] Sustainability | Free Full-Text | A Pragmatic Controlled Trial of Forest Bathing Compared with Compassionate Mind Training in the UK: Impacts on Self-Reported Wellbeing and Heart Rate Variability (mdpi.com)
[235] Natural England (2022) Links between natural environments and mental health Evidence Information Note EIN065 Available at: https://publications.naturalengland.org.uk/publication/4973580642418688
[236] 07 – Annex A Library and Cultural Services Strategy v0.11 – final.pdf (surreycc.gov.uk)
[237] Surrey libraries the second most visited in UK | Surrey News (surreycc.gov.uk)
[238] https://www.centreformentalhealth.org.uk/wp-content/uploads/2023/09/AMentallyHealthierNation_Digital_corrected-1.pdf