Sexual Health JSNA
Sexual and Reproductive Health
Publication date
This chapter was published in September 2025.
Contents
- Executive summary
- Introduction
- Strategic and policy context
- The population of Surrey
- Surrey sexual and reproductive health needs
- Evidence base for interventions promoting sexual and reproductive health
- Sexual health service provision in Surrey
- Sexual health service use in Surrey
- Insight from residents
- Insight from professionals
- Conclusions
- Recommendations for action
- Glossary
- Appendix
- Acknowledgements
- References
Executive summary (Fifteen-minute read)
Introduction
Sexual and reproductive health is an important public health issue and equitable access to services is essential to improve the health and wellbeing of residents across Surrey. This needs assessment focuses on changes in sexual health needs, recovery from the COVID pandemic, and the sexual health system across Surrey; how well we are working collaboratively to meet needs and reduce sexual health inequalities. This will inform the development of a sexual health strategy for Surrey.
Context
Sexual health is described as a state of emotional, mental and social well-being in relation to sexuality, not merely the absence of disease, dysfunction or infirmity. Many factors contribute to our sexual health including our culture and the place we grew up in, our education and the decisions we make about sex and relationships, and our sexual health needs change across the life course. This is why a whole system approach to sexual health is needed.
Population of Surrey – who is at risk of higher sexual health needs?
People living in areas of higher deprivation are significantly more likely to have a positive Sexually Transmitted Infection (STI) result, higher rates of abortion and repeat abortions compared to people living in the least deprived areas. Surrey has identified 21 key neighbourhoods that are most deprived in the county; good access to prevention and services in these neighbourhoods is particularly important.
The sexual health of young people is a priority. Young people aged 15-24 years are most likely to be diagnosed with an STI or have an unplanned pregnancy. Care experienced young people are more likely to live in deprived areas and have poorer health outcomes.
Nationally there are differences in the rates of STIs among different ethnic groups. People of Black ethnicity have the highest rates of all aggregate ethnic groups (Asian, Black, Mixed, Other, or White), although this varies among Black ethnic groups. The reasons for higher rates are complex and may include deprivation, sexual behaviours, social stigma and cultural beliefs.
The burden of STIs among gay, bisexual and other men who have sex (GBMSM) with men is high and remains a priority in Surrey, including easy access to testing, pre and post exposure prophylaxis (PrEP and PEP) and vaccination.
Other groups that are at risk of higher sexual health needs include: Asylum seekers, refugees and vulnerable migrants; people with additional needs and disabled people; people with learning disabilities, neurodiversity, mental illness; transgender people; people with problematic substance use.
Sexual health needs in Surrey
Sexually Transmitted Infections: Rates of sexually transmitted infections remain lower than the national average in Surrey. However, there have been increases in STIs in recent years, and the trend is upward in the rates of chlamydia, gonorrhoea, syphilis and human immunodeficiency virus (HIV) and are higher than before the COVID pandemic. There is variation across Surrey in the rates of STIs, with highest rates in Guildford and Epsom and Ewell.
Rates of testing for STIs (excluding chlamydia in young people) have increased since 2019, but remain lower than before the COVID pandemic, which indicates an increase in the burden of infection, and may also indicate an improvement in targeted testing for those at higher risk. Chlamydia detection rates among girls and young women have increased, but require more improvement to meet national targets, which is a challenge across the south-east and nationally.
Factors associated with the increase in STIs include a reduction in use of condoms, which may be driven by protection offered by PrEP, and the use of long-acting reversible contraception (LARC) as a contraceptive rather than barrier methods. There are also changes in sexual behaviour and social norms around relationships, including use of social media and dating apps, which may drive an increase in sexual partners.
The rates of HIV diagnosis in Surrey remain lower than nationally. However, the proportion of people first diagnosed with HIV in Surrey who receive a late diagnosis is significantly higher than the national average. It is positive that there has been an increase in the rate of testing for HIV in Surrey. One STI that has declined significantly is genital warts, which has been achieved through the introduction of the national human papillomavirus (HPV) vaccination programme, however, there has been a decline in vaccination coverage.
These trends indicate a need to strengthen work on prevention, particularly with groups and areas with higher needs, increase access to condoms, continue to increase testing of STIs, including for chlamydia and HIV, and increase coverage of the HPV vaccine.
Reproductive health: The birth rate in Surrey has declined in recent years. Access to high quality contraception and advice, as well as allowing choice in contraceptive methods is important and, overall, contraceptive outcomes, including abortion rates and teenage pregnancy, are relatively positive compared to national averages.
Rates of teenage conceptions have declined significantly since 1998, however, there are indications that there may be an increase nationally. In Surrey, rates have plateaued and there is less geographical variation. For this reason, Surrey has developed a teenage pregnancy prevention plan which focuses of priority groups, such as care experienced young people.
Abortion rates in Surrey are lower than nationally, and like national levels, nearly 90% of abortions take place under 10 weeks of pregnancy. However, the rate of abortion for women over 25 years in Surrey has been increasing over time. Possible reasons for these increases include improved access to early medical abortion methods, reduced access to contraception or changes in contraceptive methods, and financial stress related to the cost-of-living crisis.
These trends indicate the need to prioritise the teenage pregnancy prevention plan and ensure contraceptive choice and availability, including increasing access to emergency contraception.
Evidence base for Services
There is a well-established evidence base for the effectiveness of sexual health services, set out in quality standards and guidance from National Institute for Health and Care Excellence (NIHCE) and the British Association of Sexual Health) and HIV (BASHH).
Investing in sexual health and contraception services is also highly cost-effective. For example, evidence suggests that for every £1 invested in contraception there is a saving of £9, and for LARC, this rises to a saving on £48 for every £1 invested.
Sexual health services – what system do we have in Surrey?
We have mapped the sexual health system in Surrey which involves a wide range of partners and stakeholders from schools and community groups, providing relationship and sex education, through to primary care, and integrated specialist services providing treatment for people with higher needs, delivered by Central North West London NHS Foundation Trust (CNWL).
Sexual health commissioning is complex and fragmented but aims to support a service delivery system that provides open access to sexual health services and choice for residents in how they access services. Several recent developments to improve access and focus on inequalities include:
- Access to services: Expansion of sexual health online services for both STI testing and contraception; move to online booking for specialist sexual health services and improved website; GP buddy system to encourage wider access to LARC and increased training offer.
- Children and young people: ‘Teen Tuesday’ clinics for young people at 3 main clinics, with drop in and pre book sessions, plus outreach ‘clinic in a box’ service for young people with higher needs and other priority groups.
- HIV services: expansion of opt-out Blood-borne virus testing, including HIV, in Emergency Departments in some Surrey hospitals; HIV peer support worker; new PrEP champion post.
- Sexual Violence: a new independent domestic and sexual violence advocate (IDSVA) is now employed within the specialist sexual health service.
- Training and promotion: new sexual health outreach training on reducing inequalities and training for children’s social care staff supporting care leavers and asylum seekers and refugees. Co-produced, geo-targeted social media campaigns focusing on increasing chlamydia testing among girls and young women.
Our engagement with professionals who deliver sexual health services in Surrey highlighted some barriers to access, including access to GP appointments, likely to be related to accessing routine contraception; residents’ awareness about services available to them; availability of appointments at specialist sexual health services; and access to unregulated online sexual health advice.
Who uses sexual health services and how well are we meeting population needs?
Specialist sexual health services:
Overall, in 2023, there were nearly 14,000 consultations at specialist sexual health services in Surrey, delivered by CNWL, 90% of which were face to face, plus an online service which sent over 21,000 STI test kits to residents. In addition, residents accessed specialist services in other areas outside Surrey.
Specialist service use was highest in boroughs where clinics are located and in central areas of the county, including Guildford and Woking, and lowest in boroughs bordering neighbouring areas where there is much higher use of services outside the county, including Spelthorne, Epson and Ewell and Elmbridge.
Use of online sexual health services increased rapidly during the COVID pandemic. However, use has declined since 2021 among 25–34-year-olds, whereas for 18–24-year-olds, although rates of use are lower, the trend in use is upwards, indicating a sustained change. There is variation in use of the service across Surrey, with highest use in Guildford and Woking and lowest use in Spelthorne; these variations need addressing.
Findings from analysis of specialist service use by age, ethnicity, and sexual orientation is broadly in line with what would be expected considering evidence that there are higher sexual health service needs among young people, certain ethnically diverse groups, including those from Other white, Black African and Black Caribbean ethnic groups, and GBMSM.
A deep dive analysis of specialist sexual health service use by STI and contraception was undertaken to better understand if Surrey residents are using services at the level we would expect and are we testing the right people. Findings show:
STI Services, including HIV:
- In Surrey, whilst more STIs are diagnosed amongst people of white ethnicities, some ethnically diverse groups have disproportionate higher diagnosis rates.
- Higher numbers of STI tests are undertaken by those living in the least deprived areas of Surrey, but rates of testing are higher in those living in more deprived areas (IMD decile 2). The same pattern is seen when looking at diagnosis.
- Higher numbers of STI tests were done in those identifying as heterosexual, but the highest rates of testing are seen in those identifying as LGBTQ+ (lesbian, gay, bisexual, transgender, queer, and other identities). This varies depending on STI test.
- Higher numbers of testing were undertaken by males and females aged 25-34, but rates are higher amongst males and females aged 18-24. There is variation depending on STI test.
- Data has been used to compare rates of face to face and online STI testing, whilst also looking at demographics of service users. For example, data shows chlamydia and gonorrhoea testing rates are higher for online testing compared to face-to-face testing in people living in the most deprived IMD decile (IMD decline 2) in Surrey.
- Overall, our research indicates that population groups and areas likely to have higher sexual health needs have higher rates of testing and diagnosis of STIs. It is important to maintain a strong focus on priority populations and areas to reduce sexual health inequalities.
Contraception Services:
- As expected, following the COVID pandemic, there have been changes in preferences between face-to-face and online contraception consultations in Sexual Health Services in Surrey. This seems particularly relevant among 18-24-year-olds where there has been a steady increase in the number of consultations over time.
- The rate of women prescribed short acting combined hormonal contraception in both sexual health services and GPs has been reducing in Surrey and nationally. However, the majority of online contraception consultations were for the progesterone-only pill. Although, use among 25–34-year-olds has declined, which could be due to changes in contraception preferences, or changes in how this age-group access contraception.
- In 2023, Surrey had total rates of prescribed LARC higher than the national average at 56.2 per 1,000 women aged 15–44 (just over 17%). This varied widely across districts and boroughs. The proportion of LARC prescribed at GPs has remained relatively stable over time at just over 75%.
- Surrey residents who took part in the national women’s reproductive health survey indicate that compared to nationally, there is a higher use of GP and Pharmacy services and just under 90% of respondents received their preferred contraceptive choice, indicating appropriate access to services. However, a quarter of women changed their contraception method over the last year, slightly higher than nationally, with the top three reasons being: effect on mood; impact on sex life and weight change.
Primary Care Services:
There have been reducing rates of GP prescriptions for short acting hormonal contraception in Surrey and nationally over the past decade. Nationally there have been emerging concerns among younger women about negative impacts of hormonal contraception and an increase in the use of fertility apps. The use of long-acting reversible contraception (LARC) is higher in Surrey than nationally, which is positive as LARC is one of the most reliable, convenient and cost-effective methods of contraception. Just over 75% of LARC is delivered in GP practices in Surrey. However, there are variations by geography, for example, rates of LARC in Runnymede are lower than the national average.
Free emergency contraception for young women is provided by 48 Pharmacies across Surrey, and levels of use have been stable over recent years. Two thirds of 16-24 year olds accessing emergency contraception did so because they did not use contraception. Access to free emergency contraception will be made available to all women from Pharmacies later in 2025, as part of a national change to reduce inequalities in access in deprived areas and to free up GP appointments. It will be important to monitor the impact of this change, for example, uptake in priority neighbourhoods and if it contributes to stemming the increase in abortions among women over 25 years. Pharmacies in Surrey provide a small amount of chlamydia screening services, and this is an area that should be developed to increase access, especially in priority neighbourhoods.
Insight from residents and stakeholders:
Insight for this report included surveys with residents and professionals and focus groups with young people. An easy read version of the resident survey was also produced. Key themes from the engagement are highlighted below.
Overall feedback suggests that there is a good level of satisfaction with services in Surrey. Nearly three quarters of respondents found it easy to access sexual health STI services, a small minority identified difficulties, including inconvenient location of clinics and not being able to access the service quickly enough. Over 80% of respondents were satisfied or very satisfied with services.
Most people found it quite easy to access contraception services, and this was highest amongst people using GP services, however, nearly a quarter identified difficulties, the main reasons being an inconvenient location of specialist service clinics and difficulties using the booking system.
For both STI and contraceptive services there was a high level of support for online booking. Demand for flexibility and choice of walk-in and pre-bookable face to face appointments was raised, but respondents also valued the options of telephone and online services. There was some demand expressed for access to services at evening and weekends.
From our focus groups, young people emphasised the importance of confidentiality for services, particularly regarding the visibility of sexual health clinics and the use of online services. They also highlighted the importance of minimising the uncertainty and fear of using services, especially for young people with additional needs and ensuring professionals are trained to understand different situations and needs. Young people recommended more inclusive waiting rooms with clearer signage and privacy. Information about public transport options to services should be more visible.
The internet was the main source of information for most adults, although resident panel feedback indicated that they equally sought information from a GP or nurse. Young people highlighted the internet, health professionals and trusted adults as sources of information. Young people expressed caution about some social media platforms and the challenges of knowing trusted sources.
Residents who took part in engagement are not representative of all groups, for example, there were no responses to our easy read survey, limited feedback from young people and limited response to our survey from different ethnically diverse groups. When professionals were asked about the groups they identified at being most at risk of experiencing sexual health inequalities, over half of the respondents highlighted the needs of: asylum seekers and refugees; young people aged under 25; people with a learning disability; people experiencing homelessness and people from ethnically diverse backgrounds including the Gypsy, Roma & Traveller (GRT) community. Ongoing involvement should be embedded across the sexual health system, with innovative approaches to hear the views of underserved groups and tackle stigma.
We are keen to hear views on this sexual health needs assessment as part of our continuous engagement. Please e-mail comments to: [email protected]
Note on Data
The data in this needs assessment is up to date as of May 2025. We are aware that new data for STIs was published nationally in June 2025. This has been reviewed and noted that this does not change the recommendations in this report (Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care) .
Summary of Recommendations
Rationale for each recommendation is set out in the main report.
Area 1: Prevention
- Support provision of high-quality relationship and sex education across Surrey
- Maintain and increase commitment to Teenage Pregnancy prevention action plan
- Increase condom use through increased uptake and wider offer of the Condom Card scheme and social media campaigns
- Increase coverage of chlamydia screening among 15–24-year-old females, focus on areas of low coverage through campaigns and increase access
- Increase HPV vaccination uptake among eligible populations
- Increase awareness and uptake of PrEP for HIV prevention and address inequalities in uptake
Area 2: Access to services and reducing barriers:
- Reinforce the importance of continuing to offer choice in how and where to access sexual health and contraception services in Surrey, including testing in the community e.g. testing in pharmacies.
- Increase awareness of the available services for sexual health and contraception in Surrey, including online services, out of hours services, and pharmacy services available to young people.
- Ensure that inequalities are not exacerbated with a shift to increased use of online services in Surrey. Bearing in mind that online services don’t suit everyone and to consider such issues as digital poverty.
- Investigate reasons for the low uptake of online services in some boroughs, including Spelthorne, and increase promotion of online services in those areas.
- Take action to improve the return rate of online tests, particularly in areas of low return rates.
- Explore options to increase access to HIV testing in the community, particularly for those more likely to receive a late diagnosis (older adults, heterosexual men and Asian and Black individuals).
- Improve access and uptake of LARC in priority areas of lower uptake.
- Promote awareness of the expansion of access to free emergency contraception for over 25-year-olds in key neighbourhoods and groups and monitor uptake.
- Take action to address stigma around STIs and HIV, to prevent stigma being a barrier to accessing services.
- Improve accessibility of in-person specialist sexual health services for individuals with additional needs and disabilities.
- Explore and address issues identified by some young people as a barrier to accessing services, including online services.
- Continue to promote awareness and training across the sexual health system workforce, including: mental health; additional needs and disabilities; trans issues; gender and body dysphoria and trauma informed care.
Area 3: Access to information
- Promote high quality, evidence-based, trusted sexual health and contraception information for residents online, use targeted methods to reach priority audiences
- Raise awareness of misinformation on social media
Area 4: Insight and Inclusion
- Undertake further insight and engagement to better understand the needs of diverse groups of young people, including care experienced young people.
- Undertake further insight and engagement to better understand the needs of residents whose views are underrepresented in this report including Asylum seekers, refugees and vulnerable migrants; people with additional needs and disabled people, people with learning disabilities, neurodiversity and mental illness; people from Black ethnic groups and GRT; transgender people and people with problematic substance use.
- Continue to monitor trends in sexual health outcomes and service use and health inequalities.
- Continue to monitor contraception method preference and emerging evidence and impact that women are moving away from short acting hormonal contraception.
Area 5: Working as a whole system
- Ensure a system-wide approach to delivery of sexual health and contraception services in Surrey, through the development of a sexual health strategy.
- Ensure that there are clear referral pathways and awareness among professionals across the sexual health system.
- Ensure the ongoing collaborative approach to sharing information, involvement and hearing resident voices, especially among priority groups and monitoring outcomes.
1 Introduction
1.1 What is sexual and reproductive health
The World Health Organisation (WHO) define sexual health as “…a state of physical, emotional, mental and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction or infirmity. Sexual health requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination and violence. For sexual health to be attained and maintained, the sexual rights of all persons must be respected, protected and fulfilled” (1).
Sexual health services encompass the prevention and treatment of sexually transmitted infections (STIs), access to contraception for prevention of STIs and prevention of unintended pregnancies, and the promotion of healthy sexual behaviours. The sexual health needs of individuals change across their life course. Sexual and reproductive health needs in early-life focus on education around relationships, healthy behaviours and sex. Reproductive health encompasses access to contraception, as well as providing support and education on preconception care and conception. Following birth, maternal health will include access to antenatal and postnatal care, including advice around contraception. Throughout life, not just limited to reproductive years, sexually active individuals will require support and advice for prevention, diagnosis and treatment of STIs.
1.2 What is a JSNA?
A JSNA (Joint Strategic Needs Assessment) is a statutory document that measures the current and future health and social care needs of Surrey residents. Production of JSNAs is a duty of the Surrey Health and Wellbeing Board, and JSNAs are, therefore, system owned. It supports local leaders and commissioners to make informed decisions and to shape services in a way that best meets the needs of their communities. The JSNA is co-produced with partners across Surrey, as well as having meaningful representation from the local community.
1.3 Scope
This JSNA has a focus on STIs, sexual health services, and contraception services for residents of Surrey as described below.
1.3.1 Sexually transmitted infections
The World Health Organisation define STIs as infections that are “spread predominantly by unprotected sexual contact. Some STIs can also be transmitted during pregnancy, childbirth and breastfeeding, and through infected blood or blood products” (2). For the purposes of this JSNA, the STIs of main interest include chlamydia, gonorrhoea, syphilis, and HIV. Other STIs included within the scope of this JSNA include genital warts, genital herpes, mycoplasma genitalium, trichomoniasis, and sexually transmitted shigella.
Sexual health services refer to any services involved in the prevention, screening, testing or treatment of these STIs, as well as any service that provides general sexual health and wellbeing advice as part of its work.
HIV services are commissioned by NHS England and are therefore outside the scope of this JSNA, however HIV testing and the use of sexual health services by people living with HIV is within the scope.
1.3.2 Contraception
In this JSNA, contraception methods include use for both preventing pregnancy and preventing STIs. This includes emergency contraception, other contraception to prevent pregnancy, including long-acting reversible contraception (LARC), as well as barrier contraception to both prevent pregnancy and/or STIs, such as condoms. Contraception used by both women and men are within the scope of this JSNA.
Contraception services refer to any service involved in providing the above contraception methods, or providing advice or counselling about contraception, prevention of pregnancy, or abortions.
1.4 Aims
The aim of this JSNA chapter is to provide understanding of Surrey residents’ sexual and reproductive health needs and insight into sexual health inequalities to inform key partners, decision-makers and commissioners. The specific aims of this JSNA are:
- To understand for Surrey: rates of STIs, rates of teenage pregnancy, rates of abortions, preferred methods of contraception
- To assess inequalities in access to, and uptake of, sexual health and contraception services
- To understand the experiences of those needing to access sexual health services and contraception services
- To understand barriers to access to sexual health services and contraception services
- To understand the experiences of those delivering sexual health services and contraception services in Surrey
- To assess whether there are additional sexual health needs and contraception needs of Surrey residents and consider how these could be met
- To provide recommendations for how to improve the sexual health of Surrey residents, with a key focus on ‘no one left behind’
1.5 Methods and engagement
1.5.1 Overview
A mixed methods approach was used to inform this needs assessment, including:
- A review of relevant policies, guidance and evidence
- Analysis of publicly available data (note, this is up to date as of May 2025)
- Analysis of local service level data
- Resident insights from local and national surveys and focus groups
- Stakeholder insights from a local survey and meetings with partners
See Appendix 1 for further details. A multi-agency steering group was set up to guide the needs assessment.
1.5.2 Resident engagement
A questionnaire was distributed to residents exploring access to sexual health and contraception services, barriers to accessing services, preferences for accessing services, and where residents go for information on sexual health, contraception and wellbeing.
We aimed to capture the views of residents who are more likely to experience inequalities in sexual health by asking stakeholders working with individuals from different groups to disseminate the resident’s survey with their service users.
A second questionnaire for residents was distributed to the Resident Intelligence Unit’s Resident Panel. The Resident Panel is a cohort of 3,000 Surrey residents who are recruited to be representative of the wider Surrey population, with results weighted by age and sex (see Appendix 1 for detailed methods).
Focus groups were conducted to explore the perceptions, attitudes, and experiences of young people in Surrey regarding sexual health and contraception. One focus group was with participants recruited through Surrey Youth Voice, and a second was with young people attending Twister youth group (see Appendix 1 for detailed methods).
1.5.3 Professionals engagement
A questionnaire was distributed to stakeholders working in sexual health services or working in a role where they offer sexual health advice and support to Surrey residents. This survey explored services (including advice and support) offered by the respondent, challenges they experience in providing their service, and their views regarding the key priorities for improving sexual health of Surrey residents (see Appendix 1 for detailed methods).
In order to maintain a focus on representing the views of individuals from groups at risk of experiencing sexual health inequalities and/or those with greater sexual health need, the professionals’ survey was shared with individuals working with residents from these groups.
1.5.4 Quantitative data
Quantitative data was collated and analysed from the Department of Health and Social Care (via Fingertips, a large public health data collection published by the Department of Health and Social Care (DHSC) (3)), service providers in Surrey (including data from the specialist sexual health service in Surrey and out of area services), PharmOutcomes, and the Surrey Condom Distribution Scheme. Data is up to date as of May 2025. We are aware that new data for STIs was published nationally in June 2025. This has been reviewed and noted that this does not change the recommendations in this report.
2 Strategic and policy context
2.1 National strategies and policy
2.1.1 A Framework for Sexual Health Improvement in England
The last national sexual health strategy, ‘A Framework for Sexual Health Improvement in England’ was released in 2013 (4), with a new national strategy awaited. The last national strategy placed a focus on supporting effective working between those working in sexual health improvement, and promoting the availability of high quality, accessible services for all.
Since this last strategy, reviews and reports have been released by other organisations, to guide on the provision of sexual health services. In 2023 The Association of Directors of Public Health released a policy position statement on sexual health (5). They highlighted the importance of provision of preventative sexual health measures and promotion of sexual wellbeing, alongside a whole systems approach to sexual and reproductive health and HIV care. They also focused on the importance of incorporating evidence-based digital technologies into sexual health services.
In 2024, the Local Government Association released ‘A blueprint for the future: Sexual and reproductive health and HIV services in England’ (6). This report called on the national government to work with local government on a national 10-year sexual and reproductive health strategy. They also called for the commitment of national government to a funding increase for sexual and reproductive health services for councils to support the increased demand for sexual and reproductive health services and to address inequalities in sexual and reproductive health.
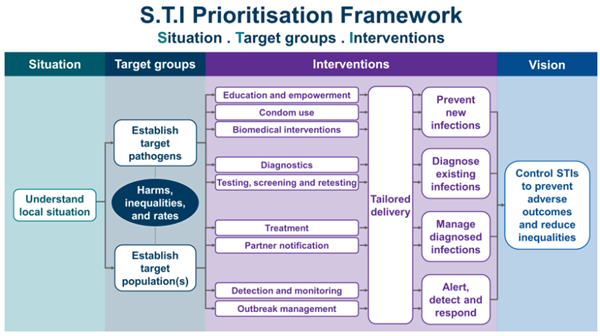
2.1.2 STI Prioritisation Framework, 2024
The UKHSA published an STI Prioritisation Framework in October 2024 (7). This framework recognises the inequalities in sexual health that exist and outlines how decisions regarding sexual health service planning and delivery can be prioritised to reduce these inequalities and prevent the associated adverse health outcomes (Figure 2.1).
2.1.3 Variation in outcomes in sexual and reproductive health in England, 2021
Public Health England (now UKHSA) published a toolkit to explore variations and local inequalities in outcomes in sexual and reproductive health in England (8). The document considers variation within areas, comparisons with the national average and variation by population demographics, including ethnicity, gender, age, socioeconomic status and sexual orientation.
2.1.4 Towards Zero – An action plan towards ending HIV transmission, AIDS and HIV-related deaths in England – 2022 to 2025
This national HIV Action Plan, published in 2021, provided a key step towards achieving the 2030 goal of ending onwards HIV transmission (9). The plan had four key objectives (9):
“Objective 1: ensure equitable access and uptake of HIV prevention programmes
Objective 2: scale up HIV testing in line with national guidelines
Objective 3: optimise rapid access to treatment and retention in care
Objective 4: improving quality of life for people living with HIV and addressing stigma”
The Action Plan included a commitment to expand HIV opt-out testing in hospital emergency departments which has been actioned.
National guidance from NHS England as part of the HIV Action Plan is due to be released by the Department of Health and Social Care in 2025, and will strengthen Surrey’s efforts to ending onward transmission of HIV.
2.1.5 Women’s Health Strategy for England, 2022
The Women’s Health Strategy for England is a 10-year plan focused on improving health outcomes for women by addressing gender disparities in health (10). The strategy aims to enhance research into women’s health issues, improve access to services, and ensure better education and awareness among healthcare professionals and the public. The strategy considered key themes across three stages of a woman’s life course, with contraception needs and sexual health and wellbeing being considered across all three life stages.
Public Health and Surrey Heartlands ICB are jointly developing a local approach to the Women’s Health Strategy, reflecting the needs of women in Surrey. Key areas of work to date include collating data available, developing a Surrey Heartlands Women’s Health Network, developing offers of training for clinicians on LARC and menopause, and expanding the existing women’s health hub in Guildford & Waverley Place.
2.2 Local Context
2.2.1 Surrey Health and Wellbeing Strategy
The Surrey Health and Well-being Board published a 10-year Health and Wellbeing Strategy in 2019, with an update in 2022, this was informed by previous JSNAs as well as engagement with residents (11). Sexual and reproductive health is strategically linked with the work of the wider system under Priority 3 of the strategy: Supporting people to reach their potential by addressing the wider determinants of health. Milestones for sexual health and wellbeing include:
- Priority and underserved groups reached
- Surrey HIV Action Plan Implemented
- Pharmacy sexual health services supported
- Chlamydia screening programme delivered
- Teenage pregnancy prevention action plan delivered
- Women’s Health agenda developed
- Availability and accessibility to LARC for women improved
This needs assessment will inform the development of a sexual health strategy for Surrey in 2025.
The Public Health approach to the sexual health team strives for a whole systems approach, working to improve and protect the sexual health of people living and working in Surrey with a focus on reducing health inequalities through strategic system leadership and collaborative working with local partners and the community.
2.2.2 Surrey’s HIV Action Plan
The HIV Action Plan for Surrey 2022-2025 was developed to reflect the England HIV action plan, ‘Towards Zero’, created in 2021 and the ambitious vision to eradicate new HIV transmissions in Surrey by 2030. The Plan contains four objectives, (Prevention, Testing, Treatment and Empowerment and Wellbeing) that reflect the objectives in the England plan. Key milestones to date include promotion and amplifying national HIV and testing campaigns, HIV testing in the community pilot project, and identifying funding for recruitment of a HIV peer support worker and a PrEP champion role.
2.2.3 Teenage Pregnancy Prevention Action Plan
All regions in England have seen declines in Under 18s conceptions since 1998 (the baseline year for the original Teenage Pregnancy Strategy). Since 1998, rates have fallen by 72% (12). However, the release of the 2021 teenage pregnancy data showed the first rise in 14 years, sounding a note of caution. In Surrey, teenage pregnancy rates continue to be lower than the rate for England (12). However, data at borough and district level shows some disparities, and overall, the Surrey rate has plateaued (12).
In order to address these concerns, the Surrey Teenage Pregnancy Prevention Action Plan was developed with partners to deliver a whole systems approach to support young people at risk of unplanned and unintended pregnancy and empower them to make informed decisions about their sexual health and wellbeing. The action plan covers the following areas and highlights the vital role they play in achieving a whole systems approach:
- Strategic leadership and accountability
- Data and insight
- Advice and access to contraception in non-clinical, education & youth settings
- Targeted prevention for young people at risk
- Support for pregnant teenagers and young parents, including prevention of subsequent pregnancies
- Relationships and sex education (RSE) in schools and colleges
- Communication – consistent messages to young people, parents and practitioners
The team have worked in partnership with the relevant Surrey organisations, including social care staff, school nurses, and youth workers, to ensure that staff feel supported within their role to access the available training sessions offered by Surrey’s specialist sexual health service. The training offer is crucial in upskilling professionals and parents and carers to feel more confident to engage with their young people about sexual health issues including healthy relationships. The training offer is always evolving, and new key groups are being targeted.
Although the action plan’s primary focus is on prevention of teenage pregnancy, it also recognises the importance of supporting young parents to make informed choices about whether or not to have subsequent pregnancies when they are still young. The action plan highlights the need for there to be support available to encourage them to return to education or employment if they want to do this. It also looks at the role of young parent groups to offer them peer support to help them feel supported and encourage them to access courses and additional groups if they are interested.
Developing a whole systems approach is crucial in reducing the incidence of teenage pregnancies and improve educational outcomes and reduce health inequalities. Through collaborative efforts with a wide range of system partners, we aim to create a supportive environment that promotes the wellbeing and aspirations of the most vulnerable young people.
2.2.4 Sexual health outreach group (SHOG)
The purpose of the SHOG is to bring together representatives from organisations working with key inclusion groups and those working with people who use sexual health services. This provides the opportunity for updates on sexual health services (Specialist service provision, Pharmacies and GPs) to be shared and is also an opportunity for those representatives to feedback on the needs of the groups they work with and share good practice. Through the SHOG, partnerships are strengthened between the sexual health providers and local community organisations to ensure that consistent sexual health messages are shared across Surrey.
3 The population of Surrey
Based on the results of the 2021 Census, there are 1,228,671 individuals living in Surrey (13) – an overview of Surrey’s population is available in The Surrey Context: People and Place | Surrey-i The population is described further below, focusing on some of the groups with greater sexual health needs.
3.1 People living in areas of higher deprivation
Surrey is a relatively affluent county, although areas of high deprivation do exist. Termed ‘key neighbourhoods’, these 21 areas represent the most deprived areas based on the Index of Multiple Deprivation (IMD) (14). Individuals living in areas of higher deprivation are significantly more likely to have a positive STI test result, including for chlamydia and gonorrhoea, as well as significantly higher rates of abortion and repeat abortion, compared with individuals living in the least deprived areas of England (15). These inequalities are explored in more depth for Surrey in this report.
Indices of Deprivation 2019 for areas in Surrey | Surrey-i
3.2 Young people
In Surrey there are 138,180 individuals aged 15 to 24 years, accounting for 11.2% of the population (13). Young people in this age group are the most likely to be diagnosed with STIs (16) and are more likely to have an unplanned pregnancy (17). Young people are at higher risk of sexual health inequalities due to being more likely to have more frequent changes of sexual partner, and less likely to use a condom with a new sexual partner. The sexual health inequalities experienced by young people are explored in more depth in this report.
3.3 Care experienced young people
Care experienced young people are more likely to live in areas of higher deprivation and experience poorer health outcomes and higher mortality rates than non-care experienced young people (18,19). There are several drivers of poor health outcomes in these individuals that relate to sexual health, including the long-term mental and physical health impacts of adverse childhood experiences, problematic substance use, lack of support to access services, and poverty (20). Educational disadvantage and increased rates of school absence may result in lack of exposure to, or engagement with, RSE at school (20).
As a result of these disadvantaging factors, care experienced young people are more likely to engage in early sexual activity, have a higher number of sexual partners, and have an increased risk of STIs (20). Furthermore, care experienced young people are less likely to use contraception, and experience higher rates of teenage pregnancy. Care experienced young people are also at higher risk of sexual assault and sexual exploitation (20). The specialist sexual health service in Surrey provides outreach to children’s residential homes in Surrey to optimise sexual healthcare provision for these individuals.
3.4 Sexual orientation
In Surrey, 90.7% of individuals aged 16 years and over identify as straight or heterosexual, 1.2% as gay or lesbian, 1.1% as bisexual, and 0.3% identified themselves as another sexual orientation, including pansexual (0.17%) and asexual (0.05%) (21). Nationally, data from the Annual Population Survey estimates that 3.8% of individuals aged 16 years and over identified as lesbian, gay or bisexual in 2023, and younger people were more likely to identify as lesbian, gay or bisexual (10.4% of 16-24 year olds).
The burden of STIs among gay, bisexual and other men who have sex with men (GBMSM) remains high nationally. Between 2022 and 2023, STI diagnoses increased among GBMSM including gonorrhoea, chlamydia, infectious syphilis, genital herpes and genital warts. Less common infections such as lymphogranuloma venereum (LGV) also increased by 15.9%. Sexually transmitted shigellosis also rose sharply by almost 50%, with growing concerns over extensively drug-resistant (XDR) strains circulating in this group (22).
3.5 Ethnicity
In Surrey, 76.6% of the population are white British, including English, Welsh, Scottish and Northern Irish (23). The next most common ethnic group was white other (8.9%), which includes those from an ‘other white’ background category, including Roma (7.5%) and Gypsy or Irish Traveller (0.2%) (23).
By highest proportion, the next most common ethnic groups were Asian, including Asian, Asian British, and Asian Welsh (7.7%), mixed or multiple ethnic background (3.4%), and black, including black, black British, black Welsh, Caribbean or African (1.7%) (23).
Nationally, there are differences in rates of STIs with higher diagnoses in some ethnic groups, particularly of syphilis, genital herpes, genital warts, and Trichomoniasis (22). Several studies have explored reasons for observed ethnic inequalities, which are complex. Whilst sexual behaviour and socio-economic deprivation are factors, they do not fully explain the inequalities seen (24, 25, 26).
There is limited data on sexual health burden among Gypsy and Roma Traveller communities with data suggesting that a lack of education and stigma and taboo around sexual behaviour and sexual health can limit access to services(27, 28).
The higher rates for some STIs in certain ethnic groups remain a concern. Public health approaches to address this need to fully understand the diversity of needs of different groups and that sexual health can be a challenging topic in some ethnically diverse groups, with potential for social stigma and cultural beliefs which may discourage open discussion. Furthermore, language barriers and a lack of understanding of cultural differences in healthcare settings may impact accessibility of services and resources.
3.6 Women’s health
Among all consultations at sexual health services nationally in 2023, over half were by women (22). Women experienced higher rates of several STIs including chlamydia, gonorrhoea, genital warts and genital herpes (22). Furthermore, women often face a higher burden of complications from STIs, such as chlamydia, leading to more severe health outcomes, including pelvic inflammatory disease (PID) and infertility if untreated (29).
Contraception services have traditionally focused on women, often placing the responsibility of contraception on them, despite the importance of promoting shared responsibility, including access to barrier methods such as condoms. Ensuring information, choice and availability in contraception is essential, because limited options or barriers to access can impact autonomy and reproductive wellbeing.
3.7 Gender identity
In 2021, for the first time, the census asked about gender identity, of which 94.8% of the population of Surrey aged 16 years and over provided a response (30). A total of 94.4% of the population of Surrey aged 16 years and over reported that their gender identity was the same as their sex registered at birth, and 0.37% reported that their gender identify was different from their sex registered at birth, with 5.2% of the population not providing a response (30).
Within the residents who indicated that their gender identify was different from their sex registered at birth, 0.08% of the population of Surrey identified as a trans man, 0.08% identified as a trans woman, and 0.05% identified as non-binary (with the remaining 0.17% either not providing a gender identity or providing a different gender identity) (30).
Risky sexual behaviours, including having multiple sexual partners and condomless intercourse, have been reported less frequently in transgender and non-binary individuals compared with cis-gender individuals (31). However, transgender individuals are significantly more likely to experience sexual violence (32).
Transgender and non-binary individuals often find challenges in navigating information about sexual health and sexual health services that have been historically designed for heterosexual individuals and their needs and for cis-gender individuals and their needs.
3.8 Asylum seekers and refugees
Vulnerable migrants (including asylum seekers and refugees) represent 0.7% of the population (33). In the year ending September 2024, Home Office estimates suggest around 0.45% of the Surrey population were on the Homes for Ukraine scheme, under the Afghan resettlement Programme, or other asylum seekers receiving support (34). This is likely to be an underestimate of the total number of asylum seekers and refugees because this does not include other migration cohorts requiring support from local authorities.
Asylum seekers and refugees may face barriers in accessing sexual health services and STI prevention due to language, limited knowledge of available services in the area, and fear of stigma, breach of confidentiality, or of disclosure having an impact on immigration applications (35, 36, 37). Many experience poor mental health and financial insecurity, which further reduces their ability to access services and prioritise their sexual health needs.
3.9 People experiencing homelessness
In Surrey, 2.74 per 1,000 households are assessed as homeless, and 4.05 households per 1,000 are threatened with homelessness (38). Across Surrey, this equates to 3,317 households assessed as homeless or threatened with homelessness.
People experiencing homelessness have higher rates of STIs as well as poorer reproductive health with high rates of pregnancy and unintended pregnancy (39, 40). Furthermore, people who experience homelessness often face individual-level and healthcare-level barriers to accessing sexual health and contraception services (41, 42, 43).
3.10 People involved in sex work
Latest data from Streetlight, an organisation which supports women involved in sex work and prostitution in Surrey, Sussex and London, showed that there were over 2,200 adult online adverts across Surrey (44). In 2024, Streetlight engaged with over 2,300 women across Surrey and, as a result, provided direct support to 119 women (44).
In England, data from sexual health services suggests that female sex workers have a higher risk of STIs and HIV compared to other females. The risk of almost all STIs were higher in female sex workers compared to other females attending sexual health clinics, although the difference between the groups varied greatly across different STIs (45). Sex workers may avoid services due to fear of judgement, which creates a barrier to accessing sexual health care.
Although most people involved in sex work are female, it is important to acknowledge that males are also involved in sex work. Data from sexual health services in England suggest that male sex workers have around twofold to threefold higher risk of certain STIs compared to other men (46).
3.11 People with additional needs and disabled people
In 2021, 13.8% of residents in Surrey reported that they were disabled under the Equality Act, including 8.7% who reported that their day-to-day activities were limited a little, and 5.1% who reported that their day-to-day activities were limited a lot (47). A further 7.4% of residents reported that they were not disabled under the Equality Act, but that they had a long term physical or mental health condition, that did not limit their day-to-day activities (47).
Individuals with additional needs and disabled people may experience inequalities in their sexual health and wellbeing due to a variety of reasons, not limited to physical barriers to accessing services. Disabled people are significantly more likely to experience sexual violence compared with people without disabilities (48). Higher rates of STIs are also seen in individuals who experience multiple disabilities, compared to those who are not disabled (49).
3.12 People with a learning disability
In Surrey, an estimated 1.8% of the population have a learning disability (50). Individuals with learning disability (LD) may face inequalities in achieving sexual wellbeing for a range of reasons (51). Topics such as sexual health, contraception and relationships may not be discussed due to stigma, as well as fears around consent, exploitation and abuse, and unintended pregnancy. However, with the right support and advice, individuals with learning disability are able to achieve healthy and fulfilling relationships, and have a right to do so (51).
Surrey and Borders Partnership (SABP) NHS Foundation Trust provides support to people with LD in Surrey. They provide a community-based nurse-led service to support individuals with sex and relationship education and to help them foster healthy sexual behaviours. There were 13 referrals to this service in 2022, 32 in 2023 and 17 in 2024 [unpublished data from SABP], the service has a waiting list indicating that there is a greater need for this service.
The second annual ‘Shout About Sex’ day was held by the community learning disability team in November 2024, to provide an opportunity for people with LD, their families, and support workers to learn about sexual health, healthy relationships and contraception, with a range of appropriate resources available, for example, Easy Read advice sheets.
3.13 People who are neurodivergent
People who are neurodivergent, including individuals with Autism Spectrum Disorder (ASD) and Attention-Deficit/Hyperactivity Disorder (ADHD) may be at higher risk of experiencing challenges relating to sexual health and wellbeing compared to neuro-typical individuals, including: sexual dysfunction; being a victim of sexual assault; child sexual exploitation; engaging in high-risk sexual behaviours and feeling dissatisfaction with sexual relationships (52). Compared with neuro-typical individuals, those with ASD were less likely to identify as heterosexual, and more often identified with other sexual orientations (52). Therefore, people who are neurodivergent are likely to have a higher sexual and reproductive health need compared with neuro-typical individuals, and are also likely to face significant barriers to accessing services (53).
3.14 People with severe mental illness
The Severe Mental Illness (SMI) register includes patients who have been diagnosed with a range of mental health illnesses including schizophrenia, bipolar affective disorder and other psychoses. In 2020/21, 0.87% of people in Surrey Heartlands Integrated Care Board (ICB), and 0.76% of people in Frimley ICB were on the SMI register (compared to 0.95% nationally) (54).
People with SMI in the UK face significant sexual health inequalities, including higher rates of STIs and unplanned pregnancies, with barriers to accessing contraception and sexual health services (55). There is limited evidence of interventions to address this in the UK (56) although one study did consider tailored sexual health interventions for people with SMI and showed these approaches are feasible and beneficial (57).
3.15 People living with HIV
People living with HIV can face significant challenges in achieving sexual wellbeing. Early access to HIV services, including medical management with antiretroviral therapy, is fundamental for individuals living with HIV (58). However, holistic advice and support on fostering healthy relationships, navigating any struggles with sexual identity and/or a diagnosis of HIV, and support with sharing a HIV diagnosis with partners is vital (58). Individuals may require services that support their own sexual health, for example, STI testing and treatment, as well as access to preventative measures to prevent onward transmission to partners, such as condoms (58). Stigma is still experienced by many individuals living with HIV, and can significantly impact on the mental and sexual health of individuals.
In 2023, the sexual health service introduced the first HIV peer support worker role in Surrey. The aim of the role is to provide emotional, information, and practical support to individuals living with HIV, drawing on their own lived experience to foster trust, reduce stigma, and promote health and wellbeing.
3.16 People experiencing problematic substance use
In Surrey in 2020-2021, the most common problem substances for adults in treatment were opiates, alcohol and cannabis (59). It is estimated that 8,308 people in Surrey had alcohol dependency in 2019-2020, representing a prevalence rate of 6.81 per 1,000 adult population, which is lower than the England average (11.32 per 1,000 adult population) (60). In Surrey in 2019-20, the estimated number of people using opiates and/or crack cocaine are 3,721 (prevalence rate of 4.99 per 1,000 adult population, lower than the rate in England of 9.54) [61].
People experiencing problematic drug or alcohol use often experience sexual health inequalities. Those reporting recent illicit drug use and high amounts of alcohol are more likely to engage in high-risk sexual behaviours, such as having multiple sexual partners and inconsistent condom use, leading to increased rates of STIs and unplanned pregnancies (62, 63, 64).
Chemsex refers to the use of drugs before or during planned sexual activity to sustain, enhance, disinhibit or facilitate the experience, typically among men who have sex with men (65). It is a risk due to the risks to physical and mental health, including the spread of blood borne viruses (65).
3.17 People experiencing domestic abuse
In Surrey, from April 2021 to September 2022, there were 11,102 referrals to domestic abuse outreach providers from 7,729 individuals (some individuals were referred multiple times) (66).
Experience of domestic abuse can lead to increased sexual health issues including STIs and an increase in unplanned pregnancy (67). Research indicates that women subjected to domestic abuse are more than twice as likely to seek emergency contraception compared to those not exposed to such violence (68). This increased need arises in part from factors such as reproductive coercion, where abusers manipulate or sabotage contraceptive methods, leading to unplanned pregnancies and heightened risks of STIs. Research also indicates that people living with HIV are 2 to 4 times more likely to experience intimate partner violence (69).
In 2024, the sexual health service introduced an independent domestic and sexual violence advocate (IDSVA) role to provide validation, emotional and practical support to victims and survivors of domestic and sexual abuse.
3.18 People in contact with the criminal justice system
In December 2024, there were 2,653 people in prison in Surrey across five prisons: His Majesty’s Prison (HMP) & Young Offender Institution (YOI) Bronzefield; HMP Coldingley; HMP & YOI Downview; HMP High Down; HMP Send (70) and remand prisoners from Surrey are held at HMP Wandsworth.
In the UK, people in prison have higher rates of some STIs (71) and, in response, the British Association for Sexual Health and HIV (BASHH) have developed a standard for the management of sexual health in prisons (72).
Separate Health Needs Assessments have been conducted for each of the 5 prisons in Surrey (last published in 2021, with an update expected in 2025) (73). These needs assessments cover the challenges and complexities of delivering healthcare services in a prison setting, including some reference to sexual health and contraception services.
4 Surrey sexual and reproductive health needs
4.1 Sexually transmitted infections
4.1.1 Headline findings and key implications
- Whilst rates of diagnosis of all STIs in Surrey remains below the national average (74), there is an upward trend in rates of chlamydia (75), gonorrhoea (76), syphilis (77) and HIV (77) and they remain higher than pre-pandemic rates. This is likely to represent an increase in the burden of STIs (rather than increased diagnosis due to increased testing), given the rates of STI testing (excluding chlamydia aged under 25) are lower compared to 2019 (78). It may also indicate an improvement in targeted testing for those at higher risk.
- The proportion of people first diagnosed with HIV in the UK who receive a late diagnosis in Surrey is significantly higher than the national average (79), which also poses a higher risk of complications to the individual, as well as increased potential for onward transmission prior to diagnosis.
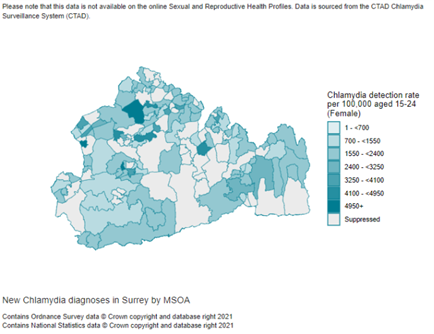
- In Surrey, the chlamydia detection rate in females aged 15 to 24 years was 1,781 per 100,000, compared with an England average of 1,962 per 100,000, in 2023 (80). These are both lower than the national target of 3,250 per 100,000 or more.
- This poses a threat to the sexual health and wellbeing of individuals in Surrey and healthcare services, due to pressures on sexual health services, the burden of complications of untreated STIs, as well as higher risk of onward transmission of STIs propagating the rising rates of STIs further.
- The rise in STIs is unlikely to be solely attributable to recent increases in testing (78).
- Other factors are associated with rising rates of STIs, include less use of condoms, which may be driven by the protection against HIV offered by PrEP, and use of LARC as a contraceptive, instead of a barrier method (81). There are also changes in sexual behaviour and social norms around relationships, including the use of social media and dating apps to meet partners, which may drive an increase in the number of sexual partners (82).
- Successful reduction in rates of genital warts has been achieved (83), due to the introduction of the HPV vaccine, however declining vaccination coverage may threaten this (84).
- Whilst sexual violence (85), including female genital mutilation (FGM) (86) affect a small number of individuals in Surrey, their impact on the individual is significant.
The trends seen for each STI are discussed in detail below.
4.1.2 All STIs
4.1.2.1 Diagnosis of all new STIs
There were 5,891 new STI diagnoses in Surrey in 2023, which was 23.7% higher than in 2022, although similar to levels in 2019 prior to the pandemic (6,005 new diagnoses) (74). The rate of all new STI diagnoses in Surrey is 485 per 100,000 people in 2023 (74). This is lower than the England average of 704 per 100,000 people. The rate of all new STI diagnoses in Surrey has risen from 392 per 100,000 people in 2022 (74). The rates in Surrey have been consistently below the England average over the past decade. Nationally, rates of all new STI diagnoses are more likely to be above the national average in more deprived areas (74).
In Surrey, there is variation in the rates of diagnosis of new STIs across boroughs, ranging from 344 per 100,000 in Waverley, to 764 per 100,000 in Epsom and Ewell in 2023.
A dashboard has been developed allowing exploration of the data in this section: Public_Sexual Health Dashboard 2025_v2 | Tableau Public

4.1.2.2 All sexually transmitted infections, excluding chlamydia in under 25s
The testing rate for all STIs (excluding chlamydia in those aged under 25 years) was 2,615 per 100,000 in Surrey in 2023 (78). This is lower than the England average of 4,111 per 100,000. The testing rate for all STIs (excluding chlamydia in under 25s) has risen from 2,376 per 100,000 in Surrey in 2022 but remains lower than pre-pandemic rates (3,099 per 100,000 in 2019) (78). Over the last decade, STI testing rates (excluding chlamydia in under 25s) in Surrey have been consistently lower than the national average.
In Surrey, there is variation in the testing rate for all STIs (excluding chlamydia in those aged under 25 years), ranging from 2,007 per 100,000 in Waverley, to 3,508 per 100,000 in Guildford in 2023.
A dashboard has been developed allowing exploration of this data – this dashboard will be made live shortly and the link published in this chapter.
The proportion of STI tests that are positive (excluding chlamydia tests in those aged under 25 years) is 5.4% in Surrey in 2023 (87). In Surrey, this has risen from 4.1% in 2022. The proportion of positive tests is lower in Surrey than the England average of 7.3%, and has been consistently lower over the last decade (87). Across Surrey, the proportion of positive STI tests (excluding chlamydia tests in those aged under 25 years) in 2023 ranged from 3.9% in Elmbridge to 7.0% in Spelthorne. There was no clear association between boroughs with higher testing rates and the testing positivity rate. Although the reasons for this are unclear, this may indicate that rates of testing are not necessarily associated with need, in terms of prevalence of undiagnosed STIs.
In Surrey in 2023, there were 4,063 new STI diagnoses (excluding chlamydia in those aged under 25 years), which was 23.2% higher than in 2022, but similar to levels prior to the pandemic (4,464 new diagnoses in 2019) (88). This is 335 per 100,000 people in 2023 (89), which is lower than the England average of 520 per 100,000 people. Across Surrey the rate of new STI diagnoses (excluding chlamydia aged under 25) ranged from 242 per 100,000 in Waverley, up to 466 per 100,000 in Epsom and Ewell.
Nationally, there is an association between higher rates of new STI diagnoses and higher levels of deprivation (88). Rates of new STI diagnoses are more likely to exceed the national average in more deprived areas.
4.1.3 Chlamydia
4.1.3.1 Background
Chlamydia is the most common bacterial STI in the UK, caused by the Chlamydia trachomatis bacterium (89). Whilst chlamydia infection is often asymptomatic, females are particularly vulnerable to long-term complications of untreated chlamydia infection, including pelvic inflammatory disease (PID), as well as an increased risk of ectopic pregnancy and infertility (89). For this reason, since June 2021, the NCSP focused on detecting chlamydia in cis-gender women, transgender men and non-binary individuals with a womb and/or ovaries aged 15 to 24 years old (90). The majority of chlamydia testing in Surrey is done by specialist sexual health services either online or in person, and a small number via pharmacies.
4.1.3.2 Females aged 15 to 24 years
In Surrey, 20.5% of females aged 15 to 24 years have been screened for chlamydia, which is similar to the England average (20.4%) (75). In Surrey and England, the coverage has been stable since 2022 (19.9% and 20.8%, respectively). Nationally, the highest coverage of screening is in individuals in the third most deprived decile (23.8%), and the lowest is in the least deprived decile (17.3%) (75). In Surrey, the lowest coverage rates were seen in Surrey Heath (18.9%), Mole Valley (18.7%), Waverley (16.8%), Runnymede (16.4%) and Spelthorne (15.6%), with rates lower in these areas compared with the national average (20.4%). In Epsom and Ewell (32.5%) and Guildford (25.7%) coverage was higher than the national average (20.4%).
In Surrey in 2023, there were 1,170 cases of chlamydia detected in females aged 15 to 24 years, a 30.9% increase since 2022 (75). In Surrey, the chlamydia detection rate in females aged 15 to 24 years was 1,781 per 100,000, compared with an England average of 1,962 per 100,000, in 2023 (80). These are both lower than the Public Health Outcomes Framework (PHOF) target of 3,250 per 100,000 or more; a target set to indicate adequate detection of chlamydia (including asymptomatic cases) (22,91). In Surrey the detection rate has increased from 1,361 per 100,000 females aged 15 to 24 years in 2022 (a 30.9% increase) and has recovered to pre-pandemic levels (1,521 per of 100,000 females aged 15 to 24 years in 2019) (80).
Nationally, there is an association between higher levels of deprivation and a higher chlamydia detection rate in females aged 15 to 24 years. The detection rate is highest in those living in the most deprived decile (2,255 per 100,000 females aged 15 to 24 years), and lowest in the least deprived decile (1,500 per 100,000 females aged 15 to 24 years) (80).
In Surrey, there tends to be higher chlamydia detection rates in females aged 15 to 24 years in the north west of Surrey (Figure 4.1). At a borough level, chlamydia detection rates are lower than the PHOF target across all areas, with the exception of Epsom and Ewell (3,359 per 100,000). Detection rates were lowest in Waverley (1,311 per 100,000). The four boroughs with the lowest coverage of chlamydia screening in females aged 15 to 24 years (Mole Valley, Waverley, Runnymede, Spelthorne) also had the lowest chlamydia detection rates in this group. Runnymede and Spelthorne have the highest proportion of households considered to be deprived (91).
4.1.3.3 Males aged 15 to 24 years
In Surrey in 2023, the chlamydia detection rate in males aged 15 to 24 years was 935 per 100,000, compared with 1,042 per 100,000 in England (92). Nationally, this follows a similar trend over time, as for females of the same age, and detection rates tend to exceed the national average in areas of higher deprivation (80, 92). In Surrey, the rates were highest in Epsom and Ewell (2,302 per 100,000) and lowest in Spelthorne (627 per 100,000).
4.1.3.4 Individuals aged 25 years and over
In all individuals aged 25 years and over in Surrey, the chlamydia diagnostic rate was 156 per 100,000 people, which is lower than the England average of 223 per 100,000 (93), in 2023. In Surrey, the rate has increased from 93 per 100,000 in 2013, and from 120 per 100,000 in 2022, with a parallel rise seen nationally (93). Nationally, there is a trend of higher diagnostic rates in areas of higher deprivation (93).
In Surrey, the chlamydia diagnostic rate in individuals aged 25 years and over is higher than the national average in Epsom and Ewell (306 per 100,000). The lowest rates were seen in Mole Valley (132 per 100,000), Elmbridge (102 per 100,000) and Waverley (98 per 100,000) in 2023.
4.1.4 Gonorrhoea
Gonorrhoea is the second most common bacterial STI in the UK, caused by Neisseria gonorrhoeae, and it is used as a used as marker for rates of unsafe sexual activity. (94). Antimicrobial resistance is a key issue in the management of gonorrhoea, with ceftriaxone (the recommended first-line treatment) being one of the few remaining antibiotics that can treat gonorrhoea infection effectively (95).
In Surrey in 2023, there were 819 diagnoses of gonorrhoea, a 32.7% rise since 2022 (76). In Surrey, the rate of gonorrhoea diagnosis in 2023 was 67 per 100,000 people (76). This is lower than the England average rate of 149 per 100,000 people, and South East average of 83 per 100,000 people. The rate of diagnosis of gonorrhoea in Surrey has increased from 29 per 100,000 people in 2013, and from 51 per 100,000 in 2022 (76). Over the last decade, gonorrhoea diagnosis rates in Surrey have been consistently lower than the England average.
Nationally, there is an association between higher rates of gonorrhoea diagnosis in areas of higher deprivation, with rates above the England average in the first to fourth most deprived deciles and the sixth most deprived decile, with lower rates in the first to fourth least deprived deciles (76). Across Surrey, the highest rate of gonorrhoea diagnosis was in Runnymede (87 per 100,000) which was almost double that compared with the lowest rate seen in Elmbridge (45 per 100,000) in 2023.
In England, a new gonorrhoea vaccination program will be launched in August 2025, making it the first country to offer such a program. The program will primarily target gay, bisexual, and other men who have sex with men (GBMSM) who are at higher risk of infection, but others may also be eligible based on risk factors.
4.1.5 Syphilis
Syphilis is an STI caused by the Treponema pallidum bacterium (96). Syphilis infection can be effectively treated with antibiotics. Long-term consequences of untreated syphilis infection include cardiovascular and neurological complications. Perinatal transmission of syphilis can occur, which, if left untreated, can cause stillbirth, or congenital infection in the baby.
In Surrey in 2023, there were 108 new cases of syphilis (97). The rate of syphilis diagnosis in Surrey in 2023 was 8.9 per 100,000 people (97). Rates in Surrey have risen from 2.7 per 100,000 people in 2012, and plateaued since 2022 (8.8 per 100,000). Diagnostic rates in Surrey are consistently lower than the England average (16.7 per 100,000 in 2023) (97).
Nationally, diagnosis of infectious syphilis is also rising, by 9.4% between 2022 and 2023 (98). Whilst the number of diagnoses is highest in GBMSM, and individuals aged 25-34 years, the number of diagnoses in heterosexual people has shown the greatest increase between 2022 and 2023 (29% increase in women who have sex with men, and 17% increase in men who have sex with women) (98).
Nationally, there is an association between higher levels of syphilis diagnosis in individuals living in more deprived areas, although the highest rate is in individuals living in the fourth most deprived decile (97).
4.1.6 HIV
Prompt diagnosis of HIV infection and early treatment with antiretroviral therapy has revolutionised the outlook for those diagnosed with HIV, with associated dramatic improvements in life expectancy (99). A late diagnosis of HIV is defined as individuals who do not have evidence of recently acquiring HIV with a CD4 count of less than 350 cells per mm3 around the time of diagnosis (79), (a CD4 count is a blood test that measures a type of white blood cell that is crucial for immune system function, helping fight off infections). Challenges remain in relation to late diagnosis, resulting in significant levels of preventable morbidity and mortality, as well as and stigma related to HIV testing and diagnosis (99).
In Surrey in 2023, the HIV testing rate was 2,180 per 100,000 people, which was lower than the England average of 2,771 per 100,000 (100). However, encouragingly, the testing rate in Surrey has increased from 1,755 per 100,000 in 2022 (100). This may be due to a variety of reasons, including increased opportunistic testing at sexual health clinics (for example, in individuals attending for LARC) and increases in online testing (101), which is likely supported by campaigns to increase awareness of HIV testing for both residents and professionals (for example National HIV Testing Week) (102).
However, the rise in HIV testing reflects increases in testing in some groups, with falls in other groups. For example, nationally the number of tests done for GBMSM increased by 34% between 2019 and 2023, whilst there was a 10% fall in the number of tests for heterosexual and bisexual women and a 22% decrease in tests done for heterosexual men since 2019 (101). Nationally, testing rates in more deprived areas are more likely to be higher than the national average, compared to less deprived areas (100).
In Surrey, the HIV testing rate exceeded the national average in Guildford (3,027 per 100,000). The HIV testing rate was lowest in Tandridge (1,812 per 100,000), Mole Valley (1,797 per 100,000) and Waverley (1,704 per 100,000).
In Surrey in 2023, there were 107 newly diagnosed cases of HIV, which was 40.8% higher than in 2022 (77), this is a rate of 8.7 per 100,000 new cases of HIV, which was similar to the England average of 10.4 per 100,000 (77). In Surrey the diagnosis rate had risen from 6.2 per 100,000 in 2022, this increase likely reflects the increase in testing. Of all the new HIV diagnoses in Surrey, 43 were in people first diagnosed with HIV in the UK, with the remaining individuals (64) having previously received a diagnosis abroad (103). A HIV diagnosis abroad means a person was tested and diagnosed with HIV while living in another country. In Surrey, the rate of HIV first diagnosed in the UK has fallen from 6.7 per 100,000 in 2013 to 3.5 per 100,000 in 2023, and has stabilised in recent years (103). A similar trend has been seen nationally, with over half of new diagnoses of HIV having previously been diagnosed abroad (101). Of individuals first diagnosed in England, in 2023, 61% of those were born outside the UK.
Nationally, 49% of new diagnosis of HIV that were first diagnosed in England were among individuals where transmission of HIV was from sex between men and women (a 36% increase for men and 30% increase for women since 2022), whilst 29% were from exposure to HIV from sex between men (101). The majority of new diagnoses that are first made in England are in individuals aged 25 to 49 years (70%), and this is the only age group that has seen a rise in the number of new diagnoses since 2019 (by 7%) (101).
In Surrey, the highest rate of new HIV diagnoses was seen in Spelthorne (18.3 per 100,000), which was higher than the national average (10.4 per 100,000). The lowest rate was in Runnymede (3.3 per 100,000) which was lower than the national average. Across Surrey, there was no clear association between testing rates and diagnosis rates for HIV between boroughs.
In people with HIV first diagnosed in the UK, 52.5% received a late diagnosis in Surrey, compared to an average of 43.5% in England (79). The proportion of individuals receiving a late diagnosis was higher than the overall Surrey average for GBMSM (56.5%) (104) and heterosexual men (78.3%) (105) and was lower for heterosexual and bisexual women (48.6%) (106) in 2023. Nationally, those living in the least deprived decile had the highest rate of late diagnosis of HIV in people first diagnosed in the UK (50.5%) (79).
Nationally, the majority of diagnoses made in individuals aged 50-64 years (53% of new diagnoses) and 65 years and over (55% of new diagnoses) are late diagnoses (101). Other groups where a high proportion of HIV diagnoses are late include: men who have sex with women (51% of new diagnoses), and individuals of Black and Asian ethnicity (44% and 43% of new diagnoses, respectively) (101).
In Surrey in 2023, the HIV prevalence rate in those aged 15 to 59 years was 1.61 per 1,000 in 2023, which was lower than the England average of 2.40 per 1,000 (107). The prevalence rate in Surrey has been relatively static in recent years. Nationally, prevalence rates are more likely to be higher than the England average in more deprived areas (107). Figure 4.2 shows a heat map of prevalence rates of HIV in Surrey. The HIV diagnosed prevalence rate in those aged 15 to 59 years is highest in Woking (2.22 per 1,000) and lowest in Waverley (1.18 per 1,000)
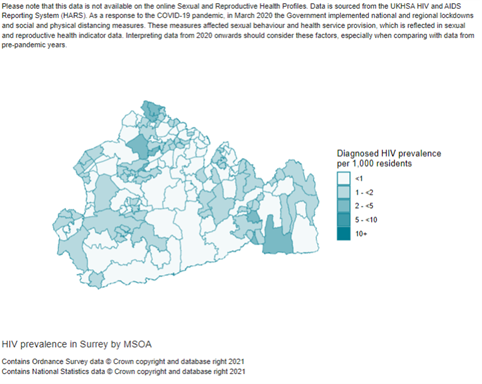
4.1.7 Genital warts and HPV vaccination
Genital warts are the most commonly diagnosed viral STI in the UK. The vast majority of genital warts are caused by human papillomavirus (HPV) infection. A national vaccination programme for HPV was introduced for girls aged 12 to 13 years in 2008 and was extended to 12 to 13-year-old boys in 2019 (22). This vaccine protects against the HPV subtypes responsible for the majority of cases of cervical cancer and also protects against genital warts (22). Eligibility for HPV vaccination was extended to include gay, bisexual and other men (GBMSM) who have sex with men aged up to 45 years, as well as other individuals who may be at higher risk from HPV, in 2018 (83). (108).
The proportion of 12 to 13-year-old who have received at least one dose of the HPV vaccine in Surrey 2022/23 was 77.3% (84). This is higher than the England average of 71.3%. In Surrey, the vaccination coverage has fallen from 89.8% in 2014-15 and has consistently been below the goal of a coverage of over 90%. Vaccination coverage rates are higher in females (77.3%) compared to males (70.7%) in Surrey, with a similar trend seen nationally (84). Nationally, there is also an association between lower coverage of the HPV vaccine, and higher deprivation. The highest coverage rate is in the least deprived decile, with 80.4% coverage, and the lowest coverage is in the most deprived decile, with 57.7% coverage (84).
This vaccination programme has led to dramatic reductions in the rates of first episode genital warts in the population, particularly younger adults, due to both direct and indirect protection from the HPV vaccine (22). For example, between 2019 and 2023, there was a 49.7% reduction in the rates of first episode genital warts in women aged 15 to 17 years (22).
In Surrey in 2023, there were 479 new cases of genital warts, a 3% rise since 2022 (83). In Surrey, the rate of genital warts diagnosis was 39.2 per 100,000 people in 2023 (83). This is lower than the England average of 45.8 per 100,000 people. The rate in Surrey has decreased dramatically from 109.3 per 100,000 people in 2012 and plateaued since 2019 (39.5 per 100,000) (83). Nationally, rates of genital warts diagnosis are highest in the third to sixth most deprived deciles, with lower rates in the most and least deprived deciles (83).
4.1.8 Genital herpes
Genital herpes is caused by the herpes simplex virus (HSV) and causes ulcerative disease, that can increase the risk of HIV transmission (109). Whilst many infections are asymptomatic, it can cause genital ulceration, as well as having the potential to cause more severe disease in neonates and immunosuppressed individuals (84).
In Surrey in 2023, there were 494 new cases of genital herpes, a rise of 24.8% since 2022 (110). In Surrey, the rate of genital herpes diagnosis was 41.1 per 100,000 people in 2023. This is lower than the England average of 47.6 per 100,000 people (110). In Surrey, the rate has risen from 32.9 per 100,000 people in 2022 but is lower than pre-pandemic levels (46.0 per 100,000 people in 2019) (110). Over the last decade, the rates of genital herpes diagnosis in Surrey have been consistently lower than the England average.
Nationally, rates of genital herpes diagnosis are highest in the second to sixth most deprived deciles, with lower rates in the most and least deprived deciles (110). In Surrey, the highest rate of genital herpes diagnosis was in Guildford (59.7 per 100,000) and the lowest was in Surrey Heath (30.7 per 100,000).
4.1.9 Mycoplasma genitalium
Mycoplasma genitalium is a bacterial STI that can cause urethritis (non-gonococcal urethritis), cervicitis and PID (111). Due to concerns regarding antimicrobial resistance of Mycoplasma genitalium to commonly used antibiotics in clinical practice, a Mycoplasma genitalium Antimicrobial Resistance Surveillance (MARS) system was set up in 2023 to monitor this issue (111).
In Surrey in 2023, there were 131 new cases of mycoplasma genitalium, a rise of 29.7% since 2022 (112). In Surrey, rates of diagnosis of mycoplasma genitalium were 10.8 per 100,000 people in 2023 (112). This is lower than the England average of 15.6 per 100,000 people. In Surrey, the rate of diagnosis of mycoplasma genitalium has risen slightly from 8.3 per 100,000 people in 2022 (112). Nationally, there is a trend of higher rates of mycoplasma genitalium diagnosis in more deprived areas (112).
4.1.10 Trichomoniasis
Trichomoniasis is an STI caused by the parasite Trichomonas vaginalis, that more commonly affects women than men. In Surrey in 2023, there were 72 new cases of trichomoniasis recorded, a rise of 10.8% since 2022 (113). In Surrey, the rate of trichomoniasis diagnosis was 5.9 per 100,000 people in 2023 (113). This is lower than the England average of 16.0 per 100,000 people in 2023 (113). The rate of trichomoniasis diagnosis has increased from 5.4 per 100,000 people in 2022 in Surrey. Nationally, there is an association between higher rates of trichomoniasis diagnosis and higher deprivation (113).
4.1.11 Shigella
Shigella is a bacterial infection previously associated with consumption of contaminated food and water in endemic countries (114). More recently, the majority of cases in England are acquired in individuals without a travel history, and are presumed to have been transmitted sexually, through faecal-oral contact (114).
In Surrey in 2023, there were 59 documented cases of sexually transmitted Shigella, a rise of 43.9% since 2022 (115). In Surrey, the rate of sexually transmitted Shigella is 12.0 per 100,000 adult male population. This is similar to the England average of 9.0 per 100,000 adult male population. In Surrey, the rate of sexually transmitted Shigella has risen from 3.0 per 100,000 adult male population in 2016.
Nationally, there does not appear to be a clear trend between rates of sexually transmitted Shigella, diagnosed in adult males, and deprivation. Rates of sexually transmitted Shigella are highest in adult men with no travel history, who are presumed to be MSM (114). Highest rates are seen in London (46%), with only 8% of cases of Shigella diagnosed in Surrey and Sussex (114).
4.1.12 Mpox
Mpox is a viral zoonotic infection that causes skin lesions, as well as non-specific viral symptoms, such as fever, muscle aches and swollen lymph nodes (116, 117). It can be transmitted via direct contact with skin lesions, such as during sexual contact, as well as through contact with bodily fluids, and contaminated objects, e.g. towels (117).
Mpox has traditionally been associated with travel to endemic areas (West and Central Africa) or contact with travel-associated cases (116). However, in 2022 there was an outbreak of cases that were acquired in the UK, caused by clade IIb infection (116). In 2022, there were 3,553 cases of confirmed or highly probably mpox clade IIb in England. This outbreak disproportionately affected GBMSM (116), with approximately 90% of cases occurring in GBMSM (118).
In 2023 and 2024, there were a total of 406 cases reported in England, of which 182 were presumed to have been acquired in the UK (95 still awaiting classification) (116). In June 2022, mpox clade IIb was down-classified in the UK and is no longer considered a high consequence infectious disease (HCID), which means that these cases no longer required care in HCID centres with more stringent guidance on management and personal protective equipment (PPE) requirements. In January 2023, there was a down-classification of all clade II mpox (119).
4.1.13 Chemsex
Chemsex refers to “the use of drugs before or during planned sexual activity to sustain, enhance, disinhibit or facilitate the experience”, typically among men who have sex with men (65). It is a risk due to the risks to physical and mental health, including the spread of blood borne viruses (65). Substance misuse services (i-access, Via and Catch22) and sexual health services in Surrey must work in partnership to support individuals who engage in chemsex and would like help and advice. The sexual health service and outreach team have chemsex packs that can be given to clients but the team report that the disclosure of chemsex is low.
4.1.14 Sexual offences
In Surrey, in 2022-23 there were 2.0 sexual offences per 1,000 people. This is lower than the England average of 3.0 per 1,000 people (85). In Surrey, the rate has risen from 0.4 per 1000 in 2012-13, with a similar trend seen nationally. Nationally, there is an association between higher levels of sexual offences and higher deprivation. The highest rate is in the most deprived decile, at a rate of 4.1 per 1000 people, and the lowest rate is in the least deprived decile, at a rate of 2.0 per 1000 people.
Risk factors for experiencing intimate partner abuse and violence include: history of anxiety and depression; substance misuse; risky sexual behaviours; witnessing previous domestic violence; parental separation and previous sexual abuse (120).
Surrey is home to several support organisations for individuals experiencing domestic or sexual abuse (121), and the Solace Sexual Assault Referral Centre (SARC) provides forensic examination, as well as medical, emotional and practical support for individuals who have been sexually assaulted or raped (122).
4.1.15 Female genital mutilation (FGM)
FGM involves the injury of a female’s genitalia, including the alteration, damage to, or partial or total removal of a female’s external genitalia, with social, religious or cultural reasons commonly reported as reasons for FGM (123). It is most often performed in childhood, and is more common in Africa, the Middle East and Asia, or in individuals of descent from these countries (123). FGM and associated activities (including arranging FGM) are illegal under the Female Genital Mutilation Act (2003) (124).
FGM is associated with significant physical health issues, including: infection; pain; difficulty urinating; menstrual problems; painful sexual intercourse and risk of complications during childbirth (123). The traumatic experience and consequences can have long-lasting mental health impacts, and the procedures themselves can be fatal (123).
Regulated professionals, including teachers, social workers and medical professionals have a legal duty to report any known cases of FGM to the police (124). Any cases of suspected FGM, or concern that an individual is responsible for the perpetration of FGM should also be reported to the police (124). In Surrey in 2023, 24 healthcare providers recorded 5 cases of FGM (number ranges between 1 and 7but has been rounded to 5 to protect confidentiality), and these were reported by midwifery and gynaecology services (86). Where country of birth was recorded, these individuals were born in Northern and Western Africa.
4.2 Reproductive and contraceptive health needs
4.2.1 Headline findings and key implications
- Access to high quality contraception and advice, as well as allowing individuals to choose their preferred contraceptive method are important to reduce teenage pregnancy and abortion rates.
- In Surrey, the rate of teenage pregnancy is lower than England and the rate of under 18s and under 16s conceptions in 2021 were lower compared to 2018. Although there is variation across the county, all districts and boroughs in Surrey have rates lower than the England average. However, although rates of under 18s conception in Surrey have been declining, this appears to have started to plateau which has prompted further work to develop the Surrey Teenage Pregnancy Prevention Action Plan (see Section 2.2.3)
- Similarly, the total abortion rate, repeat abortion rate in those under 25 years old, abortions after a birth in those under 25 years old, and the rate of abortion in those 25 years and older are all lower in Surrey compared to England. However, the total abortion rate has been increasing over time.
4.2.2 Teenage pregnancy
Contraception JSNA Fingertips dashboard | Tableau Public
There have been continued declines in under 18s conception rates in England and Surrey, with Surrey remaining below the national average. In 2021, the rate of conception in under 18-year-olds was 8.0 per 1,000 population, compared to 13.1 per 1,000 population in England (the rates for under 16s conception were 1.0 per 1,000 population in Surrey, and 2.1 per 1,000 population in England). The 2021 teenage pregnancy data showed the first rise in 14 years, sounding a note of caution and in Surrey overall the rate has plateaued.
Historically, Runnymede and Spelthorne consistently had higher teenage pregnancy rates, but this trend appears to be changing and approaches to teenage pregnancy prevention no longer focuses on borough and districts. See Section 2.2.3 for further information on Surrey’s Teenage Pregnancy Prevention Plan.
Among 18-year-olds who conceived, the proportion leading to an abortion has been increasing, with 70.5% of conceptions in this age-group in Surrey leading to an abortion in 2021 (compared to 53.4% in England). Within Surrey, this proportion also varied by district and borough, although this has fluctuated over time, partly due to relatively small numbers of abortions in this age-group in some districts and boroughs.
Further data on abortion rates in all women in Surrey are provided in Section 4.2.3.
4.2.3 Abortion rates
Contraception JSNA Fingertips dashboard | Tableau Public
The total abortion rate nationally and in Surrey has increased between 2017 and 2021, although Surrey remains below the national average. In 2021, the total abortion rate was 15.7 per 1,000 female population aged 15-44 years old, compared to a rate of 19.2 per 1,000 population in England. Rates of abortions in those aged 25 and older, have also been increasing since 2017 in both Surrey and England (rates in 2021 of 14.8 per 1,000 female population aged 25-44 and 17.9 per 1,000 population respectively). Potential drivers for increases in abortion rates could be due to improved access to early medical abortion (EMA) methods, reduced access to contraception, or changes in the type of contraception used. In addition, financial stress from the cost-of-living crisis in England could contribute to increasing abortion rates. Conversely, rates of abortions in those under 18 years of age have been decreasing between 2017 and 2022, with a rate of 4.6 per 1,000 females aged 15-17 in Surrey compared to 6.5 per 1,000 population in England.
Among women under 25 years old who had an abortion, the proportion who had previously had a birth has remained relatively stable over time and is lower than the national average. In 2021, 18.4% of those who had had an abortion under 25 years old in Surrey, and 26.0% in England, had previously had a birth. The proportion of women who had an abortion under 25 years old who had had a previous abortion also remained relatively stable. In 2021 in Surrey, 29.3% of those who had had an abortion under 25 years old in Surrey had previously had an abortion (compared to 29.7% in England).
The proportion of abortions under 10-weeks has been increasing since 2017, although remained relatively stable over the past two years nationally and in Surrey. In 2021, 88.7% of abortions in Surrey were under 10-weeks, compared to 88.5% of abortions nationally.
5 Evidence base for interventions promoting sexual and reproductive health
5.1 Sexual health
5.1.1 NICE Quality Standards for Sexual Health, 2019
NICE (the National Institute for Health and Care Excellence) published a quality standard (QS178) for sexual health in 2019 (125). The six quality statements included are:
- People are asked about their sexual history at key points of contact
- People identified as being at risk of STIs have a discussion about prevention and testing
- Local authorities provide a range of condom distribution schemes tailored to the needs of their populations
- People contacting a sexual health service about an STI are offered an appointment that is within 2 working days
- MSM have repeat testing every 3 months if they are at increased risk of STIs
- People diagnosed with an STI are supported to notify their partners
Progress against these quality statements in Surrey include:
- In the 2023-24 financial year 100% of individuals accessing the specialist sexual health service had a sexual history taken.
- The proportion of working days in 2023-24 where an appointment at a specialist sexual health service was available within 2 working days ranged from 38% to 95%, however, walk-in clinics are open every working day. It is important to note that this standard relates to individuals contacting the service regarding an STI, and not all individuals will want, or need, an appointment within two working days. Also, individuals are triaged based on their symptoms to ensure that patient care is prioritised effectively, and those who need an urgent appointment receive one.
- In 100% of cases, there was a partner notification plan documented within 4 weeks for index cases with a new diagnosis of an STI. The C-card condom distribution scheme (CDS) is available in Surrey from a range of community settings, although uptake is not as high as the need suggests (further details in section 6.9).
5.1.2 Other sexual health guidelines
Several organisations produce national guidelines to support individuals working in sexual health to provide evidence-based services and care, including:
- BASHH: UK national guideline for the management of infection with Chlamydia trachomatis, 2015 (updated 2018) (126)
- BASHH: UK national guideline for the management of infection with Neisseria gonorrhoea, 2018 (updated 2020) (127)
- BASHH: UK guidelines for the management of syphilis, 2024 (128)
- The British HIV Association (BHIVA), BASHH, British Infection Association (BIA) and the Royal College of Emergency Medicine (RCEM) Joint Working Group: Rapid guidance on opt-out blood-borne virus testing in high-prevalence and extremely high-prevalence acute medical settings and emergency departments, 2024 (129)
- BASHH, BHIVA, BIA: Adult HIV testing guidelines, 2020 (130)
- BASHH, BHIVA: UK guideline for the use of HIV post-exposure prophylaxis, 2021
- BHIVA, BASHH: The use of HIV pre-exposure prophylaxis, 2018 (131)
- BASHH, BHIVA, The Faculty of Sexual and Reproductive Healthcare (FSRH): The management of sexual and reproductive health of people living with HIV infection, 2008 (132)
- BASHH, BHIVA, Society of Sexual Health Advisors (SSHA): HIV partner notification for adults: definitions, outcomes and standards, 2015 (133)
- NICE: Reducing sexually transmitted infections [NG221] (134)
- NICE: HIV testing: increasing uptake among people who may have undiagnosed HIV [NG60] (135)
5.2 Contraception
5.2.1 NICE Quality Standards for Contraception, 2016
NICE published a quality standard (QS129) for contraception in 2016 (136). This includes four statements:
- Women asking for contraception from contraceptive services are given information about, and offered a choice of, all methods, including long-acting reversible contraception.
- Women asking for emergency contraception are told that an intrauterine device is more effective than an oral method.
- Women who request an abortion discuss contraception with a healthcare practitioner and are offered a choice of all methods when they are assessed for abortion and before discharge.
- Women who give birth are given information about, and offered a choice of, all contraceptive methods by their midwife.
5.2.2 Other contraception guidelines
Several organisations produce national guidelines to support provision of contraception and reproductive health services, including:
- FSRH: Standards & Guidance (including Guidelines, Statements and Clinical Standards) (137)
- NICE: Long-acting reversible contraception [CG30] (138)
- NICE: Contraceptive services for under 25s [PH51] (139)
- Royal College of Obstetricians & Gynaecologists (RCOG): Best practice in post-abortion contraception (140)
- RCOG, FSRH: Management of unscheduled bleeding in women using hormonal contraception (141)
5.2.3 Evidence of cost effectiveness
Investment in sexual health and contraception services in the UK has been shown to be highly cost-effective.
Evidence suggests there is an £9 saving for every £1 invested in contraception provision in England (Ref: Contraception: Return on Investment (ROI) report).
Public Health England (now UKHSA) has previously developed a tool that estimates that investment in the provision of LARC in primary care is highly cost-effective, with an estimated Return On Investment (ROI) across the system of £48 for every £1 invested.
Evidence shows that access to emergency contraception is cost-effective. For example, pharmacy access to emergency contraception can lower health sector costs by reducing the number of unintended pregnancies and associated healthcare costs. Additionally, the convenience and accessibility of pharmacies can reduce the need for more expensive healthcare interventions.
6 Sexual health service provision in Surrey
6.1 Commissioning of sexual health services in Surrey
Sexual health commissioning is complex and fragmented, with different parts of the system commissioning testing, treatment, contraception, screening and specialist provision (Table 6.1).
| Local Authority commissions: | Integrated Care Boards commission: | NHS England commissions: |
| – Sexual health service including most contraceptive services, STI testing – Outreach and prevention – Delivery of HIV pre-exposure prophylaxis (PrEP) |
– Most abortion services – Sterilisation – Vasectomy – Non-sexual-health elements of psychosexual health services – Gynaecology, including any use of contraception for non-contraceptive purposes – Adult specialist services for people living with HIV (from April 2025 |
– Contraception provided as an additional service under the GP contract and promotion of opportunistic testing and treatment for STIs and patient-requested testing by GPs – Sexual health elements of prison health services – Sexual assault referral centres – Cervical screening |
Taking a whole systems approach to sexual health involves integrating various services, stakeholders and partners to provide comprehensive care, advice and support, as well as an upstream approach, focusing on prevention. Good examples of this are the work of the sexual health outreach team, RSE guidance for schools via our Surrey Healthy Schools Approach, and the c-card scheme.
6.2 Specialist Integrated Sexual Health Service
6.2.1 Background to service
In 2022 Surrey County Council awarded a 5-year contract to Central North West London NHS Foundation Trust (CNWL) to deliver integrated sexual and reproductive health services. This was a joint procurement with NHS England who also awarded the contract for specialist HIV services in Surrey to CNWL.
The service delivers using a ‘hub, spoke and outreach’ model. The hubs are centrally located and offer a full range of services. Woking provides Level 2 service provision (which includes sexual health promotion, STI testing and treatment, emergency contraception, and IUD and implant insertion). Buryfields and Earnsdale clinics provide Level 3 service provision (which includes STI testing and treatment for more complex cases, e.g. individuals with recurrent infections, men with genital discharge, pregnant people, and infections at extra-genital sites, specialist HIV care, provision of PrEP, highly specialised contraception, and psychosexual services) [142]. Spoke clinics offer contraception, including, implant fitting and removal, chlamydia/gonorrhoea screening and condom distribution.
A key aim of this service model is to ensure that appointments for those needing specialist, complex sexual health services are available from the specialist provider. Services not requiring a specialist doctor are provided by other professionals in the specialist service or elsewhere (such as primary care or pharmacy), or online where appropriate.
6.2.2 Clinic locations
Appointments for in-person sexual health services are bookable online. These appointments provide a range of sexual health services, including assessment of genito-urinary symptoms, STI testing and treatment, contraception, and PrEP. Walk-in sexual health services are also available for time-critical issues, including emergency contraception, post-exposure prophylaxis for potential HIV exposure, and sexual assault after care (for individuals who do not wish to go to a sexual assault referral centre (SARC)). Clinics are held at Buryfields Clinic (Guildford), Earnsdale Clinic (Redhill) and Woking Clinic (Woking).
CNWL aims to ensure that their services are accessible for those with additional needs. In terms of booking appointments and provision of information regarding services, there is an Easy Read leaflet to summarise service information for individuals with learning disability or additional needs. The CNWL website supports Google translate and there is a text service for those who are deaf or hard of hearing. Furthermore, interpreters are available to book for appointments, including British Sign Language (BSL). Clinics can also accommodate the needs of individuals with mobility issues.
6.2.3 Online services
CNWL also provides online sexual health services in Surrey that are accessible via their website. STI testing is available for Surrey residents aged 16 and over who do not have symptoms, including at-home chlamydia, gonorrhoea, HIV and syphilis testing. Chlamydia and gonorrhoea testing kits for under 25s are also available to order online or via text message. PrEP is not available online.
Individuals can also access contraception online, including the progesterone only pill, and repeat prescriptions for the combined oral contraceptive pill, contraceptive patch and contraceptive ring.
6.2.4 Clinics and services for young people
There are specific clinics in Surrey that are available for young people. For individuals aged 15 years old and under, they are able to attend the walk-in clinics at Buryfields Clinic and Earnsdale Clinic. There is also a walk-in Young People’s Clinic called ‘Teen Tuesday’ for those aged 13 to 19 years on Tuesday afternoons at Buryfields Clinic, as well as pre-booked appointments at Buryfields Clinic, Earnsdale and Woking Hospital. In addition, there are contraception and sexual health advice clinics for those aged 13 to 25 years at Epsom Young People’s Clinic (NESCOT College), Weybridge Young People’s Clinic (Brooklands College) and Oxted Young People’s Clinic (Oxted Health Centre). Young people are also able to book appointments in the general clinics.
‘Clinic in a box’ is delivered by the sexual health outreach team and provides contraception and sexual health advice at an outreach location, such as a children’s residential home. This approach has been particularly helpful for engaging with young people who may find it hard to engage with sexual health services.
6.2.5 Prison sexual health service
CNWL is responsible for the integrated sexual health and HIV care across all five Surrey prisons, where those incarcerated are significantly more likely to be affected by multiple overlapping health inequalities. The service model delivers comprehensive, consultant-led, multi-disciplinary sexual health care, providing essential services such as STI diagnosis, HIV care, contraception, and sexual health promotion. In-reach clinics are held regularly according to the needs of the specific site, offering Level 3 STI services. One key aspect of the service is sexual health advisor support, offering partner notification and focus on reducing risk-taking behaviours through one-to-one sessions for high-risk individuals.
The service provides reproductive healthcare support including emergency contraception, long-acting reversible contraception (LARC), and perinatal care, prioritising high-risk pregnancies. Prison healthcare staff are regularly trained and upskilled in delivering basic sexual health care as an adjunct to specialist care. The team collaborates with other health and wellbeing services and actively participates in health promotion campaigns like National HIV Testing Week, fostering awareness and education among prisoners about sexual health, HIV prevention, and safer sex.
Along with addressing current sexual health needs, the service model also ensures continuity of care upon release, with referrals and connections to community-based sexual health services, ensuring that patients continue their treatment and prevention plans. Additionally, the provision of preventive care, including long-acting reversible contraception (LARC), vaccinations and HIV pre-exposure prophylaxis (PrEP), further enhances the health and wellbeing of prisoners by reducing the risk of unintended pregnancies and HIV transmission, promoting long-term sexual health outcomes.
6.2.6 Outreach team
Sexual health outreach is delivered as part of the integrated sexual and reproductive health service contract, delivered by CNWL.
The Surrey sexual health service outreach team play a crucial role in promoting and maintaining sexual health within the community. The team is essential in reaching out to inclusion health groups and populations and ensuring that everyone has access to the information and services they need to maintain their sexual health. The outreach team has a targeted approach, guided by a joint action plan with the public health team, which ensures that there is a focus on sexual health inequalities and differences in outcomes experience by groups in Surrey. The action plan is regularly reviewed to ensure that the areas of focus are current and appropriate. Health promotion is key in controlling the spread of STIs and preventing unintended pregnancies, as well as providing support and advice on positive sexual health.
The Surrey sexual health outreach team also manage the NCSP (see Section 6.2.9), and the C-Card condom distribution service (see Section 6.9).
The outreach team also deliver a range of training programmes for health and community professionals, including pharmacists and teachers/school staff. Other training includes the ‘c-card training’, ‘Reducing sexual health inequalities training’, and ‘Promoting healthy relationships to young people training’. The training programme aims to upskill health and community professionals with the skills to support young people and other priority groups. This is a key part of our whole systems approach to sexual health.
The outreach team attend a wide variety of events in the community, working with different groups. Examples include, school and college events, Surrey Pride, outreach at Public Sex Environments (PSE) and community events.
6.2.7 Sexual health promotion
As well as the work of the Sexual Health Service Outreach Team, the sexual health public health team contribute to sexual health promotion, ensuring that there is a focus on sexual health inequalities, supporting the reduction of STI rates and unintended pregnancies, and promoting positive sexual health, whilst taking a life course approach.
The sexual health public health team deliver a comprehensive calendar of communications throughout the year, amplifying national sexual health campaigns, such as World Aids Day or National HIV testing week, and deliver localised, targeted campaigns, such as promoting chlamydia testing for women aged 15-25. Campaign information is shared with a wide network of partners and contacts, and they are encouraged to promote the messages in their own organisations. The team promote the impact of sexual health on individuals and communities; the work of the sexual health service; share and learn good practice from beyond Surrey; attend health promotion and community events and share resources and condom packs with residents and professionals.
6.2.8 Safeguarding
The Surrey sexual health and HIV service has a Safeguarding Team who lead on issues regarding safeguarding for both young people and adults. The Surrey team consists of a named Safeguarding Lead, a Consultant with safeguarding responsibilities, and an Independent Domestic and Sexual Violence Advocate (IDSVA). The Surrey safeguarding team works closely with the London Sexual Health and HIV safeguarding team to provide on-call safeguarding advice to clinicians during clinic times. The Safeguarding Lead also provides regular safeguarding training, supervision and shared learning to ensure staff remain competent and compliant in safeguarding matters.
Patients are routinely asked about domestic abuse, sexual abuse and other harmful behaviours they may be facing as a way of enabling patients to disclose issues of concern to their clinician in a trusting and safe environment. The safeguarding team discuss all safeguarding referrals in the weekly Multi-Disciplinary Team (MDT) including all under 16-year-olds and complex cases.
In May 2024, the IDSVA joined the sexual health service. This is an important new role as it is the first time an IDSVA has been directly employed into the Surrey service. The IDSVA provides validation, emotional and practical support as an advocate to victims and survivors of domestic and sexual abuse and can refer onto other services, signpost and liaise with professionals. The service meets the needs of all victims and survivors of domestic and sexual violence, including female, male and LGBTQ+ survivors. Patients have reported confidence in the service being offered and that they feel it is a ‘safe space’ should they need to discuss or disclose safeguarding issues.
6.2.9 The National Chlamydia Screening Programme (NCSP)
CNWL deliver the NCSP for Surrey, which is available via their website, as well as other providers, including pharmacies.
In 2022, UKHSA facilitated a chlamydia care pathway workshop with the public health sexual health team and the sexual health service. The workshop provided a helpful opportunity to identify issues and make improvements to areas such as data quality and testing opportunities. As a result, a joint action plan was developed and implemented.
6.2.10 HIV services
In Surrey, CNWL provide specialist HIV services, at the Buryfields Clinic in Guildford, Earnsdale Clinic in Redhill and the Woking Clinic (HIV services are commissioned by NHS England, not the local authority). Therefore, whilst HIV prevention and testing is included within the scope of this JSNA, HIV management is outside of the scope.
6.2.11 Psychosexual therapy
The remit of psychosexual therapy is to provide advice and support for residents presenting with problems relating to psychological issues around sexual relationships and sexual behaviour. Local authorities are responsible for commissioning the sexual health aspects of psychosexual therapy. ICBs are responsible for commissioning the non-sexual health elements of psychosexual therapy.
In Surrey, CNWL provides a specialist sexual medicine service, led by a Consultant qualified in sexual medicine and psychosexual therapy and a psychologist. Patients with sexual problems are referred by their GP and assessed by the Consultant in a regular clinic, and an appropriate management plan is instituted. This could involve further investigation, one to one or group interventions.
In 2024, there were 331 patients seen by the Surrey sexual health service for psychosexual support.
6.2.12 Out of area specialist sexual health services
Sexual health services are designed to be available to those who need it whenever and wherever they require support. Individuals are therefore able to attend clinics across England, irrespective of where they live or where they are registered with a GP. Surrey residents may choose to access a service ‘out of area’, meaning that they choose to use a service outside of Surrey, and the opposite is also true, with non-Surrey residents using sexual health services within Surrey. The most commonly used out of area services for Surrey residents are provided by Epsom and St Helier University Hospitals, Hampshire and Isle of Wight Healthcare NHS Foundation Trust, Kingston Hospital NHS Foundation Trust, Chelsea and Westminster NHS Foundation Trust, and University Hospitals Sussex NHS Foundation Trust. These providers deliver services close to the Surrey borders. Surrey online services are only available to Surrey residents.
6.3 General practice
6.3.1 STI testing and treatment
STI testing and treatment is available in primary care, including general practice. This is usually done in response to symptoms, with asymptomatic individuals signposted to the self-test service provided by the sexual health service. STI testing may be performed for asymptomatic individuals, for example, prior to insertion of an intrauterine device (IUD) or as part of a wider panel of investigations, such as for fertility issues.
6.3.2 Contraception services
General practices play a key role in delivering contraception services, providing advice and a range of contraception methods including oral contraceptives, LARC, and emergency contraception. Variation exists in the services offered by GP practices, with some practices unable to offer LARC fitting, although they should signpost to another practice or service that are able to offer this.
GP Practices are commissioned by Public Health to deliver LARC and can also delivery LARC via the LARC Buddy scheme which encourages inter-practice referrals and surgeries to deliver the service to patients from other surgeries. This increases availability and accessibility for women.
6.4 Pharmacy sexual health services
6.4.1 Overview
In Surrey, community pharmacies are an important part of the local sexual health delivery model, offering a convenient and accessible route for sexual health services. Delivering these services in community pharmacies improves access for residents in areas further away from the specialist sexual health hub or spoke clinics. The pharmacy supports and advises patients on avoiding pregnancy and STIs through safer sex and condom use, regular contraceptive methods, and refers them to services for LARC and full STI screening and treatment. This enables patients to address immediate sexual health needs in one location.
Surrey County Council Public Health encourage community pharmacies to offer sexual health services and there is a focus on pharmacies in the 21 key neighbourhoods. The services available to deliver include:
- Emergency contraception
- Chlamydia and gonorrhoea testing and treatment
- Condom Distribution Scheme known as the C-card
Pharmacies must be fully trained and should display posters promoting services and display the Sexual Wellbeing Surrey window sticker.
6.4.2 STI testing and treatment
Chlamydia and gonorrhoea testing is available for under 25-year-olds at pharmacies that have signed up to deliver these services. They also signpost to the specialist sexual health clinics and the online full STI screening service. In addition, many pharmacies display the screening kits on their counters to enable patients to opportunistically pick up when visiting.
The chlamydia screening kits are offered to under 25-year-olds, both males and females, but the promotional materials that are displayed target females which is in line with national guidance from UKSHA. Pharmacies provide support and advice to patients, including advice on safer sex, condom use and advice on the use of regular contraceptive methods, when required.
Chlamydia and gonorrhoea treatment is available for under 25-year-olds at pharmacies that have signed up to deliver this service. Pharmacists can dispense antibiotic treatment without the need for a prescription. When a young person receives notification of a positive chlamydia test from the specialist sexual health service outreach team, they will be signposted to the nearest pharmacy offering the service.
Community services are an effective and essential part of the chlamydia treatment pathway in Surrey. Their ability to offer free, confidential, and accessible care contributes to early detection and treatment, ultimately reducing the prevalence of chlamydia and promoting better sexual health outcomes for young people.
6.4.3 Contraception services
Emergency Contraception (EC) is available for under 25-year-olds at pharmacies that have signed up to deliver these services. Pharmacists can dispense EC free of charge for the patient and can sell emergency contraception to individuals aged over 25 years. Following the provision of emergency contraception, patients are offered free condoms and chlamydia and gonorrhoea testing kits, provided by the specialist sexual health service for distribution in the pharmacy. They are also encouraged to sign up to the C-card scheme (for under 25s).
In addition, some community pharmacies offer the NHS contraceptive pill service. This service is commissioned by NHS England. Through this service, individuals can obtain the contraceptive pill (progesterone only pill and combined oral contraceptive pill) without the need for a GP appointment, making it easier for those seeking contraception to access it in a convenient, private, and non-judgmental setting. This initiative improves access to contraception and supports public health efforts to prevent unintended pregnancies.
Access to free emergency contraception will be made available to all women from Pharmacies later in 2025, as part of a national change to reduce inequalities in access in deprived areas and free up GP appointments.
6.5 Secondary care
6.5.1 STI testing and treatment
STI testing and treatment has very recently been introduced to secondary care, with a focus on using A&E attendances as an opportunity to test for HIV. As part of the HIV action plan for England, NHSE are funding implementation of Emergency Department opt out testing for Blood Born Virus (BBV) e.g. HIV, hepatitis B and C. Implementation in other areas of England has proved very effective in identifying thousands of undiagnosed BBV and supporting previously diagnosed people to reengage with care. In 2024, the Government announced expansion of the programme which will now include Ashford St Peters Hospital (ASPH) and East Surrey Hospital, will roll out planned later in 2025/26. Epsom Hospital have been testing for HIV in ED since 2022, as part of the first wave roll out which included Epsom and St Helier University Hospital NHS Trust.
Opt-out point of care BBV testing was introduced at Frimley Park Hospital A&E in early 2025. All clinicians are encouraged to ‘Think HIV’ when treating individuals, to increase awareness for HIV testing, and to overcome assumptions and stereotypes that might mean an individual may experience a missed opportunity to be tested for HIV due to their demographic characteristics, including age, ethnicity and sexuality.
The roll out of the scheme to Frimley Hospital, ASPH and East Surrey Hospital provides a great opportunity to expand HIV testing opportunities and raise awareness of HIV to the wider system.
6.5.2 Screening in pregnancy
All pregnant women and birthing people are offered screening for blood borne viruses (BBV) during pregnancy as part of the Infectious Diseases in Pregnancy Screening Programme. Individuals are offered testing for hepatitis B, HIV and syphilis. The aim of this programme is to provide an opportunity for diagnosis and subsequent optimisation of care for pregnant individuals infected with blood borne viruses, reduce the risk of vertical transmission to the unborn child, and ensure early diagnosis and treatment for children at risk of vertical transmission. The coverage of HIV screening during pregnancy is 99.8% in England. Women giving birth in the UK who did not receive antenatal care in the UK may not have been offered this screening and may be at higher risk of undiagnosed blood borne viruses.
6.5.3 Contraception services
For routine contraception needs, women are unlikely to use secondary care services. However, contraception advice and provision may be offered in secondary care services, largely Obstetrics and Gynaecology, for management of complex cases, contraception-related health conditions and following a birth (see below section on postnatal care).
6.6 Abortion services
Abortion services will often include provision of advice and options for contraception to reduce unplanned pregnancies and lower repeat abortion rates. NICE Quality Statements propose that contraception should be discussed with women requesting an abortion and women should be offered a choice of contraception method before discharge [143].
6.7 Preconception health
Women’s health prior to conception (pre-conception), at conception and during pregnancy will impact on their health as well as the health of their child [144, 145, 146]. The importance of discussing advice around modifiable factors which could affect pregnancy health is recognised. These factors include improving nutrition and diet, maintaining a healthy weight, reducing alcohol consumption and reducing smoking. Whilst this falls outside of the direct scope of this JSNA chapter, contraception counselling and advice services may well provide an opportunity for healthcare professionals to start these discussions.
6.8 Postnatal care
Women who have recently given birth have a higher risk of pregnancy which may be unintended and can lead to health risks for both the woman and child if conceiving within 18 months of birth [147]. NICE Quality Statements on contraception after childbirth [148] recommend that women who give birth are provided with information on contraception and, if required, a choice of method of contraception. The Faculty of Sexual and Reproductive Healthcare recommend that provision of advice and contraception methods should be offered by all clinicians involved in the care of pregnant women [149]. This may include staff in hospital at discharge following birth, or at postnatal check-up appointments.
There is an ambition in Surrey to explore postnatal contraception delivery within maternity services. This has been included as a focus area as part of the Women’s Health agenda being led jointly by Surrey Heartlands ICS and Public Health.
6.9 Condom distribution scheme
The C-Card is a free and confidential CDS for young people aged 13–24 years old in Surrey. The aim of the scheme is to provide free condoms, lubricant, sexual health information and signposting in places young people already access. The CNWL Outreach Team work deliver free C-Card training to upskill professionals working with young people to feel confident to discuss sexual health with them, carry out condom demonstrations and distribute condoms. In addition to this, they are also trained in how to support young people to complete chlamydia screening tests. The CNWL outreach team provide the resources and any additional support that is needed to enable an organisation to offer the Scheme.
The Scheme provides regular, easy and confidential access to free condoms and chlamydia kits at a number of outlets across Surrey. The CDS is delivered by various providers across all Surrey boroughs, including: in general practice; pharmacies; sexual health services; youth, third sector and voluntary services; education settings; children and young people’s services; supported housing providers, and drug and alcohol services. The aim of the scheme is to provide contraceptive & sexual health information and signposting to sexual health services in places young people already access.
If a young person is 16-24 years old, they can register online, all they need to do is fill out their details and an Outreach Team member will email them with a virtual C-Card which will allow them to pick up free condoms at any participating outlet across Surrey. If they choose to, they can receive first supply of condoms in the post.
Under 16 year olds can still register for C-Card by visiting nearest outlet that provides the registration service and get signed up with a trained professional. Once registered, they can receive a C-Card that gives them regular, easy access to free condoms at any outlet displaying the Surrey Sexual Wellbeing logo.
The list of outlets can be found on the Healthy Surrey website [150].
6.10 Relationships and sex education (RSE) in schools
6.10.1 Overview
RSE should form an integral part of Personal, Social Health and Economic (PSHE) Education and be embedded as a whole school approach. In September 2020, relationships education in primary schools, RSE in secondary schools, and health education in both primary and secondary schools became a statutory requirement. This includes academies, free schools, faith schools and the independent sector. Statutory guidance on this was published in 2019 and was updated in 2025. RSE is crucial for students’ wellbeing development because it focuses on promoting healthy relationships, self-esteem, and informed decision-making as well as covering STIs, contraception and access to services.
6.10.2 Surrey’s Healthy Schools Approach
The Surrey Healthy Schools whole system approach is a aimed at promoting the wellbeing, health, inclusion, and achievement of children and young people in Surrey. This holistic way of working brings together evidence based services and partners to support schools in enhancing their curriculum and implementing best practice. Key areas of focus include: emotional; mental, and physical health; reducing inequalities; increasing social inclusion and raising academic achievement. The initiative provides resources, training, and a self-evaluation tool to help schools reflect on their practices and access support from local and national services.
The specialist sexual health provider, CNWL, deliver RSE training for school staff that was developed in partnership with the Surrey Healthy School’s approach. This training aims to support school staff so that they feel confident to deliver effective RSE. Surrey PSHE Education Guidance on Relationships and Sex Education was updated in 2025, developed by the Surrey Healthy Schools Lead, it offers a comprehensive array of resources to support the delivery of RSE sessions. Maintaining effective RSE in Surrey schools is a key action in the Teenage Pregnancy Prevention Action plan.
6.11 Sexual assault referral centres
The Solace Centre is the sexual assault referral centre (SARC) in Surrey [151]. Their service is for anyone, of any age, who has experienced sexual assault, including rape. They have a 24/7 helpline that individuals who have experienced sexual assault can use to access support, as well as to discuss options for accessing the range of services they offer. These include immediate advice, support and signposting, crisis support, forensic examinations, and referral to independent sexual violence advisors. They also provide support and advice for individuals who have non-recent experiences of sexual assault in their life.
6.12 Other services
Extending sexual health testing to the community can help to take services to groups that may not usually access sexual health services and help to break down stigma. Many voluntary, community and social enterprise organisations, such as youth groups, include promotion of sexual wellbeing as part of their work, as well as providing additional support, for example the CDS.
The Public Health sexual health team and sexual health service have recently undertaken a pilot project taking HIV point of care testing into community settings. Testing was piloted by community providers and aimed to provide opportunities for individuals already accessing a service to receive an HIV test, removing the barriers to accessing traditional healthcare and sexual health services that may exist for these individuals. The pilot has shown a low uptake in testing and is currently being reviewed for further development.
7 Sexual health service use in Surrey
7.1 Headline findings and key implications
- Data on consultations at specialist sexual health service use by age, ethnicity, and sexual orientation is broadly in line with what would be expected given differences in service needs among young people, certain ethnic groups, and GBMSM.
- Recent years have seen a shift to increasing availability of a range of sexual health services online, including STI testing and accessing contraception.
- STI testing and diagnosis patterns in Surrey show disparities by ethnicity, deprivation, sexual orientation, and age, with disproportionately higher diagnosis rates among some ethnically diverse groups, more deprived areas, among LGBTQ+ individuals, and in the 18–24 age group.
- The number of face-to-face consultations for contraception in Surrey are highest among 18–34-year-olds and people of white ethnicity which is what would be expected. The contraception attendance rates among Black and mixed ethnic groups were slightly higher relative to the population in Surrey, but lower in those of Asian ethnicity.
- As expected, online contraception consultations in Surrey have dropped since the COVID pandemic, although online services remain important, particularly among 18-24-year-olds where there’s been a steady increase in the number of consultations over time.
- The majority of online contraception consultations were for the progesterone-only pill. However, use among 25-34 year olds has declined which could be due to changes in how this age-group access contraception, or changes in contraception preferences.
- Among Surrey residents who chose to use out-of-area providers, this appeared to be largely influenced by geographical proximity with boroughs that are closer to the borders of Surrey having a higher proportion of residents using out-of-area services.
- Pharmacies in Surrey provided chlamydia screening (provided by 28 of 99 accredited pharmacies in 2024) and emergency contraception (provided by 46 pharmacies in 2024). The number of people accessing both services has remained relatively stable over the past five years.
- In 2024, Surrey’s Condom Distribution Scheme (CDS) saw rising engagement, with 223 users and over 1,000 condoms distributed in Quarter 1. Some barriers to accessing condoms remain including embarrassment, lack of information and confidentiality concerns.
- In 2023, Surrey had total rates of prescribed LARC higher than the national average at 56.2 per 1,000 women aged 15–44. This varied widely across districts and boroughs. The proportion of LARC prescribed at GPs has remained relatively stable over time at just over 75%.
- The rate of women prescribed short acting combined hormonal contraception in both sexual health services and GPs has been reducing in Surrey and nationally.
7.2 Specialist sexual health services
7.2.1 Clinics
7.2.1.1 Total consultations
Excluding online consultations, in the calendar year 2023, there were a total of 13,860 consultations at sexual health clinics in Surrey, including for STI-related care, and contraception [unpublished data from specialist sexual health service provider]. The vast majority of these consultations were delivered face to face (89.9% of activity), followed by telephone (9.7% of activity), with the remainder of clinic consultations delivered by ‘other’ methods.
7.2.1.2 Service use by borough
Of all the clinic services delivered, 87.6% of consultations were for Surrey residents, and 12.4% were for individuals who were not Surrey residents. Overall, the rate of Surrey residents accessing a sexual health clinic was 988 per 100,000 residents (Figure 7.1) (152). This ranged from 207 per 100,000 for residents in Epsom and Ewell, to 2,021 per 100,000 for residents of Guildford. Higher service use in Guildford and Woking is likely due to the presence of sexual health clinics in these boroughs, and Guildford has a high proportion of residents in the 20-24 years age group (152), which may be, in part, due to the presence of a university. The lower rates in other boroughs may be explained by lower sexual health needs, as well as residents accessing non-Surrey specialist sexual health clinics that are geographically closer to their homes, despite being in a different county.
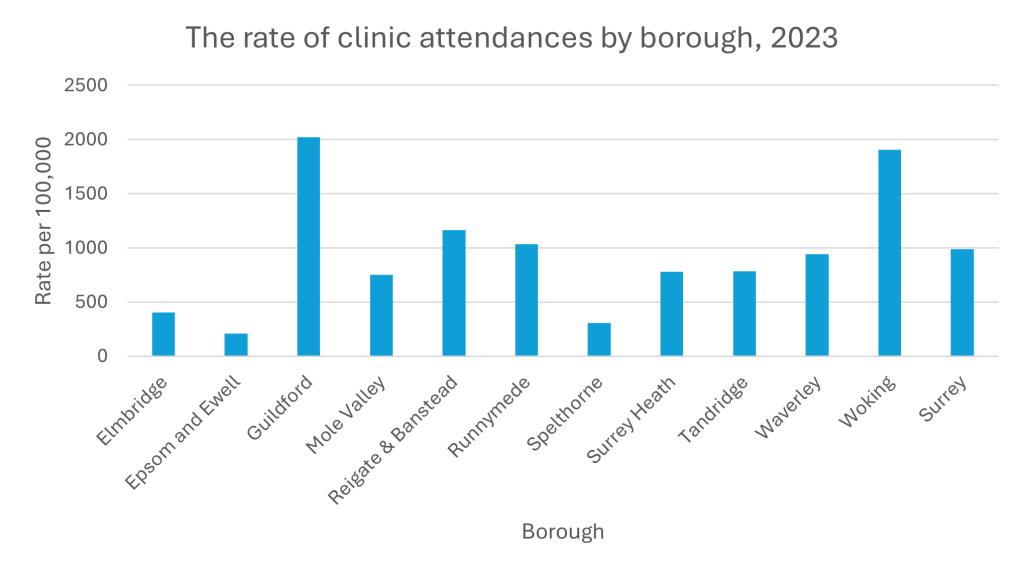
7.2.1.3 Service use by sex and age
The following data refers to all individuals accessing specialist sexual health services in Surrey, including use by non-Surrey residents. Of the 13,860 consultations, 6,120 were for males (44.2%) and 7,740 were for females (55.8%). Females therefore account for a higher proportion of attendees at sexual health clinics compared to what would be expected if usage mirrored the Surrey population in terms of sex distribution, as they only account for 51.3% of the population of Surrey (152).
The sexual health service collect data for people that identify as transgender and non-binary. Numbers for these groups are small and therefore are not published.
The age groups accounting for the highest proportion of clinic attendances were 18- to 25-year-olds (n=4,255, 30.7%), followed by 26- to 35-year-olds (4,230, 30.5%) and 36- to 45-year-olds (n=2,470, 17.8%) (Figure 7.2). These age groups account for a higher proportion of attendances at sexual health clinics compared to what would be expected if use mirrored the age structure of the Surrey population; individuals aged 18 to 45 account for a total of 79.0% of clinic attenders, whilst the Surrey population of individuals aged 15 to 44 years (a slightly different age range than described above due to inconsistent age categories between data sets) only accounts for 36.2% of the total population of Surrey (152). Over-representation of young people at sexual health clinics is consistent with the national picture [153], and is to be expected, as younger individuals often have higher sexual health need due to their sexual behaviours. However, national data indicates that whilst rates of all new STIs have fallen for men aged 13 to 34 years between 2019 and 2023, rates have risen slightly in men aged 35 years and over, therefore this may indicate rising sexual health need in this group [154].
The age structure by sex indicates higher activity in the older age groups in males compared with females. Nationally, in 2023, women outnumbered men for attendances at specialist sexual health services up to and including the 35-44-year-old age bracket, and men outnumbered women in the 45-64 and 65 years and over age groups [154]. Therefore, in Surrey, a male predominance in attendances occurs at a lower age compared with nationally. Females likely account for a higher proportion of attendances at sexual health clinics in the younger age categories, in part, due to contraceptive needs.
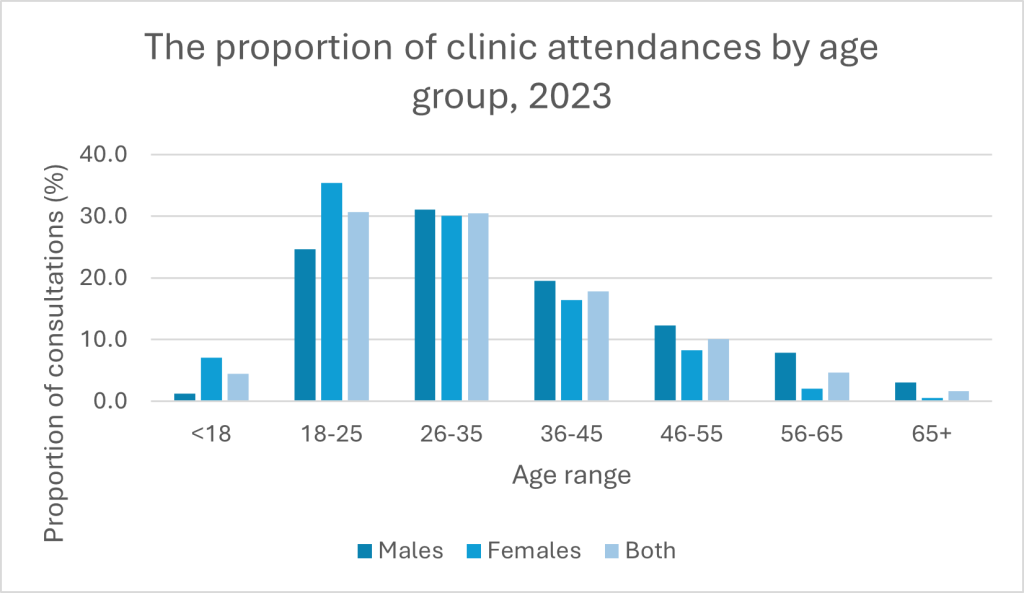
7.2.1.4 Service use by ethnicity
Of the 13,860 clinic attendances in 2023, 1,050 (7.6%) did not have an ethnic group stated. Of those with a recorded ethnic group, the majority of these were for individuals from a White British ethnic background (n=9,095, 71.0% of attendances). The number of consultations for individuals from each ethnic group are shown in Table 7.1, as well as the proportion of all attendances that are accounted for by individuals from each ethnic group. The proportion of total consultations that were for individuals from each ethnic group was compared to the Surrey population (23). A limitation of this is that a minority of these consultations (12.4%) were not for Surrey residents, however this provides an interesting opportunity for comparison.
Compared to what would be expected if the attendances at sexual health clinics was proportional to the ethnic profile of Surrey, there was a higher proportion of total consultations for individuals from Other White (9.6% vs 7.7%), Black Caribbean (1.1 vs 0.4%), Black African (3.9 vs 1.1%), Other Black (0.5% vs 0.2%), White and Black Caribbean (1.1% vs 0.6), White and Black African (1.0% vs 0.4%), and Other Mixed (1.8% vs 1.0%) ethnic groups. There were a lower proportion of total consultations for individuals from White British (71.0% vs 76.6%), White Irish (0.8% vs 1.2%), Indian (1.7% vs 2.9%) and Bangladeshi (0.2% vs 0.4%) ethnic groups. This aligns with national data which suggest that attendance at sexual health clinics within the past 5 years was highest in Black Caribbean, Black African, White other and mixed ethnicity groups, and lowest in Indian and Pakistani ethnic groups [155].
| Ethnicity | Number of consultations | Proportion of total consultations (%) | Proportion of Surrey residents in each group (%) |
| White British | 9095 | 71.0 | 76.6 |
| White Irish | 105 | 0.8 | 1.2 |
| Other White | 1230 | 9.6 | 7.7 |
| Black Caribbean | 145 | 1.1 | 0.4 |
| Black African | 505 | 3.9 | 1.1 |
| Other Black | 70 | 0.5 | 0.2 |
| Indian | 220 | 1.7 | 2.9 |
| Pakistani | 180 | 1.4 | 1.5 |
| Chinese | 120 | 0.9 | 0.9 |
| Bangladeshi | 25 | 0.2 | 0.4 |
| Other Asian | 255 | 2.0 | 2.0 |
| White and Black Caribbean | 140 | 1.1 | 0.6 |
| White and Black African | 125 | 1.0 | 0.4 |
| White and Asian | 185 | 1.4 | 1.3 |
| Other Mixed | 225 | 1.8 | 1.0 |
| Other | 185 | 1.4 | 1.6 |
7.2.1.5 Service use by sexual orientation
The majority of clinic attendees in 2023 identified as heterosexual (n=10,335, 74.6%), followed by gay (n=2,140, 15.4%), individuals identifying as having another sexual orientation (n=745, 5.4%) and bisexual (n=640, 4.6%) (Figure 7.3). There were differences in the proportion of individuals who reported each sexual orientation by sex, with a higher proportion of clinic attendances for heterosexual females, and a higher proportion of clinic attendances for gay men (Figure 7.3).
In Surrey, 90.7% of individuals aged 16 years and over identify as straight or heterosexual, 1.2% as gay or lesbian, 1.1% as bisexual, and 0.3% identified themselves as another sexual orientation (21), therefore, compared to what would be expected if attendances mirrored the Surrey population in terms of the proportion of individuals with each sexual orientation, there is higher use by individuals who are gay, bisexual or identify as having another sexual orientation, compared with heterosexual individuals.
These findings are broadly in keeping with what would be expected based on the national data available, (although note that Surrey data uses sex and national data, gender, which means results are not fully comparable), with the vast majority of women attending specialist sexual health services in England identifying as being women who have sex with men and a more even split between men attending services identify as GBMSM and men who have sex with women [154].
The high proportion of female clinic attendees who identify as heterosexual or straight may be due to higher need for hormonal contraception and LARC for these individuals.
The significant over-representation of male clinic attendees identifying as gay may be due to higher rates of STIs in GBMSM, as well as due to accessing services such as PrEP.
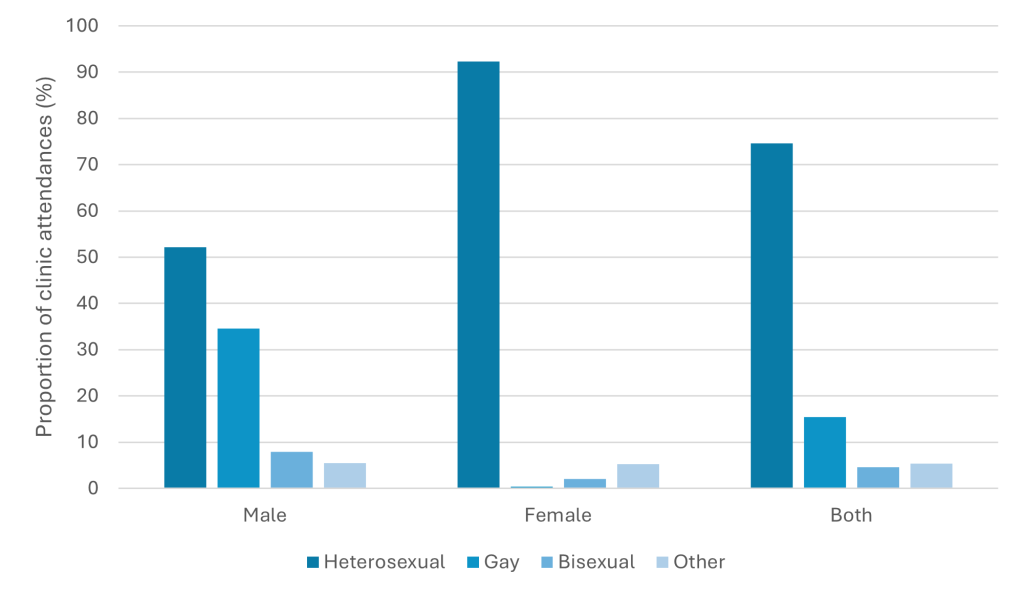
7.2.2 Online services
Recent years have seen a shift to increasing availability of a range of sexual health services available online, including STI testing and accessing contraception. This shift was accelerated by the COVID pandemic, during which in-person health services were limited to prevent the transmission of the virus, and services sought innovative ways to provide care remotely [156].
CNWL’s online services in Surrey are exclusively available to Surrey residents; therefore, the data presented pertains to individuals residing in Surrey, unlike the data for clinic service use [unpublished data from specialist sexual health service provider].
A total of 21,270 online tests were sent to residents in the calendar year of 2023. Of these, 16,130 tests were completed and returned to the service for testing. The rate of online test kits requested and sent to residents was 1,731 per 100,000 in Surrey, and the rate of online test kits completed and returned for testing was 1,313 per 100,000 (Figure 7.4). The highest rate of residents requesting test kits online was for Guildford residents (2,554 per 100,000 residents), and the lowest was for Spelthorne (1,275 per 100,000 residents).
Guildford and Spelthorne also had the highest and lowest rates, respectively, of returned online tests kits, which is expected given requesting a kit is a pre-requisite to returning it (Figure 7.4). Higher service use in Guildford is likely due to the high proportion of residents in the 20-24 years age group (152), which may be, in part, due to the presence of a university. Furthermore, the clinics do give out online test kits in reception, therefore Guildford residents may be more likely to collect a test kit in the Guildford clinic. However, it is of interest that rates of requesting online tests are lowest in Spelthorne, considering the locality of Surrey sexual health clinics, therefore online tests may provide a convenient opportunity for testing. It may be that individuals in Spelthorne are more likely to use out of area in person services (Section 7.2.5) and therefore have less familiarity with the range of services available in Surrey, including online testing.
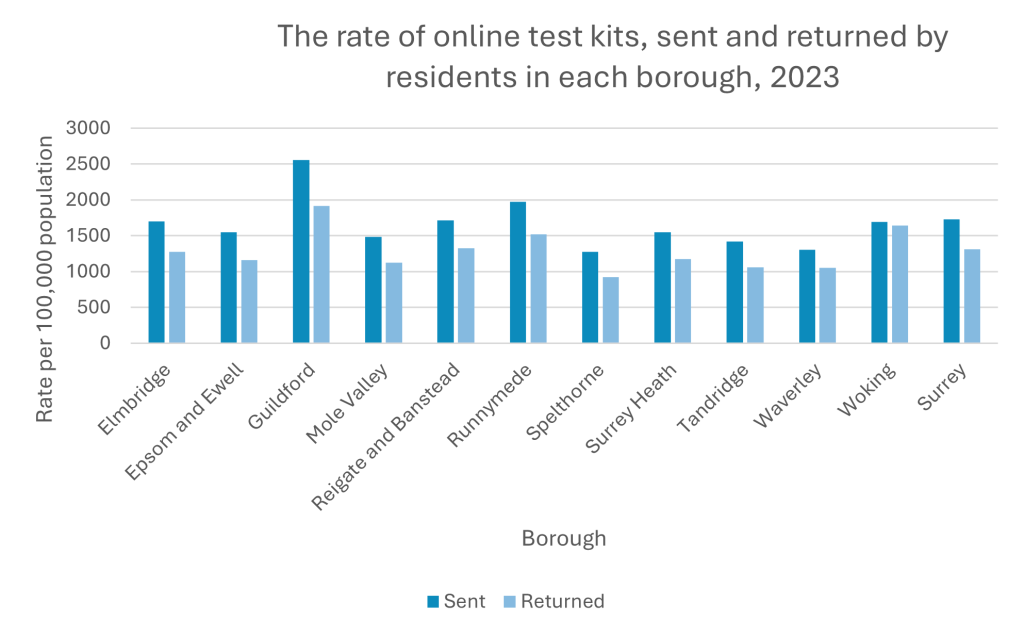
Across Surrey, the return rate for tests requested online was 75.8% in 2023. The return rate varied across the Surrey district and boroughs, from 72.3% in Spelthorne, to 97.2% in Woking (Figure 7.5).
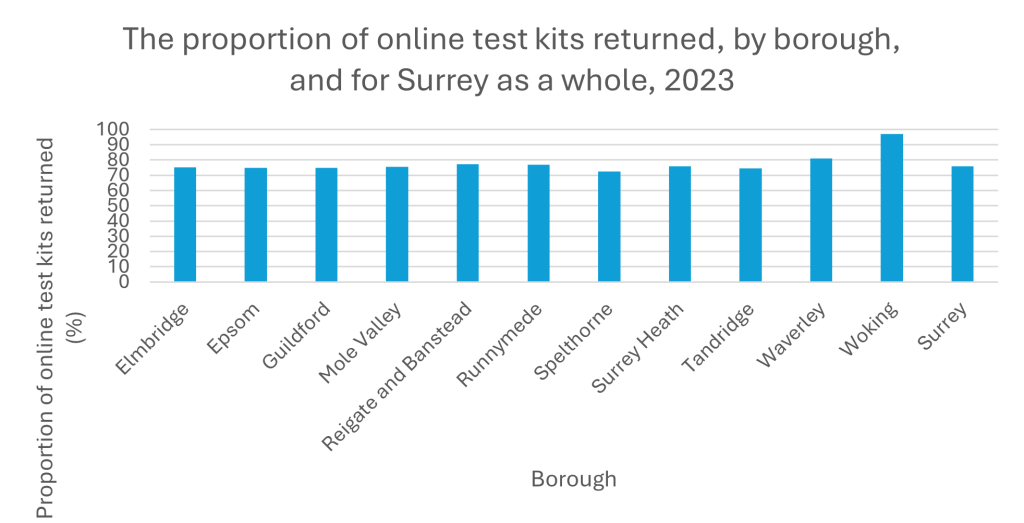
7.2.3 STI testing and diagnosis
Are Surrey residents using services at the level we would expect? Are we testing the right people?
Links to the STI dashboard will be made live shortly.
Chlamydia Testing and diagnosis:
According to Surrey sexual health service data from 2023:
- The lowest numbers of tests were undertaken in Epsom and Ewell and Spelthorne. These are areas where we typically see higher out of area usage. The highest rates of diagnosis were seen in Guildford (118.3 per 100,000 population) and Woking (81.8 per 100,000 population).
- Whilst more chlamydia is diagnosed amongst people of white ethnicities, some ethnically diverse groups have disproportionate higher diagnosis rates. People of black ethnicity had the highest rates of chlamydia diagnosis of all aggregated ethnic groups (Asian, Black, Mixed, Other, or White).
- Data shows that whilst the highest number of chlamydia tests are undertaken by those living in the least deprived areas, rates are higher in those living in higher areas of deprivation (IMD decile 2). The same pattern is seen when looking at chlamydia diagnosis.
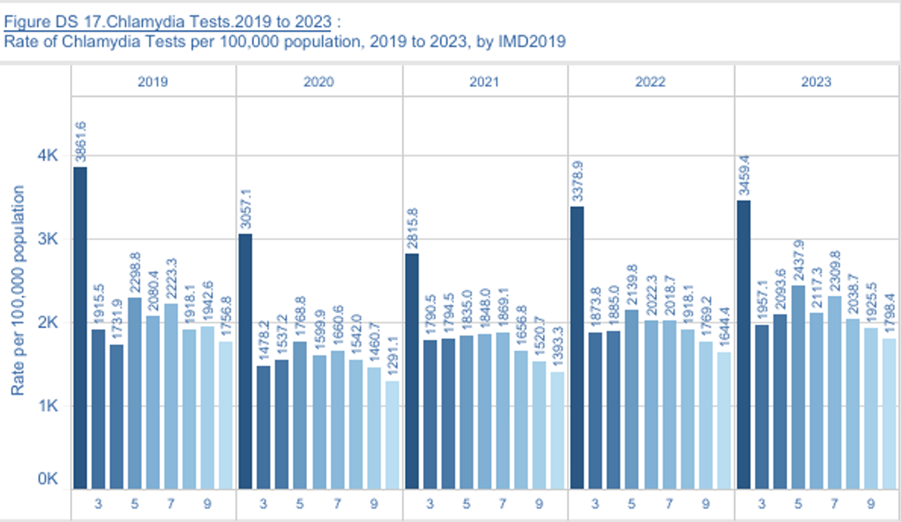
- The highest number of chlamydia tests was recorded among females aged 25–34, whereas the highest testing rate was observed among females aged 18–24. This is to be expected as it reflects the target population of the chlamydia screening programme. The same pattern is reflected when looking at chlamydia diagnosis.
- The highest number of chlamydia tests were done by those identifying as heterosexual (13,710) (rate of 1555.0 per 100,000 population). The highest rates (21,400.3 per 100,000) of testing are seen in those identifying as LGBTQ+. Sexual orientation rates should be interpreted with caution because 7% of respondent’s sexual orientation is unknown in the 2021 census used to calculate these rates.
Gonorrhoea Testing and diagnosis:
According to Surrey sexual health service data from 2023:
- The highest number of gonorrhoea tests were undertaken in Guildford, followed by Reigate and Banstead and Woking. The highest rates of testing were undertaken in Guilford (3,379.7 per 100,000 population) and Woking (2,977.5 per 100,000 population).
- When looking at diagnosis by ethnicity, a similar picture is seen for gonorrhoea to chlamydia. More gonorrhoea diagnoses were seen amongst people from white ethnicities (440), but the highest rates are seen amongst people of black ethnicity (96.0 per 100,000 population) closely followed by people of mixed ethnicity (86.5 per 100,000 population).
- Data shows that whilst the highest number of gonorrhoea tests are undertaken by those living in the least deprived areas, rates are higher in those living in higher areas of deprivation (IMD decile 2).
- The highest numbers of gonorrhoea tests (5,235) were undertaken by females aged 25-34. For men, the same age category undertook the highest number of tests (3,415). However, the highest rates of gonorrhoea tests were undertaken by females aged 18-24 (11,300.4 per 100,000 population). The same pattern is reflected when looking at gonorrhoea diagnosis.
- The highest number of gonorrhoea diagnosis were seen in those identifying as heterosexual (265) (rate of 30.1 per 100,000 population). The highest rates of diagnosis are seen in those identifying as LGBTQ+ (1,893.4 per 100,000 population). Sexual orientation rates should be interpreted with caution because 7% of respondent’s sexual orientation is unknown in the 2021 census used to calculate these rates.
Syphilis testing and diagnosis:
Numbers of syphilis diagnosis are too small to report and discuss by demographic groups.
According to Surrey sexual health service data from 2023:
- The highest number of syphilis test were undertaken in Guildford (4,465). The highest rate of syphilis testing was undertaken in Guildford (3,108.2 per 100,000 population), and Woking (2,751.2 per 100,000 population).
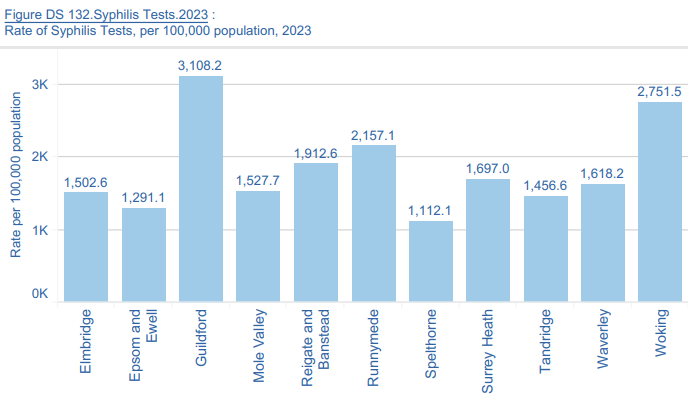
- When looking at ethnicity, in 2023, the highest numbers of syphilis tests were seen amongst people of white ethnicities (16,305). However, rates show the highest numbers of syphilis tests were seen amongst people of black ethnicities (5,303.6 per 100,000 population).
- The highest number of syphilis tests (6,645) were undertaken by people living in the least deprived IMD decile. Rates of syphilis tests are higher in those living in more deprived areas (IMD decile 2) (3,137.6 per 100,000 population).
- The highest numbers of syphilis tests were undertaken by males and females aged 25 – 34 (male 3,300 and females 4,890 tests). Rates are higher in females aged 18-24 years (10,357.8 per 100,000 population) with male rates being highest in ages 25 – 24 years (5,0006.8 per 100,000 population), closely followed by males aged 18-24 years (4,914.2 per 100,000 population).
HIV testing and diagnosis
Numbers of HIV diagnosis are too small to report and discuss by demographic groups.
According to Surrey sexual health service data from 2023:
- The highest rate of HIV tests were undertaken in Guildford (3,038.6 per 100,000 population) and Woking (2,645.6 per 100,000 population). The lowest rates of HIV testing was in Spelthorne (1,102.4 per 100,000 population).
- Although numbers of HIV testing were highest in those of white backgrounds, rates of HIV testing were higher in those of black ethnicities (4,799.6 per 100,000 population). Rates have been increasing since 2020.
- The highest number of HIV tests were undertaken by people living in the least deprived IMD decile (6,555). Rates of HIV tests in 2023 are highest in those living in more deprived areas (IMD decile 2) (3,057.1 per 100,000 population).
- The highest rates of HIV testing were seen in females aged 18-24 years (10,289.6 per 100,000 population). In males, rates are lower with very similar rates for both 18-24 years (4,903.3 per 100,000 population) and 25-34 years (4,923.4).
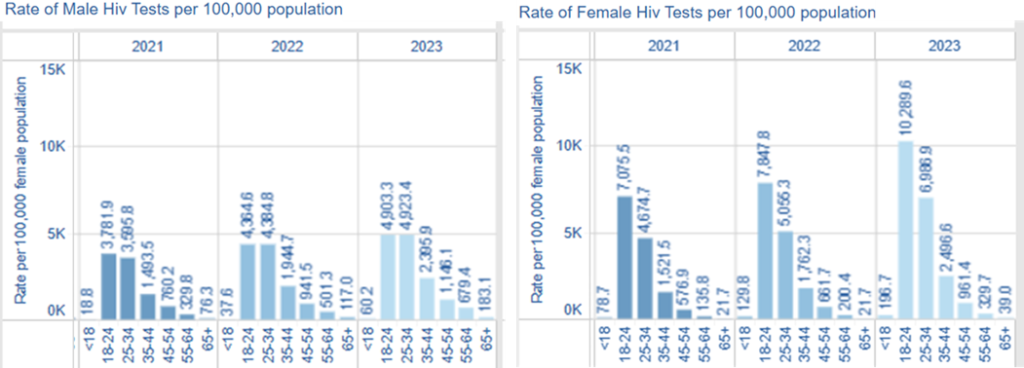
In person and online STI testing comparison:
The 2023 Surrey sexual health service data was used to compare rates of face to face and online STI testing, whilst also looking at demographics of service users.
Data shows chlamydia and gonorrhoea testing rates are higher for online testing compared to face to face testing in people living in the most deprived IMD decile (IMD decline 2) (1,930.8 per 100,000 population compared to 1,528.6).
Data also shows that when looking at testing rates by ethnicity, online syphilis testing rates are higher compared to face to face testing rates. For example, people of black ethnicity had higher online syphilis testing rates (3,095.8 per 100,000 population), compared to face to face testing rates (2,207 per 100,000 population).
These findings may indicate a preference for online testing among certain populations, such as individuals living in more deprived areas or those from ethnically diverse backgrounds. This is a positive development, as these groups often have greater sexual health needs. It may also highlight potential barriers to accessing in-person services. However, since online testing for asymptomatic individuals is encouraged, this trend could reflect an appropriate and effective use of available services.
PrEP
Pre-exposure prophylaxis (PrEP) is a drug taken by HIV-negative individuals before they have sex to stop them acquiring HIV. As part of a combination approach to HIV prevention, specialist sexual health services are responsible for the delivery of PrEP to those at higher risk of acquiring HIV.
In Surrey, rates of sexual health service attendees who were eligible for HIV PrEP have been increasing since 2020.
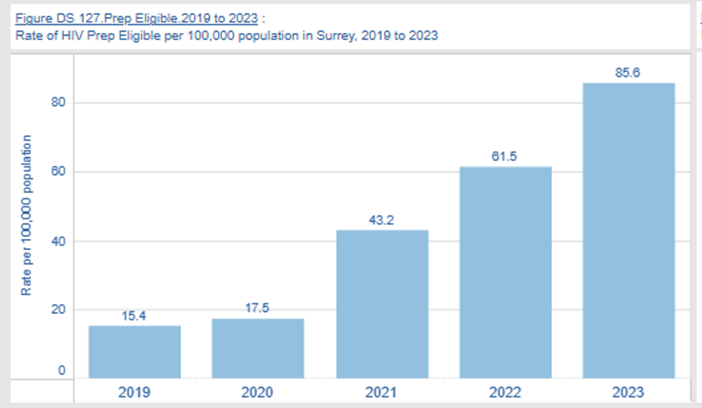
Since 2020, the proportion of individuals attending sexual health services who have initiated or continued PrEP has steadily increased. These rates closely align with those of the eligible population, suggesting that PrEP is reaching those who are most likely to benefit from it.
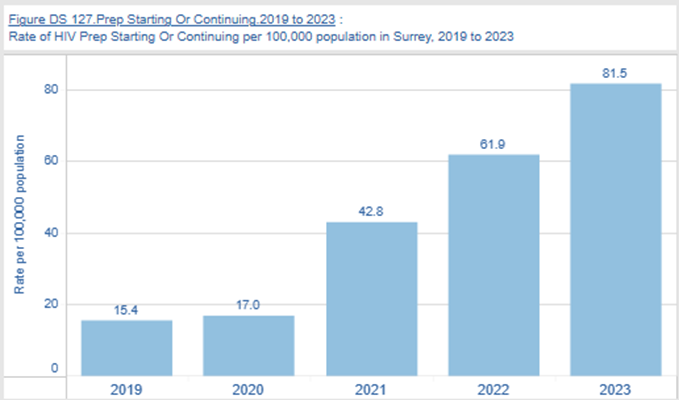
In 2023, those in the 25 to 34 years age group had the highest rate of starting or continuing PrEP (202.9 per 100,000 population). Rates were also highest in those identifying as LGBTQ+ (70,001.3 per 100,000 population).
Rates for those starting or continuing PrEP in 2023 were highest amongst people from other ethnic backgrounds (197.6 per 100,000 population), followed by those from mixed backgrounds (135.9 per 100,000 population).
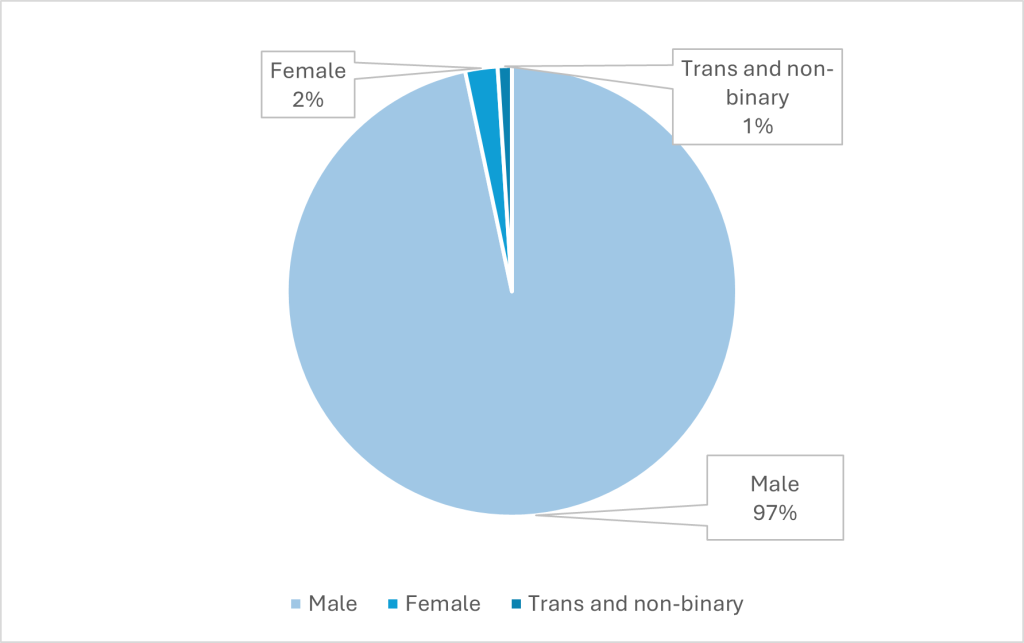
Clinic attendances by gender show 97% of attendances (1334) were by males. While PrEP uptake has grown significantly among men, particularly men who have sex with men, there remains a critical gap in access and usage among women and transgender individuals. This disparity persists despite evidence that these groups face elevated HIV risk and could benefit substantially from PrEP.
7.2.4 Contraception services
7.2.4.1 Sexual health clinic consultations
The number of face-to-face consultations specifically relating to contraception care in sexual health clinics in Surrey was 9,780 in 2019. Since 2020, this number has been lower and remained between 3,525 and 4,805 consultations per year (Figure 7.12).
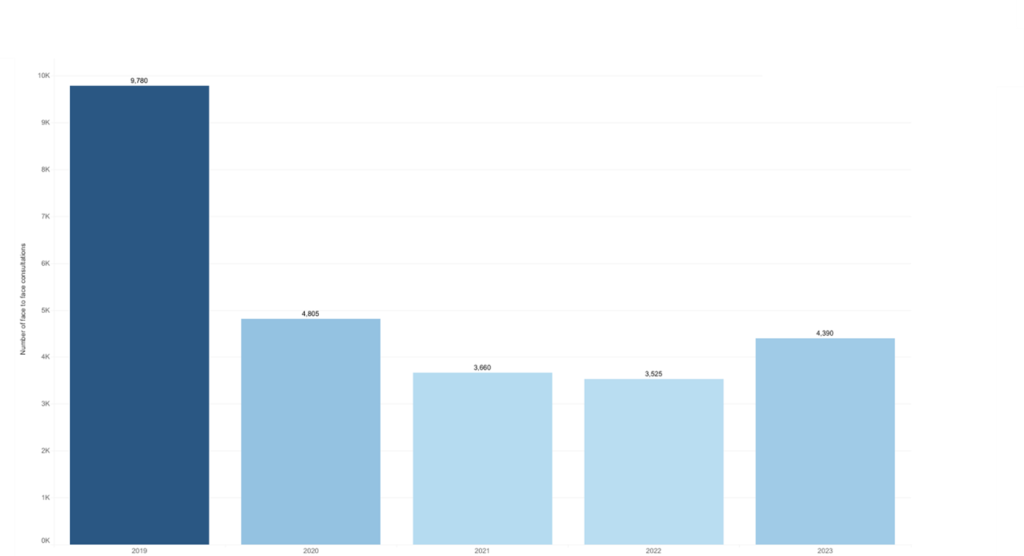
The highest number of consultations were among 18-24 year olds and 25-34 year olds (Figure 7.13). The number of consultations declined between 2019 and 2020 in all ages although this was most notable among these youngest age-groups.
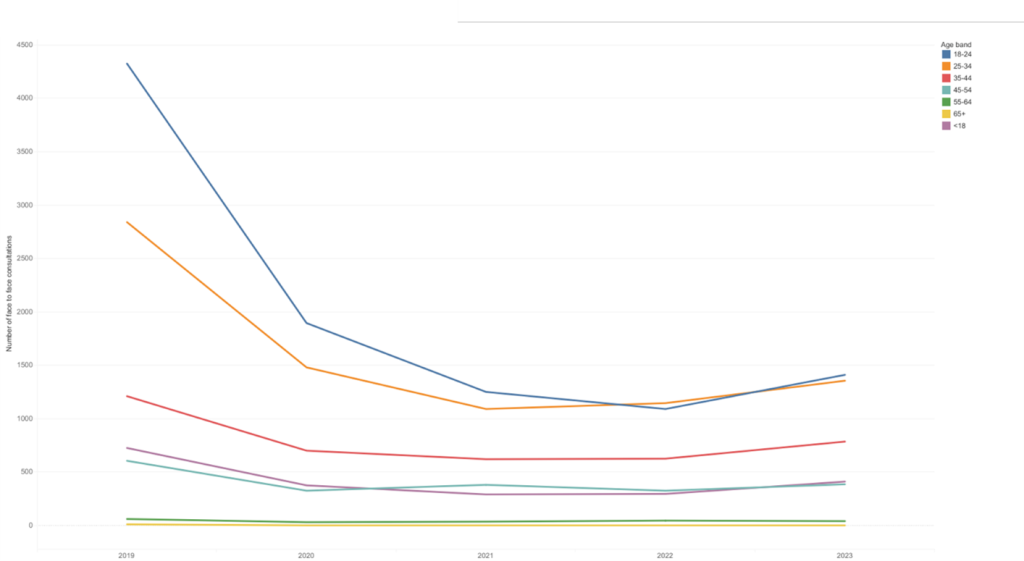
In 2023, just over 6% of face-to-face sexual health clinic consultations for contraception did not have an ethnicity recorded. For those with a known ethnicity, data were grouped into ethnic groups white, black, mixed, Asian and other due to small numbers in some ethnic groups. The majority of face-to-face attendances in Surrey were by people of white ethnicity (83.5%), followed by black ethnicity (5.0%), mixed ethnicity (5.0%), and Asian ethnicity (4.1%) (Figure 7.14). If the attendances at sexual health clinics were proportional to the ethnic profile of Surrey then this suggests that the rate of attendance is slightly higher in those of black ethnicity and mixed ethnicity but lower in those of Asian ethnicity, which is similar to data presented in Section 7.2.1.4).
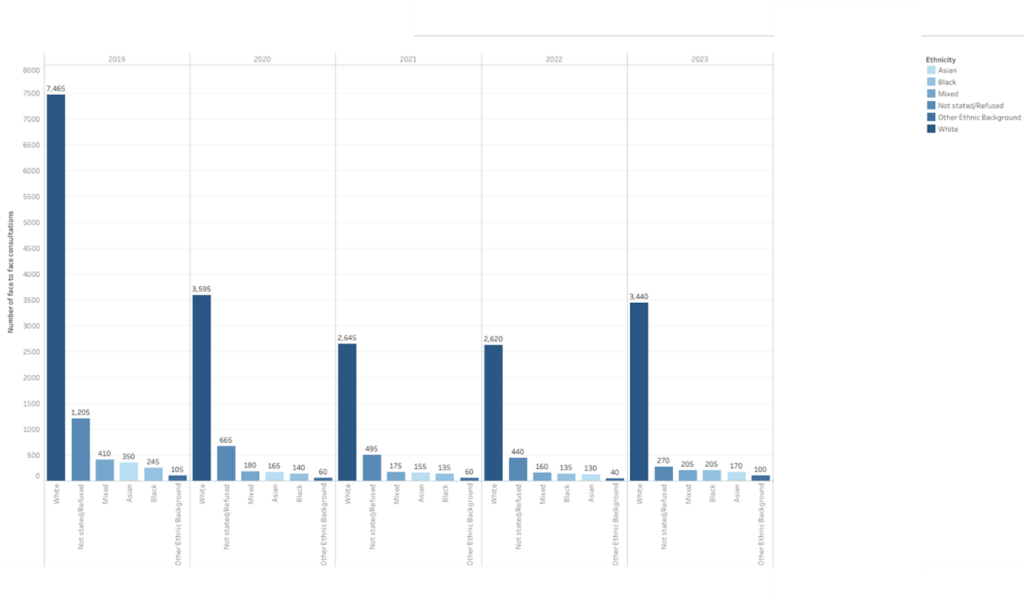
In 2023, almost half (46.6%) of face-to-face sexual health clinic consultations for contraception were by people in the two least deprived IMD deciles (Figure 7.15). This is not unexpected as more than half of Lower Layer Super Output Areas (LSOAs) in Surrey are in the least two deprived deciles [157].
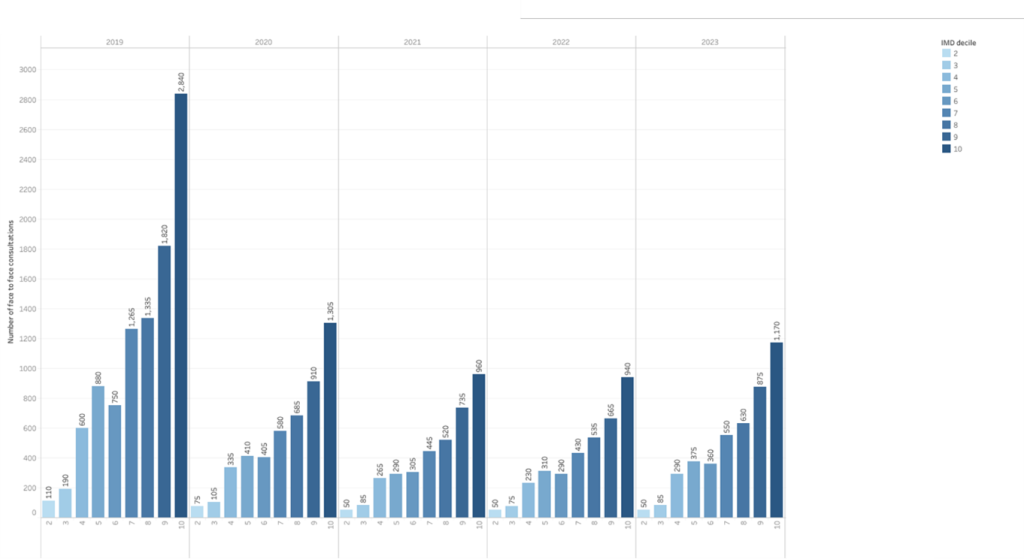
7.2.4.2 Online contraception consultations
As expected, due to COVID restrictions, the number of online sexual health clinic consultations relating to contraception by Surrey residents peaked in 2020. Since April 2021, the number of online contraception consultations have been steadily declining but still remain an important source of contraception services (Figure 7.16).
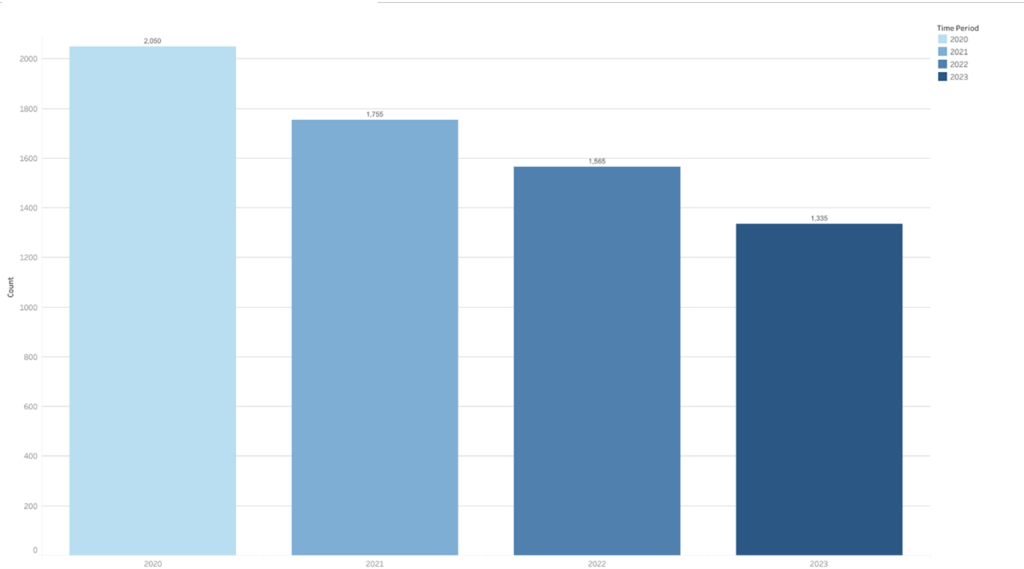
Interestingly, there has been an increase in online consultations by 18-24-year-olds which could suggest a change in preference on how this group access sexual health services. However, among 25-34-year-olds, there has been a decrease in online consultations (Figure 7.17). There has been a slight increase in sexual health clinic consultations in this age-group, however, this could also reflect changes in where this age-group are accessing contraception services (i.e. outside of sexual health clinics), or reduced use of contraception services if, for example, this age-group could be shifting away from hormonal contraception to barrier contraception methods.
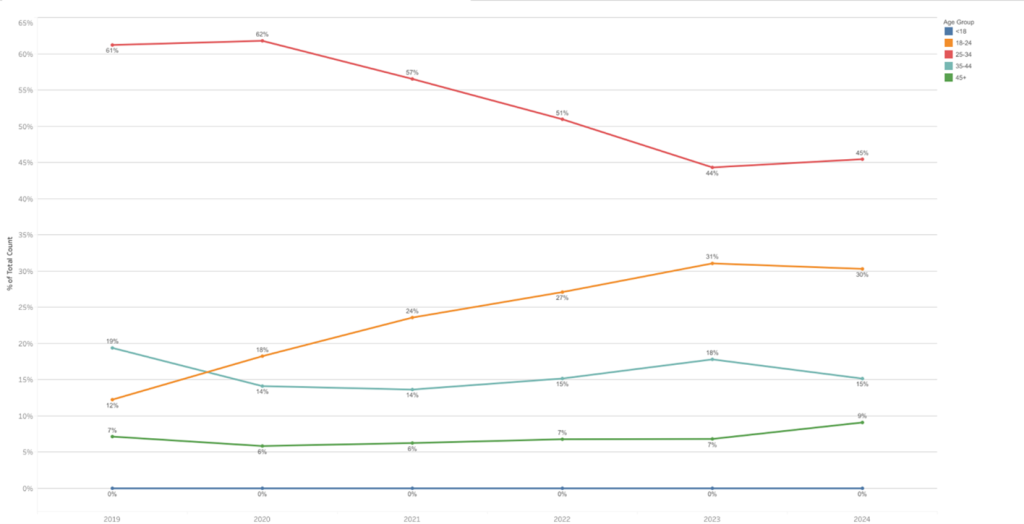
Online consultations by district and borough are shown in Figure 7.18. The three districts with the highest number of annual consultations in 2023 were Guildford (23% of all online consultations in Surrey), Woking (22% of all online consultations in Surrey) and Reigate and Banstead (17% of all online consultations in Surrey).
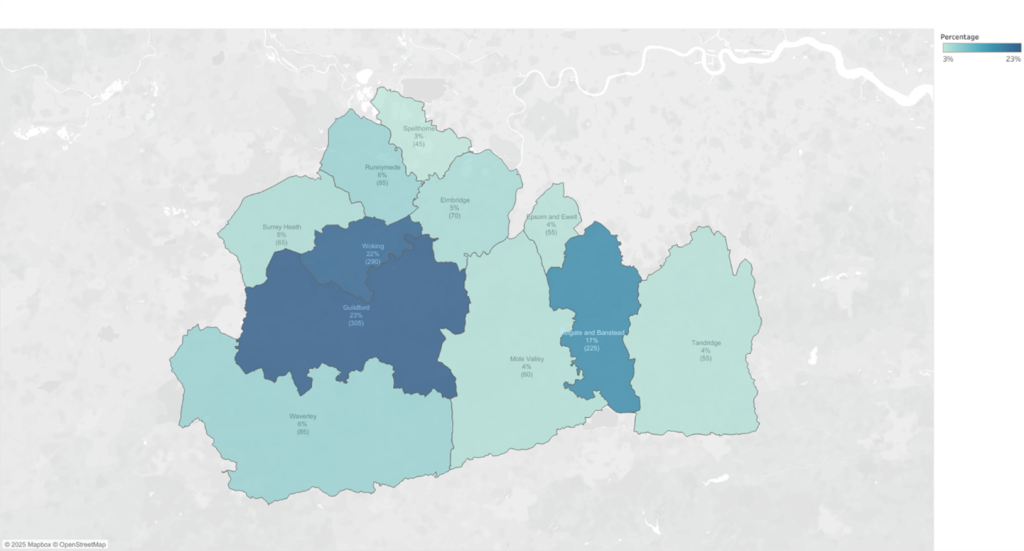
In Guildford, and Reigate and Banstead districts the majority of consultations were among residents aged under 35 years (88% and 80% respectively), whereas in Woking, this was slightly lower (65% of consultations were in residents aged <35 years, 24% in residents aged 35-44 years, and 12% in residents aged 45 or over) (Figure 7.19).
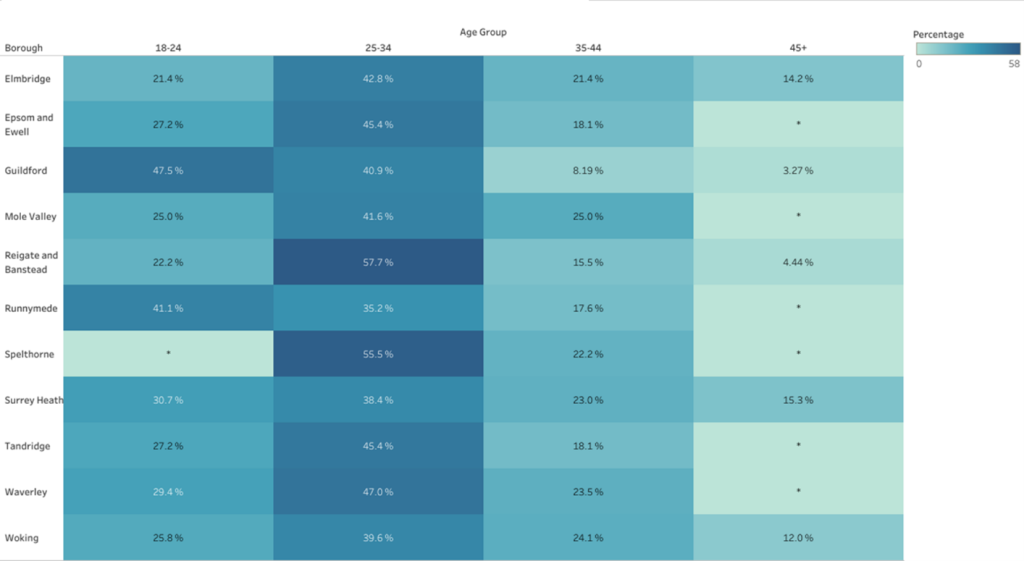
Between 2021 and 2024, around two-thirds of online contraception consultations in sexual health services have been for the progesterone-only pill and around one-third for the combined pill (Figure 7.20).
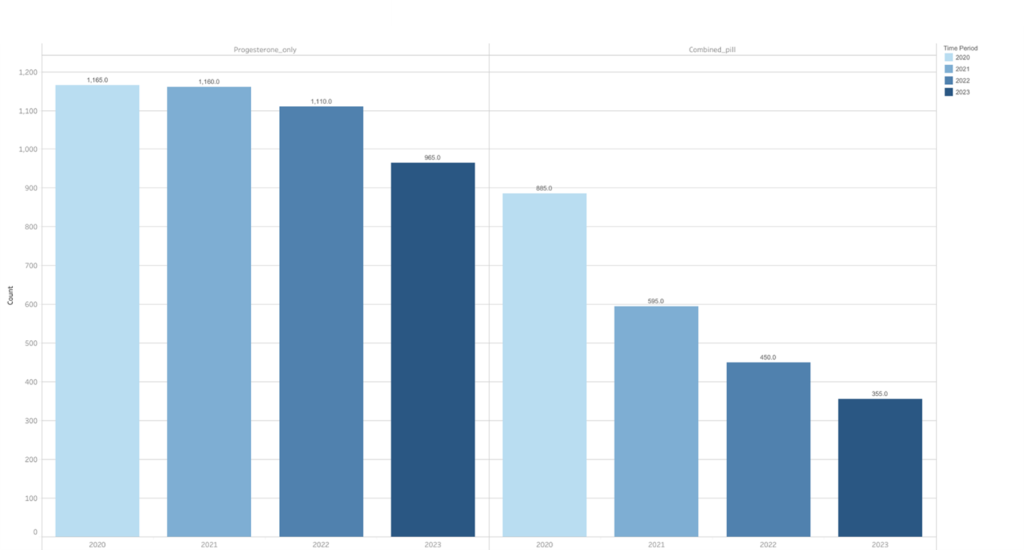
Notably, the number of online consultations for the progesterone-only pill and combined pill reduced dramatically among 25-34-year-olds between 2020 and 2023 (Figure 7.21). Similar declines in progesterone-only pill were not observed for other age-groups. There were some declines in other ages in online consultations for the combined pill although these were less dramatic. One possible explanation could have been that this age-group are seeking contraception from other services, such as GPs or pharmacies, although we do not observe increases in prescribed combined pill or progesterone-only pill at GPs (Section 7.4.2). Another explanation could be a change in preference for contraception methods away from short acting hormonal contraceptive methods. Nationally there have been emerging concerns among younger women about the negative impacts of hormonal contraception and an increase in the use of fertility apps.
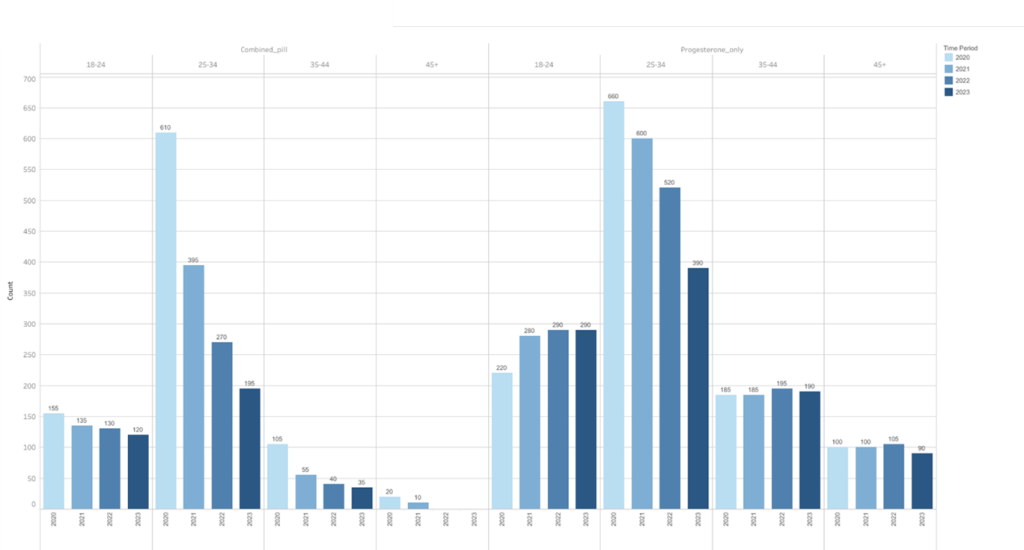
7.2.5 Out of area services
For the financial year of 2023/24, there were 13,290 clinic attendances (for both contraception and genitourinary medicine) of Surrey residents at Surrey’s specialist sexual health service (CNWL). However, some residents choose to access sexual health services delivered by providers outside of Surrey. The most commonly used providers by Surrey residents are Kingston Hospital NHS Foundation Trust (and Your Healthcare, who provide contraception services in Kingston) (n=3,800 Surrey residents used this service in 2023/24), Chelsea and Westminster Hospital NHS Foundation Trust (n=1,940), University Hospitals Sussex NHS Foundation Trust (n=1,040), Hampshire and Isle of Wight NHS Foundation Trust (n=730), and Epsom and St Helier University Hospitals NHS trust (n=605)
The rate of Surrey residents using out of area services for Surrey as a whole is 660 per 100,000 residents (0.7% of residents), compared with 1,082 per 100,000 Surrey residents using CNWL clinic services (1.1% of residents). However, there is variation by borough (Figure 7.22). Boroughs that are closer to the borders of Surrey have a higher proportion of residents using out of area services, indicating that use is likely to be driven by geographical proximity.
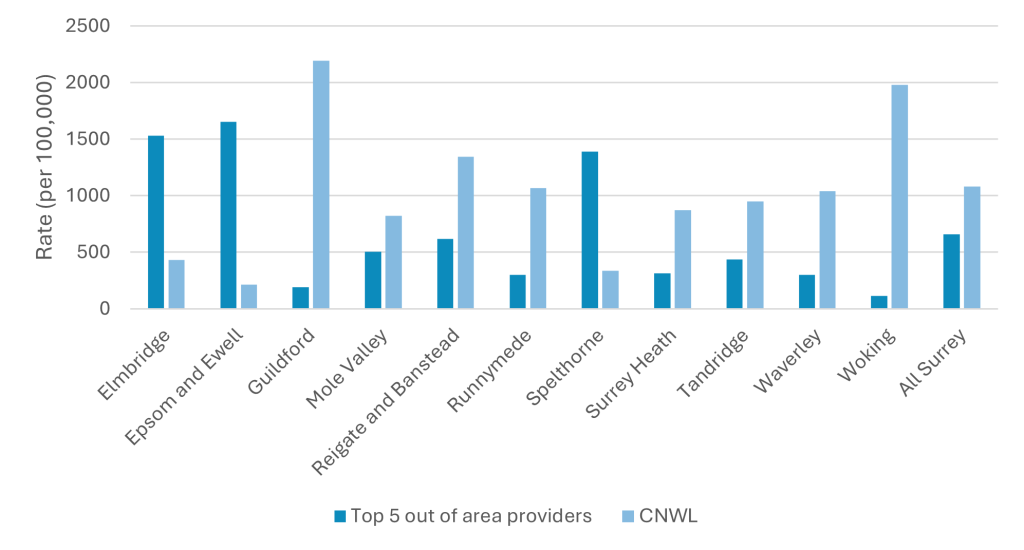
In Spelthorne, of the total number of individuals using a specialist sexual health clinic at CNWL or one of the top five out of area providers, 63% used a service provided by Chelsea and Westminster NHS Foundation Trust, 20% used CNWL services, and 17% used a service provided by Kingston Hospital NHS Foundation Trust (Table 7.2). This is because Spelthorne sits on the border of Surrey, and is in close proximity to services in Hounslow and Kingston. Whereas, for residents of Guildford and Woking, the vast majority of people using sexual health clinics used a service delivered by CNWL, as CNWL clinics are based in these boroughs. It is important to note that this analysis only includes a breakdown of activity at services provided by CNWL and the top five out of area providers and does not include specialist sexual health services provided by other out of area providers. There may also be duplication of individuals who use services provided by multiple providers.
| Provider | Elmbridge | Epsom and Ewell | Guildford | Mole Valley | Reigate and Banstead | Runnymede | Spelthorne | Surrey Heath | Tandridge | Waverley | Woking |
| Chelsea and Westminster Hospital NHS Foundation Trust | 5.6 | 6.2 | 2.0 | 4.3 | 2.3 | 15.4 | 63.4 | 3.7 | 3.2 | 1.7 | 3.0 |
| Epsom and St Helier University Hospitals NHS Trust | 0.4 | 16.3 | 0.0 | 3.8 | 8.8 | * | 0.0 | 0.0 | 2.0 | * | 0.0 |
| Hampshire and Isle of Wight NHS Foundation Trust | * | * | 4.5 | * | * | * | * | 21.9 | * | 17.0 | 0.7 |
| Kingston Hospital NHS Foundation Trust and Your Healthcare | 71.9 | 65.4 | 0.8 | 17.9 | 4.2 | 6.1 | 16.8 | 0.9 | * | 1.1 | 1.6 |
| University Hospitals Sussex NHS Foundation Trust | * | * | 0.7 | 12.0 | 16.2 | * | * | * | 25.3 | 2.5 | * |
| CNWL | 22.0 | 11.4 | 92.0 | 62.0 | 68.5 | 78.1 | 19.6 | 73.5 | 68.3 | 77.9 | 94.5 |
NB: This analysis does not include specialist sexual health services provided to Surrey residents by other out of area providers that are not included in the top five most commonly used out of area providers, and there may be duplication of individuals using multiple providers.
* indicates censored data due to a count of <8.
When exploring what types of sexual and reproductive health services individuals use out of area, using Kingston Hospital NHS Foundation Trust as an example, 59% of activity was relating to STI testing, treatment or prevention, 14% of activity was related to contraception, and 27% of activity was for another reason (including ultrasound, sexual and reproductive health advice, and sexual assault services). This indicates that the service use split between STIs and contraception is similar to that within Surrey, therefore there is unlikely to be a particular unmet need in relation to either STI or contraception care. The predominance of STI-related activity may indicate scope for Surrey residents to use CNWL STI testing services online, if appropriate, rather than using out of area in-person services.
7.3 Pharmacy services
7.3.1 Chlamydia testing and treatment in pharmacies
Of the 99 pharmacies accredited to provide chlamydia testing and treatment services in Surrey in 2024, 28 provided the service to a total of 180 individuals [unpublished data from PharmOutcomes reports]. The remainder may not provide services due to a range of reasons, including lack of time and competing clinical priorities. This number of pharmacies providing the service has risen from 19 in 2019, however the number of service users has remained relatively stable over time (Figure 7.23).
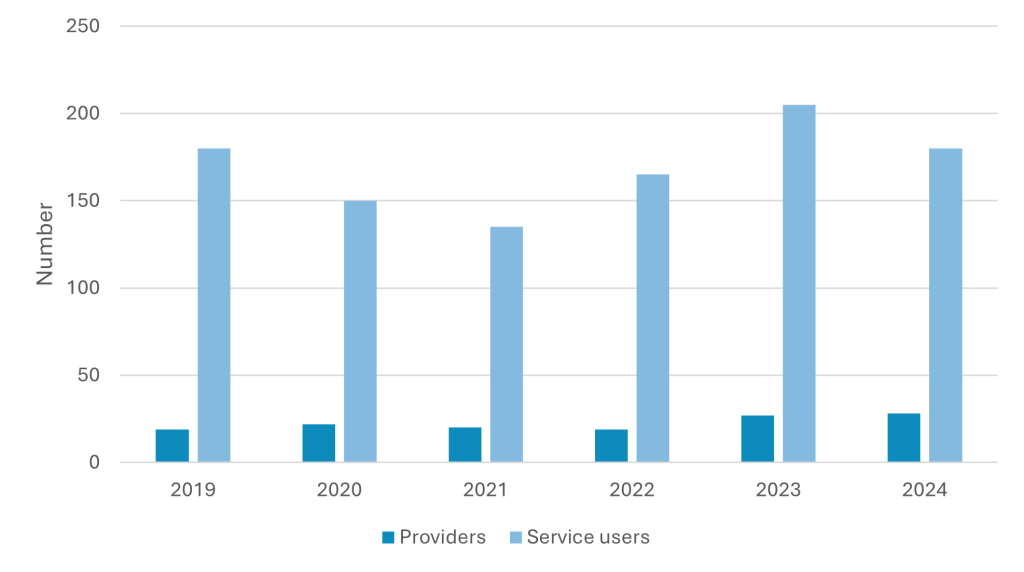
The majority of individuals using chlamydia testing and treatment services in Pharmacies Surrey are Surrey residents (86.1% in 2024), the service is also used by non-Surrey residents in a minority of cases (11.1% in 2024). Of service users accessing chlamydia testing and treatment in pharmacies, the majority are aged 20-24 years (n=115, 63.9% in 2024), and 52.8% identified as female, including transgender women. Whilst the number of individuals that this service is reaching is small, young women are a priority for chlamydia testing and treatment, due to the complications of untreated infection that they face. Therefore, the service is reaching this demographic group. In 2024, of the 180 service users, 125 were White British (69.4%).
Of the 180 individuals accessing chlamydia testing and treatment at pharmacies in 2024, 170 (94.4%) accessed the service because they were referred through the chlamydia screening service. This was the most common reason for accessing the pharmacy service across all years since 2019. The majority of individuals accessing chlamydia testing and treatment at a pharmacy attended on a weekday (94.4%). Pharmacies may play an important role in providing a chlamydia testing and treatment service on weekends when CNWL clinic services are not available, therefore the barriers to activity out of hours should be explored.
7.3.2 Emergency contraception services delivered in pharmacies
A total of 46 pharmacies in Surrey provided emergency contraception services on 1,035 interactions (this may include more than one interaction per service user) [unpublished data from PharmOutcomes reports]. The number of pharmacies providing the service and the number of interactions has been relatively stable over the last 5 years (Figure 7.24).
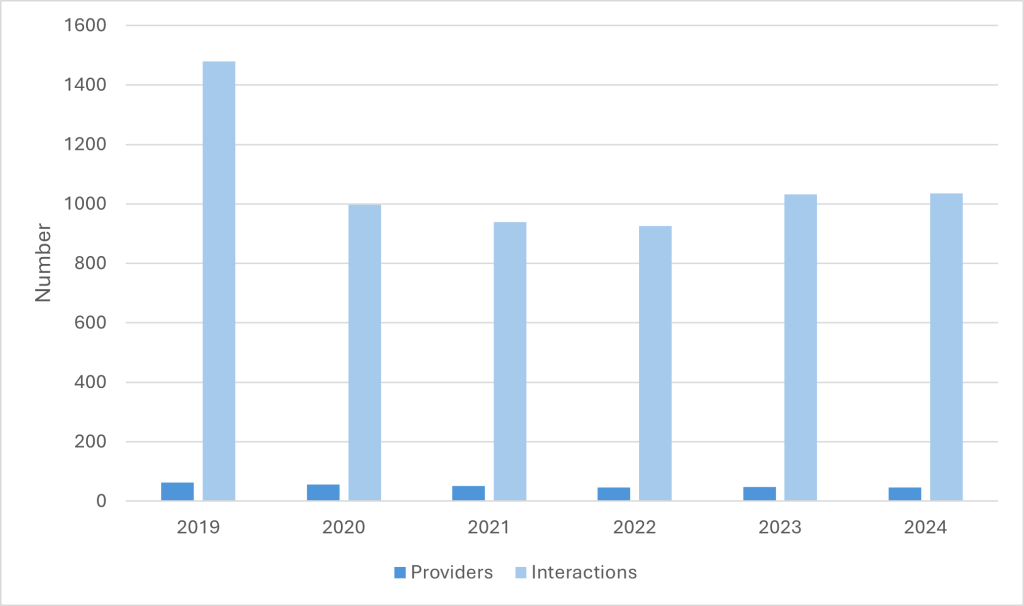
In 2024, the majority of users were aged between 16 and 24 years old (34% aged 16-19 years; 41% aged 20-24 years) and were white British (75% of service users with ethnicity recorded). Just over two-thirds (66.8%) of those using emergency contraception in 2024 did so because they did not use contraception, with a further 27.8% having a failure of barrier contraception (e.g. split condom) and 5.3% a hormonal contraception failure (e.g. missed pill or sickness)
7.4 Condom Distribution Scheme
There are a total of 94 providers signed up to deliver the CDS in Surrey, although not all are delivering the scheme actively. Education settings (n=29) and the youth, third sector, and voluntary services (n=21), pharmacies (n=13) and GPs (n=12) are the most common providers of the CDS in Surrey.
In financial quarter one of 2024 there were 223 individuals using the CDS in Surrey, of which there were 138 new registrations. A total of 1,090 condoms were distributed in quarter one of 2024, across a total of 128 visits by service users. Since 2022 (quarter three) the activity of the CDS, in terms of individuals registered, new registrants, number of visits, and number of condoms distributed, has risen. The number of condoms given out has risen by over ten-fold in this time, as has the total number of service users.
In 2024, the Public Health sexual health team ran a survey for young people under 25 exploring the CDS, which received 54 responses. The survey showed that young people’s preferred choice for accessing condoms was via a pharmacy. They are also keen to access condoms from non-clinical settings such as school, college and university. Online services were their third most preferred option.
The findings also highlight that while these locations are seen as the most convenient and accessible, significant barriers still exist. Young people reported that main barriers to accessing condoms are embarrassment, lack of information and confidentiality concerns. Addressing these concerns through more discreet and youth-friendly services could help improve access and promote better sexual health outcomes.
7.5 Contraception services delivered in primary care
7.5.1 Prescribed long-acting reversible contraception (LARC), excluding injections
LARC provides a reliable and convenient method of contraception with a high efficacy to reduce the risk of unintended pregnancy. Studies have demonstrated that LARC methods, such as an implant or IUS, have efficacy of over 99% [158] and are cost-effective in the long-term [159].
Contraception JSNA Fingertips dashboard | Tableau Public
In Surrey in 2023, there were 12,700 LARC prescriptions and the rate of total prescribed LARC (excluding injections) was 56.2 per 1,000 female population aged 15-44 years. There was a reduction in LARC use in 2020, likely due to the impact of the COVID pandemic, although rates have been increasing in 2021 and 2022 and are now similar to pre-COVID rates (54.6 per 1,000 females aged 15-44 in 2018 and 59.1 per 1,000 in 2019). These rates are higher than the national average for England (43.5 per 1,000 female population aged 15-44 in 2023) although follow a very similar trend over time for the past five years.
In 2023 in Surrey, the rates of total prescribed LARC varied substantially by district with Runnymede having the lowest rate at 29.2 per 1,000 female population aged 15-44 years. All other districts had total prescribed rates higher than the England average with Mole Valley having the highest rate at 81.3 per 1,000 female population aged 15-44 years.
Total rates include LARC prescribed in GPs and sexual health services. Across the last five years in Surrey, the proportion of LARC prescribed at GPs has remained relatively consistent at between 76% and 79% of the total prescribed LARC [160].
7.5.2 Prescribed oral contraception
This section includes data on women prescribed with short acting combined hormonal contraception and progesterone only pill, in both GPs and sexual and reproductive health (SRH) services [161].
The rate of women prescribed short acting combined hormonal contraception in both sexual health services and GPs is lower compared to rates prior to the COVID pandemic. The large majority of women access oral contraception from General Practice. In GPs, there has been a steady decline in the rate of prescribed combined hormonal contraception every year from 186.4 per 100,000 women in 2016 to 106.7 per 100,000 women in 2023. In specialist sexual health services, the rate declined from 23.6 per 100,000 women aged 15-44 years in 2016 to 7.6 per 100,000 women in 2021. Over the last two years, there has been a modest increase in the rate of prescribed short acting combined hormonal contraception to 9.1 per 100,000 women.
The rates of prescribed progesterone only pill in GP practices has varied over the past 8 years. The rate in 2023 was 125.5 per 100,000 women aged 15-44 years which has been declining since the peak rate in 2020 of 140.0 per 100,000 women. The rate of those prescribed progesterone only pill in SRH services has also varied over time. Although this has increased slightly for the past two years (from a rate of 9.6 per 100,000 women aged 15-44 years in 2021, to a rate of 11.6 per 100,000 women in 2023) this is still lower than the peak rates in 2016 of 18.8 per 100,000 women.
In summary, there have been reducing rates of prescriptions of short acting hormonal contraception in Surrey and nationally.
8 Insight from residents
A survey was distributed to Surrey residents to collect their thoughts and experiences of accessing sexual health services and contraception services in Surrey. Section 8.1 includes the responses related to sexual health services. Section 8.2 includes the responses related to contraception services. In addition Surrey residents panel were asked for their views (8.3) and focus groups with young people took place (8.4).
8.1 Sexual health residents’ survey
8.1.1 Key implications
- Whilst the respondents of this survey do not reflect the Surrey population, the survey findings provide key insights, particularly for cis-gender females and those aged 25-44 years. The majority of individuals had used a sexual health service for STI testing, with most reporting a positive experience of using a service that they found easy to access. Location was both a key determinant of difficulty of accessing a sexual health service in Surrey, as well as a driver of using a sexual health service outside of Surrey, and this is recognised to be a challenge to the geography of Surrey.
- Individuals’ preferences for accessing services were well aligned with the current service provision by CNWL, including the ability to book appointments online, and ability to access both face to face and online services. Reassuringly, when individuals were asked what could improve sexual health services for them, the responses were things that CNWL already provide, including an online booking system. This may indicate a lack of awareness of the service from some respondents. Overall, this indicates that the service provided is well suited to the needs of residents identified in this survey.
- Some individuals identified that they would prefer to access services in the evenings and weekends, therefore this may present an opportunity for building awareness of the services available during these times, including online test kit ordering, and pharmacy services.
- This survey highlights that the internet is a key source of information for the majority of respondents. Whilst most reported using reputable online sources, the risk of misinformation should be a key focus, particularly in younger individuals, who were not well represented in this survey, but who may be more likely to use social media to inform their sexual health understanding and choices.
8.1.2 Respondents
This section includes a summary of the survey results related to sexual health services. Full details of the responses to the sexual health questions of the survey are available on request.
There were a total of 121 questionnaire responses to the sexual health questionnaire completed by Surrey residents. A minority of questionnaires were completed on behalf of someone else (n<5).
The majority of the 121 respondents reported their sex to be female (n=85, 70.2%), and the age category with the most respondents was 35-44 years (n=44, 36.4%) followed by 25-34 years (n=37, 30.6%). The majority of the 121 respondents reported that their ethnic group was white British (n=90, 74.4% of respondents), with low numbers of respondents from other ethnic groups. A total of 44 of the 121 respondents indicated that they are disabled (36.4%).
Of all respondents, 116 (95.9%) reported that the gender they identify with is the same as their sex registered birth, and the majority identified as women (n=82, 67.8%). A total of 57.9% of respondents (n=70, respondents were able to select more than one response) selected that they were heterosexual or straight, 16.5% identified as gay (n=20), and 15.7% as bisexual (n=19).
8.1.3 Use of sexual health services in Surrey
Individuals were asked about the last time they used a sexual health service in Surrey. A total of 83 individuals had previously used a sexual health service in Surrey and gave a valid response to the question. When asked when they had last used a sexual health service in Surrey, 31.3% (n=26) reported they had used a service within the last month, 22.9% (n=19) in the previous 1-6 months, 12.0% (n=10) in the previous 6-12 months ago, and 33.7% (n=28) more than a year ago.
Individuals were asked what they used a sexual health service for the last time they accessed it, with 82 individuals giving reasons for their use (respondents were able to select multiple answers). The most common reason was STI testing at the Surrey sexual health service (n=40, 48.8% of respondents) (Figure 8.1).
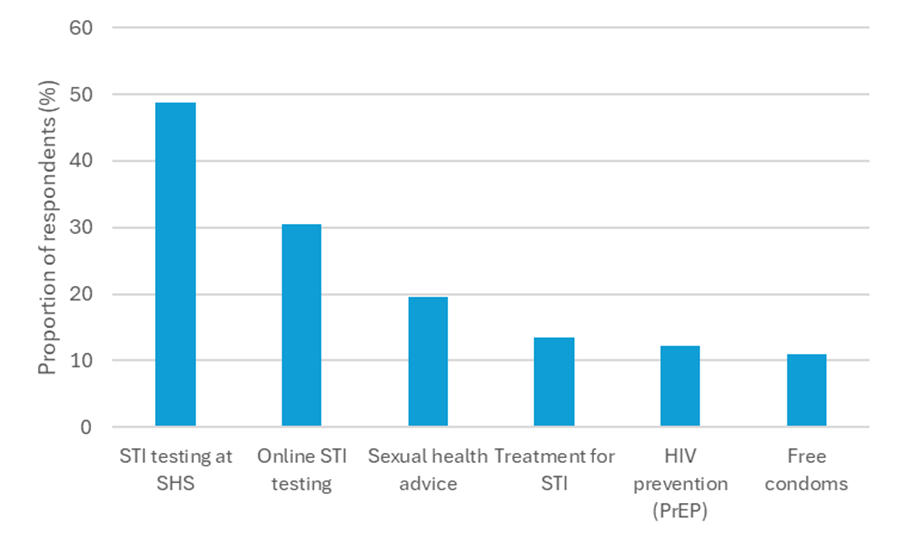
Abbreviations: PrEP: pre-exposure prophylaxis; SHS: sexual health service
When asked where they last accessed a sexual health service in Surrey, 82 individuals gave a response. Of these, 57.3% (n=47) of respondents reported that they used a sexual health clinic in person, 23.2% (n=19) used a sexual health service online, and 6.1% (n=5) visited their GP surgery in person.
8.1.4 Experience of accessing sexual health services
Of the 83 respondents, the majority reported that the last time they accessed a sexual health service in Surrey, it was very easy to access (n=31, 37.3%), and 73.5% (n=61) of respondents reported it was very easy or quite easy to access. Of those who found it quite or very difficult to access the sexual health service the last time they used it (n=14), the most commonly reported reasons were inconvenient location (n=8, 57.1%), not being able to access the service quickly enough (n=7, 50.0%), and not being able to use the service at a convenient time (n=6, 42.9%).
Of the 83 respondents, the majority reported that they were very satisfied (n=38, 45.8%) or satisfied (n=31, 37.3%) with the service they received when they last accessed a sexual health service in Surrey.
8.1.5 Sexual health services outside of Surrey
Of the 121 respondents, 29.8% (n=36) reported that they had used a sexual health service outside of Surrey whilst living in Surrey, whilst 70.2% (n=85) did not. Of those who had used a sexual health service outside of Surrey (n=36), the most commonly reported reasons for this were being able to get an appointment more quickly (n=13, 36.1% of respondents), more convenient appointment times (n=8, 22.2%), a location nearer to the individual’s home (n=7, 19.4%), nearer to the individual’s educational establishment (n=5, 13.9%), the service having a good reputation (n=5, 13.9%), and feeling the service outside of Surrey met their needs better (n=5, 13.9%).
8.1.6 Preferences for accessing sexual health services in Surrey
Individuals were asked about their preferences for accessing sexual health services, and were able to give multiple responses to each question. 120 individuals responded to the following questions.
Individuals were asked how they would prefer to book appointments for sexual health services. Booking appointment for sexual health services online was selected by the vast majority of individuals (n=114, 95.0%).
Individuals were then asked how they would prefer to access sexual health services. Accessing sexual health services at a face-to-face pre-booked appointment was selected by 83.3% (n=100) of individuals, followed by an online ordering service (e.g. STI test kits ordered online) (n=69, 57.5%), face-to-face walk-in appointments (n=62, 51.7%) and telephone consultations (n=40, 33.3%).
Respondents were asked where they would like to access sexual health services. A sexual health clinic was selected by 85.0% (n=102) of respondents, followed by GP surgery (n=84, 70.0%) and pharmacy (n=46, 38.3%).
Respondents were asked when they would prefer to access sexual health services, and were able to give multiple responses. Of the 121 individuals who responded, the most commonly selected time was a weekday evening (after 5pm) by 59.5% (n=72) of respondents. Weekend (n=60, 49.6%) and weekday daytime appointments (n=46, 38.0%) were also popular responses (Figure 8.2).
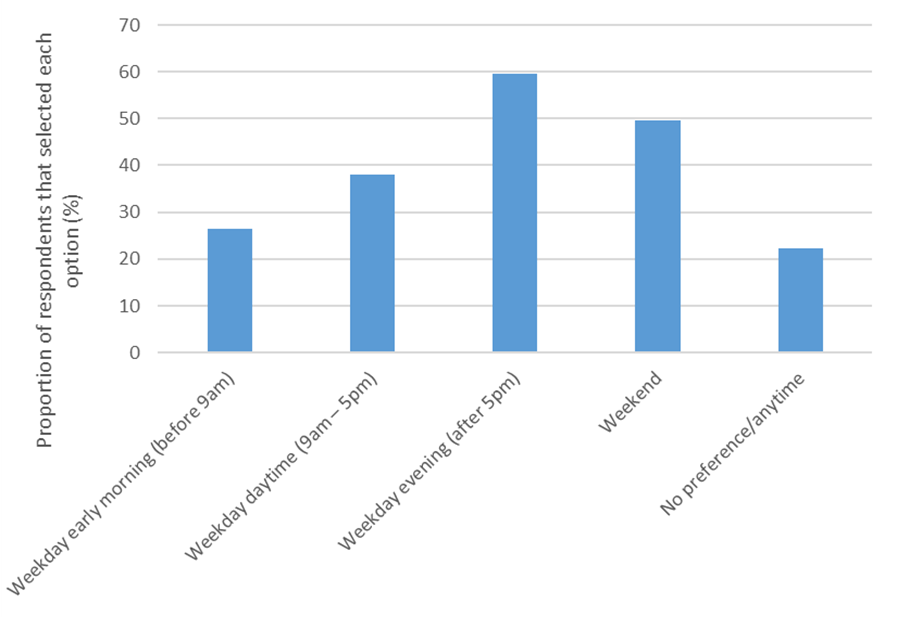
8.1.7 Improving sexual health services
Respondents were asked what could improve sexual health services for them, and were able to give multiple responses. Of the 119 individuals who responded, the most commonly selected improvement was the ability to book appointments online (n=91, 76.5% of respondents), followed by more self-test kits available to order online (n=54, 45.4%) and more walk-in and wait sessions (n=52, 43.7%).
8.1.8 Finding information on STIs
Individuals were asked where they would go to find information on STIs, and were able to select more than one response. 115 responses were received for this question. The most commonly selected response, by far, was the internet (n=111, 96.5%), followed by a GP or nurse (n=56, 48.7%) and the Surrey Sexual Health service (n=54, 47.0%) (Figure 8.3).
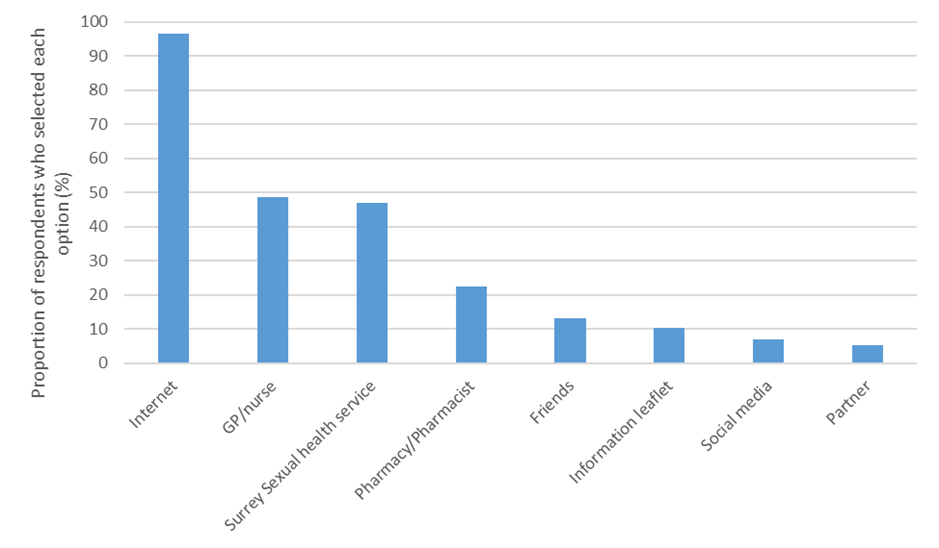
Respondents were then asked, if they were to look online for information on STIs, where they would look. Again, they were able to select multiple options, and a total of 120 individuals responded to this question. The most commonly selected response was the NHS online website (n=97, 80.8%), followed by an internet search engine (n=87, 72.5%) and the Surrey sexual health service website (n=45, 37.5%) (Figure 8.4).
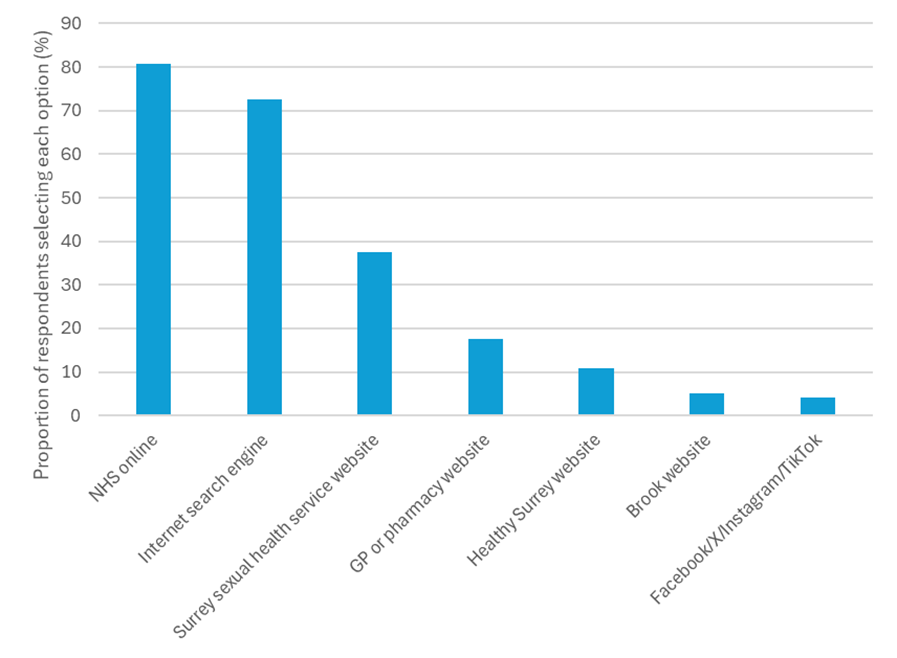
Individuals were asked to rate how comfortable they would be to discuss sexual health with a range of people. They were able to score this from ‘not at all comfortable’ (1 on the scale) to ‘very comfortable’ (5 on the scale). Due to small numbers of responses in some categories, data has been grouped for scores 1 and 2 (uncomfortable), 3 (neither uncomfortable nor comfortable) and 4 and 5 (comfortable). The groups that received the highest proportion of responses indicating that individuals would be comfortable to discuss with them were Surrey Sexual Health Service (n=97, 84.3%), a GP or nurse (n=90, 74.4%) and partner (n=83, 83.0%).
8.2 Contraception residents’ survey
8.2.1 Key Findings and implications
- Among the respondents to the contraception survey, over 70% had accessed contraception services in Surrey and offer some important insights into service use and preferences.
- Respondents accessed services at GP surgeries, sexual health clinics and pharmacies and this generally aligned with their preferences. Most of those that had accessed services found it easy although there was still a noteworthy proportion that had difficulties accessing services due to inconvenient clinic location, inconvenient clinics times or challenges with booking appointments.
- Whilst the vast majority of respondents preferred to book contraception services online, there was a desire for flexibility with options for walk-in appointments and phone booking. Similarly, most respondents preferred face-to-face appointments but valued flexibility of having online services, telephone appointments, and the option for appointments at evenings and weekends.
- A variety of contraception methods were used and the majority of respondents were able to get their preferred method of contraception. Almost all respondents stated that the internet would be their main key source of information on contraception which highlights the importance of ensuring that trusted internet sites have high quality information available.
8.2.2 Respondents
This section includes a summary of the survey results related to contraception services. Full details of the responses to the contraception questions of the survey are available on request.
There were 97 responses to the contraception questionnaire completed by Surrey residents. The majority of respondents reported their sex at birth as female (90.7%), and the age category with the most respondents was 35-44 years (36.1%) followed by 25-34 years (33.0%). Of all respondents, 94.8% reported that the gender they identify with is the same as their sex registered birth, whilst 5.2% reported their gender was different to the sex registered at birth. A total of 68.0% of respondents selected that they were heterosexual or straight (n=66, respondents were able to select more than one response), 14.4% identified as bisexual (n=14) and 7.2% as pansexual (n=7).
8.2.3 Use of contraception services in Surrey
A total of 70 respondents (72.2%) had reported ever having used contraception services in Surrey. Participants were asked what services they had used and could provide more than one response. The most common responses were GP survey in person (72.9% of respondents) and Sexual Health clinics in person (57.1% of respondents).
Most respondents (67.6%) accessed services for contraception to prevent pregnancy. Other responses were accessing contraception for another reason, for example to manage menstrual symptoms, or to regulate my periods (23.5%), for contraception advice (13.2%) and for emergency contraception (11.8%) (Figure 8.5). Other less common reasons included contraception to prevent STIs and for removal of contraceptive devices.
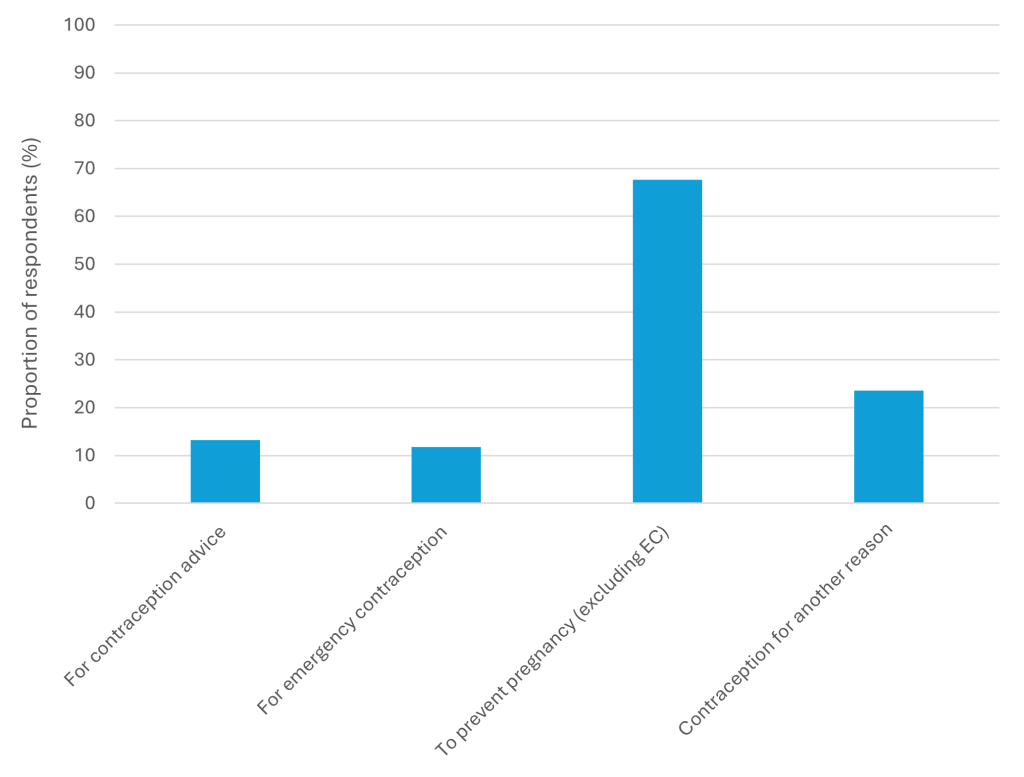
Of the 70 respondents, the majority reported that the last time they accessed a contraception service in Surrey, it was very easy or quite easy to access (60.0%) although 25.7% did find access quite difficult. This varied by service type, with 68.6% (24/35) attenders at GP surgery finding it quite or very easy, compared with 43.8% (7/16) of attenders at sexual health services finding it quite or very easy.
Of those who found it quite or very difficult to access the contraception service the last time they used it (n=22), the most commonly reported reasons were inconvenient location (50.0%), not being able to access the service quickly enough (50.0%), not being able to use the service at a convenient time (40.9%), and difficulties with being able to use the appointment booking system (31.8%).
8.2.4 Use of contraception services outside of Surrey
Of the 97 respondents, 29.9% reported that they had used a contraception service outside of Surrey whilst living in Surrey, whilst 70.1% did not. Of those who had used a contraception service outside of Surrey (n=29), there were many different reasons for this with the most commonly reported reason that the clinic was in a location nearer to the individual’s school, college or university (20.7%).
8.2.5 Preferences for accessing contraception services in Surrey
Individuals were asked how they would prefer to book appointments for contraception services, and were able to provide more than one response. Of the 97 respondents, booking appointment for contraception services online was selected by the vast majority of individuals (90.7%). Accessing services by a walk-in appointment was selected by 36.1% of individuals, and booking appointments by phone was selected by 35.1% of respondents.
Individuals were asked how they would prefer to access contraception services, and were able to provide more than one response. Many of the respondents included multiple preferences. The most common responses were face-to-face appointments (71.1%), online contraception services (56.7%), walk-in face-to-face visits (47.4%) and telephone appointments (29.9%).
Respondents were also asked where they would like to access contraception services, and again were allowed to select multiple responses. Of the 97 individuals who responded to this question, the most common responses were GP surgery (74.2%), sexual health clinics (63.9%) and pharmacy (53.6%).
Respondents were asked when they would prefer to access contraception services, and were able to give multiple responses. Of the 97 respondents, 22 (22.7%) had no specific preference. Of those who did have a preference, the most commonly selected time was a weekday evening after 5pm (66.7%) and at a weekend (61.3%). Weekday daytime appointments and weekday morning appointments were selected by 42.7% and 36.0% of respondents respectively.
Respondents were asked what could improve contraception services for them, and were able to give multiple responses. Of the 97 individuals who responded, the most commonly selected improvement was the ability to book appointments online (selected by 77.3% of respondents), more walk-in and wait sessions (38.1%), and more contraception to be available to order online (35.1%).
8.2.6 Contraception use and preferences
The vast majority of respondents (98.9%) had used contraception at some point (either current or past users) with 62.4% currently using contraception. Respondents were asked about the type of contraception that they are currently using. The most common types of contraception used were condoms (31.0%), intrauterine system (IUS) (25.9%) and IUD (20.7%).
The 34 respondents who were not currently using contraception but had previously used were asked about when they stopped using contraception, and their reason for stopping contraception. The majority of these respondents stopped using contraception more than one year ago (72.7%). For reason for stopping contraception respondents could report multiple reasons. Among those that stopped, the majority (71.9%) stopped because contraception was no longer required, either because they were trying to conceive, following menopause, or for other reasons. Other common reasons for stopping contraception were side effects (37.5%) and wanting to stop, take a break from, hormonal contraception (25.0%).
8.2.7 Finding information on contraception
Respondents were asked where they would go to find information on contraception and were able to select more than one response. Of 90 respondents, the most common responses were the internet (96.7%), a GP or nurse (61.1%) and a Sexual Health service (42.2%) (Figure 8.6).
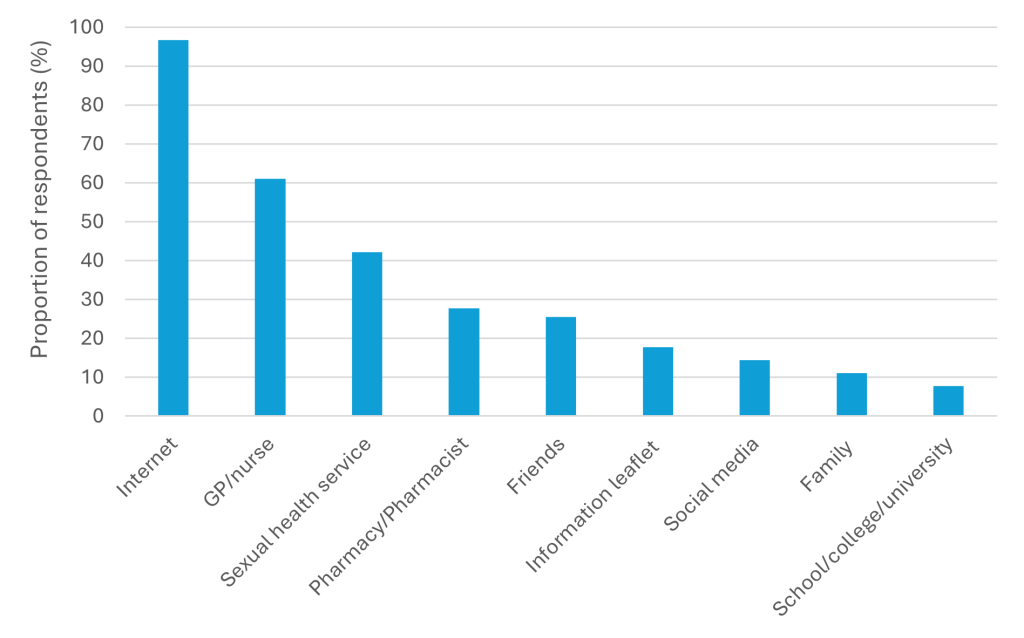
Respondents were then asked where they would look for information on contraception online (including internet and social media). Again, respondents were able to select more than one response. Of 96 respondents who answered this question, the most common responses were the NHS online website (81.3%), an internet search engine (60.4%), the Surrey sexual health service website (37.5%), and a GP or pharmacy website (25.0%).
Finally, individuals were asked to rate how comfortable they would be to discuss contraception with a range of people. The groups that received the highest proportion of responses indicating that individuals would be comfortable to discuss with them were their partner (94.0%), Surrey Sexual Health Service (86.4%), a GP or nurse (85.7%), a midwife (85.1%), and friends (74.7%).
8.3 Resident panel feedback
8.3.1 Key findings and implications
- The resident panel survey was weighted to better reflect the demographic breakdown of Surrey. Most respondents had not used a sexual health service in Surrey and, among those that had, the majority had used the service more than 2 years ago. A higher proportion of respondents had used a contraception service in Surrey although this varied greatly by sex (with around two-thirds of females having used a contraception service, but most males had not).
- Among respondents that had accessed sexual health services, this was mostly at sexual health clinics. However, among all respondents (including those that hadn’t accessed services in Surrey), there was a preference to be able to access services at multiple different settings, with GP surgery being the most common response, and a flexible approach to appointments with face-to-face, telephone and online options. This likely reflects differences in preference depending on demographics and sexual health and contraception needs.
- For contraception services, most of those accessed services at GP surgeries, which aligned with the preferences among all respondents. Similar to sexual health services, respondents wanted flexible options for appointment types (i.e. face-to-face, telephone and online).
- When asked about where respondents would find information on sexual health (STIs and contraception), around two-thirds said the internet and a similar proportion said a GP/nurse. This differed slightly from the more detailed sexual health and contraception residents’ surveys (Sections 8.1 and 8.2) where almost all respondents would use the internet for information. However, although this proportion is lower than the other survey, this still highlights the importance of the internet as a source of information on sexual health.
8.3.2 Findings
A total of 715 residents responded to the survey using an online platform. Full results are available on a public dashboard: Sexual Health January 2025 | Tableau Public.
As described in the methods section, responses were weighted by age and sex, hence these demographic breakdowns align with the population of Surrey. After weighting, over 90% of responders identified as heterosexual or straight, with 2.3% identifying as bisexual and 1.8% identifying as gay.
The first questions (Q2 to Q7) relate to sexual health services in Surrey.
Of all responders, the vast majority (80.6%) had never used a sexual health service in Surrey, although this was very dependent on age (this proportion was much lower in 25–34-year-olds (63.1%) and 35-44 year olds (71.1%)), and sex (87.6% of males had never used a sexual health service in Surrey, compared to 73.8% in females)). The most common reasons for using sexual health services were for testing or treatment of STIs (12.4%), sexual health advice (9.1%) and free condoms (4.5%).
Among responders that had used a sexual health service in Surrey, the majority of these (70.1%) had used the service over 2 years ago, with 20.3% having used a service in Surrey within the last 12 months.
Of those that had attended services in Surrey, the majority (65.5%) attended a sexual health clinic, with 21.2% attending a GP surgery and the remaining attending a different service (including a pharmacy or CDS outlet). Interestingly, this differed from preferences from all responders on where they would like to access services (responders could select more than one response, hence percentages sum to more than 100%); 73.5% responders said they would like to access services at a GP surgery, 47.7% at a sexual health clinic, 26.4% at a pharmacy and 24.2% on another online website.
The number of responses regarding access to sexual health services were relatively limited (n=33) although the majority of responders felt it was easy to find out about services, easy to use the appointment booking system, the location was convenient, the service opening times were convenient, and the service was accessible. Under 50% of responders to this question felt they could access the service they needed quickly with 41.6% disagreeing or strongly disagreeing with this statement.
Responders were then asked about how they would prefer to get support from sexual health services (responders could select multiple options so percentages sum to more than 100%). Three-quarters of responders (75.0%) preferred the option of face-to-face appointments, 45.8% a telephone consultation, 37.4% online ordering (e.g. online STI testing kits) and 25.9% an online video consultation.
The next questions (Q8 to Q13) related to contraception services in Surrey.
Over 60% of responders (62.6%) had never used a contraception service in Surrey although this was very different for males and females (93.1% of males had never used a contraception service in Surrey, compared to 33.3% of females). Among female responders, this was also very variable by age (ranging from only 8.0% of females ages 25-34 years that had never used a contraception service in Surrey, to 57.4% in 65+ year olds). Among females that had used a contraception service, 44.3% use the service for contraception to prevent pregnancy (excluding emergency contraception), 31.1% for advice about contraception, 27.2% for contraception for a different reason, and 18.7% for emergency contraception (responders could select multiple responses).
Among those that had used a contraception service in Surrey, just over two-thirds (67.7%) had used this service more than two years ago, with 18.5% using a service within the last 12 months. The majority of these responders access services at a GP surgery (77.2%) with a smaller percentage accessing at a sexual health clinic (13.0%) or a pharmacy (10.5%). Among all responders (including those that had not used a service in Surrey), the majority still said they would like to access services in a GP surgery (61.5%) with fewer 38.5%, 32.8% and 22.2% of responders saying they would like to access services at a pharmacy, sexual health clinic, or other online website, respectively.
Similarly to the sexual health response, the number of responses regarding access to contraception services were relatively limited (n=70). The majority of responders felt it was easy to find out about services, the location was convenient, the service opening times were convenient, they could access the service quickly, it was easy to use the appointment booking system, and the service was accessible.
Responders were then asked about how they would prefer to access contraception or support from contraception services (responders could select multiple options so percentages sum to more than 100%). Over half of responders (57.4%) preferred the option of face-to-face appointments, 39.2% a telephone consultation, 29.7% online ordering and 21.8% an online video consultation.
The final question, Q14, asked about where responders find information on all aspects of sexual health (including STIs and contraception). A similar proportion of responders would find information on the internet (65.6%) or from a GP/nurse (63.2%). Other common sources of information were from a pharmacy (30.1%) and asking friends, family or a partner (18.4%).
8.4 Focus groups
8.4.1 Key findings and implications
- The focus groups aimed to understand young people’s perspectives on accessing sexual health and contraception services in Surrey, particularly due to low survey response rates from this group. Across both the sessions, the discussions involved 10 participants aged 13-25, conducted both online and in person.
- The discussions focused on how young people find information about sexual health, where they go for support, and the barriers they face in accessing services. It was found that there was no single primary source for sexual health information; participants reported using a mix of online resources, healthcare professionals, and community staff. Social media was mentioned cautiously as a potential source of information, with participants favouring content from reliable, expert sources.
- Participants expressed varying levels of awareness of available services, with some being unaware of options like pharmacies for sexual health. When discussing service access, barriers such as transport and appointment booking were highlighted, with preferences for online or in-person booking over telephone services.
- Concerns around confidentiality were raised, especially regarding the visibility of sexual health clinics. Participants suggested improvements such as more discrete service locations, better communication about appointment details, and trained staff to handle mental health and additional needs. They also recommended more inclusive and accessible waiting rooms and clearer guidance for signing in to ensure comfort and privacy during visits.
8.4.2 Methods
Due to a low response rate from young people in our surveys, engagement with this important group and hearing the voice of young people in Surrey was a key priority. In order to meet this gap in engagement, focus groups with young people were conducted. Two focus groups were completed as follows:
- A session of 5 participants aged 16-25 years old attended a session held using an online platform. The participants were recruited through Surrey Youth Voice.
- A session of 5 participants aged 13-23 years old attended an in-person session at a Twister youth group.
The focus group discussions were all around 60-minutes and were guided by a semi-structured interview schedule that covered the following topics:
- How young people find out about key issues including sexual health and/or contraception
- Where young people think they/their friends might go if they had specific issues with sexual health and/or contraception
- Whether young people think there is anything that could make it difficult for them to access advice or support about sexual health and/or contraception
8.4.3 Findings
8.4.3.1 Sources of Information about sexual health and contraception
- There was no single primary source of sexual health information. Participants reported seeking information from online resources, sexual health and contraception services in different settings, and seeking advice or information from trusted individuals (including healthcare professionals, family members, teachers, and staff/volunteers from community groups).
- Services where participants would seek information about sexual health and contraception included general practitioners (GPs), sexual health clinics and hospitals. Participants suggested that they may feel more comfortable seeking advice or information from a setting if they had previous experience with that service.
- Online sources of information included using a search engine, using a GP website, or using an NHS symptoms checker website.
- Participants did not initially suggest social media as a potential source of information. When specifically asked about social media platforms, participants expressed that they may find this useful although they would be cautious using these platforms as a source of information. In particular, participants suggested that they may only look to certain social media platforms which they considered more reliable, posts which linked to official data sources or websites, or posts from reliable accounts, such as posts by doctors, registered nurses and/or other experts. Some participants said that they would find it useful if sexual health services were promoted on social media. Participants had different opinions on whether they would feel confident in identifying which content on social media could be trusted.
Reactions about sources of information about sexual health
Trust in social media:
“I wouldn’t initially use social media but I think as a resource for things like this [sexual health] might be useful”
“you can usually tell if someone is educated in the field and who to trust on social media”
8.4.3.2 Knowledge and awareness of sexual health and contraception services in Surrey
- Some participants had a good understanding of different sexual health services including sexual health clinics, GPs, and pharmacies. Participants also mentioned NHS111 and A&E although acknowledged that they were less clear whether these services could be used for sexual health. However, this was variable between groups, with some participants being less aware of available services in Surrey. When asked, some participants were unaware that pharmacies offered any sexual health services.
- Participants expressed that they would seek support or advice on which services were available from trusted individuals including family members, staff/volunteers from community groups, and/or school nurses.
8.4.3.3 Preferences for online vs. in-person attendances
- Participants’ preference between online and in-person services varied although generally they expressed that this would depend on the urgency and severity of the situation. Participants suggested that if they were particularly worried, or wanted a quick appointment, they would prefer to attend in person. However, if there was less urgency, participants preferred the options of online services.
- Some participants raised that they felt online services and information may be unclear, so they would prefer to attend a clinic in person to mitigate this.
- Some participants expressed a preference for online services to provide more privacy and confidentiality. Conversely, some participants expressed concerns about confidentiality if sexual health testing kits or contraception was sent in the post to a home address.
8.4.3.4 Barriers and facilitators to accessing sexual health and contraception services in Surrey
- Several participants highlighted challenges accessing services. This included two key areas; transport to services, and ability to be able to book appointments. Barriers around transport are included in the following section. For appointment booking, participants preferred in-person or online booking rather than telephone booking which could have a long wait. At time of booking, participants expressed a preference for being able to view available dates and times up to one month ahead, but that it was important that appointments would be available within a week for more urgent issues. Another potential barrier raised related to accessibility was that participants weren’t aware that they were able to access all clinics (and not just young people’s clinics).
- Participants highlighted uncertainty and fear about accessing services which were unfamiliar to them. This could be of particular importance for some individuals, such as people with autism. It was suggested that clear explanations of what to expect during the visit would be beneficial. Suggestions included providing clear information on how to get to the service, what to do at arrival at a service (for example, whether it is necessary to sign in at a reception desk), providing a virtual walkthrough on websites, and fixed appointment times to avoid uncertain waiting times. It was suggested that information should also be provided in easy read format.
- Some participants raised concerns about not wanting to access services if they were clearly labelled as sexual health clinics. As a result, they preferred accessing services within general health settings, or services with more discrete signage. Some participants also raised concerns with having to speak to receptionists in an area where this could be overheard.
- Some participants expressed a view that young people’s clinics (for example, for 13-19 year olds) would make it easier to access services.
- Having staff trained to understand different situations was a key theme identified. Specific issues raised by participants included having staff trained in mental health and additional needs and disabilities, in trans issues, gender dysphoria and body dysphoria, and in trauma informed care.
- Participants expressed that they may have a preference regarding the gender of the member of staff who they would be seen by, and had concerns about whether this could be accommodated.
- Participants expressed concerns about confidentiality attending services including whether parents may find out, or someone they know seeing them accessing the service.
Reactions about barriers and facilitators for accessing services
Challenges booking appointments:
“I would prefer to book appointments online or using an online form rather than phone where you may have to wait in a queue”
Uncertainty and fear about accessing services:
“I would like a virtual building walkthrough to know where to go and what to do”
“If an appointment is at a fixed time, then you can prepare and know what to expect [unlike a walk-in]. I like to know what to expect in advance”
Awareness and understanding of staff:
“Staff trained in mental health and additional needs and disabilities [means you] feel like you are in a safe pair of hands”
8.4.3.5 Considerations related to travelling to sexual health and contraception services in Surrey
- Participants were asked about their preferred location of services. Some participants suggested that this is often a balance between not being too close to home/place of education/place of work (in case they were recognised) but being within a reasonable distance.
- A key theme raised by participants was the importance of public transport access to services. It was raised that not only were good public transport links important, but also clear directions with different travel options should be included on information provided by services.
- There was some discussion that the distance people would be willing to travel for a service varied depending on the severity. There was general agreement that participants would ideally not have to take more than two buses, and travel for no longer than 45-60 minutes (although some participants would not have been willing to travel for this long).
8.4.3.6 Other suggestions for Improvement
- Participants had several suggestions that they felt would make them feel more comfortable in waiting rooms. Ideas included more autism and mental health friendly waiting rooms, calming and relaxing posters or pictures, providing books or magazines, spacing out seating, and offer of smaller/quieter waiting rooms with fewer people. Participants also suggested that if there were delays with appointments that this was communicated at arrival, or on screens in the waiting room.
- Participants also suggested ensuring that the process for signing in at arrival was clearly indicated, ideally with options to do this at a reception desk or without having to speak to someone. Participants also suggested training for staff to know how to deal with people who have challenges with communication (for example, training on Picture Exchange Communication Systems (PECS) and tablet communication devices).
8.5 Women’s Reproductive Health Survey, 2023
8.5.1 Key findings and implications
- Findings from Surrey residents who took part in the national women’s reproductive health survey indicate that compared to nationally, there is a higher preference for Intrauterine systems of contraception and the Combined Pill; there is higher use of GP and Pharmacy services, and lower use of over-the-counter condoms and specialist services, and just under 90% of respondents got their preferred contraceptive choice, all of which indicates good access to appropriate services.
- A quarter of women changed their contraception method over the last year, slightly higher than nationally, with the top three reasons being effect on mood, impact on sex life and weight change.
The Women’s Reproductive Health Survey 2023 is a national online survey that collected data on the reproductive health experiences of women and people assigned female at birth in England [162]. This survey was delivered by the London School of Hygiene and Tropical Medicine and funded by the Department of Health and Social Care. Key results on contraception for Surrey responses, with comparisons to national data, are summarised below:
- There were a total of 59,332 responses to the Women’s Reproductive Health Survey 2023. Of these, 1,064 responses were from Surrey residents.
- 70% of responders from Surrey reported using some form of contraception within the last 12 months (compared to 69% nationally)
- Among Surrey responders that had used contraception, the preferred methods were:
- Male condom: 24.6%
- Intrauterine system (IUS): 17.6%
- Combined pill: 13.9%
Nationally, male condom and IUS were also the preferred methods of contraception (24.6% and 13.3% respectively) but progesterone-only pill was more common than the combined pill (11.0% vs. 10.5%).
- Of those that has used contraception, the service which provided the contraception was:
- General Practice (GP): 44.0%
- Condoms from over the counter: 17.4%
- Pharmacy: 13.2%
- Sexual Health clinic: 11.3%
GP was also the most common service provider nationally (41.3%) but nationally there was greater use of sexual health clinics (16.7%) compared to retail settings (15.7%) and pharmacies (11.3%).
- Just under 90% of responders in Surrey (88.4%) and nationally (86.6%) were able to get their preferred contraceptive method.
- Of responders who reported having used contraception in the last 12 months, around a quarter (25.1% in Surrey; 23.7% nationally) reported either stopping or changing contraception method. Of these, in Surrey the most common reasons for stopping/changing were:
- Effect on mood: 37.5%
- Impact on sex-life: 30.0%
- Weight change: 27.5%
- Changes in bleeding patterns: 26.3%
- Wanted to give body a break from contraception: 25.4%
- Wanted a non-hormonal method: 21.7%
- Wanted to get pregnant: 18.8%
A similar proportion of respondents reported stopping or changing contraceptive methods nationally, although reasons related to mood, sex-life, and weight change were slightly less common compared to Surrey.
9 Insight from professionals
9.1 Professionals’ survey
9.1.1 Key findings and implications
- The professionals’ survey provided helpful insights into some key themes experienced by professionals. Lack of time and limited availability of face-to-face appointments were common themes raised by both staff at GP surgeries and CNWL, indicating that staff and service capacity may be insufficient to meet demand.
- The majority of respondents were concerned about residents’ awareness of sexual health services in Surrey, as well as the availability of appointments with these services. Therefore, increasing awareness of the services on offer, referral pathways and overcoming the perceived lack of availability of appointments may be key.
- Several groups were identified as being at risk of experiencing inequalities in their sexual health. Over half of respondents highlighted the needs of: asylum seekers and refugees, young people aged under 25, people with a learning disability, people experiencing homelessness, and people from ethnically diverse backgrounds including the Gypsy, Roma, Traveller community. These findings support the engagement done as part of this JSNA, and reaching under-represented groups will be prioritised in engagement work going forward.
9.1.2 Overview and respondents
A survey was distributed to individuals working to support the sexual health needs of Surrey residents as part of their role. The aims of the survey were to understand the barriers and challenges that individuals experienced in providing sexual health services for Surrey residents, and for respondents to share what they felt the priority issues in sexual health are, as well which groups they perceived to be at higher risk of experiencing inequalities in their sexual health and wellbeing.
A total of 76 individuals completed the online professionals’ survey. The majority of respondents reported working at a GP surgery (n=24, 31.6%), followed by CNWL (n=22, 28.9%) and a pharmacy (n=7, 9.2%). Other respondents included those working for Surrey County Council, community healthcare and community mental health services, schools, colleges and universities, hospitals, family centres, SARCs, foster carers, and voluntary services. The findings provide useful insight into the challenges and priorities for professionals delivering services.
Detailed results are available on request: [email protected]
9.1.3 Barriers to providing sexual health and contraception services
Of the 24 respondents working at GP surgeries, 13 reported they experience challenges (54.2%) in delivering sexual health and contraception services. The most commonly selected challenges were lack of time to provide services (n=9, 69.2%), limited availability of face-to-face appointments (n=7, 53.8%), and a need to prioritise other services (n=6, 46.2%).
For staff working at CNWL, of the 19 respondents to this question, 13 reported they did experience challenges (68.4%) and 6 reported that they did not (31.6%). Of those who experienced challenges, the most commonly selected challenges were lack of time to provide services (n=7, 53.8%), a limited availability of face-to-face appointments (n=6, 46.2%), and challenges in residents being able to book appointments (n=5, 38.5%). Other challenges reported including inappropriate referrals, as well as other healthcare professionals missing opportunities to refer patients who may benefit, individuals accessing the services for non-sexual health issues, insufficient workforce, demand for services exceeding supply, and a challenge around ensuring that those individuals with highest need are reached by the service.
These challenges were mirrored for professionals working outside of primary care and CNWL, with lack of time and need to prioritise other services reported as common barriers to providing sexual health and contraception services.
9.1.4 Priority issues
Respondents were asked to identify their main concerns about the sexual health of Surrey residents and/or their service users. Of the 72 individuals who identified concerns they had, the most commonly reported concern was availability of appointments at GP surgeries (n=49, 68.1%). This may refer to demand for contraception via GP surgeries, or a more wider concern regarding availability of GP appointments for non-sexual health issues.
Other concerns raised were residents’ awareness of sexual health and contraception services in Surrey (n=46, 63.9%), and availability of appointments at specialist sexual health services in Surrey (n=39, 54.2%) (Figure 9.1).
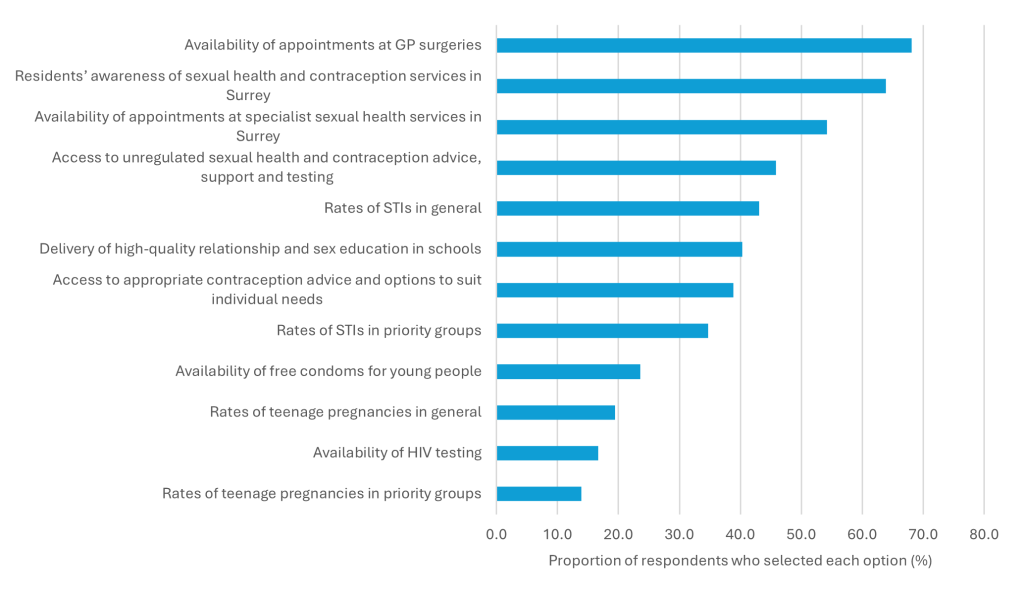
All respondents were asked which specific groups they felt are particularly vulnerable to experiencing inequalities in sexual health and contraception services. Of the 75 individuals who identified groups with greater sexual health and contraception needs, the most commonly selected groups were asylum seekers and refugees (n=48, 64.0%) and young people under 25 years old (n=48, 64.0%) (Figure 9.2). Other groups identified in addition to the options given were prisoners and women. The groups identified overlap significantly with the groups with greater sexual health need identified in section 3 of this report, and supports the engagement with individuals from some of these groups achieved in this piece of work, as well as supporting ongoing engagement with these groups for future work.
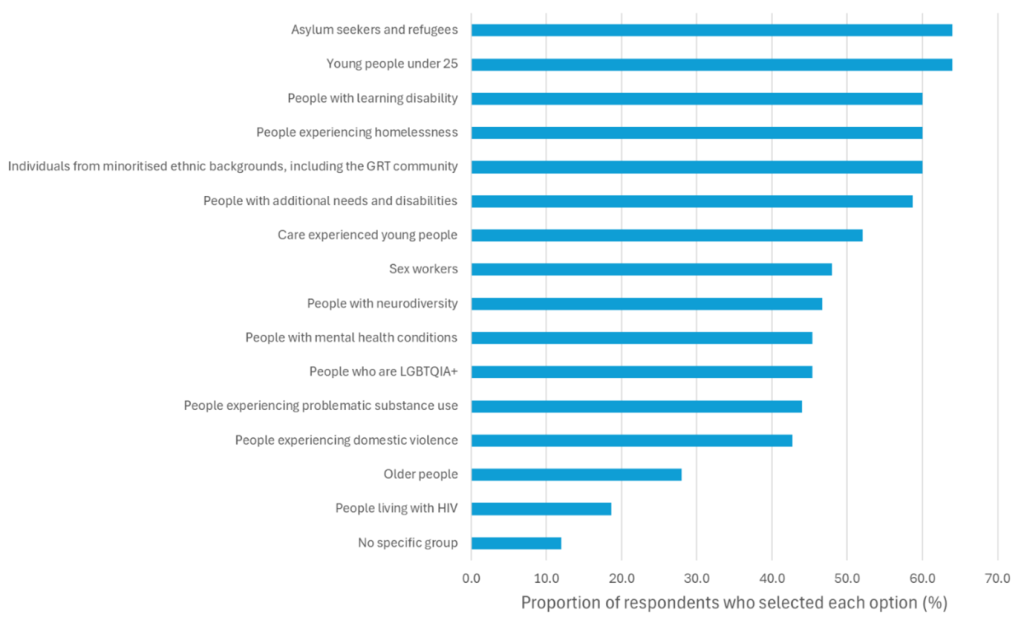
Abbreviations: GRT: Gypsy, Roma and Traveller; LGBTQIA+: Lesbian, gay, bisexual, transgender, queer, intersex, asexual and other identities
10 Conclusions
Achieving the vision of ‘positive sexual wellbeing for all’ requires a coordinated effort from all partners working to deliver high-quality sexual health services in Surrey, including commissioners and providers, as well as the residents of Surrey themselves. This JSNA has provided an evidence base of sexual health need within Surrey, drawing on the data and insight from both residents and professionals within Surrey.
Whilst rates of diagnosis of all STIs in Surrey remains below the national average [74], rates of chlamydia [75], gonorrhoea [76], syphilis [77] and HIV [78] are rising, and remain higher than pre-pandemic rates. Preventative sexual health care is already delivered across a range of settings in Surrey, including RSE in schools, the C-card scheme in community venues, the chlamydia screening programme, and PrEP prescribed by specialist sexual health services. However, given the rise in the number of STIs diagnosed, expansion of these preventative services is vital to meet this rising need. It is also important to ensure that where there have been successful reductions in some STIs, such as genital warts (83), the value and uptake of preventative measures, namely HPV vaccination, is not lost.
Rates of STI testing are also lower compared to 2019 [78]. This poses a threat to the sexual health and wellbeing of individuals in Surrey and healthcare services, due to pressures on sexual health services, the burden of complications of untreated STIs, as well as higher risk of onward transmission of STIs propagating the rising rates of STIs further. Surrey sexual health service offer both in person and online STI testing, however there is significant variation in the proportion of residents from each borough accessing online testing within Surrey, which may represent unmet need for residents in some areas. This may be due to lack of awareness of the online testing offered by the service, therefore promotion of this service is vital. There is also variation in rates of testing and diagnosis when looking at different demographic groups. Whilst more STIs are diagnosed amongst people of white ethnicities, some ethnically diverse groups have disproportionate higher diagnosis rates. Higher numbers of STI tests are undertaken by those living in the least deprived areas of Surrey, reflecting the higher proportion of people living in these areas, however, rates of testing are higher in those living in more deprived areas. The same pattern is seen when looking at diagnosis.
The proportion of people first diagnosed with HIV in the UK who receive a late diagnosis is significantly higher than the national average [79], with late diagnosis associated with a higher risk of complications to the individual, as well as increased potential for onward transmission prior to diagnosis. Nationally, late diagnosis is more common for over 50s, heterosexual men, and Asian and Black individuals. Late diagnosis indicates a significant need for earlier and more frequent testing, particularly in the aforementioned groups. This need can be met both by increasing testing at specialist sexual health services, as well as other settings, including emergency departments, GP surgeries and community settings with access to point of care HIV testing. Achieving this will only be possible by addressing the stigma that surrounds STIs, including HIV. This includes the stigma which contributes to individuals perceiving they are not at risk as well as the stigma-induced fear that is a deterrent to people accessing testing. Stigma amongst clinicians must also be addressed to ensure testing opportunities are not missed in individuals who are perceived not to fit a pre-conceived risk profile.
In Surrey, overall contraception outcomes, including abortion rates and teenage pregnancy, are relatively favourable compared to the national average [161]. However, there is some variation across districts and boroughs within the county reflecting some areas, particularly Runnymede, with a greater need for access to contraception services, education and advice.
Potential changes in preferences around contraception methods is another important consideration for both provision of services and ensuring appropriate education and understanding around contraceptive choices. This JSNA highlights the importance of flexible options in terms of where people seek contraception and offering multiple contraception methods. Gaining a better understanding of changes in contraception preferences will be important to ensure residents are provided with accurate information on the use of different methods, and that appropriate methods are available at contraception services in Surrey.
We recognise that individuals from some groups are more likely to have greater sexual health and contraception needs, or more unmet sexual health and contraception needs, including, but not limited to, young people, LGBTQIA+ individuals, those from ethnically diverse groups, asylum seekers and refugees, disabled people, people who are neurodivergent, and those experiencing problematic substance use. Understanding the specific needs of these groups, through ongoing focused engagement, is necessary to address inequalities in sexual health and wellbeing within Surrey.
It is also important to acknowledge some successes. Surrey County Council recognises the committed efforts that individuals providing sexual health and contraception services in Surrey make to improving the lives of residents, under significant time and resource pressures. Residents reported positive experiences of using services in Surrey, and individuals’ preferences for accessing services were well aligned with current service provision by CNWL, GPs and pharmacies. Some individuals identified that they would prefer to access services in the evenings and weekends, therefore this may present an opportunity for building awareness of the services available during these times, including online test kit ordering, and additional pharmacy-based services.
Misinformation regarding sexual health and contraception is also a rising threat, with many residents reporting use of the internet to access information and advice on sexual health. There is therefore a need for promotion of evidence-based information online, to ensure individuals are able to access reliable and safe advice when they need it.
Promotion of sexual health and wellbeing already has a strong strategic base in Surrey, including the Surrey Health and Wellbeing strategy, the HIV Action Plan and the Teenage Pregnancy Prevention Action Plan. The publication of Surrey’s Sexual Health Strategy will go one step further to strengthen Surrey County Council’s commitment to achieving positive sexual wellbeing for all.
11 Recommendations for action
Area 1: Prevention
| Recommendation | Rationale |
| 1.1: Support provision of high-quality Relationships and Sex Education across Surrey. | With rising rates of STIs and a potential plateau in teenage pregnancy rates, preventative measures should be strengthened, particularly in high-risk groups, which includes young people (section 2.2.3, 3.2, 4). Professionals identified the delivery of high-quality Relationships and Sex Education as a priority issue in Surrey (section 9.1.3). |
| 1.2: Maintain and increase commitment to Teenage Pregnancy Prevention Action Plan across system-partners. | There is a potential plateau in teenage pregnancy rates in Surrey, and there are disparities within Surrey at district and borough level (section 2.2.3, 4.2.2) |
| 1.3: Increase access to condoms, through increasing awareness and uptake of the C-card (condom distribution scheme), and through social media campaigns. | With rising rates of STIs and a potential plateau in teenage pregnancy rates, preventative measures should be strengthened, particularly in high risk groups, which includes young people (section 2.2.3, 3.2, 4). There is currently low activity at some C-card outlets (section 7.4). |
| 1.4: Increase coverage of the National Chlamydia Screening Programme, focusing on areas of lower coverage through campaigns and increased access. | In Surrey, the chlamydia detection rate in females aged 15 to 24 years is below the Public Health Outcome Framework target (section 4.1.3.2). The lowest coverage rates of chlamydia screening in females aged 15 to 24 were seen in Surrey Heath, Mole Valley, Waverley, Runnymede and Spelthorne, with rates lower in these areas compared with the national average (20.4%) (section 4.1.3.2). |
| 1.5: Improve HPV vaccination uptake in Surrey among eligible populations. | The proportion of 12- to 13-year-olds who have received at least one dose of the HPV vaccine in Surrey 2022/23 was 77.3% and has fallen since 2014/15. The coverage is consistently below the target of over 90% (section 4.1.7). |
| 1.6: Improve awareness and uptake of PrEP for HIV prevention in Surrey, particularly addressing inequalities in access to PrEP among people who are at high risk of HIV. | In Surrey in 2023 there were 107 newly diagnosed cases of HIV, which was 40.8% higher than in 2022 (section 4.1.6). Clinic attendances show there remains a gap in access and usage among certain groups, despite evidence that these groups could benefit substantially from PrEP. |
Area 2: Access to services and reducing barriers
| Recommendation | Rationale |
| 2.1: Reinforce the importance of continuing to offer choice in how and where to access sexual health and contraception services in Surrey, including testing in the community, e.g. testing in pharmacies | There is evidence of diverse needs for sexual health services (section 3, 4.1) and contraception services (section in Surrey (section 3, 4.2). There is also evidence of differences in where people access sexual health and contraception services (section 7) and a preference to maintain flexibility in how and where to access services (section 8). |
| 2.2: Improve awareness of the available services for sexual health and contraception in Surrey, including online out-of-hours services, and pharmacy services, especially among young people. | There is evidence of diverse needs for sexual health services (section 3, 4.1) and contraception services (section in Surrey (section 3, 4.2). There is also evidence of differences in where people access sexual health and contraception services (Section 7) and a preference to maintain flexibility in how and where to access services (Section 8). Some young people in the focus groups expressed a lack of awareness around existing services (Section 8.4.3.2). |
| 2.3: Ensure that inequalities are not exacerbated with a shift to increased use of online services in Surrey, and awareness that online services don’t suit everyone and of issues such as digital poverty. | There is evidence of increased use of online sexual health and contraception services (Section 8.1, 8.2, 8.4.3.3). |
| 2.4: Whilst the geographical proximity of services across the Surrey border may be more convenient for residents in some districts and boroughs of Surrey, investigation into the reasons for low uptake of online testing in some boroughs (particularly Spelthorne) is required, and increased promotion of services in those areas. | Some residents in Surrey prefer to use specialist sexual health services that are out of area, and the survey highlighted that geographical proximity of services is a driver of this (section 8.1, 8.2, 8.4). This was mirrored in the data showing higher use of out of area services by residents in Elmbridge, Epsom and Ewell and Spelthorne, which are on the borders of Surrey (section 7.2.5). Although in-person clinics in different boroughs may be more convenient for residents in these areas, access to online services delivered by CNWL should be a convenient service for all Surrey residents. However, online test orders were lowest in Spelthorne (section 7.2.2). |
| 2.5: Take actions to increase the return rate of online tests that are sent out by CNWL, particularly in areas with low return rates of tests ordered online. | The return rate of online STI test kits ordered by residents in Spelthorne, Tandridge, Epsom and Ewell and Guildford was under 75% (section 7.2.2), which may represent a missed opportunity for testing and inefficient use of resources. |
| 2.6: Explore and address issues identified by some young people as barriers to accessing services, including online testing. | Young people in focus groups raised concerns about visibility of services and concerns about home testing (section 8.4) |
| 2.7: Improve the accessibility of in-person specialist sexual health services for individuals with additional needs and disabled people, and people who are neurodivergent. | Individuals in the focus group raised the issue that attending sexual health clinics in-person can be challenging due to unfamiliarity and being uncertain as to what to expect, particularly for people who are neurodivergent (section 8.4). They suggested a virtual tour of the clinics may be helpful. |
| 2.8. Explore options to increase access to HIV testing in the community, particularly for individuals more likely to receive a late diagnosis (older adults, heterosexual men, and Asian and Black individuals). | HIV testing rates in Surrey are lower than the England average, and national data indicates a high proportion of older adults, heterosexual men, and Asian and Black individuals who are diagnosed with HIV receive a late diagnosis (section 4.1.6). |
| 2.9 Improving access and uptake of LARC, particularly in areas with a lower rate of prescribed LARC | Rates of total prescribed LARC in Surrey are higher than the national average although there is evidence that the rate varies greatly across Surrey. The lowest rates of LARC in Surrey is in Runnymede at 28.8 per 100,000 population (section 7.5.1). |
| 2.10 Promote awareness of the expansion of access to free emergency contraception for over 25 year olds in key neighbourhoods and groups, and monitor uptake | Access to free emergency contraception will be made available to all women from Pharmacies later in 2025, as part of a national change to reduce inequalities in access in deprived areas and free up GP appointments |
| 2.11 Take action to address stigma surrounding STIs, particularly HIV, to prevent stigma being a barrier to individuals accessing the services they need. | Stigma around sexual health was identified as a key theme in the literature for several groups, including ethnically diverse groups, asylum seekers and refugees, people with LD, and people living with HIV (Section 3). Focus group participants reported a preference for services that were discrete due to potential embarrassment around accessing sexual health clinics (section 8.4.3.4). |
Area 3: Access to Information
| Recommendation | Rationale |
| 3.1: Promote high-quality evidence-based sexual health and contraception information for residents online by using targeted methods to reach priority audiences and individuals living in certain geographies, and raise awareness of the misinformation that exists. | Surrey residents highlighted their preference to use the internet as a source of information across our surveys and focus groups, and the challenge of finding reputable information online and avoiding misinformation was raised by the focus groups (section 8.1, 8.2, 8.3, 8.4). Professionals also identified challenges with residents accessing reputable information regarding sexual health and contraception as a priority issue (section 9.1.3). |
Area 4: Insight and inclusion
| Recommendation | Rationale |
| 4.1: Undertake further insight and engagement work to better understand the needs of residents who were underrepresented in this JSNA. This includes: Asylum seekers refugees and vulnerable migrants Individuals with additional needs and disabled people, including learning disability, neurodiversity and mental illness Individuals experiencing homelessness People involved in prostitution and sex work Individuals from ethnically diverse groups, including people from GRT groups Transgender individuals Individuals involved in problematic substance use People who have experienced domestic abuse. |
There is evidence that individuals from these groups are at risk of experiencing inequalities in their sexual health (section 3). We had a low response rate to our residents’ survey from individuals from these groups (section 8), and the individuals who completed the professionals’ survey identified these groups as being at risk of experiencing inequalities in sexual health and contraception services (section 9.1.3). |
| 4.2 Undertake further insight and engagement work to better understand the needs of young people in Surrey, recognising that this is a diverse group and some young people may have higher need, such as care experienced young people. | There is evidence that young people and care experienced young people have higher sexual health needs (Section 3.2, 3.3). We had a low response rate to our residents’ survey from young people (Section 8), and the individuals who completed the professionals’ survey identified young people as being at risk of experiencing inequalities in sexual health and contraception services (section 9.1.3). |
| 4.3: Continue monitoring of trends in sexual health service use and diagnosis rates of STIs. | There is evidence of an increase in service use and diagnosis rates of STIs post-pandemic, and it is unclear at this stage whether this rise will plateau (section 4.1 and 7.2). |
| 4.4: Continue monitoring contraception method preference and use, and whether changes lead to changes in outcomes such as teenage pregnancy rates and abortions. | There is emerging evidence that women are moving away from use of short-acting hormonal contraception (section 7.2.4.2, 8.2, 8.5). |
Area 5: Working as a whole system
| Recommendation | Rationale |
| 5.1 Ensure a systems wide approach to delivery of sexual health and contraception services in Surrey, through the development of a sexual health strategy. | There is evidence of differences in where people access sexual health and contraception services (section 7) and a preference to maintain flexibility in how and where to access services (section 8). |
| 5.2 Ensure there are clear referral pathways and awareness among professionals across the sexual health system. | Ensuring appropriate referral to other services was raised by professionals as a potential barrier to providing sexual health and contraception services in Surrey (section 9.1.2). |
| 5.3 Ensure there are ongoing collaborative approaches to sharing of information, involving and hearing resident voices, especially among priority groups, and monitoring of outcomes. | There is evidence of differences in where people access sexual health and contraception services (section 7) and a preference to maintain flexibility in how and where to access services (section 8) |
Glossary
| ADHD | Attention-Deficit/Hyperactivity Disorder |
| ASD | Autism Spectrum Disorder |
| BASHH | British Association for Sexual Health and HIV |
| BHIVA | The British HIV Association |
| BIA | British Infection Association |
| CD4 | Cluster of differentiation 4 cells (type of immune cell) |
| CDS | Condom distribution scheme |
| CNWL | Central North West London |
| DHSC | Department of Health and Social Care |
| FGM | Female genital mutilation |
| FSRH | The Faculty of Sexual and Reproductive Healthcare |
| GBMSM | gay, bisexual and other men who have sex with men |
| GP | General practitioner/practice |
| GRT | Gypsy, Roma and Traveller |
| GUMCAD HCID | Genito-urinary medicine clinic activity dataset High consequence infectious disease |
| HIV | Human Immunodeficiency Virus |
| HMP | His Majesty’s prison |
| HPV | Human papillomavirus |
| HSV | Herpes simplex virus |
| ICS | Integrated care system |
| IMD | Index of multiple deprivation |
| JSNA | Joint Strategic Needs Assessment |
| LARC | Long-acting reversible contraception |
| LGBTQIA+ | Lesbian, gay, bisexual, transgender, queer, intersex, asexual and other identities |
| LGV | Lymphogranuloma venereum |
| LPC | Local pharmaceutical committee |
| LSOA | Lower Layer Super Output Areas |
| MARS | Mycoplasma genitalium Antimicrobial Resistance Surveillance |
| MSM | Men who have sex with men |
| MSOA | Middle super output area |
| NCSP | National Chlamydia Screening Programme |
| NHS | National Health Service |
| NICE | National Institute for Health and Care Excellence |
| PECS PPE | Picture Exchange Communication Systems Personal protective equipment |
| PHOF | Public health outcomes framework |
| PID | Pelvic inflammatory disease |
| PrEP | Pre-exposure prophylaxis |
| RCEM RCOG | Royal College of Emergency Medicine Royal College of Obstetricians & Gynaecologists |
| RSE | Relationships and sex education |
| SABP | Surrey and Borders Partnership |
| SARC | Sexual assault referral centre |
| SHOG | Sexual health outreach group |
| SMI | Severe mental illness |
| SSHA | Society of Sexual Health Advisors |
| STI | Sexually transmitted infection |
| UKHSA | UK Health Security Agency |
| WHO | World Health Organisation |
| XDR | Extensively drug resistant |
| YOI | Young offender institution |
Appendix
Appendix 1 – Methods
Residents’ questionnaire
- A questionnaire was distributed to residents exploring access to sexual health and contraception services, barriers to accessing services, preferences for accessing services, and where residents go for information on sexual health, contraception and wellbeing. This questionnaire was distributed to residents via our key partners, as well promoted using paid advertisements on Instagram and Facebook, and shared organically on X using Healthy Surrey social media. The questionnaire was available on the Surrey Says survey platform, with accessible versions including screen reader accessible, large print and easy read available, as well as an option to request a paper copy. The survey ran from 26th November 2024 to 29th December 2025. Our strategy to share this survey was focused on reaching inclusion health groups and groups with greater sexual health needs, therefore the respondents of this survey may not be representative of the Surrey population.
- A second questionnaire for residents was distributed to the Resident Intelligence Unit’s Resident Panel. The Resident Panel is a cohort of 3,000 Surrey residents who are recruited to be representative of the wider Surrey population. To ensure the distribution of responses is as representative as possible of the Surrey population, results are weighted by age and sex, based on the results of the 2021 census. This survey ran from 6th January 2025 to 20th January 2025.
Focus groups
- Focus groups were conducted to explore the perceptions, attitudes, and experiences of young people in Surrey regarding sexual health and contraception. The focus group aimed to identify knowledge of existing services for sexual health and contraception in Surrey, where young people get information about sexual health and contraception, and potential barriers to accessing sexual health services. For all focus groups, participants were encouraged to share experiences and perspectives openly but without needing to share personal experiences. Participants were assured that all answers would be anonymous. Focus groups were conducted in the following settings:
- Young people aged 16-25 years in Surrey participants were recruited through Surrey Youth Voice, a partnership with young people and the User Voice and Participation Team in Surrey County Council [163]. The session was facilitated by members of the sexual health team from Surrey County Council and overseen by a Senior Participation Officer in the User Voice and Participation Team to create a safe and open environment for discussion.
- Young people aged 13-23 years attending a Twister youth group were recruited by the Twister youth worker [164]. The session was facilitated by members of the sexual health team from Surrey County Council and overseen by the youth worker to create a safe and open environment for discussion.
Professionals’ questionnaire
- A professionals’ questionnaire was distributed to stakeholders working in sexual health services or working in a role where they offer sexual health advice and support to Surrey residents. This could range from clinical staff providing a sexual health service, to others who provide formal or informal advice and support on sexual health for their service users, for example in a youth club. These questionnaires explored services (including advice and support) offered by the respondent, challenges they experience in providing their service, and their views regarding the key priorities for improving sexual health of Surrey residents. The questionnaire was available on the Surrey Says survey platform, with a screen reader accessible version available. The survey ran from 26th November 2024 to 29th December 2025. The key partners we aimed to engage with were:
- Anyone who provides sexual health or contraception advice and/or support to Surrey residents
- GPs, practice nurses, and other GP surgery staff
- Pharmacists and other pharmacy staff
- Healthcare professionals working in specialist sexual health services
- School nurses, healthcare workers at colleges and universities
- Midwives, health visitors
- Voluntary services
- Youth workers
Quantitative data
Quantitative data was collated and analysed from the Department of Health and Social Care (via Fingertips), service providers in Surrey (including data from the specialist sexual health service in Surrey and out of area services), and PharmOutcomes. Data suppression rules were applied to data from the specialist sexual health service and other clinical services, in keeping with NHS England guidance for Hospital Episode Statistics [165], with counts rounded to protect patient anonymity. Demographic groupings were chosen pragmatically due to the variation in the level of detail in which demographic characteristics were coded between data sets, as well as due to small numbers of individuals in some demographic groups. Therefore, it is important to acknowledge that within demographic groupings, e.g. for ethnicity, sexual orientation and gender identity, there is diversity within groups that was unable to be expressed separately.
Acknowledgements
Sexual Health JSNA Chapter Delivery Group
Lead Authors: Dr David Mesher and Dr Grace Monori, Public Health Registrars, Public Health and Communities, Surrey County Council
Project Manager: Dr Louis Hall, Public Health Consultant, Intelligence and Insight, Public Health and Communities, Surrey County Council
Project Manager: Julia Groom, Public Health Consultant, Sexual Health, Public Health and Communities, Surrey County Council
Project Manager: Rachael Taylor, Senior Public Health Lead, Sexual Health, Public Health and Communities, Surrey County Council
Programme Manager: Rebecca Matthews, JSNA Programme Manager, Public Health and Communities, Surrey County Council
Contributing Author: Kate Crockatt, Public Health Lead, Sexual Health, Public Health and Communities, Surrey County Council
Contributing Author: Agnieszka Rembialkowska, Public Health Sexual Health Development Worker, Public Health and Communities, Surrey County Council
Contributing author: Amy Bennett, Consultant GUM/HIV, Surrey Integrated Sexual Health & HIV Services, Central and North West London NHS Foundation Trust
Contributing author: Denise Rayner, Service Manager, Surrey Integrated Sexual Health & HIV Services, Central and North West London NHS Foundation Trust
Contributing author: Olga Charlestan, Health Improvement Practitioner Apprentice, Public Health and Communities, Surrey County Council
Data Analysts: Charlene Carayol, Lynne Sawyer, Neil Molkenthin, Conor Woolley and Kate Harris; Public Health Analytics Team, Public Health and Communities, Surrey County Council
Resident Intelligence Unit: Louise Doherty-Harwood, Research Project Manager, Surrey County Council; Abigail Linyard-Tough, Strategic Lead, Research and Resident Insight, Surrey County Council
Equality, Diversity and Inclusion Team: Nikki Parkhill and Ioni Sullivan, Equality Diversity and Inclusion, Surrey County Council
Information and Engagement Team: Sarah Linington, Engagement and Partnership Officer, Information and Engagement, Surrey County Council.
Surrey Youth Voice: Gemma Neathey, Senior Participation Officer, User Voice and Participation, Quality Practice, Relationships and Support, Surrey County Council.
With thanks to the young people from Surrey Youth Voice and Twister who shared their views in focus groups, as well as all of the Surrey residents and stakeholders who completed the surveys. We would also like to acknowledge the contributions of members of the Sexual Health JSNA Working Group, and other stakeholders who supported this piece of work.
Sponsor
With special thanks to our sponsor, Dr Russell Hills, GP and Executive Clinical Director, Surrey Downs Health and Care Partnership.
References
1. World Health Organisation. Sexual Health: Definitions [Internet]. 2006 [cited 2025 Mar 10]. Available from: Sexual health
2. World Health Organisation. Sexually transmitted infections (STIs) [Internet]. 2025 [cited 2025 Mar 11]. Available from: Sexually transmitted infections (STIs)
3. Department of Health and Social Care. Fingertips [Internet]. 2025 [cited 2025 Mar 25]. Available from: Fingertips | Department of Health and Social Care
4. Department of Health and Social Care. Guidance: A Framework for Sexual Health Improvement in England [Internet]. 2013 [cited 2025 Mar 13]. Available from: A Framework for Sexual Health Improvement in England – GOV.UK
5. The Association of Directors of Public Health. Policy Position: Sexual Health [Internet]. 2023 [cited 2025 Mar 13]. Available from: Sexual-Health-Policy-Position-Statement-2023-Amended-Oct-2024.pdf
6. Local Government Association. A blueprint for the future: Sexual and reproductive health and HIV services in England [Internet]. 2024 [cited 2025 Mar 13]. Available from: A blueprint for the future: Sexual and reproductive health and HIV services in England | Local Government Association
7. Pulford C, Bell E, Fagan L, Jajja A, Buitendam E, Folkard K, et al. STI Prioritisation Framework, 2024. October 2024. UKHSA, London.
8. Public Health England. Variation in outcomes in sexual and reproductive health in England: A toolkit to explore inequalities at a local level [Internet]. 2021 [cited 2025 Feb 12]. Available from: Variation in outcomes in sexual and reproductive health in England 2021
9. Department of Health and Social Care. Towards Zero – An action plan towards ending HIV transmission, AIDS and HIV-related deaths in England – 2022 to 2025 [Internet]. 2021 [cited 2025 Mar 13]. Available from:Towards Zero – An action plan towards ending HIV transmission, AIDS and HIV-related deaths in England – 2022 to 2025 – GOV.UK
10. Department of Health and Social Care. Women’s Health Strategy for England [Internet]. 2022 [cited 2025 Feb 12]. Available from: Women’s Health Strategy for England – GOV.UK
11. Healthy Surrey. Health and wellbeing strategy [Internet]. 2022 [cited 2025 Mar 11]. Available from: Health and wellbeing strategy | Healthy Surrey
12. Department of Health and Social Care. Sexual and Reproductive Health Profiles – Under 18s conception rate [Internet]. [cited 2025 Feb 20]. Available from: Fingertips | Department of Health and Social Care
13. Surrey County Council. Population, A quick guide to content [Internet]. 2024 [cited 2024 Oct 22]. Available from: Population | Surrey-i
14. Surrey County Council. The 21 Health and Wellbeing Key Neighbourhoods in Surrey [Internet]. 2025 [cited 2025 Jan 30]. Available from: Key Neighbourhoods | Surrey-i
15. Solomon D, Gibbs J, Burns F, Mohammed H, Migchelsen SJ, Sabin CA. Inequalities in sexual and reproductive outcomes among women aged 16–24 in England (2012–2019). J Epidemiol Community Health (1978). 2024 Jul;78(7):451–7.
16. UK Parliament. The prevalence of sexually transmitted infections in young people and other high risk groups [Internet]. 2024 [cited 2025 Jan 30]. Available from: The prevalence of sexually transmitted infections in young people and other high risk groups – Women and Equalities Committee
17. Wellings K, Jones KG, Mercer CH, Tanton C, Clifton S, Datta J, et al. The prevalence of unplanned pregnancy and associated factors in Britain: findings from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). The Lancet. 2013 Nov;382(9907):1807–16.
18. McKenna S, O’Reilly D, Maguire A. Childhood contact with social services and risk of suicide or sudden death in young adulthood: identifying hidden risk in a population-wide cohort study. J Epidemiol Community Health (1978). 2024 Jan;78(1):47–53.
19. Murray ET, Lacey R, Maughan B, Sacker A. Non-parental care in childhood and health up to 30 years later: ONS Longitudinal Study 1971–2011. Eur J Public Health. 2020 Dec 11;30(6):1121–7.
20. Nixon C, Elliott L, Henderson M. Providing sex and relationships education for looked-after children: a qualitative exploration of how personal and institutional factors promote or limit the experience of role ambiguity, conflict and overload among caregivers. BMJ Open. 2019 Apr 11;9(4):e025075.
21. Surrey County Council. Sexual orientation from the 2021 Census [Internet]. 2024 [cited 2024 Oct 22]. Available from: 2021 Census: Sexual Orientation | Surrey-i
22. UK Health Security Agency. Sexually transmitted infections and screening for chlamydia in England: 2023 report [Internet]. 2024 [cited 2025 Jan 27]. Available from: Sexually transmitted infections (STIs): annual data – GOV.UK
23. Surrey County Council. Ethnic Group from the 2021 Census [Internet]. 2024 [cited 2024 Oct 22]. Available from: Census 2021: Ethnic Group | Surrey-i
24. Bardsley M, Wayal S, Blomquist P, Mohammed H, Mercer CH, Hughes G. Improving our understanding of the disproportionate incidence of STIs in heterosexual-identifying people of black Caribbean heritage: findings from a longitudinal study of sexual health clinic attendees in England. Sex Transm Infect. 2022 Feb;98(1):23–31.
25. FUREGATO M, CHEN Y, MOHAMMED H, MERCER CH, SAVAGE EJ, HUGHES G. Examining the role of socioeconomic deprivation in ethnic differences in sexually transmitted infection diagnosis rates in England: evidence from surveillance data. Epidemiol Infect. 2016 Nov 11;144(15):3253–62.
26. Wayal S, Hughes G, Sonnenberg P, Mohammed H, Copas AJ, Gerressu M, et al. Ethnic variations in sexual behaviours and sexual health markers: findings from the third British National Survey of Sexual Attitudes and Lifestyles (Natsal-3). Lancet Public Health. 2017 Oct;2(10):e458–72.
27. Lime Culture. Working with victims and survivors from Gypsy, Roma and Traveller Communities [Internet]. 2022 [cited 2025 Mar 14]. Available from: Working with victims and survivors from Gypsy, Roma and Traveller Communities
28. Friends F& T. Test Treat and Trace for Gypsy Roma and Traveller communities. 2023 [cited 2025 Mar 14]. Available from: Test-Treat-and-Trace-for-Gypsy-Roma-and-Traveller-communities-updated-document-final_SH.pdf
29. Price MJ, Ades A, Soldan K, Welton NJ, Macleod J, Simms I, et al. The natural history of Chlamydia trachomatis infection in women: a multi-parameter evidence synthesis. Health Technol Assess (Rockv). 2016 Mar;20(22):1–250.
30. Surrey County Council. Gender identity from the 2021 Census [Internet]. 2024 [cited 2024 Oct 22]. Available from: 2021 Census: Gender Identity | Surrey-i
31. Hickson F, Appenroth M, Koppe U, Schmidt AJ, Reid D, Weatherburn P. Sexual and Mental Health Inequalities across Gender Identity and Sex-Assigned-at-Birth among Men-Who-Have-Sex-with-Men in Europe: Findings from EMIS-2017. Int J Environ Res Public Health. 2020 Oct 10;17(20):7379.
32. Closson K, Boyce SC, Johns N, Inwards-Breland DJ, Thomas EE, Raj A. Physical, Sexual, and Intimate Partner Violence Among Transgender and Gender-Diverse Individuals. JAMA Netw Open. 2024 Jun 25;7(6):e2419137.
33. Tableau Public. South East Migration Schemes Data Explorer [Internet]. 2024 [cited 2024 Oct 22]. Available from: South East Migration Schemes Data Explorer
34. Home Office and Ministry of Housing C and LG. Regional and local authority data on immigration groups [Internet]. 2024 [cited 2025 Feb 12]. Available from: Regional and local authority data on immigration groups – GOV.UK
35. Office for Health Improvement and Disparities. Women’s health: migrant health guide [Internet]. 2021 [cited 2025 Feb 12]. Available from: Women’s health: migrant health guide – GOV.UK
36. Office for Health Improvement and Disparities. Sexually transmitted infections (STIs): migrant health guide [Internet]. 2021 [cited 2025 Feb 12]. Available from: Sexually transmitted infections (STIs): migrant health guide – GOV.UK
37. Aibangbee M, Micheal S, Mapedzahama V, Liamputtong P, Pithavadian R, Hossain Z, et al. Migrant and Refugee Youth’s Sexual and Reproductive Health and Rights: A Scoping Review to Inform Policies and Programs. Int J Public Health. 2023 Jun 5;68.
38. Surrey County Council. JSNA Housing and Related Support [Internet]. 2024 [cited 2025 Feb 20]. Available from: JSNA Housing and Related Support | Surrey-i
39. Gorton S. Homeless young women and pregnancy: Pregnancy in hostels for single homeless people [Internet]. 2000 [cited 2025 Feb 12]. Available from: Homeless young women and pregnancy: Pregnancy in hostels for single homeless people | HomelessHub
40. The Department of Health. A Framework for Sexual Health Improvement in England [Internet]. 2013 [cited 2025 Feb 12]. Available from: A Framework for Sexual Health Improvement in England
41. Paisi M, March-McDonald J, Burns L, Snelgrove-Clarke E, Withers L, Shawe J. Perceived barriers and facilitators to accessing and utilising sexual and reproductive healthcare for people who experience homelessness: a systematic review. BMJ Sex Reprod Health. 2021 Jul;47(3):211–20.
42. McGregor F, Paisi M, Robinson A, Shawe J. Improving the sexual health of young people experiencing homelessness. Br J Community Nurs. 2021 Nov 2;26(11):560–6.
43. Shah P, Koch T, Singh S. The attitudes of homeless women in London towards contraception. Prim Health Care Res Dev. 2019 Sep 12;20:e131.
44. Streetlight UK. Sussex and Surrey Outreach Team. 2025. [cited 2025 Sept 09] Available from: Sussex & Surrey – StreetlightUK
45. Mc Grath-Lone L, Marsh K, Hughes G, Ward H. The sexual health of female sex workers compared with other women in England: analysis of cross-sectional data from genitourinary medicine clinics. Sex Transm Infect. 2014 Jun;90(4):344–50.
46. Mc Grath-Lone L, Marsh K, Hughes G, Ward H. The sexual health of male sex workers in England: analysis of cross-sectional data from genitourinary medicine clinics: Table 1. Sex Transm Infect. 2014 Feb;90(1):38–40.
47. Surrey County Council. Disability from the 2021 Census [Internet]. 2024 [cited 2024 Oct 22]. Available from: 2021 Census: Disability | Surrey-i
48. Mailhot Amborski A, Bussières EL, Vaillancourt-Morel MP, Joyal CC. Sexual Violence Against Persons With Disabilities: A Meta-Analysis. Trauma Violence Abuse. 2022 Oct 4;23(4):1330–43.
49. Parekh T, Gimm G, Kitsantas P. Sexually Transmitted Infections in Women of Reproductive Age by Disability Type. Am J Prev Med. 2023 Mar;64(3):393–404.
50. Surrey County Council. Joint Strategic Needs Assessment – People with learning disabilities [Internet]. 2023 [cited 2025 Jan 30]. Available from: People with learning disabilities | Surrey-i
51. Mencap. Sexuality – research and statistics [Internet]. 2025 [cited 2025 Jan 30]. Available from: Learning Disability Sex and Relationships Research | Mencap
52. Young S, Cocallis K. A Systematic Review of the Relationship Between Neurodiversity and Psychosexual Functioning in Individuals with Autism Spectrum Disorder (ASD) or Attention-Deficit/Hyperactivity Disorder (ADHD). Neuropsychiatr Dis Treat. 2023 Jun;Volume 19:1379–95.
53. Babalola T, Sanguedolce G, Dipper L, Botting N. Barriers and Facilitators of Healthcare Access for Autistic Children in the UK: a Systematic Review. Rev J Autism Dev Disord. 2024 Jan 5;
54. Surrey County Council. Joint Strategic Needs Assessment: Emotional and Mental Wellbeing in Surrey Adults [Internet]. 2023 [cited 2025 Feb 12]. Available from: Emotional and Mental Wellbeing in Surrey Adults | Surrey-i
55. Hope H, Pierce M, Johnstone ED, Myers J, Abel KM. The sexual and reproductive health of women with mental illness: a primary care registry study. Arch Womens Ment Health. 2022 Jun 2;25(3):585–93.
56. Kaltenthaler E, Pandor A, Wong R. The effectiveness of sexual health interventions for people with severe mental illness: a systematic review. Health Technol Assess. 2014 Jan;18(1):1-74.
57. Hughes E, Mitchell N, Gascoyne S, Moe-Byrne T, Edmondson A, Coleman E, et al. The RESPECT study: a feasibility randomised controlled trial of a sexual health promotion intervention for people with serious mental illness in community mental health services in the UK. BMC Public Health. 2020 Dec 17;20(1):1736.
58. Shapiro K, Ray S. Sexual Health for People Living with HIV. Reprod Health Matters. 2007 Jan 23;15(sup29):67–92.
59. Surrey County Council. Substance Misuse Joint Strategic Needs Assessment [Internet]. 2024 [cited 2025 Feb 12]. Available from: JSNA Substance Misuse | Surrey-i
60. Office for Health Improvement and Disparities. Alcohol dependence prevalence in England [Internet]. 2024 [cited 2025 Feb 12]. Available from: Alcohol dependence prevalence in England – GOV.UK
61. Office for Health Improvement and Disparities. Opiate and crack cocaine use: prevalence estimates [Internet]. 2023 [cited 2025 Feb 12]. Available from: Opiate and crack cocaine use: prevalence estimates – GOV.UK
62. Paquette R, Tanton C, Burns F, Prah P, Shahmanesh M, Field N, et al. Illicit drug use and its association with key sexual risk behaviours and outcomes: Findings from Britain’s third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). PLoS One. 2017 May 18;12(5):e0177922.
63. Li J, McDaid LM. Alcohol and drug use during unprotected anal intercourse among gay and bisexual men in Scotland: what are the implications for HIV prevention? Sex Transm Infect. 2014 Mar;90(2):125–32.
64. Khadr SN, Jones KG, Mann S, Hale DR, Johnson AM, Viner RM, et al. Investigating the relationship between substance use and sexual behaviour in young people in Britain: findings from a national probability survey. BMJ Open. 2016 Jun 30;6(6):e011961.
65. Surrey County Council. Surrey Substance Misuse Strategy, Drugs Section [Internet]. 2019 [cited 2025 Jan 27]. Surrey Combating Drugs Partnership | Healthy Surrey
66. Surrey County Council. Surrey Domestic Abuse Needs Assessment 2023 [Internet]. 2023 [cited 2025 Feb 12]. Available from: High level overview of domestic abuse in Surrey | Healthy Surrey
67. National Institute for Health and Care Research. The ADViSE pilot: Using sexual health services to support people who have experiences domestic violence and abuse [Internet]. 2019 [cited 2025 Feb 12]. Available from: The ADViSE pilot: Using sexual health services to support people who have experienced domestic violence and abuse – ARC West
68. Jackson J, Lewis N V, Feder GS, Whiting P, Jones T, Macleod J, et al. Exposure to domestic violence and abuse and consultations for emergency contraception: nested case-control study in a UK primary care dataset. British Journal of General Practice. 2019 Mar;69(680):e199–207.
69. UK Health Security Agency. Positive Voices 2022: survey report [Internet]. 2024 [cited 2025 Jul 21]. Available from: Positive Voices 2022: survey report – GOV.UK
70. Ministry of Justice. Prison population: monthly prison figures 2024 [Internet]. 2024 [cited 2025 Feb 12]. Available from: Prison population: monthly prison figures 2024 – GOV.UK
71. Enayat Q, Yorke K, Mullen D, Talebi A, Willner S, Dunn J, et al. Trends in sexually transmitted infection diagnoses among people in prison in England, 2018-2023: analysis of surveillance and pilot seroprevalence data. International Journal of Prison Health. 2025 Apr 29;21(2):176-186
72. Gohil J, Ross S, Prime K, Clarke E. BASHH standards for the management of sexual health in UK prisons. Int J STD AIDS. 2024 Oct 20;35(12):997–8.
73. Surrey County Council. HNA Prisons [Internet]. 2021 [cited 2025 Feb 12]. Available from: HNA Prisons | Surrey-i
74. Department of Health and Social Care. Sexual and Reproductive Health Profiles – All new STI diagnoses rate per 100,000 [Internet]. 2025 [cited 2025 Jan 28]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
75. Department of Health and Social Care. Sexual and Reproductive Health Profiles – Chlamydia proportion of females aged 15 to 24 screened [Internet]. 2025 [cited 2025 Jan 28]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
76. Department of Health and Social Care. Sexual and Reproductive Health Profiles – Gonorrhoea diagnostic rate per 100,000 [Internet]. 2025 [cited 2025 Jan 27]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
77. Department of Health and Social Care. Sexual and Reproductive Health Profiles – Syphilis diagnostic rate per 100,000 [Internet]. 2025 [cited 2025 Jan 27]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
78. Department of Health and Social Care. Sexual and Reproductive Health Profiles – New HIV diagnosis rate per 100,000 [Internet]. 2025 [cited 2025 Jan 30]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
79. Department of Health and Social Care. Sexual and Reproductive Health Profiles – STI testing rate (exclude chlamydia aged under 25) per 100,000 [Internet]. 2025 [cited 2025 Jan 28]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
80. Department of Health and Social Care. Sexual and Reproductive Health Profiles – HIV late diagnosis in people first diagnosed with HIV in the UK [Internet]. 2025 [cited 2025 Jan 30]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
81. Department of Health and Social Care. Sexual and Reproductive Health Profiles – Chlamydia detection rate per 100,000 aged 15 to 24 (Female) [Internet]. 2025 [cited 2025 Jan 28]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
82. WHO. Alarming decline in adolescent condom use, increased risk of sexually transmitted infections and unintended pregnancies, reveals new WHO report [Internet]. 2024 [cited 2025 Mar 13]. Available from: Alarming decline in adolescent condom use, increased risk of sexually transmitted infections and unintended pregnancies, reveals new WHO report
83. Alsing K, Sejersen T, Jemec G. Geosocial Dating Applications Mirror the Increase in Sexually Transmitted Diseases. Acta Dermato Venereologica. 2021;101(1):adv00378.
84. Department of Health and Social Care. Sexual and Reproductive Health Profiles – Genital warts diagnostic rate per 100,000 [Internet]. 2025 [cited 2025 Jan 27]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
85. Department of Health and Social Care. Sexual and Reproductive Health Profiles – Population vaccination coverage: HPV vaccination coverage for one dose (12 to 13 year old) [Internet]. 2025 [cited 2025 Jan 27]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
86. Department of Health and Social Care. Sexual and Reproductive Health Profiles – Violent crime – sexual offences per 1,000 population [Internet]. 2025 [cited 2025 Jan 27]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
87. NHS England. Female Genital Mutilation, Annual Report – April 2023 to March 2024 [Internet]. 2024 [cited 2025 Jan 27]. Available from: Female Genital Mutilation, Annual Report – April 2023 to March 2024 – NHS England Digital
88. Department of Health and Social Care. Sexual and Reproductive Health Profiles – STI testing positivity (excluding chlamydia aged under 25). 2025.
89. Department of Health and Social Care. Sexual and Reproductive Health Profiles – New STI diagnoses (excluding chlamydia aged under 25) per 100,000 [Internet]. 2025 [cited 2025 Jan 28]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
90. UK Health Security Agency. Chlamydia: surveillance, data, screening and management [Internet]. 2022 [cited 2025 Jan 28]. Available from: Chlamydia: surveillance, data, screening and management – GOV.UK
91. Public Health England. Changes to the National Chlamydia Screening Programme (NCSP) [Internet]. 2021 [cited 2025 Jan 28]. Available from: Changes to the National Chlamydia Screening Programme (NCSP) – GOV.UK
92. Surrey County Council. Household deprivation estimates from the 2021 census [Internet]. 2025 [cited 2025 Mar 10]. Available from: Census 2021: Household deprivation | Surrey-i
93. Department of Health and Social Care. Sexual and Reproductive Health Profiles – Chlamydia detection rate per 100,000 aged 15 to 24 (male) [Internet]. 2025 [cited 2025 Jan 28]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
94. Department of Health and Social Care. Sexual and Reproductive Health Profiles – Chlamydia diagnostic rate per 100,000 aged 25 years and older [Internet]. 2025 [cited 2025 Jan 28]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
95. UK Health Security Agency. Gonorrhoea: guidance, data and analysis [Internet]. 2024 [cited 2025 Jan 27]. Available from: Gonorrhoea: guidance, data and analysis – GOV.UK
96. UK Health Security Agency. Case-series of ceftriaxone-resistant Neisseria gonorrhoeae infections detected in England [Internet]. 2024 [cited 2025 Jan 27]. Available from: Case-series of ceftriaxone-resistant Neisseria gonorrhoeae infections detected in England – GOV.UK
97. UK Health Security Agency. Syphilis: surveillance, data and management [Internet]. 2022 [cited 2025 Jan 23]. Available from: Syphilis: surveillance, data and management – GOV.UK
98. UK Health Security Agency. Tracking the syphilis epidemic in England: 2013 to 2023 [Internet]. 2024 [cited 2025 Jan 23]. Available from: Tracking the syphilis epidemic in England: 2013 to 2023 – GOV.UK
99. UK Health Security Agency. HIV: surveillance, data and management [Internet]. 2024 [cited 2025 Jan 30]. Available from: HIV: surveillance, data and management – GOV.UK
100. Department of Health and Social Care. Sexual and Reproductive Health Profiles – HIV testing rate per 100, 000 population [Internet]. 2025 [cited 2025 Jan 30]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
101. UK Health Security Agency. HIV testing, PrEP, new HIV diagnoses and care outcomes for people accessing HIV services: 2024 report [Internet]. 2024 [cited 2025 Mar 14]. Available from: HIV testing, PrEP, new HIV diagnoses and care outcomes for people accessing HIV services: 2024 report – GOV.UK
102. UK Parliament. National HIV testing week [Internet]. 2025 [cited 2025 Mar 14]. Available from: HIV Testing Week – House of Commons Library
103. Department of Health and Social Care. Sexual and Reproductive Health Profiles – New HIV diagnoses among persons first diagnosed in the UK rate per 100,000 [Internet]. 2025 [cited 2025 Jan 30]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
104. Department of Health and Social Care. Sexual and Reproductive Health Profiles – HIV late diagnosis in gay, bisexual and other men who have sex with men first diagnosed with HIV in the UK [Internet]. 2025 [cited 2025 Jan 30]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
105. Department of Health and Social Care. Sexual and Reproductive Health Profiles – HIV late diagnosis in heterosexual men first diagnosed with HIV in the UK [Internet]. 2025 [cited 2025 Jan 30]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
106. Department of Health and Social Care. Sexual and Reproductive Health Profiles – HIV late diagnosis in heterosexual and bisexual women first diagnosed with HIV in the UK [Internet]. 2025 [cited 2025 Jan 30]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
107. Department of Health and Social Care. Sexual and Reproductive Health Profiles – HIV diagnosed prevalence rate per 1,000 aged 15 to 59 [Internet]. 2025 [cited 2025 Jan 30]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
108. UK Health Security Agency. HPV vaccination programme moves to single dose from September 2023 [Internet]. 2023 [cited 2025 Mar 11]. Available from: HPV vaccination programme moves to single dose from September 2023 – GOV.UK
109. Public Health England. Guidance, Genital Herpes [Internet]. 2013 [cited 2025 Jan 27]. Available from: Genital herpes – GOV.UK
110. Department of Health and Social Care. Sexual and Reproductive Health Profiles – Genital herpes diagnosis rate per 100,000 [Internet]. 2025 [cited 2025 Jan 27]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
111. UK Health Security Agency. Mycoplasma genitalium Antimicrobial Resistance Surveillance (MARS) report: 2023 [Internet]. 2024 [cited 2025 Jan 27]. Available from: Mycoplasma genitalium Antimicrobial Resistance Surveillance (MARS) report: 2023 – GOV.UK
112. Department of Health and Social Care. Sexual and Reproductive Health Profiles – Mycoplasma genitalium diagnostic rate per 100,000 [Internet]. 2025 [cited 2025 Jan 28]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
113. Department of Health and Social Care. Sexual and Reproductive Health Profiles – Trichomoniasis diagnostic rate per 100,000 [Internet]. 2025 [cited 2025 Jan 27]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
114. UK Health Security Agency. Sexually transmitted Shigella spp. in England: 2016 to 2023 [Internet]. 2024 [cited 2025 Jan 27]. Available from: Sexually transmitted Shigella spp. in England: 2016 to 2023 – GOV.UK
115. Department of Health and Social Care. Sexual and Reproductive Health Profiles – Sexually transmitted Shigella spp. per 100,000 adult male population [Internet]. 2025 [cited 2025 Jan 27]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
116. UK Health Security Agency. Mpox outbreak: epidemiological overview, 9 January 2025 [Internet]. 2025 [cited 2025 Jan 27]. Available from: Mpox outbreak: epidemiological overview, 9 January 2025 – GOV.UK
117. UK Health Security Agency. Mpox: background information [Internet]. 2025 [cited 2025 Jan 27]. Available from: Mpox: background information – GOV.UK
118. Fink DL, Callaby H, Luintel A, Beynon W, Bond H, Lim EY, et al. Clinical features and management of individuals admitted to hospital with monkeypox and associated complications across the UK: a retrospective cohort study. Lancet Infect Dis. 2023 May;23(5):589–97.
119. UK Health Security Agency. HCID status of mpox [Internet]. 2024 [cited 2025 Feb 20]. Available from: HCID status of mpox – GOV.UK
120. Herbert A, Heron J, Barter C, Szilassy E, Barnes M, Howe LD, et al. Risk factors for intimate partner violence and abuse among adolescents and young adults: findings from a UK population-based cohort. Wellcome Open Res. 2021 Jan 21;5:176.
121. Surrey Police. Domestic abuse – Support organisations [Internet]. 2025 [cited 2025 Jan 27]. Available from: Support organisations for victims of domestic violence | Surrey Police
122. Healthy Surrey. Surrey Sexual Assault Referral Centre (SARC) [Internet]. 2025 [cited 2025 Jan 27]. Available from: Surrey Sexual Assault Referral Centre (SARC) | Healthy Surrey
123. World Health Organisation. Female genital mutilation [Internet]. 2024 [cited 2025 Jan 27]. Available from: Female genital mutilation
124. Surrey Police. Female genital mutilation [Internet]. 2025 [cited 2025 Jan 27]. Available from: Female genital mutilation (FGM) | Surrey Police
125. National Institute for Health and Care Excellence. Sexual Health, Quality Standard [QS178]. London; 2018 Feb.
126. BASHH. 2015 UK national guideline for the management of infection with Chlamydia trachomatis. 2018 [cited 2025 Mar 13]; Available from: Chlamydia 2015 | BASHH
127. BASHH. UK national guideline for the management of infection with Neisseria gonorrhoeae. 2020 [cited 2025 Mar 13]; Available from: Gonorrhoea 2018 | BASHH
128. BASHH. UK guidelines for the management of syphilis 2024 [Internet]. 2024 [cited 2025 Mar 13]. Available from: Syphilis 2024: Updated Guideline | BASHH
129. BHIVA, BASHH, BIA, RCHEM Joint Working Group. BHIVA, BASHH, BIA and RCEM Joint Working Group. 2024 [cited 2025 Mar 13]. Rapid guidance on opt-out blood-borne virus testing in high-prevalence and extremely high-prevalence acute medical settings and emergency departments. Available from: BHIVA, BASHH, BIA and RCEM joint working group: rapid guidance on opt-out blood-borne virus testing in high-prevalence and extremely high-prevalence acute medical settings and emergency departments | BASHH
130. BASHH, BHIVA, BIA. Adult HIV Testing Guidelines 2020 [Internet]. 2020 [cited 2025 Mar 13]. Available from: HIV Testing Guidelines (with BHIVA/BIA) 2020 | BASHH
131. BASHH, BHIVA. The use of HIV Pre-Exposure Prophylaxis 2018 [Internet]. 2018 [cited 2025 Mar 13]. Available from: HIV Pre-Exposure Prophylaxis 2025 – updated guideline | BASHH
132. BASHH, BHIVA, FSRH. The management of the sexual and Reproductive Health of people living with HIV infection 2008 [Internet]. 2008 [cited 2025 Mar 13]. Available from: Sexual and Reproductive Health of PLWHIV (2008) (with BHIVA and FSRH) | BASHH
133. BASHH, BHIVA, SSHA, NAT. HIV Partner Notification for Adults: Definitions, Outcomes and Standards 2015 [Internet]. 2015 [cited 2025 Mar 13]. Available from: BASHH/BHIVA/SSHA/NAT HIV Partner Notification for Adults: Definitions, Outcomes and Standards 2015 | BASHH
134. NICE. Reducing sexually transmitted infections [Internet]. 2022 [cited 2025 Mar 13]. Available from: Overview | Reducing sexually transmitted infections | Guidance | NICE
135. NICE. HIV testing: increasing uptake among people who may have undiagnosed HIV [Internet]. 2016 [cited 2025 Mar 13]. Available from: Overview | HIV testing: increasing uptake among people who may have undiagnosed HIV | Guidance | NICE
136. National Institute for Health and Care Excellence. Contraception, Quality Standard [QS129] [Internet]. 2016 [cited 2025 Feb 20]. Available from: Overview | Contraception | Quality standards | NICE
137. The Faculty of Sexual and Reproductive Healthcare. Standards & Guidance. 2025 [cited 2025 Sep 09]. Available from: Standards and Guidelines | CoSRH
138. NICE. Long-acting reversible contraception. 2019 [cited 2025 Sep 09]. Available from: Overview | Long-acting reversible contraception | Guidance | NICE
139. NICE. Contraceptive services for under 25s. 2014 [cited 2025 Sep 09]. Available from: Overview | Contraceptive services for under 25s | Guidance | NICE
140. RCOG. Best practice in post-abortion contraception. 2022 [cited 2025 Sep 09]. Available from: post-abortion-contraception-best-practice-paper-2022.pdf
141. RCOG, FSRH. Management of unscheduled bleeding in women using hormonal contraception. 2009 [cited 2025 Sep 09]. Available from: CEU-Unscheduledbleeding
142. Office for Health Improvement and Disparities. Integrated sexual health service specification [Internet]. 2023 [cited 2025 Mar 11]. Available from: Integrated sexual health service specification
143. NICE. Quality standard: Contraception after an abortion [Internet]. 2016 [cited 2025 Feb 12]. Available from: Quality statement 3: Contraception after an abortion | Contraception | Quality standards | NICE
144. NICE. Pre-conception – advice and management [Internet]. 2023 [cited 2025 Feb 12]. Available from: Pre-conception – advice and management | Health topics A to Z | CKS | NICE
145. Hall J, Carr H, Connolly A, Barrett G. How, when, and who should ask about pregnancy intentions in primary care? A qualitative study of primary healthcare professionals’ preferences. BJGP Open. 2024 Dec;8(4):BJGPO.2024.0148.
146. Public Health England. Health of women before and during pregnancy: health behaviours, risk factors and inequalities. 2019 [cited 2025 Sep 09]. Available from: Health of women before and during pregnancy: health behaviours, risk factors and inequalities
147. World Health Organisation. Report of a WHO technical consultation on birth spacing: Geneva, Switzerland 13-15 June 2005. [Internet]. 2007 [cited 2025 Feb 12]. Available from: Report of a WHO Technical Consultation on Birth Spacing
148. NICE. Quality standard: Contraception after childbirth [Internet]. 2016 [cited 2025 Feb 12]. Available from: Quality statement 4: Contraception after childbirth | Contraception | Quality standards | NICE
149. The Faculty of Sexual and Reproductive Healthcare. Contraception After Pregnancy [Internet]. 2020 [cited 2025 Feb 12]. Available from: FSRH Guideline Contraception After Pregnancy
150. Healthy Surrey. Young people’s sexual health services (under 25 year olds) [Internet]. 2025 [cited 2025 Feb 12]. Available from: Young people’s sexual health services (under 25 year olds) | Healthy Surrey
151. Mountain Healthcare. Solace Centre Sexual Assault Referral Centre [Internet]. 2025 [cited 2025 Mar 11]. Available from: Home – The Solace Centre
152. Surrey County Council. Population, A quick guide to content [Internet]. 2024 [cited 2024 Oct 22]. Available from: Population | Surrey-i
153. NHS England. Sexual and Reproductive Health Services, England – 2016-17 [Internet]. 2017 [cited 2025 Mar 10]. Available from: Sexual and Reproductive Health Services, England – 2016-17 – NHS England Digital
154. UK Health Security Agency. Sexually transmitted infections: annual data [Internet]. 2024 [cited 2025 Mar 14]. Available from: Sexually transmitted infections (STIs): annual data – GOV.UK
155. Wayal S, Hughes G, Sonnenberg P, Mohammed H, Copas AJ, Gerressu M, et al. Ethnic variations in sexual behaviours and sexual health markers: findings from the third British National Survey of Sexual Attitudes and Lifestyles (Natsal-3). Lancet Public Health. 2017 Oct;2(10):e458–72.
156. Mitchell HD, Vilaplana TG, Mandal S, Ratna N, Glancy M, Shah A, et al. Effects of COVID-19 Pandemic Response on Service Provision for Sexually Transmitted Infections, HIV, and Viral Hepatitis, England. Emerg Infect Dis. 2022 Mar;28(3):739–42.
157. Surrey County Council. Index of Multiple Deprivation 2019: What it is and what it tells us about Surrey. 2020 [cited 2025 Sep 09]. Available from: Index of Multiple Deprivation 2019 What it is and What it tells us about Surrey
158. Mestad RE, Kenerson J, Peipert JF. Reversible Contraception Update: The Importance of Long-Acting Reversible Contraception. Postgrad Med. 2009 Jul 13;121(4):18–25.
159. Mavranezouli I. The cost-effectiveness of long-acting reversible contraceptive methods in the UK: analysis based on a decision-analytic model developed for a National Institute for Health and Clinical Excellence (NICE) clinical practice guideline. Human Reproduction. 2008 Apr 11;23(6):1338–45.
160. Department of Health and Social Care. Sexual and Reproductive Health Profiles – LARC [Internet]. 2025 [cited 2025 Feb 12]. Available from: Fingertips | Department of Health and Social Care
161. UK Health Security Agency. Summary profile of local authority sexual health: Surrey. 2025 [cited 2025 Sep 09]. Available from: Sexual and Reproductive Health Profiles – Data | Fingertips | Department of Health and Social Care
162. London School of Hygiene and Tropical Medicine. Women’s Reproductive Health Survey 2023: Summary of Initial Findings [Internet]. 2024 [cited 2025 Feb 12]. Available from: Women’s Reproductive Health Survey 2023 – initial results
163. Surrey County Council. Surrey Youth Voice [Internet]. 2025 [cited 2025 Jan 31]. Available from: Surrey Youth Voice – Surrey County Council
164. Surrey County Council. Support for young people who are LGBT+ [Internet]. 2024 [cited 2025 Feb 12]. Available from: Support for young people who are LGBT+ – Surrey County Council
165. NHS England. Disclosure control methodology for Hospital Episode Statistics (HES) and Emergency Care Data Set (ECDS) [Internet]. 2023 [cited 2025 Feb 26]. Available from: Disclosure control methodology for Hospital Episode Statistics (HES) and Emergency Care Data Set (ECDS) – NHS England Digital